WCF: Week Three- Labor & Birth Process; Pain Management in Labor-EXAM ONE
1/97
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
98 Terms
what are the 5 p's of labor and delivery?
-passenger (baby), passageway (maternal pelvis), powers (physiological forces), position (of the baby), and psychological response of the pregnant patient
what is the largest part of a baby's head?
-the parietal bone
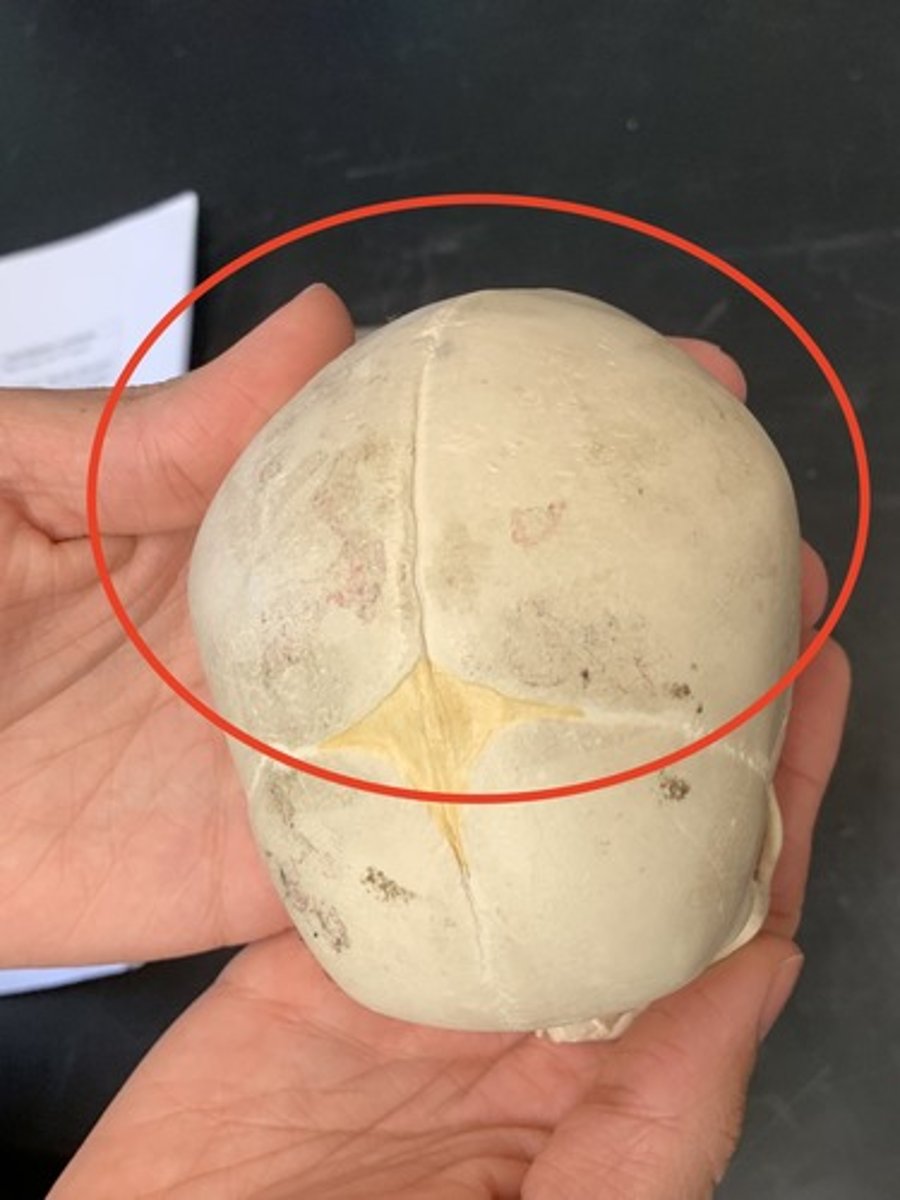
what is the landmark we use to determine birthing positioning of the head of a baby?
-the occipital bone
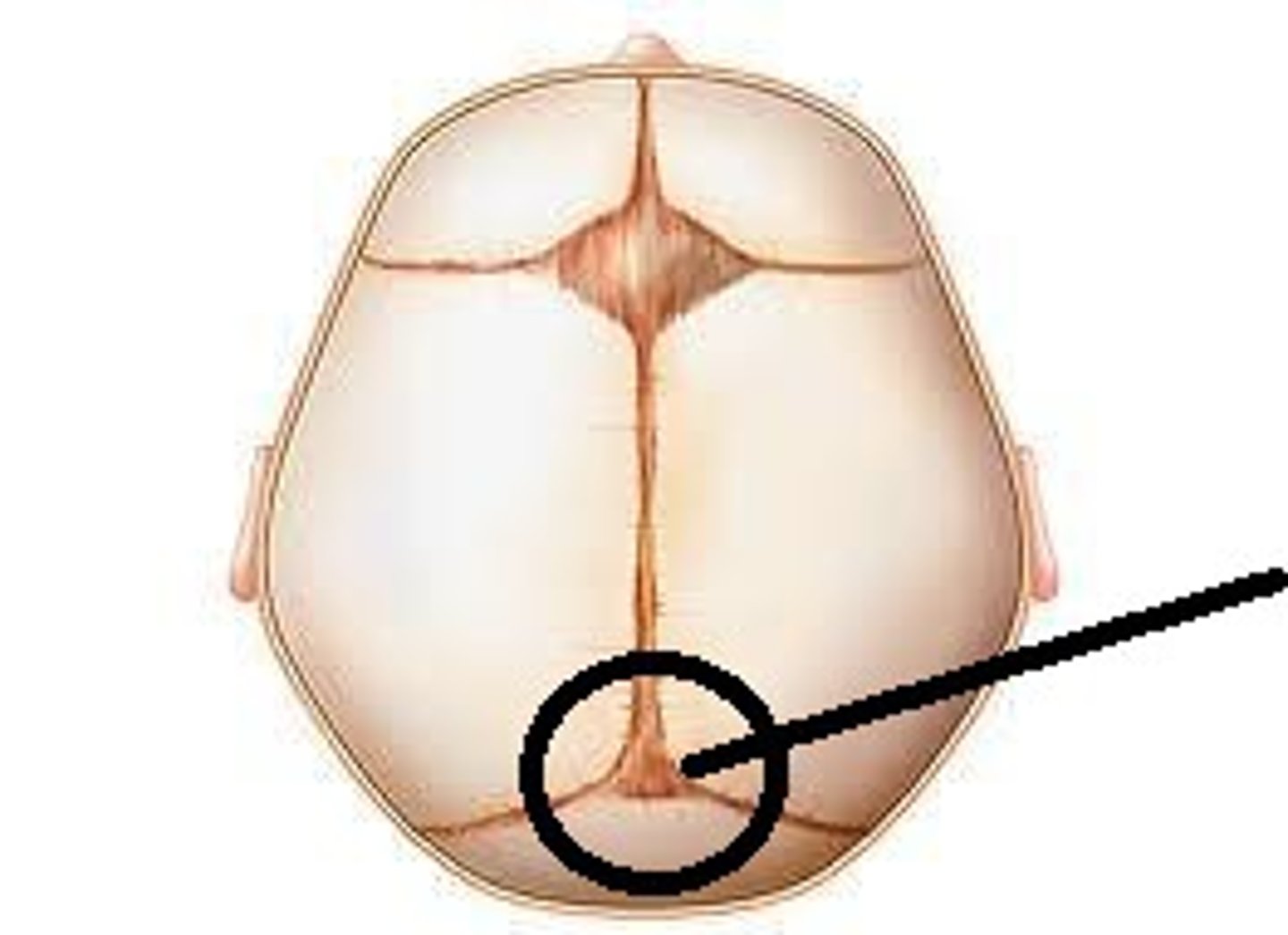
when does the anterior fontanelle close?
18 months to 2 years of age
when does the posterior fontanelle close?
2 months of age
what is molding in a newborn baby?
