Hematology Unit 2 Exam
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
WBC and PLT estimates
WBC estimate average x 2000 → must be within ± 20% of count
PLT estimate average x 20,000 → must be within ± 20% if > 50,000/uL and ± 10,000 if < 50,000/uL
Normal and abnormal RBC morphology
Normal = normocytic, normochromic
Abnormal = anything that’s not that
Define total blood volume, including RBC mass and plasma volume
Total blood volume (TBV) is the combined volume of all blood circulating in the cardiovascular system at a given moment. It has two main components:
Total Blood Volume = Red Blood Cell (RBC) Mass + Plasma Volume
RBC Mass (Red Cell Volume) The total volume occupied by erythrocytes in the circulation. It reflects the body's oxygen-carrying capacity.
Plasma Volume The liquid portion of blood — water, proteins (albumin, globulins, fibrinogen), electrolytes, hormones, and nutrients — excluding cells.
Define the term anemia
Decrease in RBC count, HGB and/or HCT values
Blood unable to supply proper oxygenation to tissues: hypoxia
Discuss the hematologic (e.g., signs of erythropoiesis) and physiologic (e.g., clinical symptoms) responses to anemia
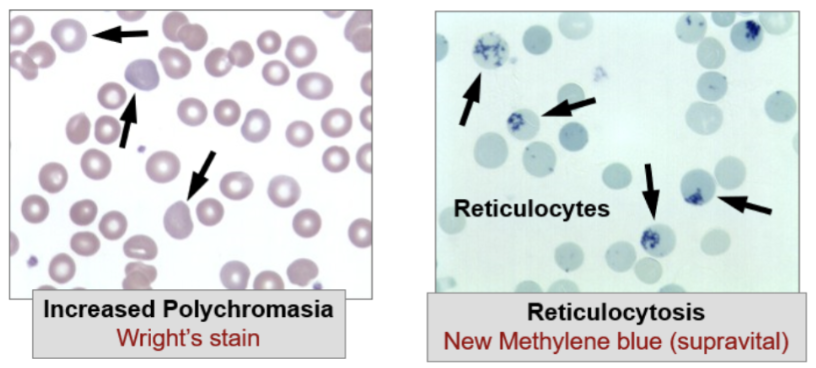
Signs of accelerated erythropoiesis:
Tissue hypoxia causes increased renal release of erythropoietin to accelerate bone marrow erythropoiesis
Bone marrow can increase its activity 7-8x normal
Bone marrow becomes hyper-cellular due to increase in RBC precursors
Nucleated RBCs may be released into the blood along with reticulocytes
NRBC# correlated with severity
Increased # retics = increased amount of polychromasia
If demand exceeds what the bone marrow can provide, production can occur in extramedullary sites
Liver and/or spleen
Causes hepatosplenomegaly… spleen enlargement
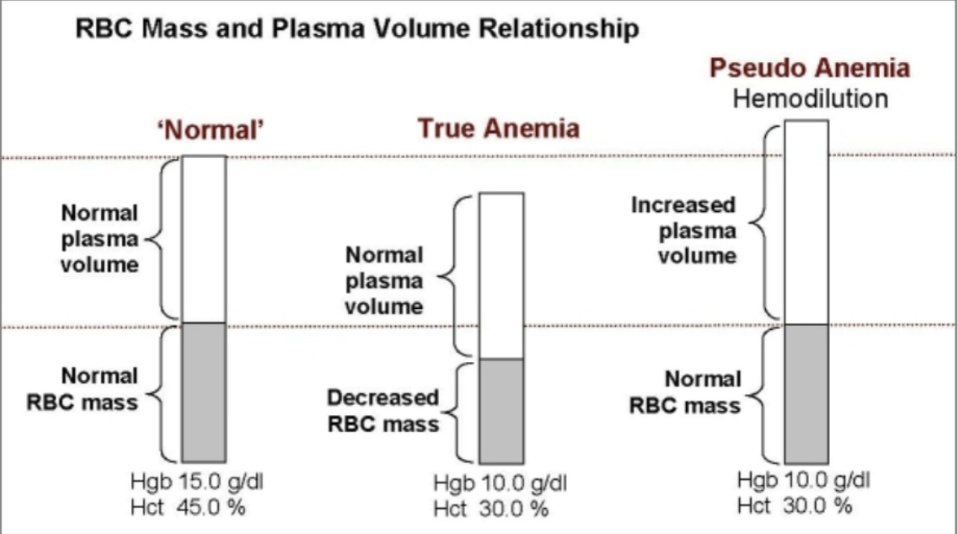
Contrast true anemia and pseudo anemia (hemodilution).
