ESP Comp
1/221
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
222 Terms
What is physical function crucial for?
Independent living and involves various components such as balance, cardiopulmonary endurance, coordination, flexibility, mobility, muscle performance, neuromuscular control, postural control, and stability
What is the purpose of therapeutic exercise?
Systematically planned to remediate or prevent impairments, enhance activities and participation, reduce health-related risks, and optimize overall health and well-being. Physical therapists tailor these programs to meet individual patient needs
What are the components of therapeutic exercise?
Examination, intervention, and outcomes assessment, aiming to improve physical function, health, wellness, and fitness while reducing complications, pain, and risks during activities
What is the overload principle?
Exercise must challenge the body more than usual to stimulate adaptation
What is the SAID principle?
Training adaptations are specific to the type of exercise performed
Specific Adaptation to Imposed Demands
What is the reversibility principle?
Benefits gained from exercise are lost if the exercise is discontinued
What is the individual differences principle?
Responses to exercise vary due to factors like age, genetics, and initial fitness levels
What is the FITT-VP Framework?
Frequency, Intensity, Time, Type, Volume, and Progression
Essential for structuring exercise prescriptions. This approach ensures that exercise interventions are tailored, progressive, and aligned with the patient's goals
Why do PT's emphasize task-specific exercises?
Improve performance in daily activities and participation in life roles, thereby enhancing the overall quality of life
What are the macronutrients broken down in ATP for energy and much do they yield?
Carbohydrates: 4 kcal/gram
Fats: 9 kcal/gram
Proteins: 4 kcal/gram
How are the fuel choices used for energy production?
Carbohydrates are absorbed primarily as glucose and are rapidly used to produce energy, though the yield is lower compared to fats
Fats, absorbed as fatty acids and triglycerides, produce more energy but require a longer process and depend on carbohydrate metabolism to proceed
Proteins serve as a vital building block for cells and can also be used for energy during prolonged activities through processes like deamination and gluconeogenesis
What are the 3 major energy systems?
Phosphagen System: Provides immediate energy for short bursts of activity (<30 sec)
Anaerobic Glycolysis: Supports high-intensity activities without oxygen (30-90 sec)
Aerobic System: Sustains lower-intensity activities over longer periods, utilizing oxygen to metabolize carbohydrates, fats, and proteins (>2 mins)
What is VO2?
Oxygen consumption which is a critical measure of energy production and is used to assess aerobic capacity during rest, submaximal, and maximal exercise
What are the main fuel sources during endurance activities?
Fats are a significant fuel source for endurance activities lasting more than 90 minutes, with proteins also contributing as an energy source through gluconeogenesis during prolonged exercise
How does substrate use change based on exercise intensity?
Lower Intensity (< 70% VO2 max): Relies more on fats (60%) and less on glucose (40%)
Higher Intensity (> 70% VO2 max): Shifts to using primarily carbohydrates (glucose) for energy
What are GLUT4 transporters?
Muscles use these to absorb glucose without the need for insulin
T/F: energy systems function independently without crossover (like on/off switch)
False, they operate concurrently, with their contributions varying depending on the intensity and duration of the activity
What is the resting oxygen consumption?
3.5 ml/kg/min
1 MET
What is VO2 max?
Maximum volume of oxygen that can be taken in, transported, and utilized by the body during intense exercise
= product of maximal cardiac output and the maximal arteriovenous oxygen difference
What are examples of field tests for estimating VO2 max?
Cooper Walk/Run Test: Running or walking as far as possible in 12 minutes
1.5 Mile Run Test: Running 1.5 miles as quickly as possible
Step Test: Stepping up and down on a platform for 3 minutes
Rockport Walk Test: Walking one mile as quickly as possible
What are ventilatory responses to exercise?
Ventilation increases rapidly at the onset of exercise due to signals from muscle receptors, followed by fine-tuning based on blood gas levels by chemoreceptors. This ensures efficient oxygen intake and carbon dioxide removal.
What are cardiovascular responses to exercise?
Cardiac output and muscle blood flow increase significantly during exercise, with systolic blood pressure rising linearly with intensity. This enhances oxygen delivery and nutrient supply to active muscles
What are metabolic responses to exercise?
The body mobilizes energy stores (like glycogen and fat) and increases oxygen transport to meet the demands of working muscles
What are exercise specific changes to blood flow distribution?
Blood is shunted from less active tissues to active muscles, leading to a significant increase in cardiac output
What are exercise specific changes to heart rate?
