Hematology Unit 1 Exam
1/69
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
70 Terms
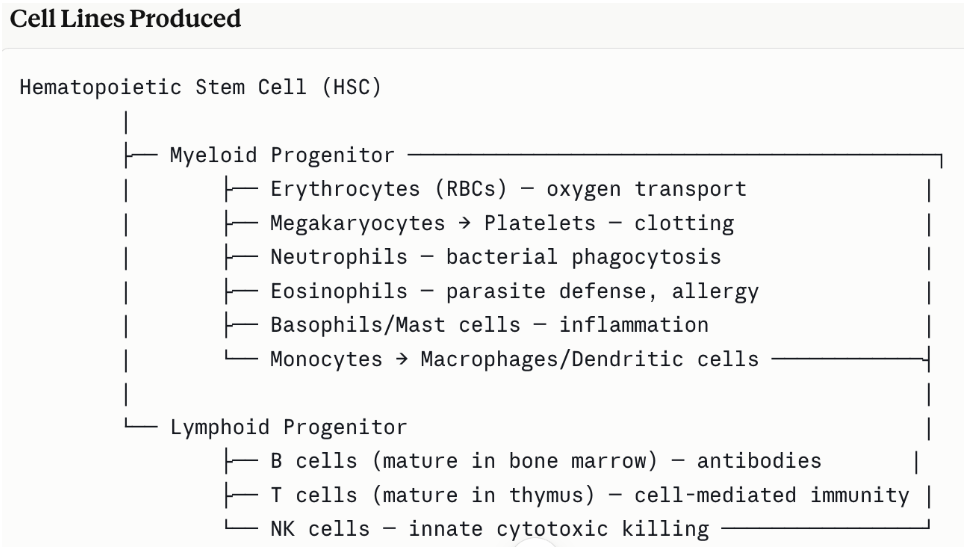
Hematopoiesis
The dynamic process of blood cell production and development of the various cells of the blood
Bone Marrow Function
main site of cell production in fetus (from 2-7 months)
Primary site of hematopoiesis
Core functions:
Generating rbcs for O2 transport
Producing platelets for clotting
Creating all leukocytes, including lymphocyte precursors
Serving as a primary lymphoid organ where B-cells mature and become immunocompetent
Provide stem cell reservoir (hematopoietic stem cells) from which all blood lineages derive
Spleen Function
Second largest lymphoid organ and serves as a blood filter and immune surveillance hub
Filters the blood: removes old, damaged, or abnormal rbcs
Immune surveillance: traps blood-born Ag and presents them to lymphocytes
Mounts immune responses to blood-borne pathogens (bacteria, viruses, parasites)
Stores a reserve of monocytes and platelets
In fetal life, major site of hematopoiesis
Liver Function
Primary site of fetal hematopoiesis before the bone marrow takes over
Produces majority of complement proteins
Synthesizes acute-phase proteins during inflammation
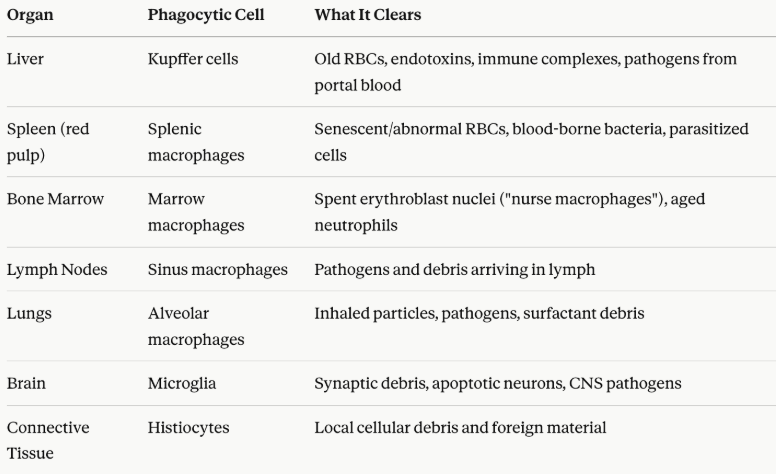
Houses Kupffer cells: resident macrophages that phagocytose pathogens and debris from portal blood
Metabolizes and clears immune complexes and endotoxins
Produces clotting factors essential for hemostasis
Thymus Function
Primary lymphoid organ critical for T-cell development and self-tolerance
Site where T-cell precursors mature into functional, immunocompetent T-cells
Oversees positive selection — ensuring T cells can recognize self-MHC molecules
Oversees negative selection — eliminating T cells that react too strongly to self-antigens (preventing autoimmunity)
Exports mature naïve T cells to the peripheral circulation
Most active during childhood; undergoes involution (shrinkage) with age, though it retains some function throughout life
Lymph Nodes
Lymph nodes are small, bean-shaped secondary lymphoid organs distributed throughout the body along lymphatic vessels:
Filter lymph fluid, trapping pathogens, cancer cells, and foreign antigens
Serve as sites of antigen presentation — where dendritic cells present antigens to T and B cells
Facilitate adaptive immune responses — clonal expansion of antigen-specific lymphocytes occurs here
Produce antibody-secreting plasma cells (from activated B cells) and effector/memory T cells
The characteristic swelling of lymph nodes during infection ("swollen glands") reflects active immune responses
Reticuloendothelial system (RES)
The reticuloendothelial system (RES) — also called the mononuclear phagocyte system (MPS) in modern terminology — is a diffuse network of phagocytic cells and supporting stromal (reticular) cells distributed throughout the body.
Rather than a discrete anatomical organ, it is a functional system spanning multiple organs and tissues, unified by its roles in hematopoiesis, waste clearance, and immune defense
RES and Cell Production
Hematopoiesis is the generation of all cellular blood components from hematopoietic stem cells (HSCs). The RES both produces and supports this process through reticular stromal scaffolding and cytokine signaling.
Red bone marrow = site of adult hematopoiesis
Role of Reticular Stroma
The reticular cells and fibers of the bone marrow, lymph nodes, and spleen create the microenvironmental niche (hematopoietic niche) that:
Physically anchors developing blood cells
Provides growth factors (SCF, IL-3, GM-CSF, EPO, TPO)
Regulates the balance between self-renewal and differentiation
RES and Cell Destruction
The RES is the body's primary system for removing aging cells, debris, pathogens, and abnormal cells through two overlapping mechanisms.
Phagocytosis: the active engulfment and degradation of particles by professional phagocytes — chiefly macrophages, monocytes, neutrophils, and dendritic cells.