True Anemia: decrease RBC mass and normal plasma volume
Pseudo or Dilution Anemia: normal RBC mass and increased plasma volume
High amounts of IV fluid administration, or fluid accumulation in congestive heart failure or pregnancy
Identify the two general mechanisms or causes responsible for the development of anemia.
Decreased delivery of red cells to the blood: Retic count is inappropriately low
The bone marrow fails to respond appropriately due to disease or lack of essential supplies
Increased loss of red cells from the blood: Retic count is typically high
Anemia results when red cell loss exceeds in the bone marrow’s capacity to increase its activity
Microcytic/Hypochromic Anemia
Retics = normal to low
Maturation Defect: Low HGB synthesis
Differential Diagnosis: Iron deficiency, thalassemia syndromes, Sideroblastic anemia (anemia of chronic disease)
Macrocytic/Normochromic Anemia
Maturation Defect: Decreased DNA synthesis
Normal to low retic
Differential Diagnosis: Vitamin B12 deficiency, folic acid deficiency
Normocytic/Normochromic
Production Defect: bone marrow injury, decreased erythropoietin, marrow infiltration.
Retic: normal to low
Differential diagnosis: aplastic anemia, renal disease, malignant cells
Anemias caused by decreased delivery of red cells to circulation
microcytic/hypochromic
macrocytic/normochromic
normocytic/normochromic
Anemias caused by increased loss of red cells from circulation
Hemorrhage
normocytic/normochromic
Retic = high
Differential diagnosis: acute blood loss
RBC Survival Defect: increased destruction
normocytic/normochromic
Retic = high
Differential diagnosis: hereditary and acquired hemolytic anemias
Assess the clinical significance of CBC and differential, including red cell morphology
Detects mild (~10 g/dL Hgb) to severe anemia (<8 g/dL Hgb)
RBC indices (MCV) are used to classify anemia
RBC morph abnormalities can be diagnostic or suggest a cause that guides further testing
WBC & PLT counts are normal or increased in most anemia but low in aplastic anemia
Assess the clinical significance of Reticulocyte count
Retic count (absolute)
Measures rate of RBC production by the bone marrow
Helps differentiate normocytic anemias
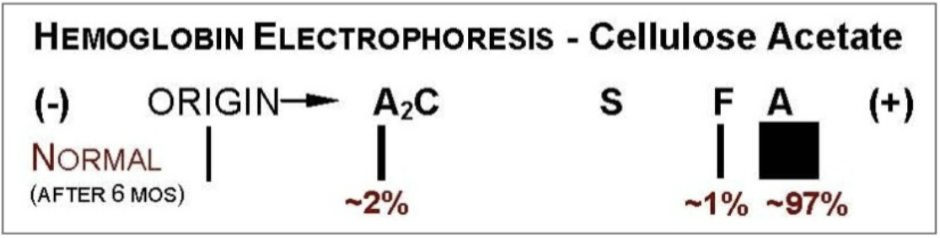
Assess the clinical significance of Hemoglobin electrophoresis
Detects and quantitates both normal and abnormal Hgb types
Useful for Thalassemias and Hemoglobinopathies
Assess the clinical significance of Hemoglobin S turbidity/solubility prep
based on the principle that deoxygenated HbS is insoluble in a high-phosphate buffer solution and forms a turbid precipitate, unlike normal hemoglobin which remains in solution — providing a rapid bedside or laboratory screening tool for the presence of HbS
Its primary clinical significance lies in screening for sickle cell disease and sickle cell trait, particularly in urgent settings such as preoperative evaluation or neonatal screening programs, where a quick qualitative result is needed before more definitive testing is available.
the test cannot distinguish between sickle cell trait (HbAS), sickle cell disease (HbSS), or compound heterozygous states (e.g., HbSC, HbS-β-thalassemia), nor does it quantify HbS percentage, so a positive result must always be followed by hemoglobin electrophoresis or HPLC for definitive diagnosis and clinical management decisions
Asses the clinical significance of Iron Studies (serum iron, TIBC, percent saturation, serum ferritin)
Iron Tests
Used to differentiate microcytic anemias or detect iron overload
Iron circulates bound to transferrin
Transferrin is normally ⅓ saturated with iron
Iron Tests included
Serum iron level: measures the amount of iron bound to transferrin
Total Iron Binding Capacity (TIBC): an indirect measure of the amount of transferring protein in the blood
Serum Ferritin: indirectly reflects stored iron in tissues
Assess the clinical significance of Vitamin B12 and folate levels (serum and RBC)
Identify the cause of macrocytic anemias (megaloblastic)
Assess the clinical significance of Intrinsic factor or parietal cell antibody tests
Intrinsic factor antibodies (IFA) and parietal cell antibodies (PCA) are serological markers used in the investigation of megaloblastic anemia due to vitamin B12 deficiency, specifically to identify pernicious anemia as the underlying cause — an autoimmune condition where destruction of gastric parietal cells and/or blockade of intrinsic factor impairs B12 absorption in the terminal ileum.