Increases linearly with exercise intensity and plateaus at maximum effort
What are exercise-specific changes to blood gases?
Arterial oxygen levels typically remain stable during submaximal exercise; deviations indicate poor exercise tolerance
What are ventilatory adaptations to training?
Increased lung volumes and diffusion capacities improve ventilatory efficiency, allowing for better oxygen utilization during exercise
What are cardiovascular adaptations to exercise?
Regular exercise results in a lower resting heart rate and blood pressure, increased stroke volume, and enhanced blood oxygen-carrying capacity
What are metabolic adaptations to training?
Exercise leads to muscle hypertrophy, increased mitochondrial density, improved fat metabolism, and a reduced reliance on immediate energy stores like phosphocreatine and ATP
What are age-related differences in exercise outcomes?
Children: Exhibit higher heart rates and respiratory rates but lower cardiac output and stroke volume compared to adults.
Older Adults: Experience a decline in maximum heart rate, cardiac output, VO2 max, and muscle strength, with increased blood pressure and longer recovery times.
Define physical fitness
Defined as the ability to perform physical work efficiently, requiring cardiorespiratory function, muscle performance, and joint range of motion. Fitness is often measured by VO2 max
Define endurance
The capacity to sustain prolonged physical activity, specific to the type and duration of exercise, and involves both muscular and cardiovascular endurance
Define central fatigue
Originates in the central nervous system (CNS) and affects the brain and spinal cord's ability to stimulate muscles. It is influenced by psychological factors, neurotransmitter activity, and physiological conditions like brain oxygenation
Impacts both physical and cognitive functions and develops slowly during submaximal exercise
Define peripheral fatigue
Occurs within the muscles due to metabolic changes and the accumulation of byproducts like reactive oxygen species (ROS), inorganic phosphates, and lactate
Impairs muscle function and slows contraction, particularly during high-intensity exercise
What are the mechanisms of fatigue?
Motor Performance Fatigue: Refers to a measurable decline in the neuromuscular system's force production capacity due to neural and muscular factors
Perceived Motor Fatigue: The subjective experience of fatigue during a motor task, often described as tiredness, weariness, or lack of energy
What factors influence fatigue?
Various factors such as health status, diet, lifestyle, stress, sleep deprivation, and motivation can influence the onset and severity of fatigue
Mental fatigue, in particular, increases the perception of effort, making tasks feel more demanding
Describe the recovery from fatigue
Varies depending on whether it is central or peripheral
Central fatigue typically recovers quickly, while peripheral fatigue, particularly from resistance exercise, can take days due to muscle damage
Recovery also depends on the duration of the exercise, with longer activities requiring more extended recovery periods
Describe the fitness-fatigue model
Balance between fitness improvements and temporary performance reductions due to fatigue
Proper management of intensity, volume, and recovery can optimize training gains while minimizing the risk of overtraining.
Define overreaching
Short-term performance decrements that recover within days to weeks
Define overtraining
Long-term performance decrements that require weeks to months for recovery, often accompanied by a range of physiological and psychological symptoms
Define overtraining syndrome
A complex condition resulting from excessive training with insufficient recovery, leading to persistent fatigue, decreased performance, mood disturbances, and other physiological and psychological symptoms
What are key exercise prescription variables in managing fatigue and ensuring optimal performance and recovery?
Rest interval, recovery, frequency, and duration
Define capacity
Refers to what an individual can do in a standardized, controlled environment, representing their highest potential level of functioning
Define performance
Describes what an individual actually does in their daily environment, considering physical, social, and personal factors
T/F: to avoid injury performance should exceed capacity
False, Performance should never exceed capacity to avoid injury
Describe the physical stress theory
The body's tissues respond to physical stress in predictable ways
Responses range from decreased tolerance (atrophy) to maintenance, increased tolerance (hypertrophy), injury, and even death, depending on the level of stress
Appropriate levels of stress can lead to beneficial adaptations, while excessively high stress can cause injury or tissue death
What is Wolff's Law?
Bones adapt to the loads they are subjected to, becoming stronger with increased stress and weaker with reduced stress. This process is known as bone remodeling
What is Davis's Law?
Soft tissues, like muscles and tendons, adapt to the demands placed on them by lengthening under tension and shortening in its absence. This law also explains how scar tissue aligns along lines of stress, which is crucial for recovery after injury or surgery
What is the envelope of function?