-the temporary shaping of the baby's head during labor and birth
-bones of a baby's skull are not fully fused, which allows them to overlap slightly as the baby passes through the birth canal

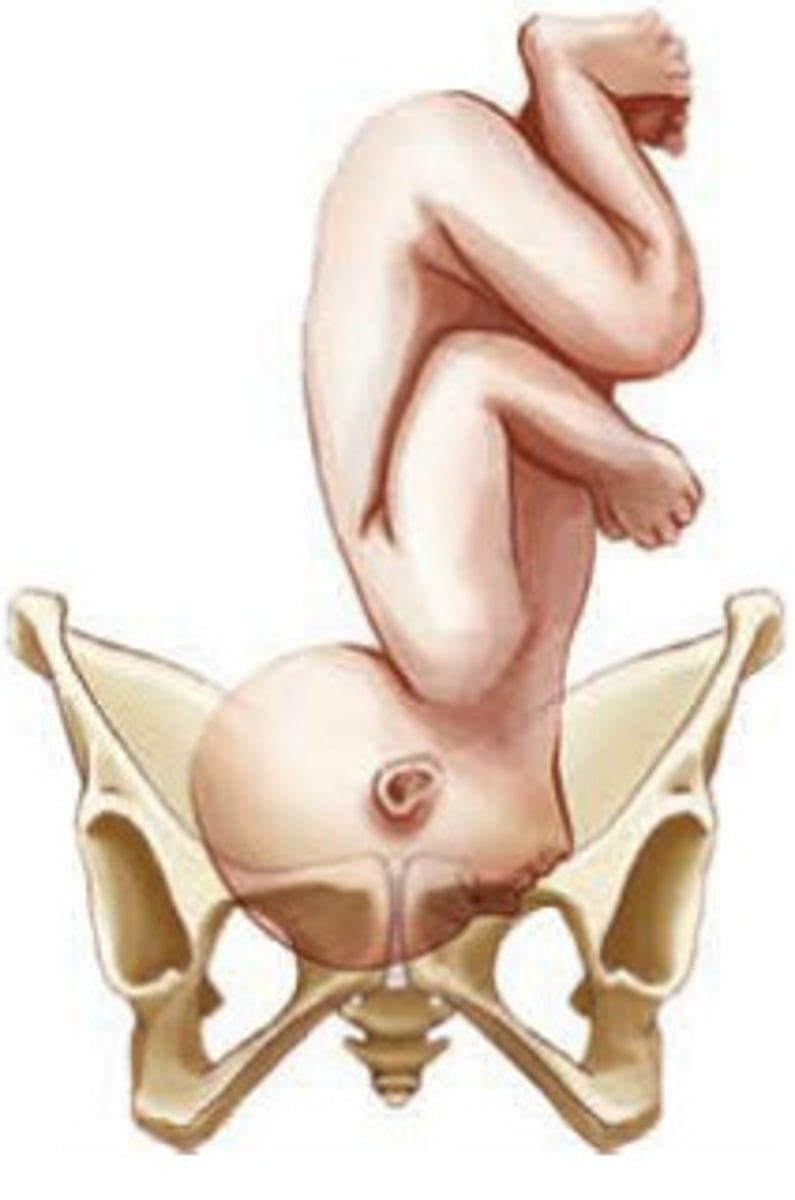
what is fetal presentation?
-part of the fetus that enters the pelvis first aka what is coming out first?
what is vertex birth?
-they are born head first
-what we want!!

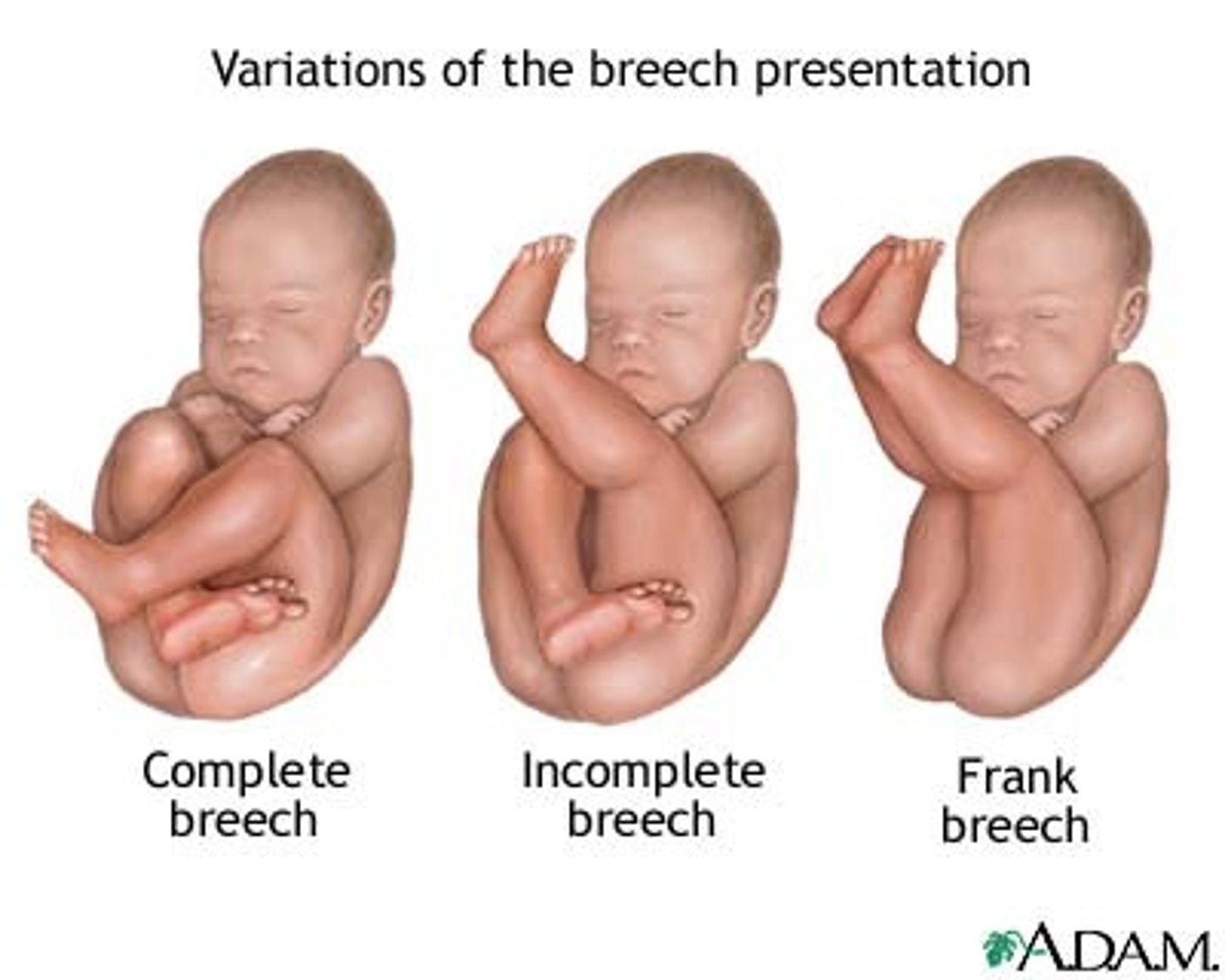
what is breech birth?
-when baby is set to come out head or buttocks first
what is a shoulder birth?
-the baby's head is delivered but one or both shoulders become stuck behind the mother's pelvic bone, preventing the rest of the body from being born easily
what is fetal attitude?
-the relationship of the fetal parts to one another.
-the fetal attitude can be flexion or extension.
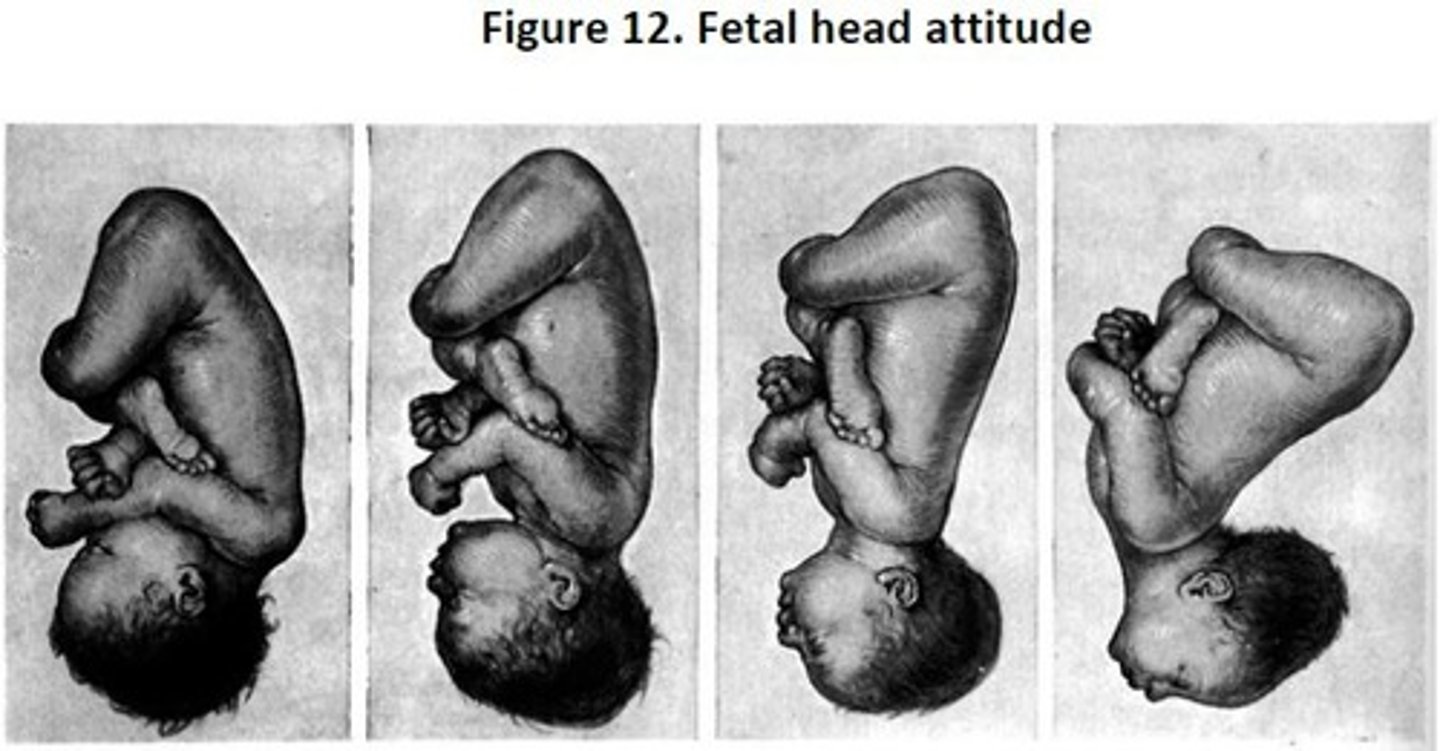
what is a good fetal attitude?