IFA are highly specific for pernicious anemia (>95%) but relatively insensitive (~50-60%), making them a confirmatory rather than screening test, while PCA are more sensitive (~85-90%) but less specific as they can be positive in other autoimmune conditions such as autoimmune thyroiditis and type 1 diabetes.
Together, these tests are clinically significant because they shift the diagnosis of B12 deficiency from a nutritional or dietary cause to an autoimmune absorptive defect, which has direct therapeutic implications — lifelong parenteral or high-dose oral B12 supplementation is required rather than simple dietary correction — and also prompts surveillance for associated autoimmune conditions and gastric carcinoid tumors.
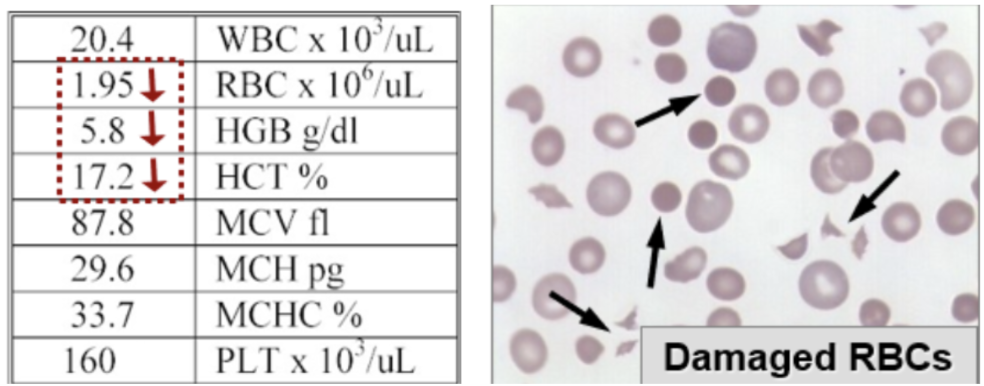
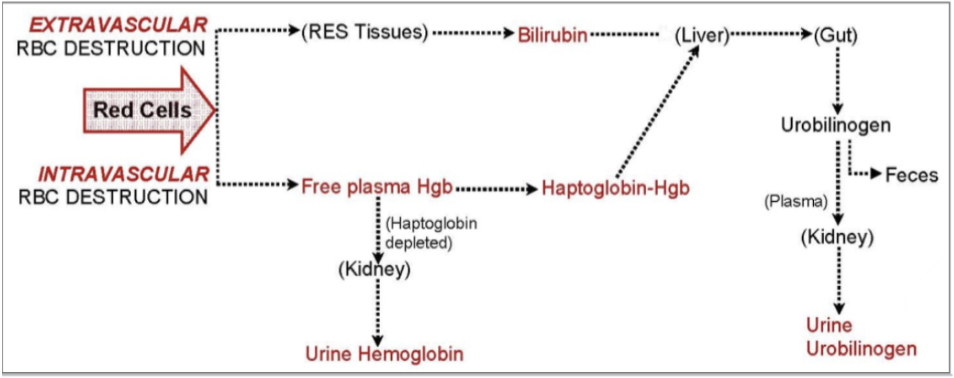
Assess the clinical significance of Red cell destruction tests (e.g., bilirubin, urine urobilinogen, lactate dehydrogenase (LD), free plasma hemoglobin, haptoglobin)
Useful for detecting hemolytic anemia
Both normal and increased red cell removal occurs mainly in tissues (extravascular RBC destruction)
Intravascular destruction occurs in the blood with release of free Hgb - haptoglobin bind free plasma Hgb
Lab results associated with RBC destruction
Increased serum bilirubin (unconjugated)
Urinalysis
Increased urine urobilinogen
Hemoglobinuria detected
Decreased haptoglobin: it’s job is to bind free plasma Hgb, but it can very quickly all become consumed
Increased lactate dehydrogenase (LD) level
Released when red cells rupture
Assess the clinical significance of Direct antiglobulin/antibody test (DAT)
Detects Ab and/or complement coated red cell
Useful for hemolytic anemias
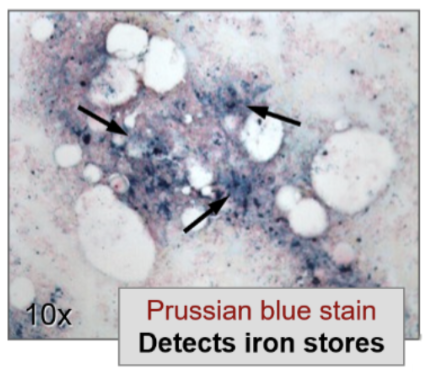
Assess the clinical significance of Bone marrow examination
Evaluates number and type of precursor cells
Restricted to anemias due to production defects
Can also assess bone marrow iron stores with Prussian blue iron stain
Assess the clinical significance of Erythropoietin (EPO) level
Helps distinguish between primary and secondary causes of erythrocytosis or anemia by revealing whether the bone marrow’s erythropoietic drive is appropriate for the degree of hypoxia or anemia present.