Illustrates the range of physical stress or training loads that influence physiological responses
Training within the "envelope" promotes adaptation, while exceeding it can lead to overtraining or injury
What is progressive overload?
For effective exercise programs, a gradual increase in training stress is necessary to stimulate adaptation and improve performance. This involves manipulating various training variables to match the stimulus to specific goals
What are training adaptations in aerobic exercise?
Increases aerobic capacity through central adaptations (e.g., increased cardiac output) and peripheral adaptations (e.g., more and larger mitochondria)
What are training adaptations in resistance exercise?
Leads to skeletal muscle hypertrophy, improved neural function (e.g., increased motor unit recruitment), and stronger connective tissues, including bones and ligaments
What are the stages of condition/rehab?
Acute/Protective: highly irritable and severe state of patient's system, goal of intervention is symptom modulation
Subacute/controlled motion: stable, moderately irritable, moderately severe state of symptoms, goal of intervention is movement control
Chronic (stable)/settled/return to function/sport: stable state of low severity/irritability of symptoms, goal of intervention is optimizing return to function/sport/recreation
Chronic (unstable): state of variable, seemingly unpredictable severity and irritability of symptoms, goal of intervention is functional optimization (often accompanied by nociplastic pain mechanism)
Acute-on-chronic: reinjury of tissue, acute exacerbation of chronic injury, repeated episodes of elevated severity and irritability
What do we do in acute/protective rehab stage?
APOLICE
Activity modification/education: positions, postures, patterns (3 Ps)
Protect: brace, splint, tape, sling, loose pack
Optimal Load: same
Ice (pain control, swelling control)
Compression: decrease swelling response
Elevate: decrease swelling response/aid venous return
Think submax isometric exercise, PROM/AROM/AAROM, exercise other areas
What are the goals in controlled motion stage of rehab?
Goal: apply load to promote tissue healing but not inhibit
Goal: return to full ROM, muscle length
Goal: Maintain aerobic fitness
Goal: Begin strengthening and/or prevent motor inhibition>>progress
Goal: Intervene for contributing factors (3 Ps)
What do we do in return to function stage of rehab?
Goal: progressively increase tissue load to tolerance without re-injury
Goal: normalize muscle performance
Goal: progress to functional movement >> functional speed
Think: Progress strengthening, Over pressure to joint mob/stretching, power, Add function-specific exercise and training, Progress endurance: cardiovascular and local, Correct biomechanics and 3 Ps: PREVENTION, Task and function-specific activities
What do we do in performance/prevention rehab phase?
Goal: improve performance and prevent injury
Consider: improve on strength, endurance, power, coordination from previous levels
What is cardiorespiratory fitness (CRF)?
Describes the capacity of the heart, lungs, and muscles to transport and use oxygen during sustained physical activity
Essential for overall health and performance, influencing how effectively the body performs prolonged physical activities
How can we determine exercise intensity in CRF?
Maximal Heart Rate (HRmax): Usage of formulas such as the Tanaka formula to estimate the maximum heart rate based on age.
Heart Rate Reserve (HRR): Utilizing the Karvonen method to calculate target zones based on fitness levels.
Metabolic Equivalents (METs): How energy expenditure during exercise compares to rest.
Rate of Perceived Exertion (RPE): Using scales like the Borg RPE to assess intensity based on personal perception of effort.
Counting Talk Test (CTT): A practical tool to gauge intensity by measuring speech comfort during exercise.
What is periodization?
Structuring training into distinct phases with varying focus on workload to maximize performance and minimize injury risk
What are the continuous training options in CRF?
Long Slow Distance (LSD): Focus on endurance by maintaining a low to moderate intensity over an extended period (builds aerobic base)
Moderate Intensity Continuous Training (MICT): Sustained effort at a moderate level, balancing energy expenditure and recovery (create adaptation in both oxidative and glycolytic energy systems)
High-Intensity Endurance Training: Still continuous exercise but performed at higher intensities near or above the lactate threshold (improves oxidative and glycolytic energy systems)
What are the interval training options in CRF?
High Intensity Interval Training (HIIT): Alternates short bursts of high- intensity work with rest or low activity periods for recovery (>80-100% HRpeak)
Sprint Interval Training (SIT): Involves brief, intense efforts followed by extended recovery times. (>100% VO2peak)
High Intensity Functional Training (HIFT): Involves full-body functional compound movements performed at high intensity (80-100% HRpeak)
Resistance Based Interval Training: Integrated into aerobic programs, increase muscular endurance and cardiovascular demand
Fartlek Training: A blend of continuous and interval styles, allowing variable intensity and spontaneous shifts in workout focus.