Mechanism: Recognition, opsonization, engulfment, killing, processing (apc activity)
Apoptosis (programmed cell death): the intrinsic death program of cells — but the RES plays a critical role in recognizing and clearing apoptotic cells (efferocytosis) before they become inflammatory
Key RES sites and phagocytic roles in photo
How the RES handles apoptosis
Apoptotic cells display "eat-me" signals
RES macrophages recognize these via receptors (integrins) and phagocytose the cell corpse silently, without triggering inflammation
This is critical in the thymus, where ~95% of developing T cells undergo apoptosis during negative/positive selection — thymic macrophages and dendritic cells rapidly clear these corpses
In germinal centers of lymph nodes, B cells that fail to bind antigen with sufficient affinity undergo apoptosis and are cleared by tingible body macrophages (macrophages visible with engulfed nuclear debris)
Failure to clear apoptotic debris efficiently (as in lupus) can lead to autoimmune disease
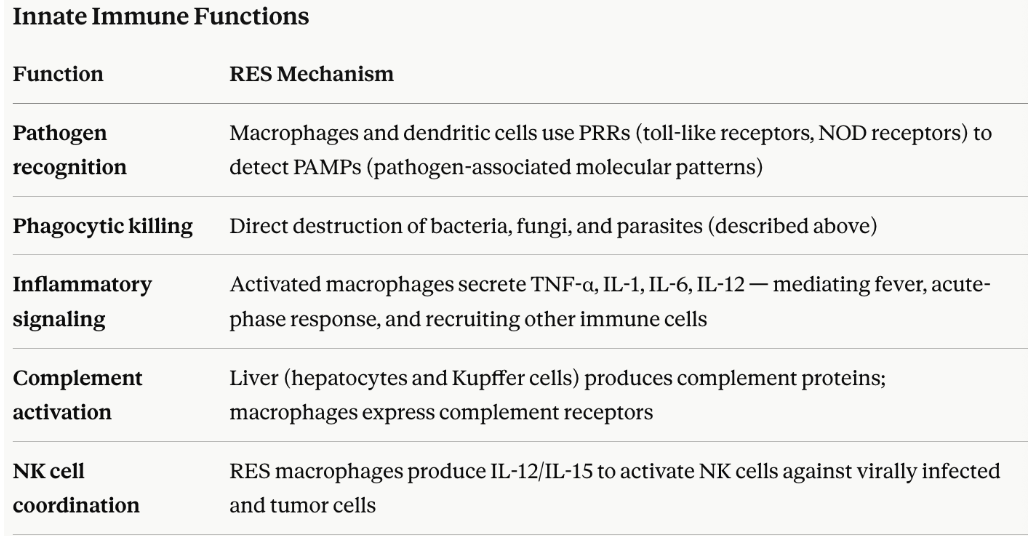
RES and immunologic defense
RES sits at the intersection of innate and adaptive immunity, both executing immediate defense and orchestrating long-term immune responses
Bridge to Adaptive Immunity - Ag presentation
A defining immunologic role of the RES is antigen processing and presentation, linking innate sensing to adaptive (T and B cell) responses:
Dendritic cells (the most potent APCs) in skin, mucosa, and tissues capture antigens
They migrate to lymph nodes and spleen — both RES organs
Antigenic peptides are loaded onto MHC class I (for CD8⁺ T cells) or MHC class II (for CD4⁺ T helper cells)
Macrophages in lymph nodes and spleen present antigen and provide co-stimulatory signals
This initiates clonal expansion of antigen-specific T and B cells → effector cells and immunological memory
Describe the function of nuclear and cytoplasmic cell structures (e.g., chromatin, nucleolus, mitochondria, Golgi, lysosomes, ribosomes).
Generally, they regulate gene expression and produce proteins necessary for cellular survival.
Chromatin: packaged DNA and proteins that condense into chromosomes during cell division
Nucleolus: sub-structure
Mitochondria: generates most of the cell’s ATP for energy
Golgi: packages proteins and lipids for delivery to designated locations
Lysosomes: break down worn-out cell parts, foreign invaders like bacteria, and biomolecules (proteins, lipids, and carbohydrates) into simpler building blocks for the cell to reuse or expel
Ribosomes: make proteins based on instructions delivered from nucleus
erythropoiesis
The production of red blood cells in the bone marrow
Describe factors involved in the regulation of erythrocyte production, including substances needed for erythropoiesis and hemoglobin synthesis
Production of rbcs is controlled by rate of oxygen delivery
Regulated by EPO, EPO response takes ~5 days
Androgens influence RBC production
Leukopoiesis
Production of leukocytes (WBCs)
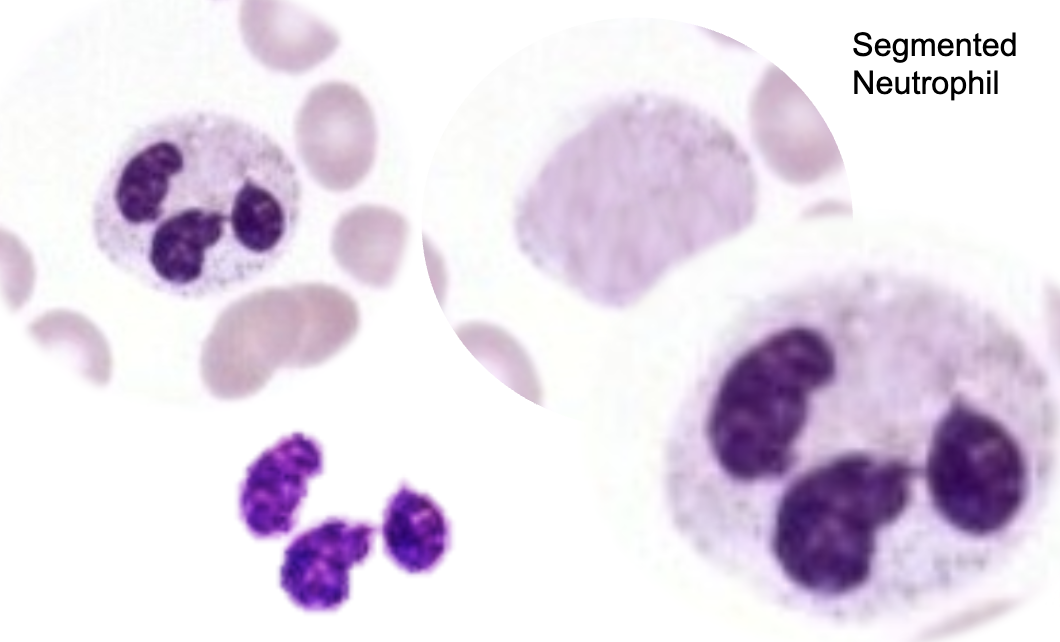
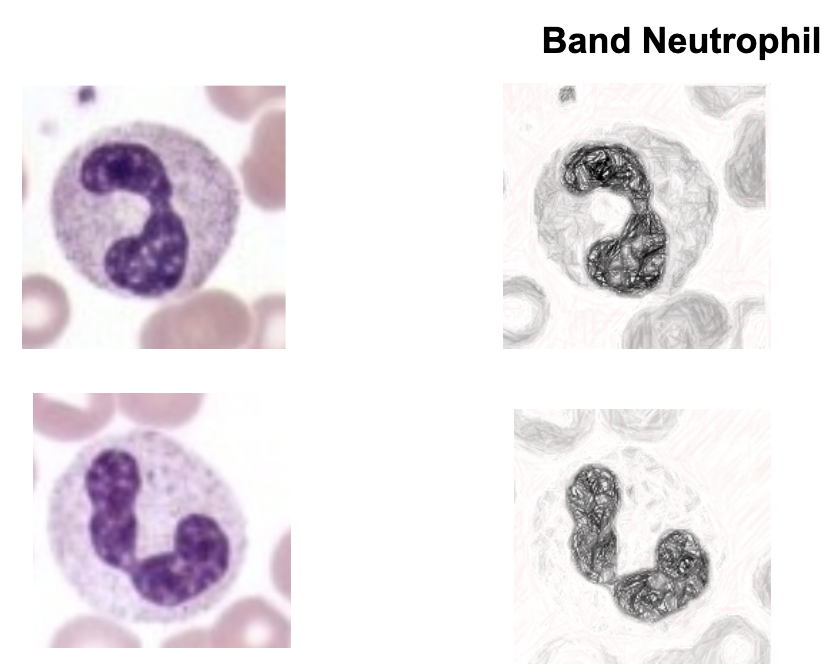
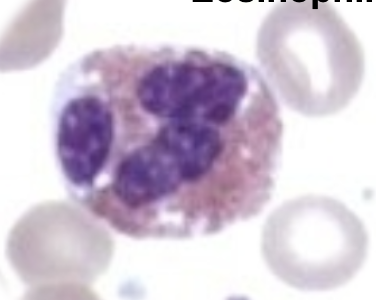
Neutrophils
the primary first responders of the innate immune system. Produced daily in the bone marrow, they circulate in the blood and quickly migrate to sites of infection or injury to destroy invading pathogens and clear cellular debris
Circulation is less than 24 hours, but lifespan can be 3-5 days in tissues.
