Uterine Growths and Diseases
1/74
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
75 Terms
What is the 'red flag' rule regarding vaginal bleeding in post-menopausal patients?
Any bleeding in a post-menopausal patient is considered malignancy until proven otherwise.
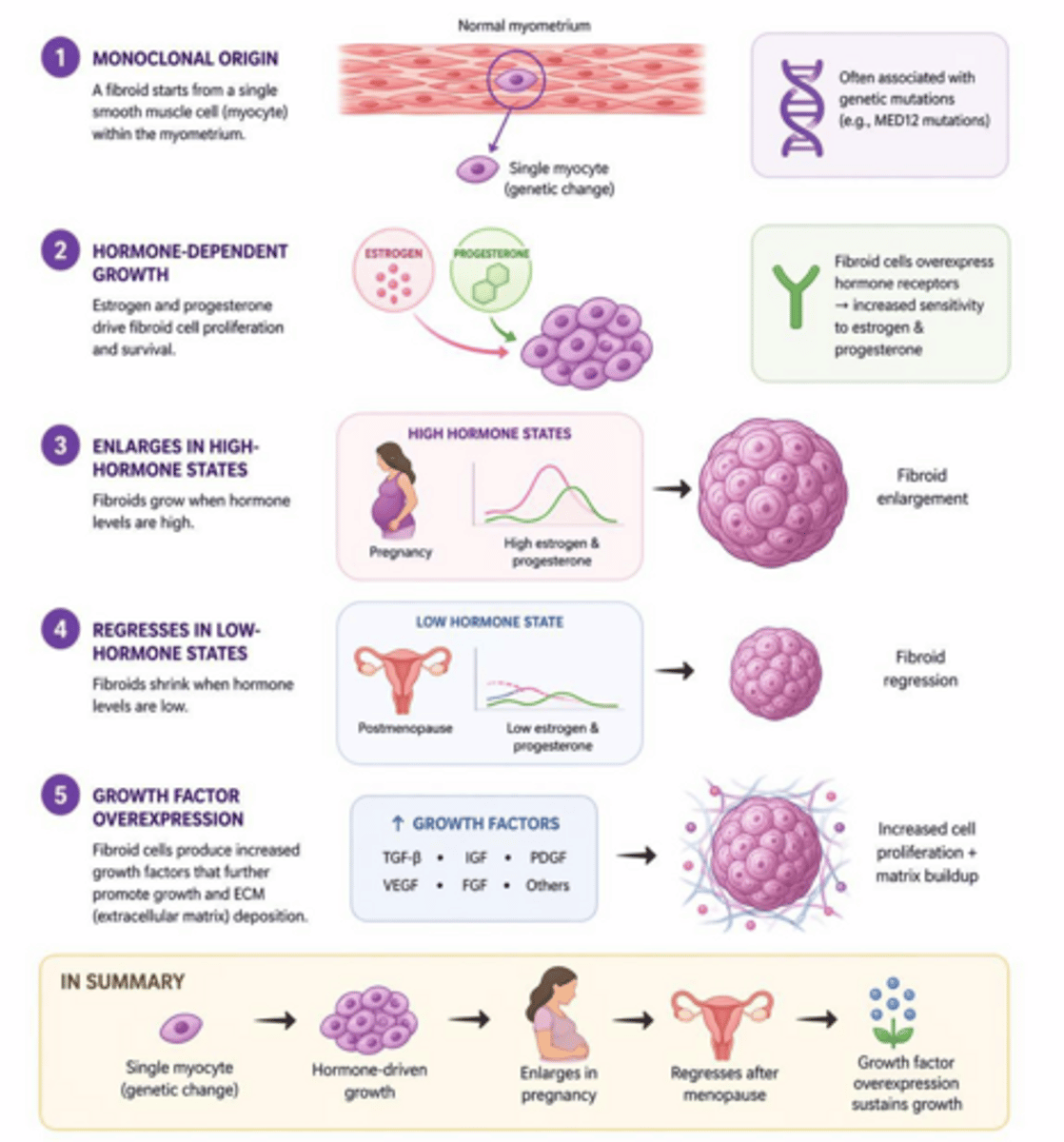
What are uterine leiomyomas (fibroids) derived from?
They are benign monoclonal tumors arising from the smooth muscle cells of the myometrium.
What is the most common pelvic tumor in women?
Uterine leiomyoma (fibroid).
What are the risks factors for fibroids?
Ethnicity (African American women 2-3x higher risk), early menarche, nulliparity, obesity, family history, HTN.