In cases of anemia, a low or inappropriately normal EPO level points toward renal insufficiency or primary bone marrow disorders (e.g. myelodysplasia), since the kidneys are failing to up-regulate EPO production as expected.
A marked elevated EPO level in an anemic patient suggests an appropriate compensatory response to a non-renal cause — such as iron deficiency, hemolytic anemia, or chronic blood loss — or, in the context of erythrocytosis, may indicate a secondary/paraneoplastic EPO-secreting tumor.
assess the clinical significance of Heinz body prep (supravital stain)
Detects denatured, precipitated hemoglobin aggregates within red blood cells, which form when hemoglobin is oxidatively stressed beyond the cell's capacity to protect itself
Their presence is clinically significant in identifying G6PD deficiency, where the lack of adequate glutathione-mediated antioxidant defense leaves hemoglobin vulnerable to oxidation — typically triggered by certain drugs, infections, or foods — as well as in unstable hemoglobin variants that spontaneously denature.
This test is particularly valuable because Heinz bodies are not visible on standard Wright-stained peripheral smears, so a targeted supravital stain is necessary to reveal the underlying oxidative hemolytic mechanism and guide further confirmatory testing such as G6PD enzyme assay or hemoglobin electrophoresis
Assess the clinical significance of Osmotic fragility test
measures the ability of red blood cells to withstand hypotonic stress, with increased fragility indicating cells that lyse more readily due to a reduced surface-area-to-volume ratio — the hallmark of spherocytes.
This test is most clinically significant in the diagnosis of hereditary spherocytosis, where defects in membrane-cytoskeletal proteins (such as spectrin, ankyrin, or band 3) cause RBCs to lose membrane surface area and assume a spherical shape with limited ability to expand in hypotonic conditions, and it can also be positive in autoimmune hemolytic anemia where antibody-mediated membrane loss similarly produces spherocytes
Iron Deficiency Anemia
Decreased iron availability
Progressive depletion of iron in the body
Lack of iron results in reduced red blood cell and hemoglobin production
Causes:
Nutritional lack (rare in males)
Malabsorption
Increased need
Chronic blood loss (usual cause in males)
Sequence of iron depletion
Iron stores depleted first: asymptomatic, low serum ferritin test
Iron-deficient erythropoiesis
Iron-deficiency anemia
Blood findings:
Mild to severe microcytic/hypochromic anemia
Ovalocytes/pencils, NO RBC INCLUSIONS expected
Low serum iron, high TIBC, low serum ferritin
Clinical Symptoms
Pica – cravings for ice, dirt, etc.
Spoon shaped nails, brittle nails and hair
Tongue glossitis – raw and sore
Numbness and tingling
Treatment
Treat primary disease
Oral supplements
Marked retic response 3-5 days later, dimorphic
Thalassemias
decreased rate of globin synthesis, alpha or beta.
Inherited decrease in alpha or beta globin chain synthesis needed for Hgb A
QUANTITATIVE defect
All have microcytic/hypochromic RBC and target cells
Genetic mutations classified by:
↓ beta chains = beta thalassemia (Greek/Italian)
↓ alpha chains = alpha thalassemia (Asian)
Consult review chart posted in MLS 408
Sideroblastic Anemia
Block in protoporphyrin synthesis leads to iron overload and microcytic/hypochromic anemia. Can be primary or secondary.
Blood findings:
Variable severity micro/hypo anemia
RBC inclusions
High serum iron, high serum ferritin, and low TIBC
Sideroblastic Anemia: Primary Type
unknown or idiopathic
Blocks unknown
Can’t ID
Irreversible
Sideroblastic Anemia: Secondary Type
can identify cause of blocks
Reversible
Alcohol, anti-tuberculosis (TB) drugs, lead (multiple)
Can be caused by Lead Poisoning
Cause coarse basophilic stippling
Inhaled or ingested
Neurologic problems
Chelation therapy