Differential percentage range: 45-75%
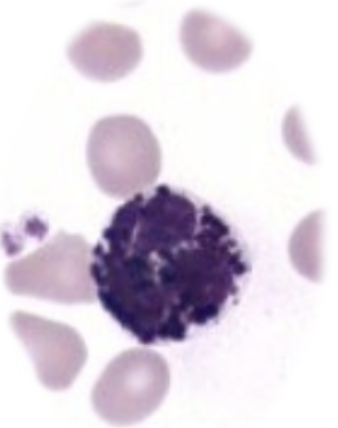
Eosinophils
fighting parasitic infections, regulating allergic responses, and maintaining tissue homeostasis
Circulate 8-18 hours, but can live in tissues for 2-5 days
Differential percentage: 0-6%
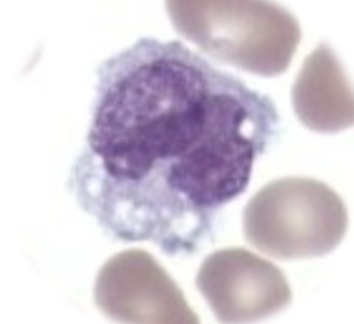
Basophils/Mast Cells
release active chemical granules—most notably histamine and heparin—to defend the body against parasites, manage allergic reactions, and regulate inflammation. One of the first responder cells for immune system.
Circulate 24-48 hours, so 1-2 days
Differential percentage: 0.2%
Monocytes/Macrophages
engulfing and destroying invading pathogens (phagocytosis), regulating inflammatory responses, cleaning up dead or damaged cells, and presenting antigens to activate the adaptive immune system
Circulate 1-3 days, then live in tissues for months to years
Differential percentage: 1-12%
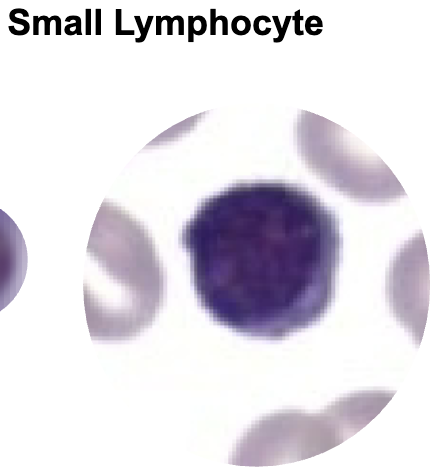
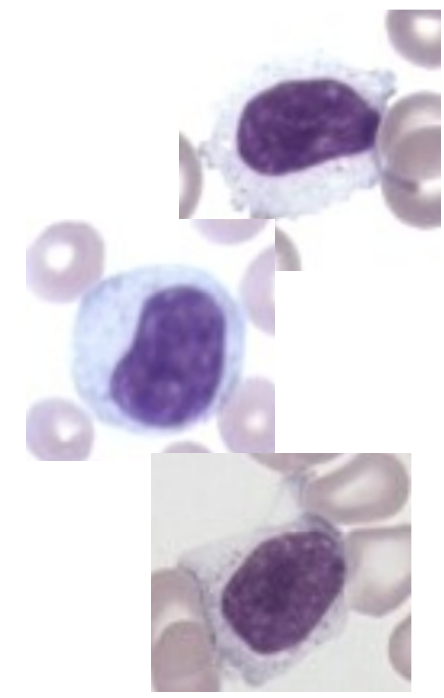
Lymphocytes
identify, target, and destroy pathogens (bacteria, viruses), abnormal cells (cancer), and toxins. They also retain "memory" of past infections to prevent you from getting sick from the same threat twice. B-cells and T-cells
Lifespan: weeks to months, but memory cells can last years
Differential percentage: 15-45%
Plasma Cells
secrete massive quantities of immunoglobulins (antibodies) to neutralize pathogens, playing a central role in humoral immunity
A few days to months, but long-lived plasma cells in bone marrow can live from decades to an entire lifetime
Differential percentage 1-3%
Thrombopoiesis
the physiological process of blood platelet (thrombocyte) formation in the bone marrow, primarily driven by the hormone thrombopoietin (TPO).