What are the general adult FITT-VP for CRF?
F: 3-5x/wk
I: moderate (40-59% HRR, 64-76% HRmax, 46-63% VO2max, 3-5.9 METs, mod RPE 4-5, RPE 12-13) or vigorous (60-89% HRR, 77-95% HRmax, 64-90% VO2max, >/= 6 METs, RPE 14-17, Mod RPE 6-8)
T: 150-300 min/wk moderate or 75-150 min/wk vigorous
T: Aerobic continuous or interval depending on choice
V: >150 min/wk moderate or >75 min/wk vigorous
P: Increase duration, then frequency, then intensity
How does exercise prescription change for children in CRF?
Higher resting HR
Immature thermoregulation
Different metabolism
>/= 60 mins/day (can accumulate in shorter sessions)
Activities should be fun, varied, skill-building
Watch for excess fatigue, decreased performance, growth plate injuries
Ensure proper equipment, safe environment, adult supervision
Encourage nutrition (Balanced meals to support growth and activity)
How does exercise prescription change for older adults CRF?
Start Low and Progress Slowly
Warm-up/Cool-down important to prevent BP fluctuations and Injury
Frequency of most days of the week (consistency key for maintaining fitness and managing chronic disease)
Prefer low-impact activities
Programs should also include: strength training, flexibility exercises, balance training (Enhance balance, coordination, and muscle function)
Stop exercise if symptoms occur: dizziness, chest pain, excessive fatigue
Social exercise improves adherence, mental health, motivation
Medical Clearance Necessary: before starting an exercise program, especially with chronic conditions
Decrease sensation of thirst
Nutrition to support exercise level and health needs
Use RPE (especially if on beta-blockers)
Skilled and individualized aerobic exercise programs for older adults can be both safe and beneficial → helping to improve QOL, enhance physical function, and manage health conditions effectively