chin to chest
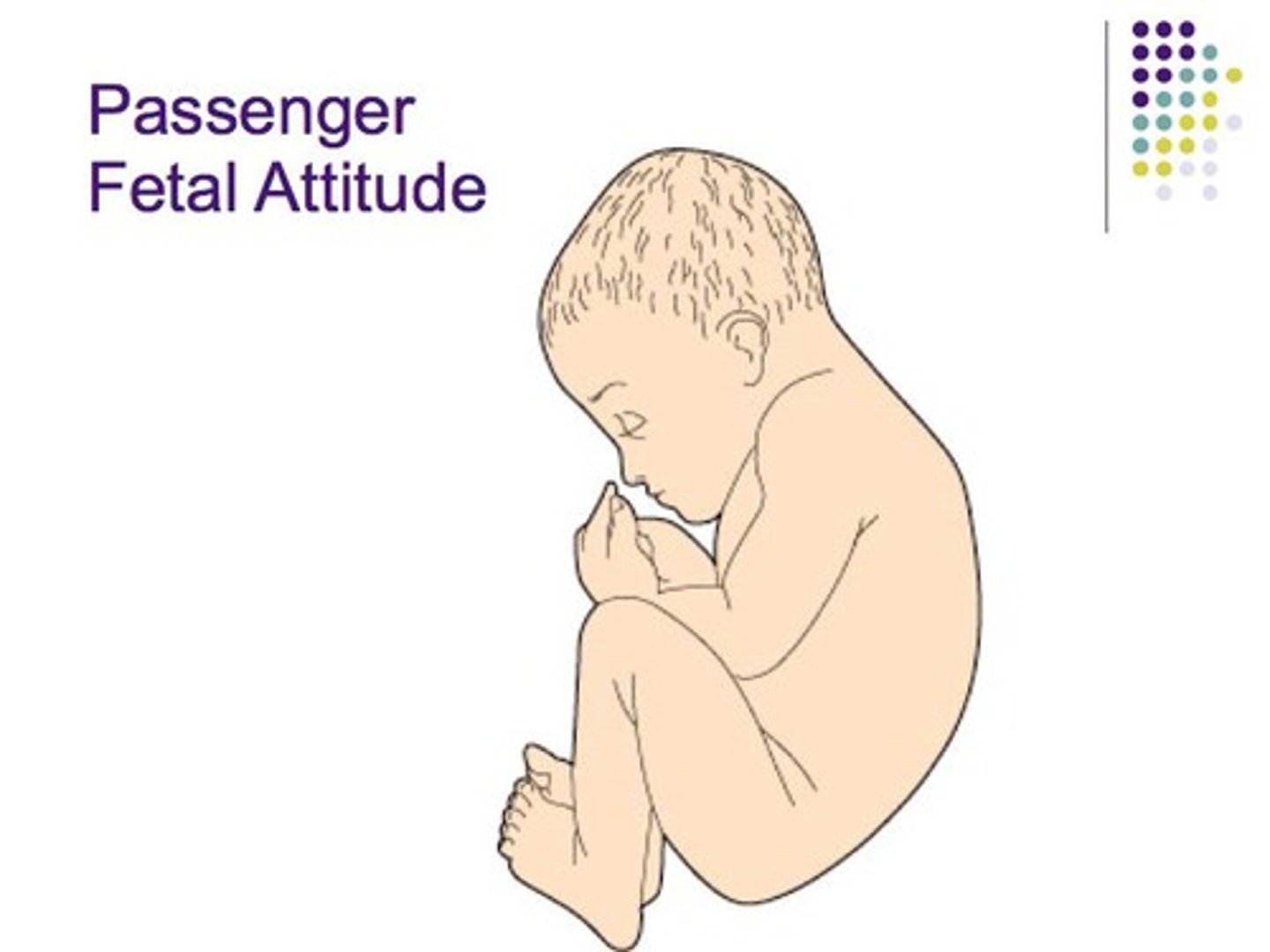
what is a bad fetal attitude?
chin extended
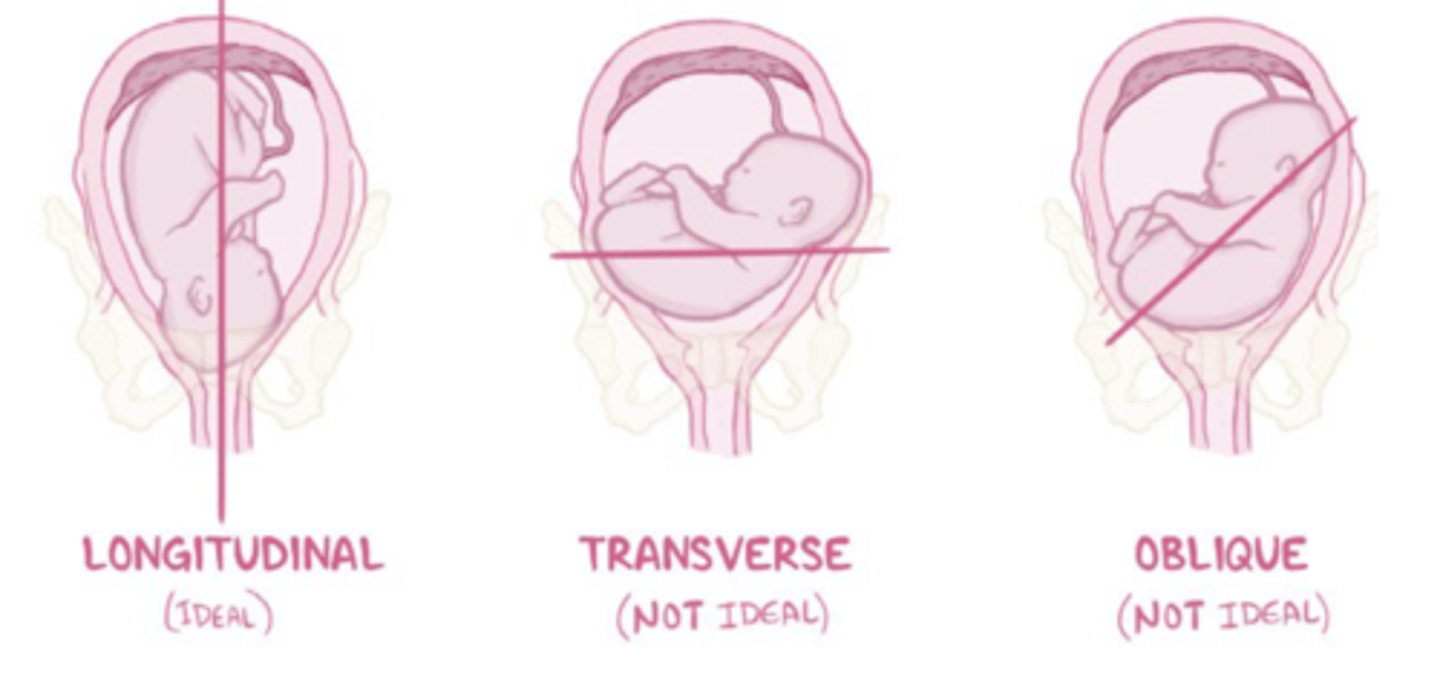
what is fetal lie?
-the relationship of the spine of the mother to the spine of the fetus.
-are the spines aligned?
-transverse is very rare!