Platelet lifespan and pools
Platelets live 7-10 days
Circulating pool: Makes up about 70% of the total platelet mass. These are the platelets actively flowing in the bloodstream
Splenic pool: Makes up the remaining 30%. The spleen acts as a dynamic reserve that freely exchanges with the circulating pool
Platelet function
clot
List the common specimen types analyzed in Clinical Hematology
Blood, bone marrow, synovial fluid, pleural fluid, serous fluid
Explain the action of the anticoagulants most commonly used to obtain whole blood or plasma specimens for Clinical Hematology testing
EDTA: prevents blood coagulation by chelating calcium (removing it from blood)
Sodium Citrate: works by chelating (binding to) calcium ions in the blood, which inhibits the clotting cascade and prevents the blood from coagulating outside the body
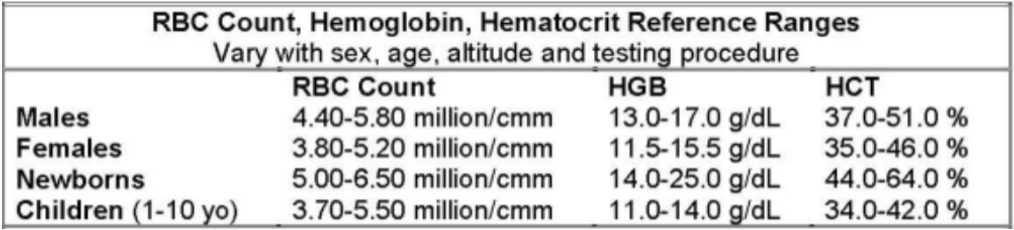
Routine Tests for Clinical Hematology
HGB:
Male: 13.0 - 17.0 g/dL
Female: 11.5 - 15.5 g/dL
Report to nearest 10th
HCT:
Male: 37.0 - 51.0%
Female: 35.0 - 46.0%
Report to nearest 10th
RBC:
Male: 4.40 - 5.80 x 10^6/uL or M/uL or M/cmm
Female: 3.80 - 5.20 x 10^6/uL
Report to nearest 100th
WBC:
Adult: 4.0 - 11.0 x 10^3/uL or K/uL or K/cmm
Report to nearest 10th if decimal (e.g. 7.7 x 10^3/uL)
Report to nearest hundred if no decimal (e.g. 7,700/uL)
PLT:
150 - 45 x 10^3/uL or K/uL or K/cmm
Report to nearest thousand (e.g. 150,000/uL or 150 x 10^3/uL)
RBC Indices:
MCV: 82.0 - 98.0 fL → report to nearest 10th
MCH: 27.0 - 33.0 pg → pg = picograms
MCHC: 32.0 - 36.0%
Evaluate specimen requirements for each routine test performed in Clinical Hematology (e.g., preferred anticoagulant for cell counts), including stability times and minimum blood draw requirements
Stability Time
Analyze within 24 hours, otherwise, store at 2-8°C if testing is delayed
Blood Draw Requirements:
EDTA, purple top tube
Venipuncture is preferred
Specimen Type: whole blood, no clots or hemolysis
Molecular structure, synthesis (e.g., protoporphyrin) and breakdown/catabolism of hemoglobin
Molecular structure:
B-chains, a-chains, Heme, iron, polypeptide chains
Major 3 are protoporphyrin, iron, and globin
Synthesis:
65% is synthesized during nucleated RBC maturation
35% during reticulocyte stage
Hemoglobin requires the following for production:
Adequate iron delivery and supply
Adequate synthesis of protoporphyrin (heme precursor)
Adequate globin synthesis
Catabolism/Breakdown
Protoporphyrin ring of Heme is cleaved and is broken down to bilverdin, then is reduced to unconjugated bilirubin
Albumin transports unconjugated bilirubin to liver and converts it to conjugated bilirubin
Conjugated bilirubin is excreted into the bile and then reduced by bacteria in the colon into urobilinogens.
Iron is released, bound to transferrin, and recycled for hgb production or goes into storage
Globin polypeptides are hydrolyzed to amino acids and returned to amino acid pool for protein synthesis
Iron metabolism and iron pools/compartments, including storage forms (e.g., ferritin) and the role of the transport protein transferrin
Iron Metabolism:
Iron is released, bound to transferrin, and recycled for hgb production or goes into storage
Iron Compartments
⅔ hemoglobin (largest storage)
Ferritin = storage iron
Myoglobin
Tissue Iron (cytochrome enzymes)
Transport proteins (smallest storage) → bound to transferrin
Storage forms
ferritin
Role of transport protein Transferrin
Dietary Iron (ferric) → reduced to ferrous (Fe2+) by HCl → ferrous absorbed through intestinal mucosa oxidized back to ferric → ferric is transported by transferrin to body tissues and storage compartments
Hemoglobin A
97% in adults
2 alpha chains
2 beta chains
Hemoglobin A2
2% of adult hgb
2 alpha chains
2 delta chains

Hemoglobin F
fetal hemoglobin
1% of adult hgb
2 alpha chains
2 gamma chains

percentage of fetal hemoglobin at birth
80%
Normal hemoglobin forms with ferrous iron and oxygen carrying function (oxyhemoglobin, deoxyhemoglobin)
Oxyhemoglobin (Fe2+ with O2)
Expelled 2,3-DPG
Deoxyhemoglobin (Fe2+ w/out O2)
Binding 2,3-DPG
Iron must be in Ferrous state (Fe2+) to transport O2
2,3-diphosphoglycerate (2,3-DPG): important for loading and unloading oxygen
Binding 2,3-DPG unloads O2, and expelling loads O2
Hemoglobin forms unable to transport oxygen (methemoglobin, carboxyhemoglobin)
These hgb are unable to transport or deliver O2
At toxic levels, tissue O2 decreases → cyanosis → hypoxia → coma/death
Methemoglobin:
Iron is oxidized to Fe3+ state (ferric)
Ferric iron can’t carry O2
Brown color of blood, reversible
Carboxyhemoglobin:
O2 replaced with carbon monoxide
Cherry red color of blood, reversible
CO is binding 200x greater than O2
Hemoglobin types with abnormal structure (S, C), including altered properties (e.g., solubility, electrophoretic mobility)
Hemoglobin S
Point mutation replaces hydrophilic glutamic acid with hydrophobic valine at the 6th position of the B-globin chain
Under low O2 conditions, the hydrophobic valine residues fit into complementary hydrophobic pockets on adjacent HbS molecules
This causes abnormal polymerisation, where the hemoglobin molecules bond together to form long, rigid, helical fibers.
This distorts RBCs, forcing them into a crescent or sickle cell shape. This makes the cells fragile, leading to chronic hemolytic anemia.
Hemoglobin C
Point mutation at same 6th position of B-globin chain replaces glutamic acid with basic lysine
Substitution of lysine decreases solubility of the Hgb molecule
Bc it lacks the polymerization tendency of HbS, it doesn’t cause sickling. The molecules tend to aggregate, and intracellularly crystallize (often forming hexagonal or rod-shaped crystals), particularly when the cells are dehydrated.
Causes mild chronic hemolytic anemia and splenomegaly (enlarged spleen) due to the spleen removing these rigid, crystal-containing cells.
Protects against severe malaria
Describe the principle and accuracy of the cyanmethemoglobin method (or modifications) for determination of hemoglobin concentration, including hemoglobin forms measured
Principle: it’s the reference method for measuring hemoglobin concentration in the blood. Uses Drabkin’s reagent (potassium ferricyanide). It converts hemoglobin to cyanmethemoglobin. Photometric absorbance of cyanmethemoglobin is measured at 540 nm. Measures all clinically significant forms of Hgb.
Considered the international reference method for hemoglobin determination.
Highly accurate because nearly all hemoglobin forms are converted to a single stable pigment.
Follows Beer-Lambert principles over a wide analytical range.
Provides excellent reproducibility and standardization between laboratories.