What are the monoclonal origins of fibroids?
They arise from a single smooth myocyte within the myometrium.
How do estrogen and progesterone affect uterine fibroid growth?
They promote proliferation; fibroids typically enlarge during pregnancy and shrink during menopause.
What are the protective factors against developing uterine fibroids?
Hormonal contraceptives are associated with a reduced risk.
Which type of uterine fibroid is the most common?
Intramural; located within the uterine wall, and can distort the cavity.
Which type of uterine fibroid has the highest risk for heavy menstrual bleeding and infertility?
Submucosal fibroids.
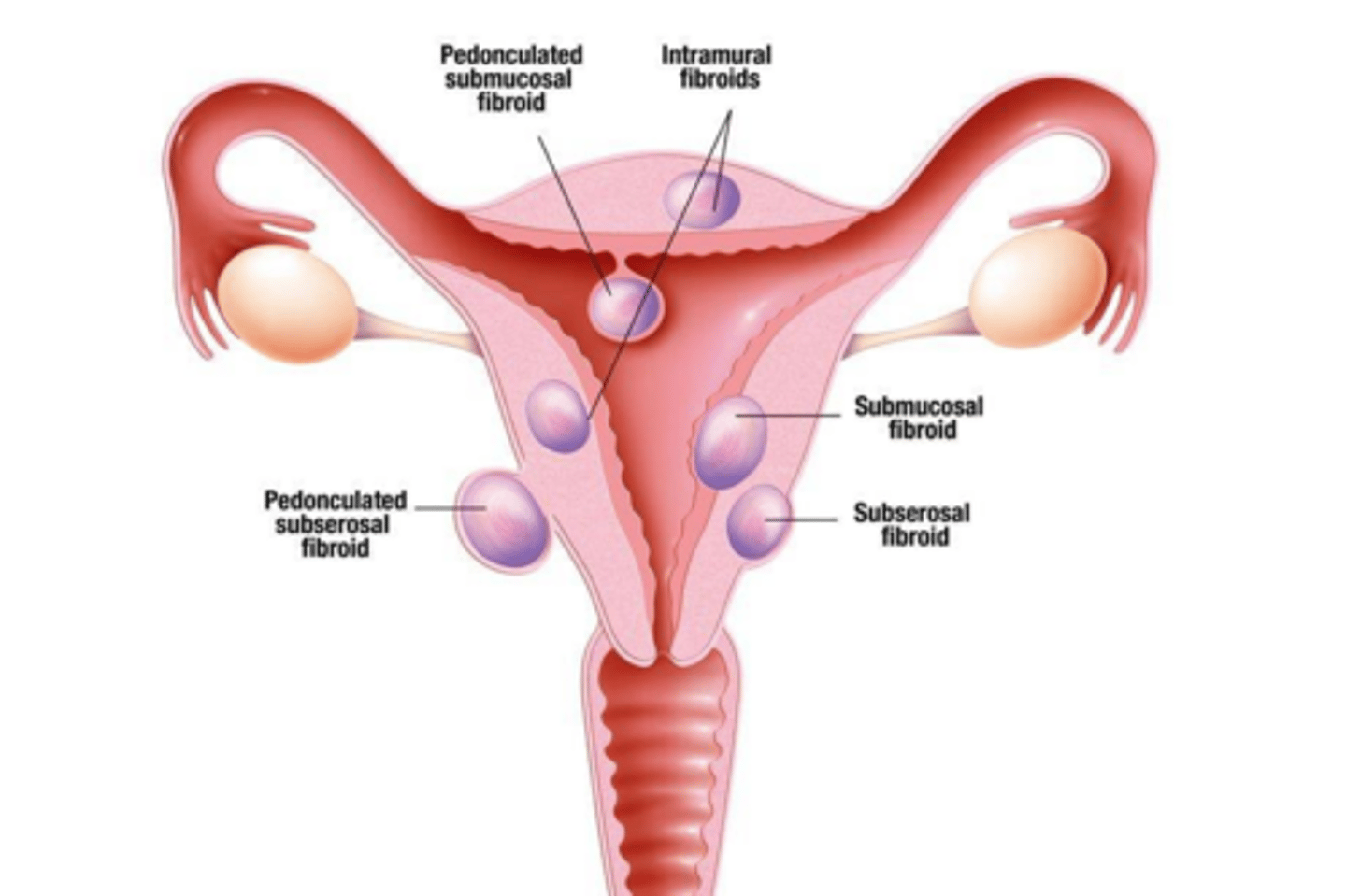
What is the primary risk associated with pedunculated fibroids?