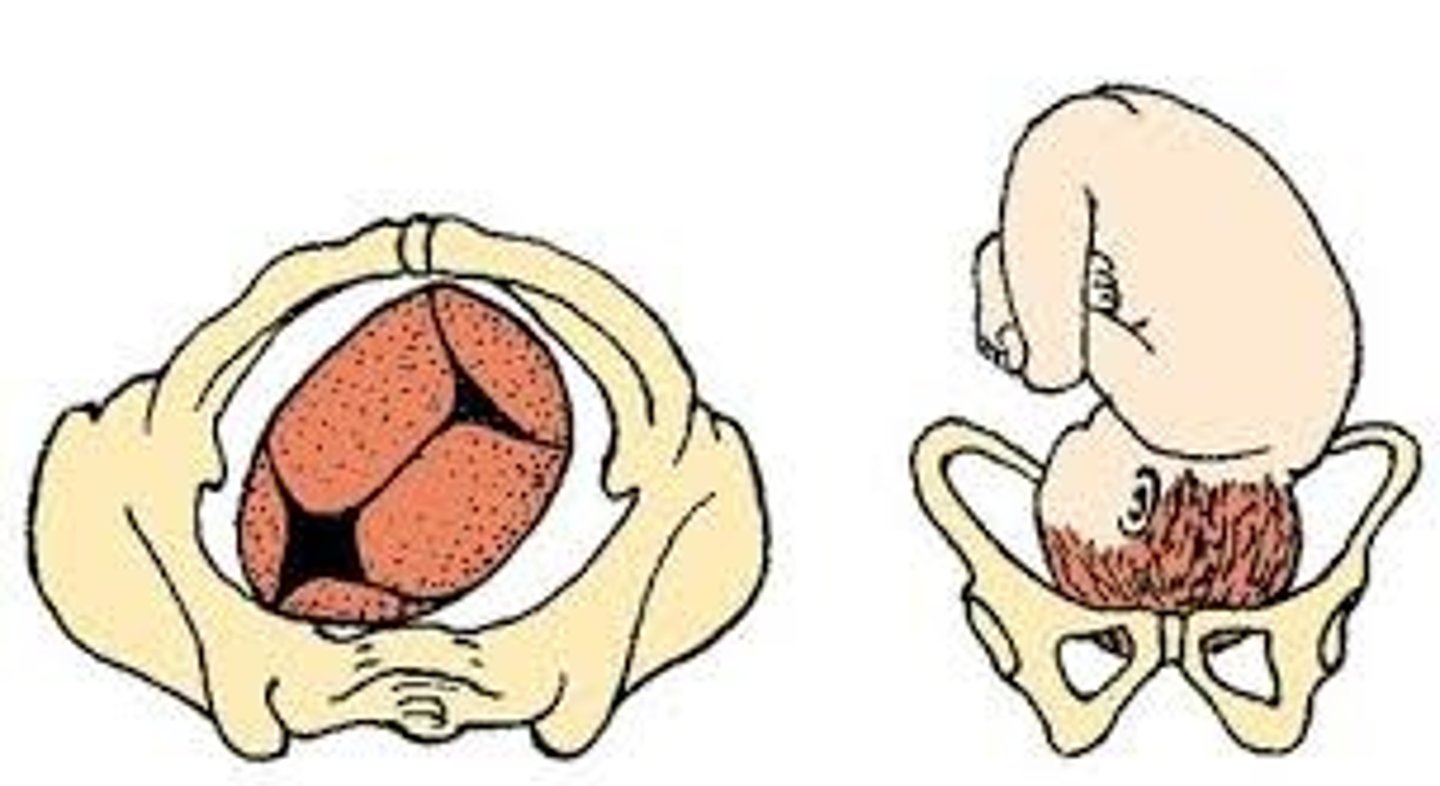
what is occiput fetal position?
-the best position
-back of the baby's head faces the front of the mother's pelvis.
-position is associated with the easiest vaginal deliveries
how do we determine fetal position?
-with 3 letter designation (ex: ROA, LOP, RSA, LMP)
-R/L= right or left side of the pregnant patient that the baby's body part is leaning toward
-O/M/S/A= baby's body part entering the pelvis
-A/P/T= side of the pelvis the baby's body part is closest to. can be anterior, posterior, or transverse
what is powers in the 5 p's of labor and delivery?
-contractions
-frequency aka how often
-duration aka how long?
-intensity aka how strong?
what is the active segment of the uterus?
-the top of the fundus that contracts during delivery and brings the baby down
-the passive segment simply stretches out and expands that is the difference!
what are factors to assess in pregnant patients prior to labor and delivery?
-emotional readiness for labor and delivery
-level of educational prep for l/d
-prior birth traumas
-support group surrounding the mom
*it is VERY important for the mom to be as relaxed and calm as possible because anxiety and fear intensify pain and can slow the birthing process
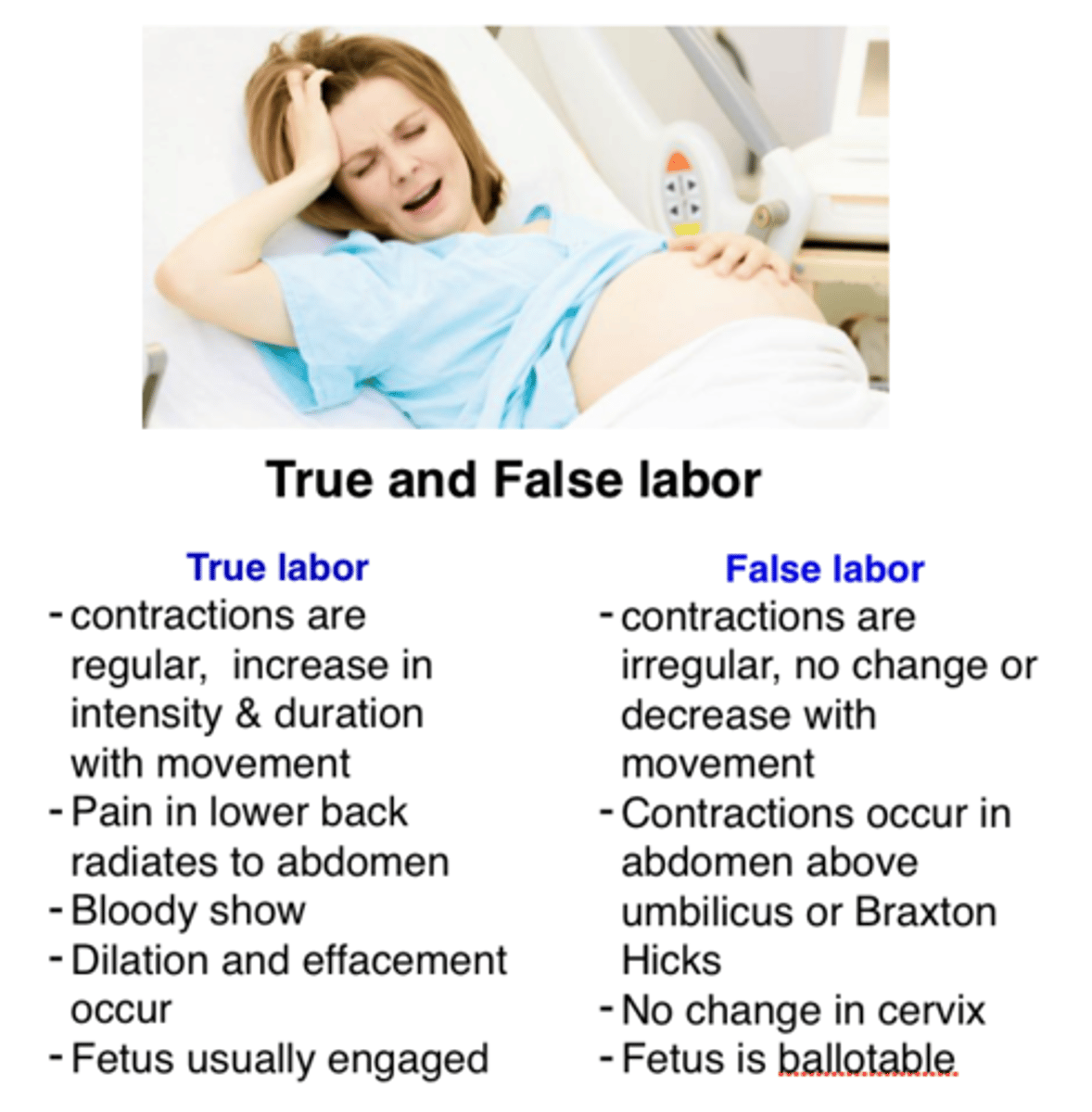
what is false (latent) labor? **
-NO CERVICAL CHANGE from previous dilation/effacement
-contractions do not intensify and may space out
-can walk/talk through contractions and walking does not make them stronger
-pain medications may stop (most likely feeling braxton hicks contractions)
what are braxton hicks contractions?
-they are preterm or false labor contractions.
what is true labor? **
-CERVICAL CHANGES
-contractions get longer, stronger, and closer together, walking can make them stronger
- "5-1-1" occurring every 5 min, lasting 1 min, happening for 1 hr
-pain meds may speed or slow up labor but NEVER stop it
what are signs of impending labor?
- lightening or engagement; fetus drops into true pelvis
-irregular contractions (braxton hicks)
- bloody show
- urinary frequency
- energy spurt "nesting" (1-2 days prior)
-loss of mucus plug
-pelvic pressure
what is bloody show in signs of impending labor?
-a pink, brown, or blood-tinged mucus discharge that occurs when the mucus plug in the cervix is released as the cervix begins to dilate and efface in preparation for labor
how does the cardiovascular system respond to labor?
-during contractions, blood from uterus to vascular system
-blood volume redirected to periphery = increased BP
how does the respiratory system respond to labor?