What are special exercise considerations for metabolic syndrome CRF?
Special attention to risk factors w/ conservative criteria for initial workloads
Reduce impact of dx, moderate or high intensity exercise recommended when safe
Reduction of body weight is important goal
Combination of resistance training w/ aerobic training can produce greater decreases in metabolic syndrome prevalence
What are special exercise considerations for overweight/obese patients CRF?
Goal of >250 min/wk may be achieved through multiple bouts of shorter time increments
Resistance exercise does not result in clinically significant weight loss, BUT may enhance physical function and other health benefits to reduce risk factors
When do we terminate exercise?
Drop in HR during increasing workload is alarming and could be a medical emergency
Drop in SBP >10 mmHg w/ increase in intensity
Exaggerated HTN response: SBP >250 mmHg, DBP >115 mmHg
Drop in SpO2 ≥5% w/ increase in intensity or SpO2<90% in normal
Onset of Angina, excessive fatigue, SOB, wheezing, leg cramps/claudication
Signs of pallor/cyanosis
Individual request to stop exercising
Describe Polarized Training
Avoid mod intensity work (gray zone)
Build strong aerobic base
70-80% low intensity and 20-30% high intensity
Describe pyramidal training
Intensity distribution resembles pyramid shape
Benefits: Balanced development of aerobic and anaerobic system and improves endurance and race performance
Application: mix low intensity steady-state workouts, mod intensity tempo sessions, and high-intensity interval training
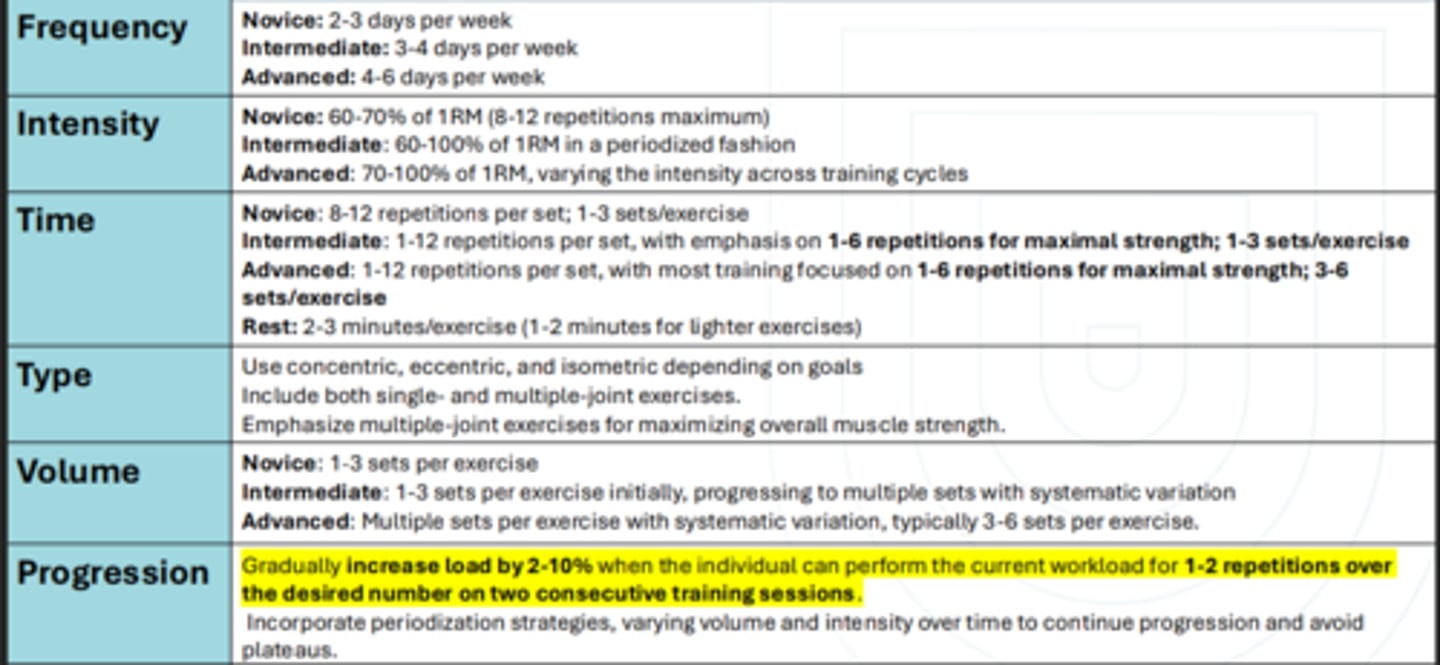
What is the FITT-VP for resistance strength?
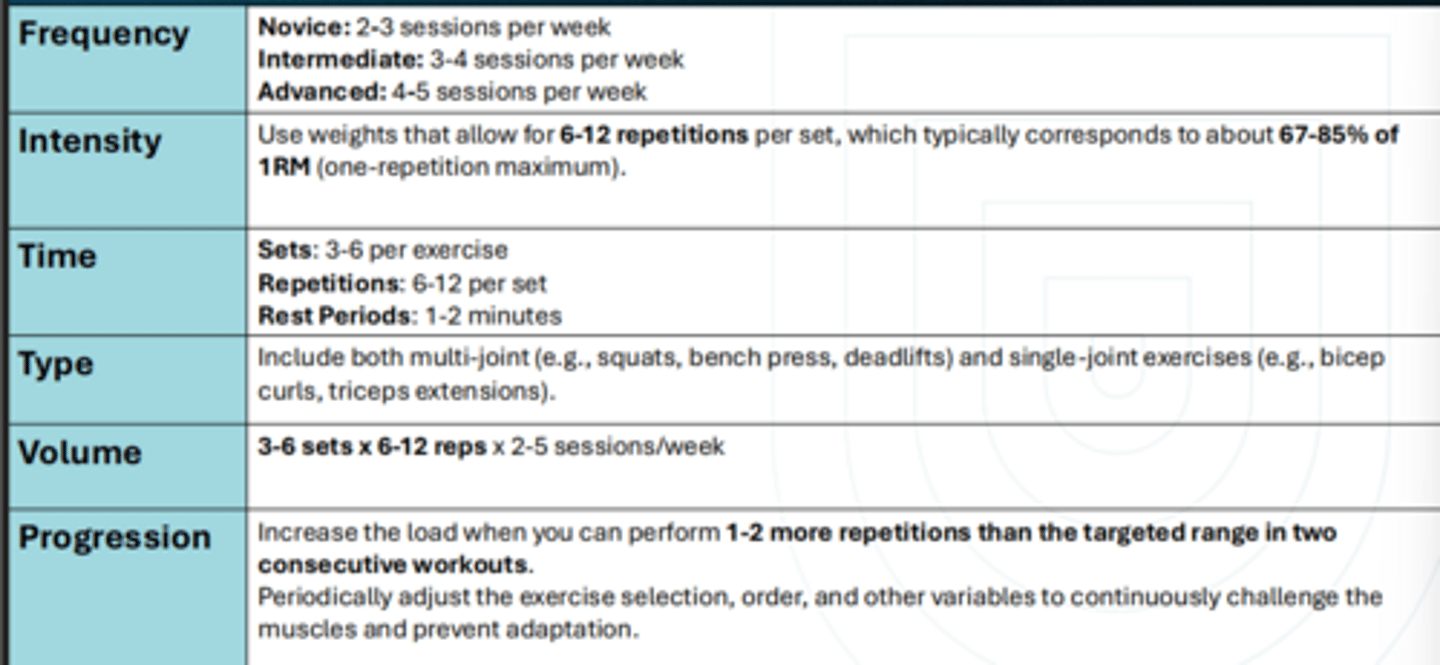
What is the FITT-VP for muscular hypertrophy?