Evaluate possible sources of error when measuring hemoglobin photometrically (e.g., lipemia, bilirubinemia, WBC count over linearity)
Lipids & Bilirubin: affect photometric measurements that check for hemoglobin → can make Hgb results inaccurate because it makes the solution cloudier than it should be
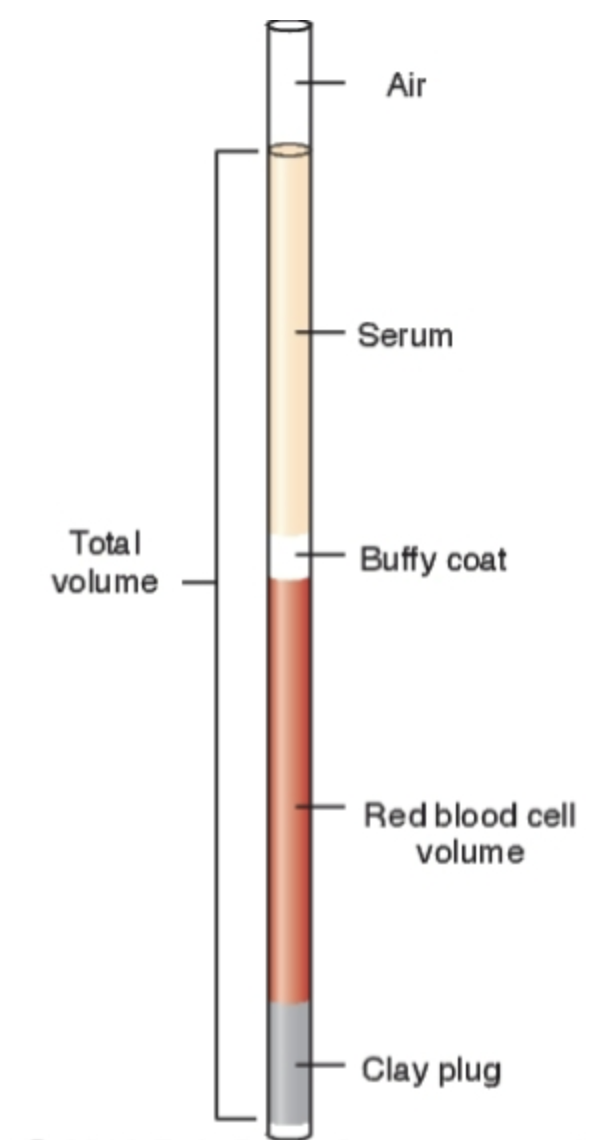
Evaluate a manual spun hematocrit determination, taking into account the principle, acceptable specimen, and sources of error caused by pre-analytical, mechanical and technical variables
Percentage of red cells in a given volume of whole blood.
Manual spun HCT centrifuges blood into layers
Volume of packed red cells reported to nearest 0.5%
Sources of Error
Pre-analytic/blood collection errors
Not wiping off first blood drop if collected by fingerstick
EDTA tube must be at least half full for manual HCTs
Analytic/technical errors
Improper use of HCT card reader
Control sample “out”
Centrifuging at improper speed or time
RBC count, Hgb and HCT measurements parallel each
Evaluating the control for a manual spun hematocrit
Control samples are run to verify the manual spun hematocrit procedure is producing accurate and reliable results. When one level is analyzed, the result is compared with the manufacturer’s est. acceptable range.
When the control is within acceptable limits: the system is functioning properly, and technique is acceptable, patient results may be reported.
Control outside acceptable limits indicates a possible problem in the analytical phase and patient results should not be reported until the issue is resolved.
Causes of erroneous results when running the hematocrit controls
centrifuge malfunction: verify RPM and timer settings and repeat centrifugation
improper centrifugation time: centrifuge using correct procedure
faulty reader: check calibration and reread specimen
improper tube filling: recollect or prepare a properly filled tube
poor mixing of specimen: remix specimen thoroughly and repeat test
Excess plasma trapped between cells: ensure proper centrifugation conditions
Deteriorated or expired control material: use fresh control material
Clotted specimen: reject specimen and obtain a new sample
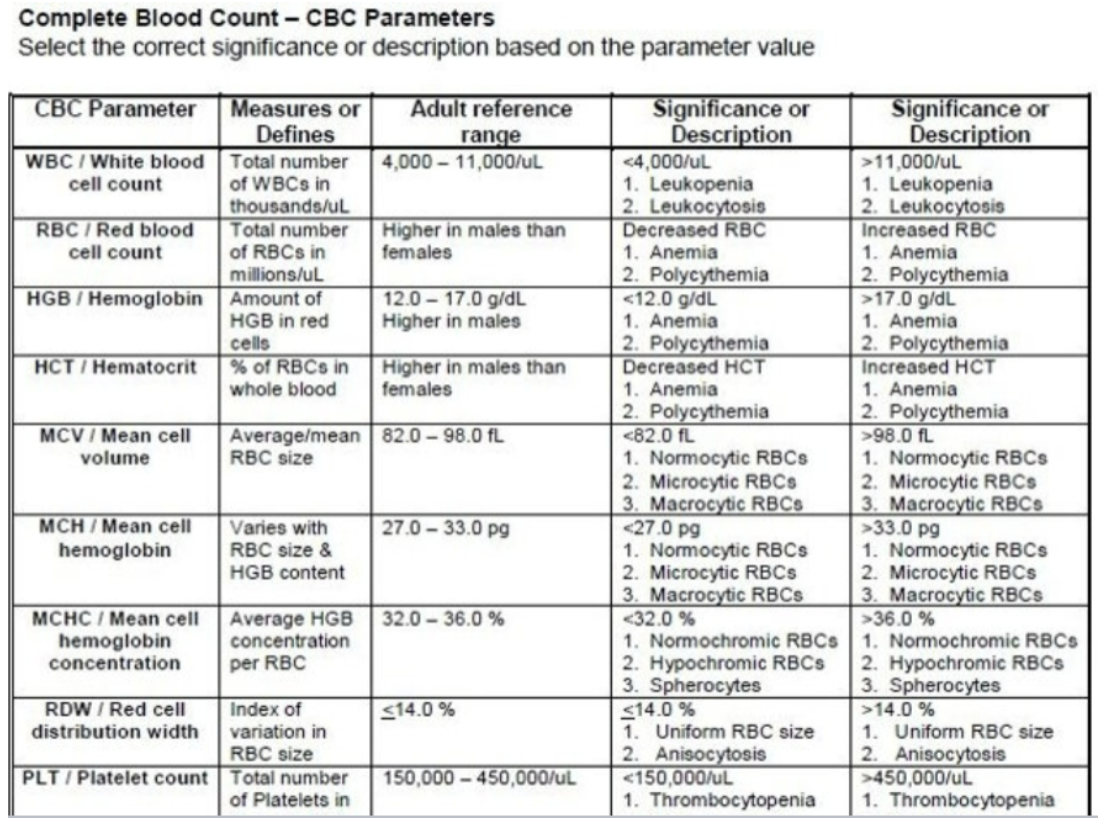
Evaluate the significance of RBC, hemoglobin and hematocrit results in terms of age and sex (e.g., anemia, polycythemia).
↓ RBC, HGB and/or HCT values….Anemia
Decreased production, increased loss/destruction
↑ RBC, HGB and/or HCT values….Polycythemia
Increase production
Critical values: Hgb <7.0 or ≥21.0 g/dL (varies)
Evaluate laboratory data using correlations between RBC, hemoglobin and hematocrit values.