-hyperventilation
-O2 consumption is increased 2nd stage of labor
how does the GI system respond to labor?
-digestion slows/stops in labor
what is a normal fetal heart rate?
-110-160 bpm (altered by movement and descent)
what are hemodynamic fetal response changes to labor?
-affected by BP
-healthy baby has reserves for anoxic episodes
what admission labs do we want to collect during the nursing assessment of a pregnant patient?
-U/A (condition dependent like UTI)
-CBC (focus on H&H and platelets monitoring for post labor hemorrhage or for epidural)
-RPR
-type & screen (in case of transfusion)
what is leopold's maneuver?
-series of four abdominal palpation techniques used during pregnancy to determine the fetus's position, presentation, and engagement in the pelvis
-also determine PMI (point of maximum intensity)
what are contraction strength levels?
-mild = slightly tense, press tip of finger to nose
-moderate = firm, like pressing finger to chin
-strong = rigid, like pressing finger to forehead
*placing your fingertips on the uterine fundus (the top portion of the uterus)
what are the components of a vaginal exam for a pregnant woman?
-dilation
-effacement
-fetal station/descent
-amniotic membranes/fluid
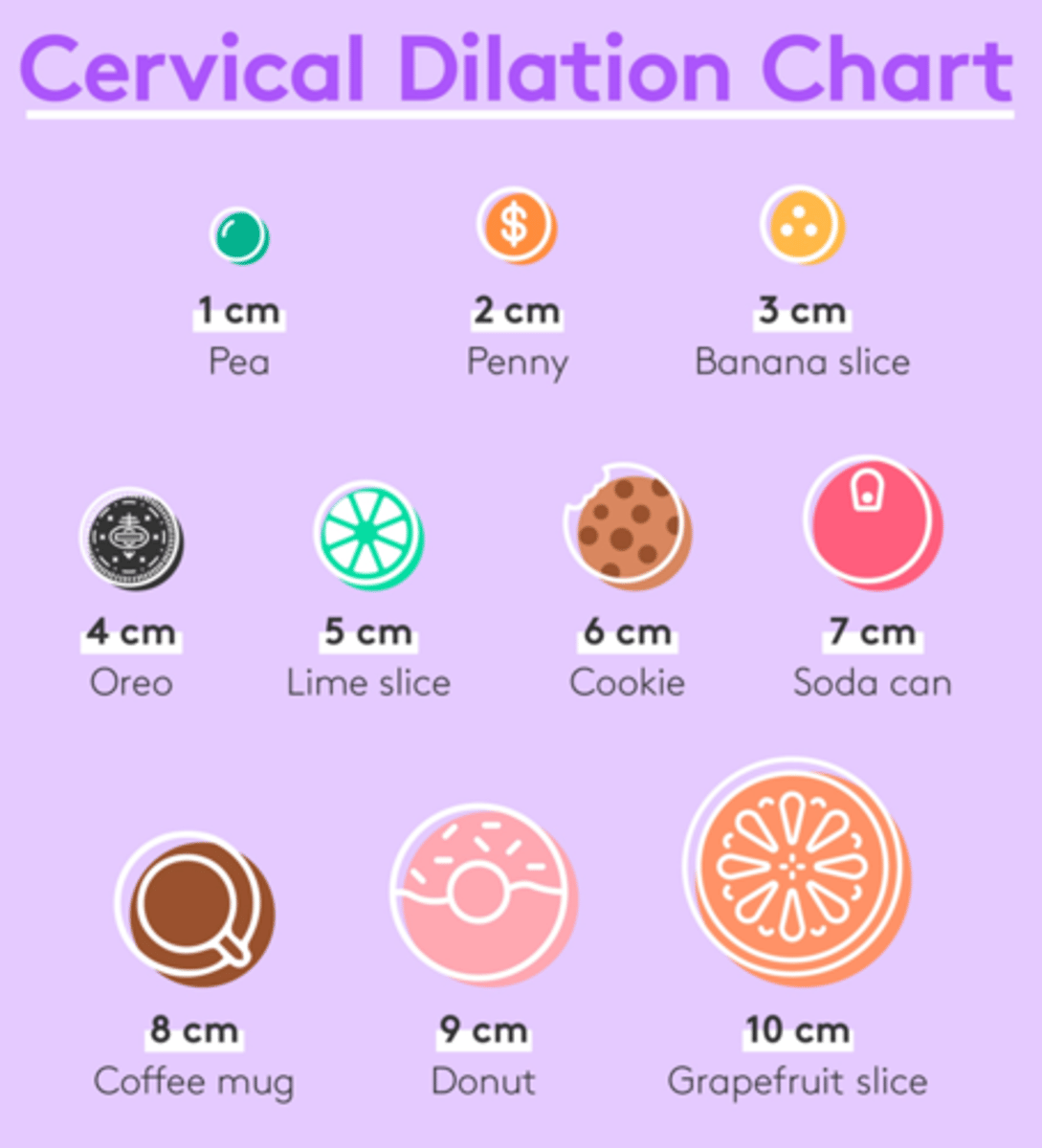
what is cervical dilation?
-opening of the cervix from 0-10 cm
-diameter across opening
what is cervical effacement?
-thinning and shortening of the cervix
-0-100%
-percentage of shortening
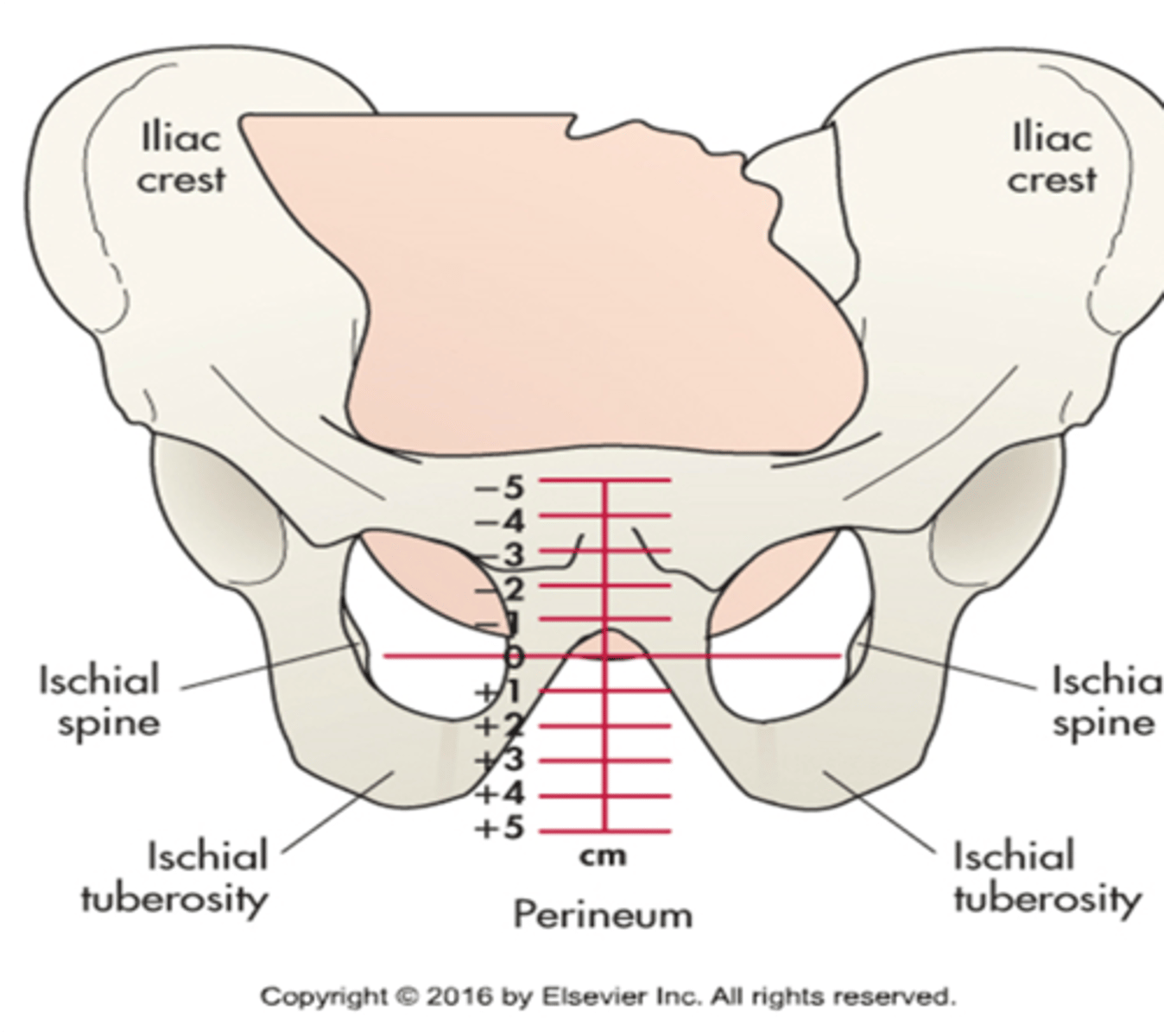
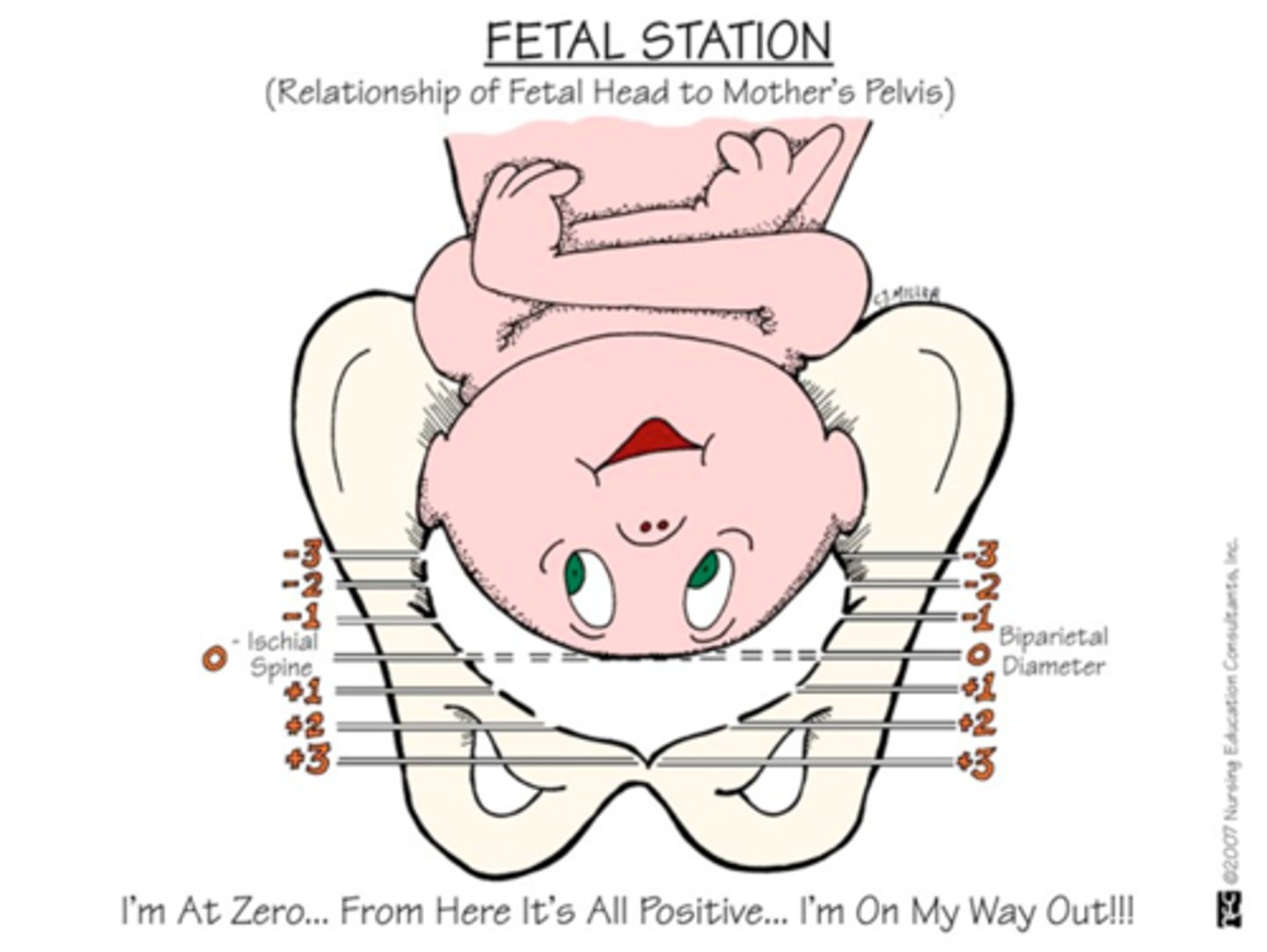
what is pelvic station?
-in relation to the ischial spines
-goes from -5 to +5
what is an example of a cervical exam?
3/90/-1
-meaning the patient is 3 cm dilated, 90% effaced, and -1 station position
at what cervical exam is a woman ready to give birth?
-10/100 they must be here!!!
what is fetal station?
a measure of the degree of descent of the presenting part of the fetus through the birth canal
what are normal findings for amniotic fluid?
-pale, straw, flecks, or lanugo or vernix
-no odor and is watery (if there is an odor it could meconium present)
-800 mL for 24 weeks, 1000 mL for 32-36 weeks, and 700-800 mL for 37+ weeks
what are tests to diagnose or confirm rupture of membranes aka determining if it is just pee or if it is amniotic fluid?
-amnisure if it turns blue the BABY IS COMING if it is yellow it is just pee
-FERN testing of amniotic fluid under the microscope
-amniotic fluid index using an ultrasound
what is pre-labor (false labor)?
-episodes of uterine contractions that ripen the cervix (may be intermittent for 3-4 weeks)
what is the 1st stage of labor?
-begins at the onset of true labor and ends with cervical dilation of 10 cm
-0-10 cm
what are the 3 phases within the first stage of labor?
-phase one-latent= 0-3 cm with mild to moderate contractions
-phase two-active= 4-7 cm with moderate to strong contractions
-phase three-transition= 8-10 cm with strong painful contractions
what are nursing interventions within the first stage of labor?
-palpate contractions every 30 minutes and every 15 minutes in transition
-EFM monitoring can be either intermittent if low risk or continuous if high risk with possibility of internal monitoring