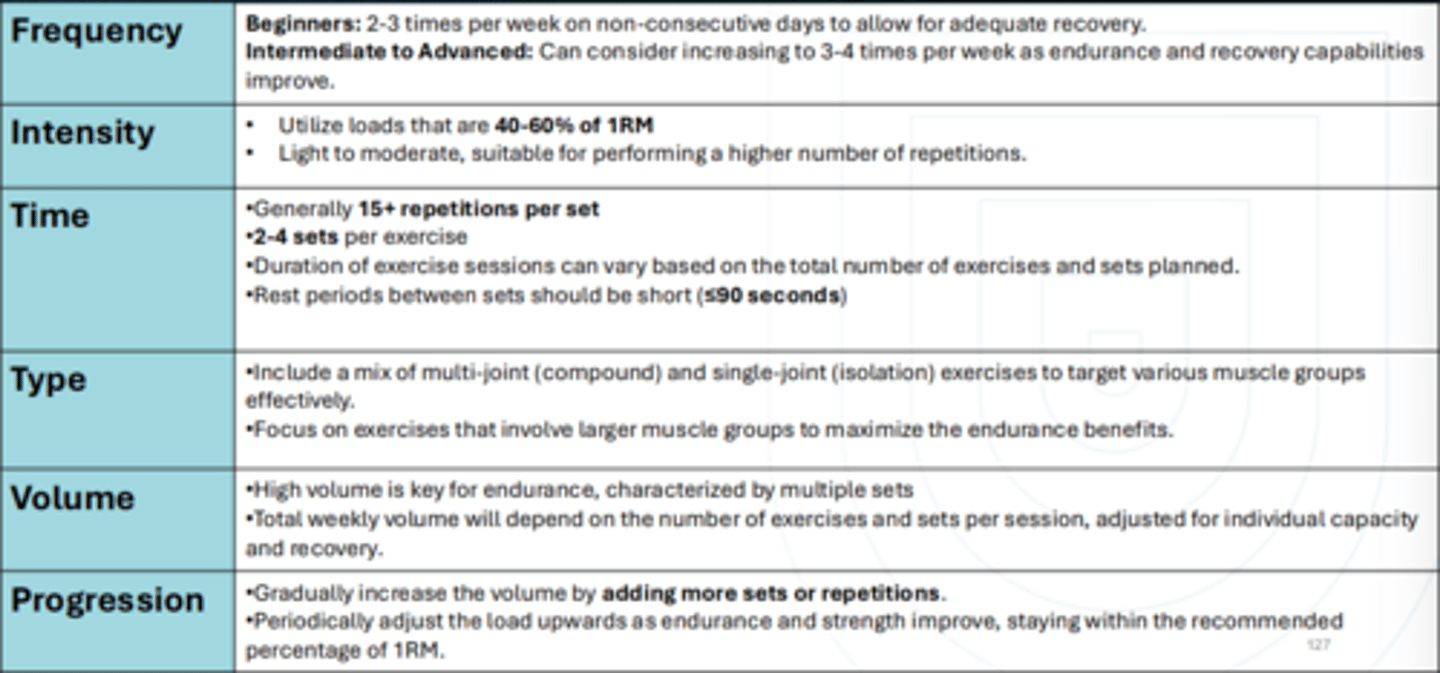
What is the FITT-VP for local muscular endurance?
What is the FITT-VP for power?