Rule of Three
HGB x 3 = HCT +/- 3%
RBC x 3 = HGB
RBC x 9 = HCT
Used to estimate values or check data correlation
Rules only apply if red cells are normal in size and hgb content
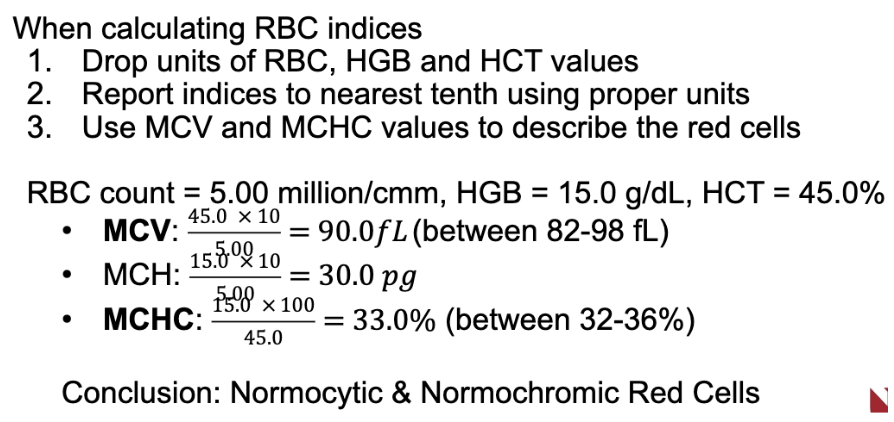
Calculate the RBC indices including MCV, MCH and MCHC using proper reporting format
MCV (mean cell volume)
MCH (mean cell hemoglobin)
MCHC (mean cell hemoglobin concentration)
Calculated using RBC, HGB, and HCT values
Invalid if erroneous values used for calculation
MCV and MCHC are used to describe the red cells and classify types of anemia
Correlate with appearance of red cells seen on blood smear
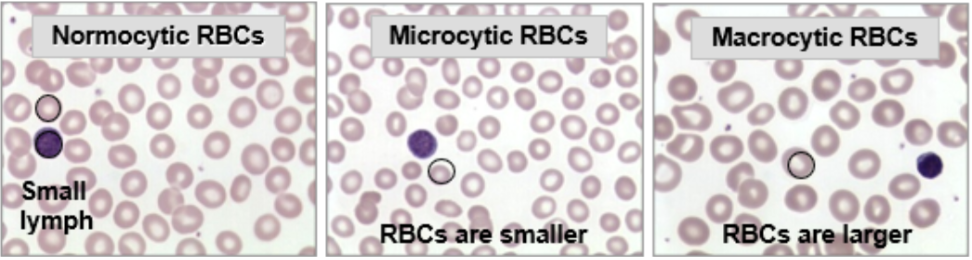
Correlate normal and abnormal RBC size and hemoglobin content with MCV
MCV: RBC Size
Normal MCV (82.0-98.0 fL): normocytic red cells, about the size as the nucleus of a small lymph
Small MCV (<82.0 fL): microcytic red cells
Large MCV (98.0 fL): macrocytic red cells
Correlate normal and abnormal RBC size and hemoglobin content with MCH
MCH: average weight of hemoglobin per RBC in picograms
Varies with both RBC size and hgb content → not used dto describe the red cells
Normal MCH 27.0-33.0 pg = red cells are usually normocytic and normochromic
MCH <27 pg = microcytic and/or hypochromic red cells
If red cells are microcytic, MCH is low due to decreased size
If microcytic red cells are also hypochromic, MCH is lower
MCH >33 pg = macrocytic and normochromic red cells
MCV and MCH values generally parallel each other, e.g., if MCV is increased, MCH is increased
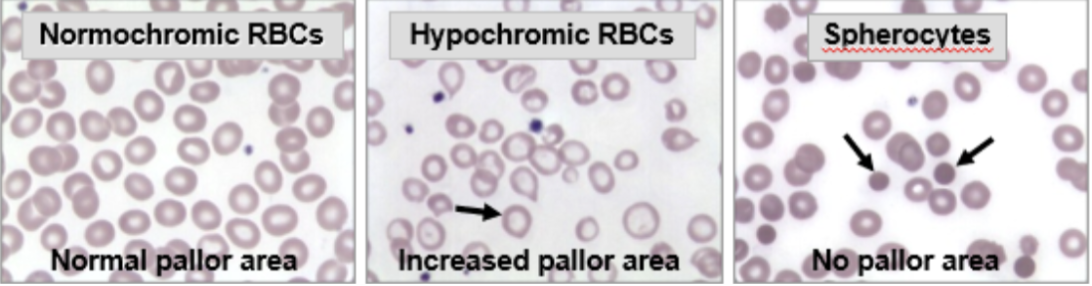
Correlate normal and abnormal RBC size and hemoglobin content with MCHC values
Normal Hgb concentration (32.0 – 36.0%): normochromic red cells
Low Hgb concentration (MCHC <32.0%): hypochromic red cells with increased pallor area
High Hgb concentration (>36.0%): red cells are spherocytes with no pallor area → NOT HYPERCHROMIC
MCV, MCH, MCHC Equations
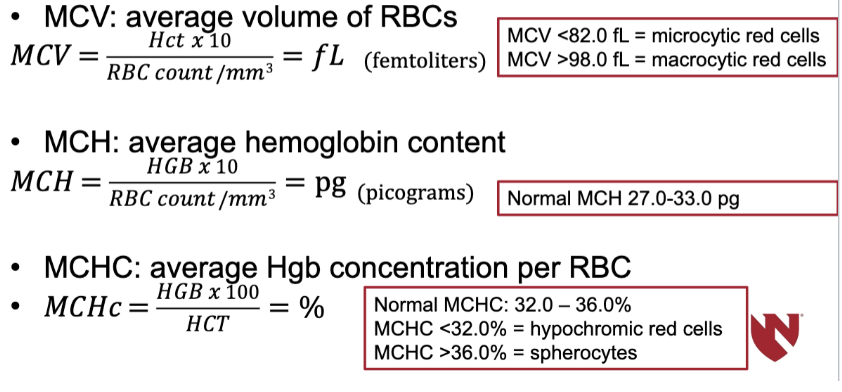
RBC Indices Equations
Evaluate the significance of WBC counts and PLT counts (e.g., leukopenia, thrombocytosis).