-assess temperature especially after water has ruptured d/t higher risk of infection (x2 hrs)
-if patient has epidural they will most likely need a catheter
do we want a pregnant patient to push early?
-NO! unless we are at 10 cm because we do not want to tear the cervix and decrease fatigue
what is the 2nd stage of labor?
-begins with complete/full dilation (10cm)
-aka the "pushing stage" and ends with delivery of baby
-duration may vary between primiparas and multiparas
what are nursing interventions within the second stage of labor?
-PRIORITY is to take out the foley catheter if the patient had an epidural
-continuous and intermittent fetal monitoring
-this stage is all about getting the mom ready to push out the baby
what anatomical alterations do we see in the second stage of labor?
-bulging of perineum and rectum
-flattening and thinning of perineum
-increased bloody show
-labia begin to separate with burning sensation
-intense pressure in rectum
-crowning
what kind of lacerations do we see in the second stage of labor?
-perineal lacerations
-vaginal and urethral lacerations
-cervical lacerations
what are the different degrees in perineal lacerations?
-first degree: skin and structures superficial to muscles
-second degree: through muscles of perineal body
-third degree: through anal sphincter muscle
-fourth degree: anterior through rectal wall
what is an episiotomy?
-a surgical cut made at the opening of the vagina during childbirth
-to aid a difficult delivery and prevent rupture of tissues
-median "midline" or mediolateral
what is the 3rd stage of labor?
-begins with the birth of the baby and ends with the delivery of the placenta
-SHOULD NOT BE ANY MORE THAN 30 MINUTES if so we are at higher risk for hemorrhage
what are the signs that the placenta is ready to deliver?
-lengthening of the cord
-gush of dark red blood (which appears after separation)
-globular shape of abdomen
-patient says, "i have to push again"
how can the provider expedite placenta delivery if reaching the 30 min mark?
-provider may massage fundus to expedite placenta detachment
-after placenta delivery, provider will inspect placenta to make sure it's intact
what are nursing interventions within the third stage of delivery?
-APGAR on infant at 1 min then 5 min then 10min if score was weird earlier
-watch for signs of placental separation as this should occur within 30 min
-skin on skin contact with mom and baby
-get lidocaine/sutures if episiotomy or laceration present
-administer pitocin IV or IM for hemorrhage
what kind of information do we want to document in the third stage of labor?
-EBL: (estimated blood loss)
-intact perineum (or type of laceration or epiostomy)
-all delivery stats
what is the 4th stage of labor?
-recovery and may last up to 4 hours or more
-physiologic readjustment begins
-critical assessments by RN are done
-fundal assessment is crucial!!
what are the 3 sources of labor pain?
-emotional: fear and tension
-functional: dilation and contractions
-physiologic: maternal and fetal contractions
is labor pain normal?
-YES! it is purposeful, anticipated, intermittent and most importantly NORMAL
what is visceral pain?
-pain related to internal organs
-related to changes in cervix, uterine ischemia during contractions

what is referred pain?