F: 2+/wk
I: UE 30-60%1RM, LE 0-60% 1RM, low RPE w/ high RIR
T: 1-3 sets for 3-6 reps (trained) or 6-10reps (untrained/older adults) w/ >2 min rest
T: Max velocity, relate to goal task (healthy) OR high velocity but min risk while focusing on major muscle groups (untrained/OA)
V: insufficient evidence
P: speed/load (rate of force production)
What is the FITT-VP for plyometrics?
F: 1-3x/wk (except older adults, few recommendations)
I: 80-100% max velocity, low RPE w/ high RIR
T: LE 50-200+ foot contacts, UE less researched w/ 6-30 sec per set and work to rest ratio of 1:2
T: plyometrics
V: more research needed, insufficient evidence recommended foot contacts mentions (beginner: 80-100, intermediate: 100-120, advanced: 120-140)
P: increase intensity, reps, number of plyo exercise in session (prioritize decreasing amortization phase)
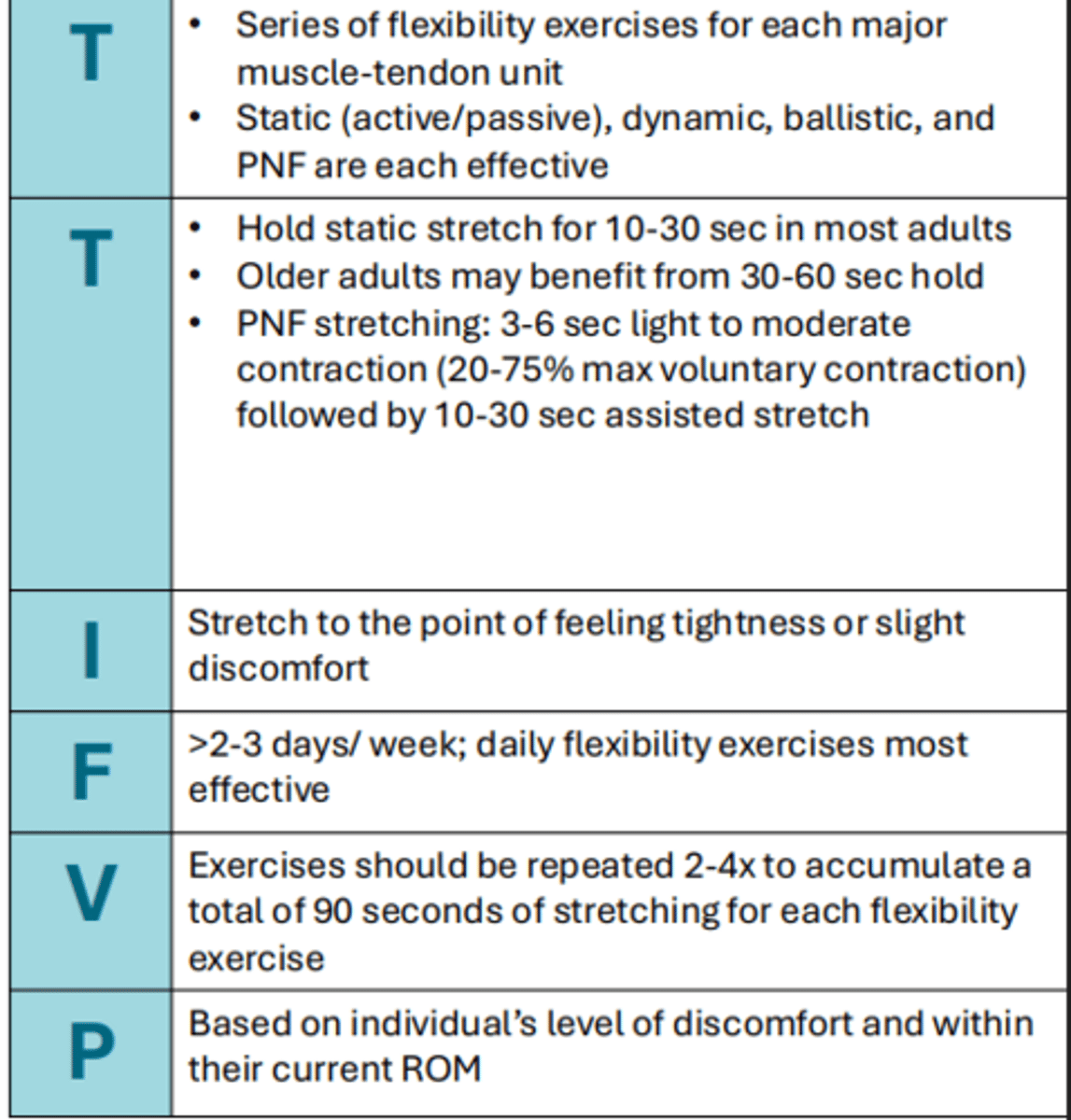
What is the FITT-VP for flexibility?