Preparation and staining of peripheral blood smears using Wright’s stain
Principle of Romanowsky-type stains
Well-made smears are essential to the evaluation of hematologic disorders
These are pH-dependent reactions
Action of the reagents/dyes
Methylene blue
Stains acid cell structures a blue color
RNA in cytoplasm, basophil granules
Eosin
Stains basic cell structures a red-orange color
Hgb in RBCs, eosinophil granules
Combo of Both Dyes
Stains neutral cell structures a pinkish-tan color
Neutrophil granules
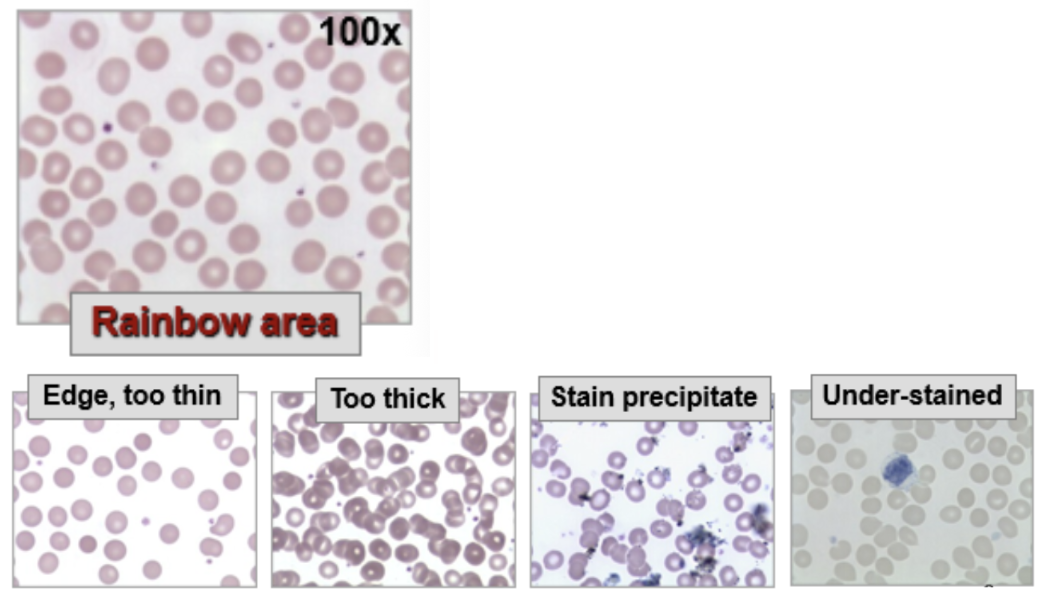
Characteristics of a properly made smear
Proper length
Proper width
Proper thickness
Presence of squared feathered edge with rainbow area
Angle of pusher and/or size of blood drop is critical and determines length and thickness
Determine actions to correct for poor smear quality (e.g., too thick) and improperly stained Wright’s stained smears
Adjust the angle of the pusher for length of smear. If it’s too short, decrease the angle of the pusher
Explain the procedure(s) for performing a WBC and platelet estimate from a Wright’s stained blood smear, including proper area, objectives used, appropriate light adjustment and sources of error.
WBC estimates are done to verify the validity of automated WBC counts
40x HPF
Count WBCs in 10 HPFs where red cells slightly overlap (2s and 3s)
Include fields with no cells in estimate; count broken cells
Take average #/HPF x 2000
Should agree with WBC count +/- 20%, the WBC estimate is never reported
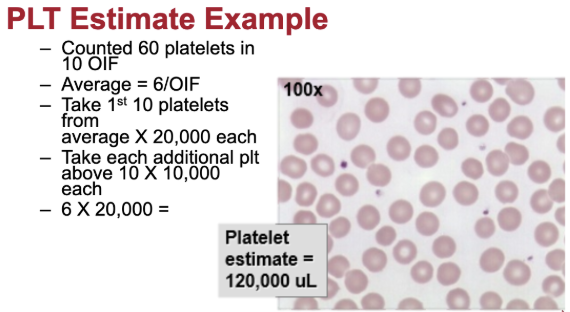
Platelet Estimates: done to verify the validity of automated PLT counts
Oil immersion and high light
Count platelets in 10 fields where red cells just touch
Include fields with no cells in estimate
Find average #/OIF
The platelet estimate is never reported
Calculate WBC and/or PLT estimates to verify the accuracy of WBC and/or PLT counts.
WBC estimate
WBC estimate average x 2000 → must be within +/- 20% of count
PLT estimate
PLT estimate average
Take first 10 of average x 20,000
Take the rest of the average x 10,000
add those values together → must be within +/- 20% if > 50,000/uL and +/- 10,000 if < 50,000/uL
Explain the procedure for performing a manual leukocyte differential, including proper area, objectives used, appropriate light adjustment and sources of error.
Manual differentials are done if significant patient abnormalities exist and/or automated differential results are flagged
Requires well-made stain/smear:
Oil immersion and high light
Rainbow are where red cells just touch, correct FOV ~150-200 RBCs
Differentials include:
WBC differential to classify WBC types
Slide is scanned from side-to-side, counting and identifying 100 consecutive WBCs = %
Usual Differential Sequence: Seg neutrophils → Band neutrophils → Lymphocytes → Monocytes → Eosinophils → Basophils
Cell Morphology/appearance
Evaluation of WBCs, RBCs, and platelets → 10 fields
Platelet estimate: done to verify the accuracy of automated platelet counts
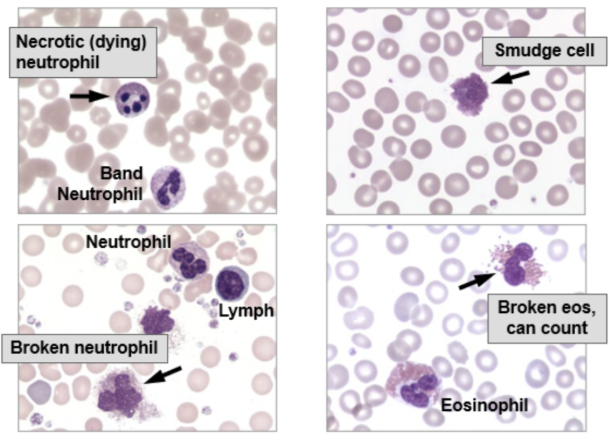
Recognize the normal differential percentage reference ranges (including age variations) of each type of leukocyte
Deviations from normal reference ranges may indicate disease → provide clues to diagnosis
No immature cells should be present
May see occasional smudge, broke, or dying cells
Critical Value: Blast Cells
Discuss manual reticulocyte counts including each of the following:
Procedure and principle of supravital stains
Sources of error
Normal reference values expressed in both relative and absolute numbers
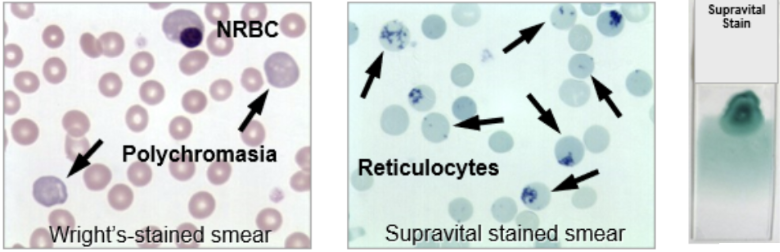
Procedure and principle of supravital stains
Principle: supravital stains are used to count retics.