-pain felt in one part of body is caused by pain in another part
-pain originates in uterus, but client might feel in abdominal wall, lower back, hips, buttocks, thighs
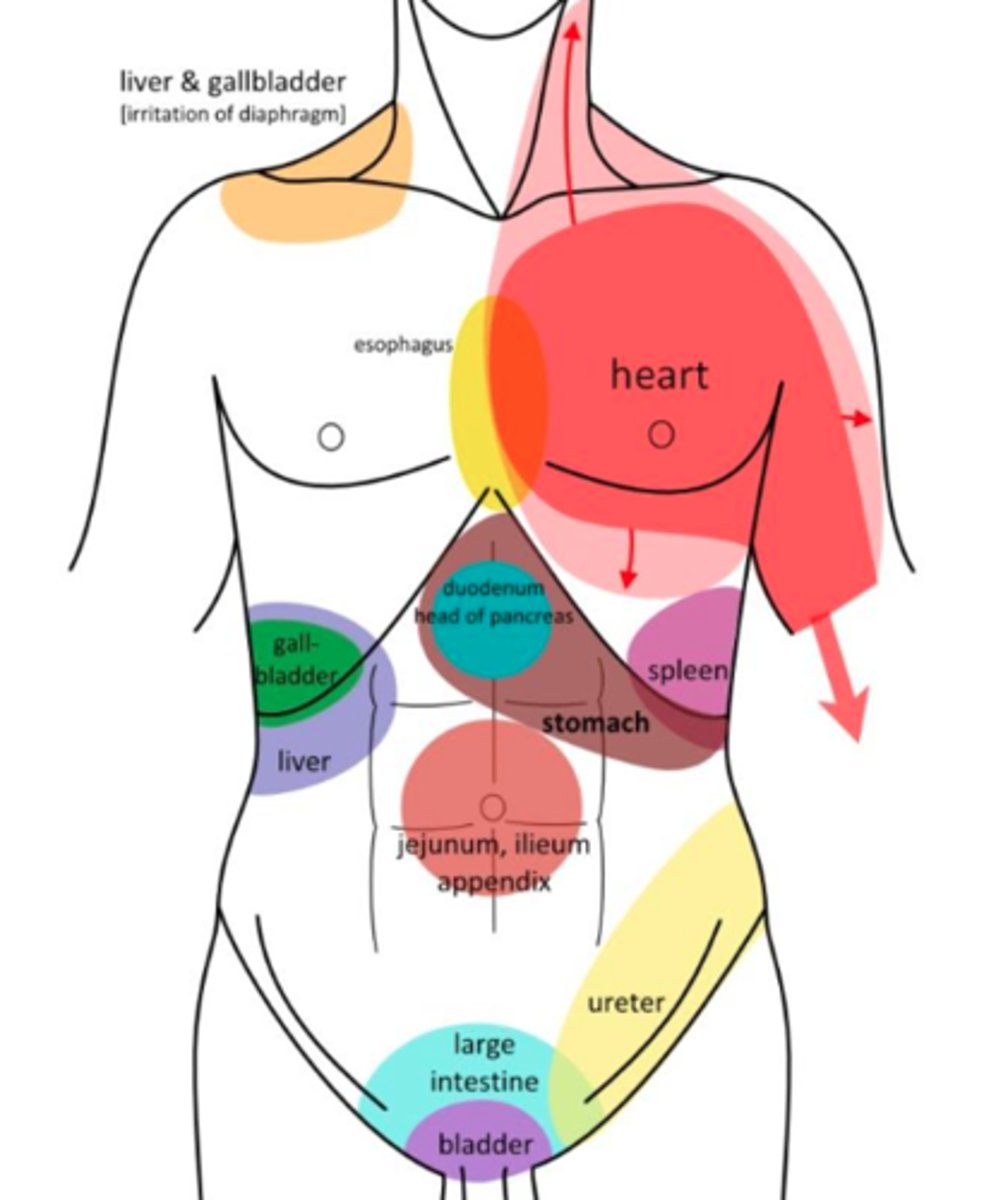
what is somatic pain?
-localized pain from muscles, bones, or soft tissues
-stretching of perineum during second stage, soft tissue lacerations, fetal pressure on structures
-mostly seen in the SECOND stage

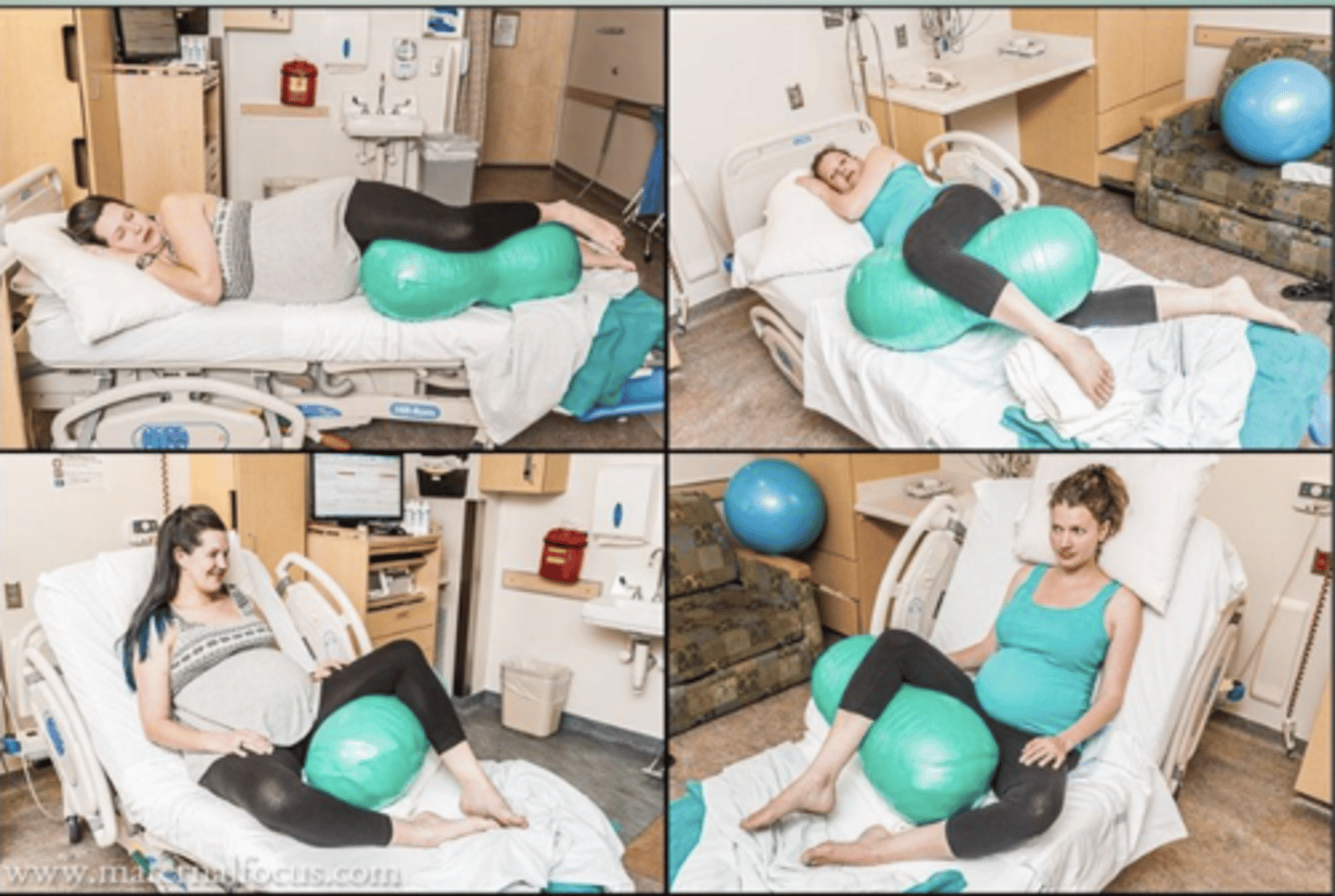
what are non-pharmalogical pain relief methods for pregnant women?
-hydrotherapy (whirlpools and showers help with endorphin levels and distraction)
-birthing balls or peanut balls
-a cub which is a cushion used in labor and delivery
-paced breathing and relaxation
-music and guided meditation
-aromatherapy
-yoga or acupressure or effleurage
what is the difference between analgesia and anesthesia?
-analgesia = pain relief without loss of sensation or consciousness.
example: an epidural during labor can provide analgesia so the patient feels less pain but is still awake and aware.
-anesthesia = loss of sensation, and sometimes loss of consciousness.
example: a spinal block for a C-section causes anesthesia below the waist, and general anesthesia causes unconsciousness
what is parental analgesia?
pain medication given by injection, usually through the intravenous (IV) or intramuscular (IM) route, to relieve pain during labor.
what are opioid agonists given as parental analgesia during labor?
-butorphanol IV/IM
-meperidine hydrochloride IV/IM
-hydromorphone hydrochloride IV/IM
-nalbuphine IV/IM
*given intermittently to reduce the awareness of pain
what do we always need nearby when giving an opioid agonist to a pregnant patient?
-naloxone aka narcan aka an opioid antagonist
what are the advantages to to parental analgesia?
-dose can be titrated
-pain relief begins in minutes
-no loss of consciousness
-increased relaxation
-decreased pain
-RN can administer aka no waiting for anesthesia team!
what are the maternal response disadvantages of parental analgesia?
-may not relieve pain
-nausea/vomiting
-drowsiness
-confined to bed
-continuous EFM
what are the fetal response disadvantages of parental analgesia?