What is the FITT-VP for balance training?
F: 20-30 min/session x 2-3 days/wk (no ACSM)
I: RPS 4-6/10
T: no ACSM clear rec, studies show improvements w/ 20-30 min session for 2-3x/wk
T: static, dynamic, anticipatory, reactive, sensory, or during functional activities
V: 60 mins/wk shows improvements
P: Intensity, duration, type
Define physical activity
The exercise modes used individually or in combination to engage in an aerobic activity/exercise
Define Exercise
A planned and structured physical activity to improve or maintain physical fitness
Define CRF
Centers around the physiological abilities of the heart, blood vessels, lungs to deliver oxygen and remove carbon dioxide as utilized or produced during cellular respiration
T/F: We should only use 1 metric for measuring intensity
False, best practice is to utilize more than 1
What are the light intensity metrics for CRF?
30%-39% HRR
0-2.9 METs
2-3/10 Modified RPE Scale
9-11 RPE Scale
57-63% HRmax
37-45% VO2max
What are the moderate intensity metrics for CRF?
40%-59% HRR
3.0-5.9 METs
4-5 Modified RPE Scale
12-13 RPE Scale
64-76% HRmax
46-63% VO2max
What are vigorous intensity metrics for CRF?
60%-84% HRR
> 6 METs
6-8 Modified RPE Scale
14-17 RPE Scale
77-95% HRmax
64-90% VO2max
Define MET
Amount of O2 required at rest calculated per mass of 1 kg body weight & time
What is the purpose of using a person's self-perception of work intensity, and in what situations is it especially useful compared to heart rate measures?
Compliments other intensity measures with
a person's self perception of work intensity
when HR measures are less reliable due to medications (i.e.: Beta- blockers), co-morbidities (i.e.: pacemaker), and exercise type
What is the major different for using Borg vs Modified Borg?
Modified is for RPE in non-linear types of exercise while Borg is for linear and correlates to HR
What is exercise intensity directly linked to?
Both the amount of improvement in exercise capacity and the risk of adverse events during exercise (especially in sensitive populations)
What is the Tanaka equation?
HRmax = 208 - (.7*age)
What allows for a better estimation of the heart's work capacity?
Utilization of the individual's resting heart rate
What is the Karvonen formula?
HRR = HRmax - resting HR
T/F: HR and O2 consumption both increase linearly with exercise
True
When is the Astrand formula used and what is it?
HRmax predictions for youth populations
HRmax = 216.6-(.84*age)
What are the purposes of different work to rest ratios?
1:1 - High intensity but allows for substantial recovery
2:1 - Work intensity will decrease due to limiting recovery time, enhancing endurance and metabolic rate
1:2 - Often used for very intense activities like sprinting, allowing more recovery time to maintain the quality and speed of each sprint
1:5+ - The goal is maximal output during work with complete recovery, rest should be long enough to maintain a maximal level of performance.
In interval training, what are the HR changes we expect to see before proceeding to the next exercise interval?
At least 12 bpm decrease after 1 minute of recovery
HR dropping to 130-150 bpm (younger individual)
Define muscle performance
The capacity of a muscle to do work (W = F x d)
Define Resistance Exercise
Physical activity involving muscle contraction is resisted by an outside force applied manually or mechanically
- Improved strength, endurance, tone, mass, or power
Define Resistance Training
Planned systematic program of exercises designed to increase an individual's ability to exert or resist force.
- Aimed to address a specific goal: impairments, improve activity
performance, general conditioning, prevent injuries
What are the benefits of resistance training?
Enhanced muscle performance
Increased strength of connective tissues
Increased bone mineral density
Decreased joint stress
Reduced risk of soft tissue injury
Improved tissue remodeling
Improved balance
Enhanced physical performance
Positive body composition
Enhanced physical well-being
Positive quality of life
What is a motor unit comprised of and innervated by?
Comprised of a group of muscle fibers and innervated by one somatic motor neuron