Supravital “living cell” stain → NEW methylene blue
Precipitates RNA into filaments or granules
2 blue “dots” or more is a retic
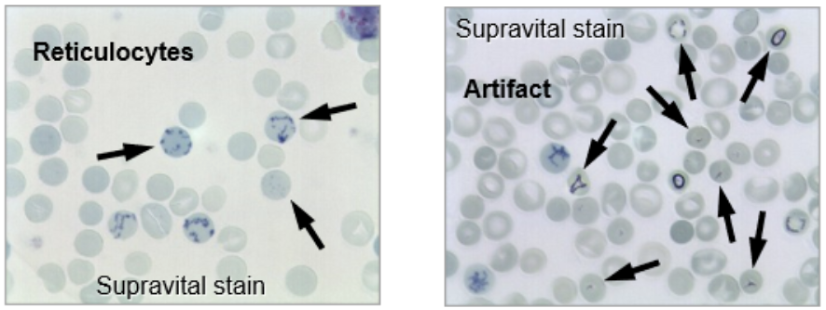
Don’t count red cells with black/shiny inclusions
Using Oil Immersion, count 500 red cells in area of slide where red cells just touch
Separate mature RBCs vs retics using 2 keys
retics/500 RBCs must agree +/- 2 retics on 2 different slides or another slide is counted
Sources of error
Absolute # is more reliable than relative %
Improper blood to stain ratio or inadequate mixing
Improper counting → counting artifact or not counting red cells with 2 “dots” as retics
Wrong calculation → especially absolute
Normal reference values expressed in both relative and absolute numbers
Adult:
0.5 - 2.0%
25-100,000/cmm Absolute #
Newborn
2.0 - 6.0%
Calculate relative and absolute retic counts, including proper reporting format.
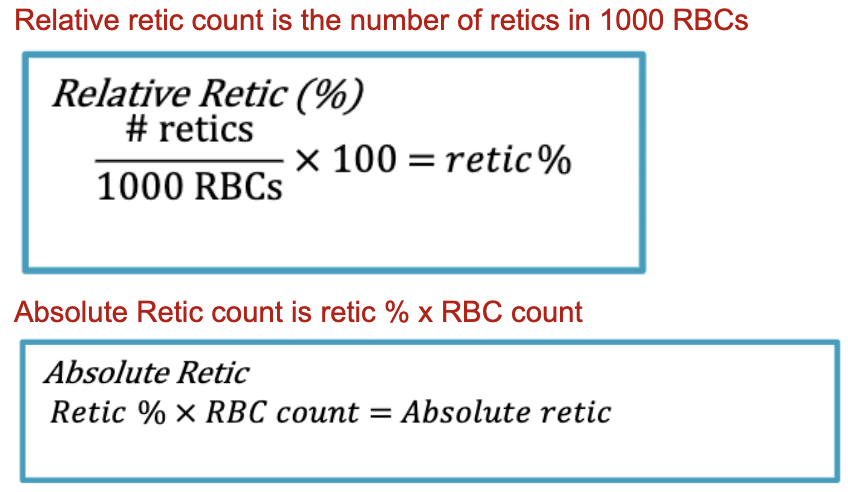
Evaluate the significance of increased or decreased reticulocytes in the blood, including causes and/or examples of conditions (e.g., hemolytic anemia, aplastic anemia, renal disease).
↑ absolute Retic count….Reticulocytosis
Increased RBC production… ↑ erythropoietin stimulation following acute blood loss or corrective therapy
Retic response is seen in about 3-5 days
Will observe increased amount of polychromasia on the Wright’s-stain blood smear
Causes: hemolytic anemias, acute or chronic blood loss, response to anemia treatment, erythroblastosis fetalis, kidney tumors/cysts
↓ absolute Retic count….Reticulocytopenia
Decreased RBC production…↓ EPO stimulation, bone marrow injury, deficiency of essential supply
Causes: Nutritional deficiencies, CKD, Bone Marrow Disorders, Anime of chronic disease, liver cirrhosis or dysfunction, medications and treatments
Causes of increased retic % can be either an increased number of retics OR, a decreased number of total red cells
Correlate retic findings with the presence or absence of polychromasia on a Wright’s stained blood smear.
On a Wright’s-stained blood smear, retics appear slightly larger than mature red cells with a grayish-blue tinge that is reported as polychromasia
The amount of polychromasia seen correlates with the # of retics in the blood
A retic count must be done to obtain a definitive number
Explain the dimensions of the Neubauer hemocytometer.
Chamber dimensions: 3mm x 3mm x 0.1mm
Identify the appropriate diluent used for performing manual cell counts.
Blood dilution is prepared using a Thrombo-tic reagent vial and capillary pipet
Vial contains 1% ammonium oxalate (diluent)
1:100 dilution (x100)
RBCs will lyse leaving WBC and platelets
Fill entire counting area under coverslip on each side of hemocytometer.
Correct magnification and light adjustment for manual cell counts
40x objective and low light, count cells in all 9 squares on each side of hemocytometer = 18 mm^2
Cells counted on each side must agree +/- 20%

Manual cell count appearance of cells
platelets appear greenish, not shiny
Manual cell count sources of error
Pre-analytic/blood collection errors, e.g., clotted blood
Analytic/technical errors
Poor diluting or plating technique
Calculation error…is the result believable??
Counting wrong area, using wrong light, or counting junk as cells
High WBC count may make counting difficult-secondary dilution?
Important that chamber is well cleaned (if using glass)
Focusing problems for manual cell count
Clean lens
Adjust condenser → open condenser
Adjust light intensity → decrease light intensity
Clean eyepiece
Start over
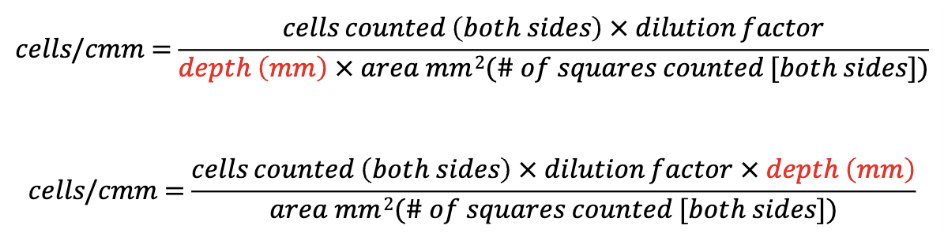
Manual cell count formula
Area (squares) to count and/or blood dilution to make is determined by cell number
Formula to obtain #cell/cm or #cells/uL
Describe instances when manual methods of cell counting might be used
Automated cell count is flagged as doubtful
Estimate from blood smear doesn’t agree w/ result
Describe the theory of the Coulter electronic impedance principle of cell counting and sizing.
The Coulter Principle (electrical impedance method) is the most widely used method for automated counting and sizing of blood cells in hematology analyzers.
The principle is based on:
Blood cells are poor conductors of electricity.
The diluent surrounding the cells is a good electrical conductor.
When a cell passes through a small aperture (opening) between two electrodes carrying an electric current, it temporarily displaces an equivalent volume of conductive diluent.
This causes a brief increase in electrical resistance (impedance) and a corresponding decrease in current flow.
Cell Counting
Each pulse generated = one cell counted.
The number of pulses produced is proportional to the number of cells passing through the aperture.
Therefore, the analyzer determines the cell count by counting the pulses.
Cell Sizing
The height (amplitude) of the pulse is proportional to the volume of the cell.
Larger cells produce larger pulses.
Smaller cells produce smaller pulses