-CNS depression
-decreased FHR variability
-respiratory depression
-decreased reflexes (suckling)
-can impair early breastfeeding
-decreased ability to regulate temperature
what is nitrous oxide for pain management in labor and delivery?
-colorless, odorless gas that is mixed 50/50 (nitrous oxide/oxygen) for laboring persons
-when breathed in, it reduces anxiety and increases feelings of relaxation and well-being
-inhaled through a mask or mouthpiece
-can utilize at any stage of labor and delivery

what are the advantages to nitrous oxide?
-does not impair patient mobility
-no additional monitoring required
-self-administration provides patient with control
-medication effects stopped as soon as the mask or mouthpiece is removed
what are the disadvantages of nitrous oxide?
-nausea and vomiting
-dizziness
-drowsiness
what are the safety concerns of nitrous oxide?
-risk of respiratory depression when combined with opioids
-may increase likelihood of maternal hypoxemic episodes
-rapidly crosses the placenta
-rapidly eliminated by the neonate upon commencement of breathing
what is local anesthesia in pain managment?
-lidocaine for episiotomy/laceration and repair
what is regional anesthesia in pain managment?
-can be pudendal, epidural, or spinal
what is pudendal regional anesthesia?
-local anesthesia to perineum, vulva, and rectal areas during delivery, episiotomy, and episiotomy repair
-administered transvaginally into space in front of pudendal nerve
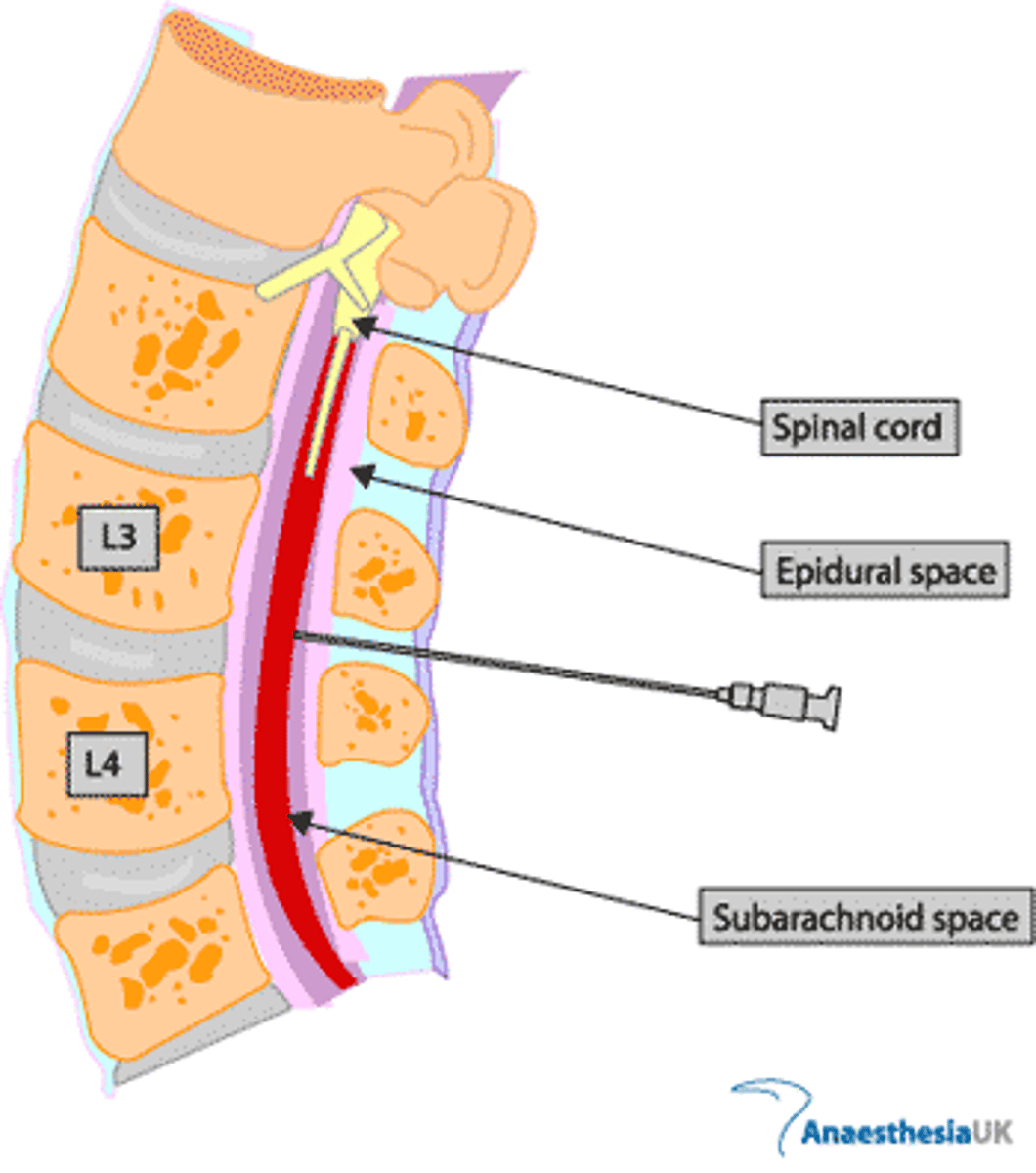
what is epidural regional anesthesia?
-bupivacaine/fentanyl on PCA pump which is an analgesia & anesthesia
-spinal anesthetic agent is administered into the CSF in the subarachnoid space
-the epidural space is located between the dura mater and the ligamentum flavum
what is spinal regional anesthesia?
-intrathecal opioid like duramorph
-spinal anesthetic agent is administered into the CSF in the subarachnoid space
what is general anesthesia?
-loss of consciousness we DO NOT like using this in labor! lots of complications
-typically used as stat cesarean or other emergencies
-usually used when regional is contraindicated
what is nursing care prior to epidural administration?
*epidural=HYPOTENSION!
-educate, consent, and safety check
-prepare the patient with positioning and monitoring must have continuous fetal monitoring
-report any HTN, bleeding disorder, or systemic infection
-administer fluid bolus to stabilize BP
what is nursing care during/after epidural administration?
-BP every 5 minutes or per protocol
-review labor progress, FHR & CTX patterns
-keep bladder empty make sure to insert foley
-position for pain and passenger aka do NOT leave supine for an extended period of time we want to continue to reposition
what are potential structural contraindications for epidurals?
-previous spinal injury/surgery
-severe scoliosis
-BMI of 50+ space-occupying brain lesion (ICP)
-local or systemic infection
what are potential hematological contraindications for epidurals?
-thrombocytopenia aka LESS THAN 150,000
-coagulation disorders like von willebrand disease!
-actual or anticipated maternal hemorrhage
what is von willebrand disease?
-an inherited bleeding disorder caused by a deficiency or dysfunction of von Willebrand factor (vWF), a protein that helps platelets stick together and helps stabilize clotting factor VIII
is an epidural sterile?
YES
what are the advantages of epidural anesthesia?
-continuous and indefinite pain relief, relaxation
-excellent coverage in labor
-titratable in relation to stage of labor and patient can administer bolus
-patient remains alert and participate in birth
-no blood loss
-no delay in gastric emptying
-respiratory reflexes remain intact
-fetal complications rare
what are the most serious disadvantages of epidurals?
-BIG RISK of hypotension
-leads to fetal bradycardia
-maternal cardiac arrest
what are some general disadvantages of epidurals?
-may interfere with pushing and fetal descent
-may result in longer labor or C/S (recent studies report it can help progress labor)
-possible post-dural puncture headaches
-can't ambulate as early (client must regain sensation and be able to control legs, several hours)
what is post-dural puncture headaches?
-a headache that can occur after an epidural or spinal anesthesia if the dura is accidentally punctured and cerebrospinal fluid (CSF) leaks out
-SEVERE EXCRUCIATING PAIN
-treatment is epidural blood patch (the patient's own blood is injected into the epidural space to seal the leak)
what are nursing actions to treat hypotension due to epidural?
-turn them to their LEFT side THIS IS THE 1ST THING WE DO!!
-make sure to elevate legs
-bolus of IV fluids
-oxygen by face mask
*after all this is done THEN we contact the provider
what are spinal blocks for C/S (c-section)?
-anesthetic into CSF
-various dermatomes with red Block for vaginal and blue block for C/S
-this is a RAPID onset and lasts around 2 hours prep the patient with fluids
-high risk for spinal headaches and tx is blood patch
epidural vs spinal space
image
what is general anesthesia in labor and delivery?
-this is usually given unplanned and for emergency C/S
what are the complications associated with general anesthesia?
-fetal depression
-anesthetic agents reach fetus in minutes and need to deliver immediately
-not advised for high-risk fetus (preterm)
-greater blood loss due to uterine relaxation
-aspiration- increased chance of emesis
what are nursing interventions for general anesthesia?
-give antacid pre-op
-wedge under right hip for L lateral tilit
-pre-oxygenate 3-5 minutes of 100%
-IV fluid bolus
-cricoid pressure during ET tube placement
slide 47 in pain managment pp