Torsion, which is considered a surgical emergency.
Do majority of women know they have a fibroid?
No, 80% of patients are asymptomatic
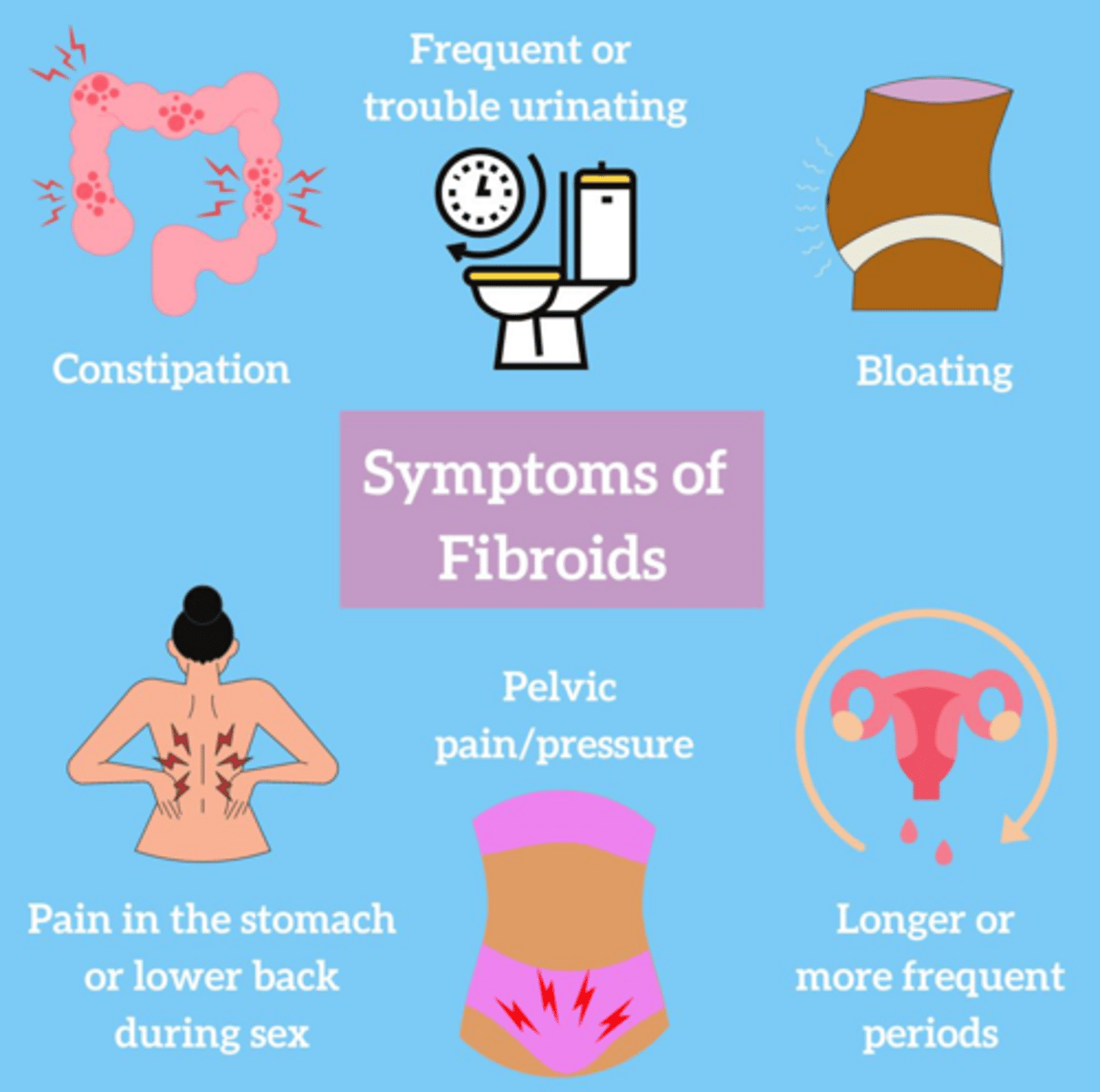
What are the most common 'bulk symptoms' associated with large uterine fibroids?
Pelvic pain/pressure, urinary frequency, urgency or retention, back pain, constipation, and dyspareunia.
What are the classic physical exam findings for a uterus with fibroids?
A firm, enlarged, irregular, and non-tender uterus.
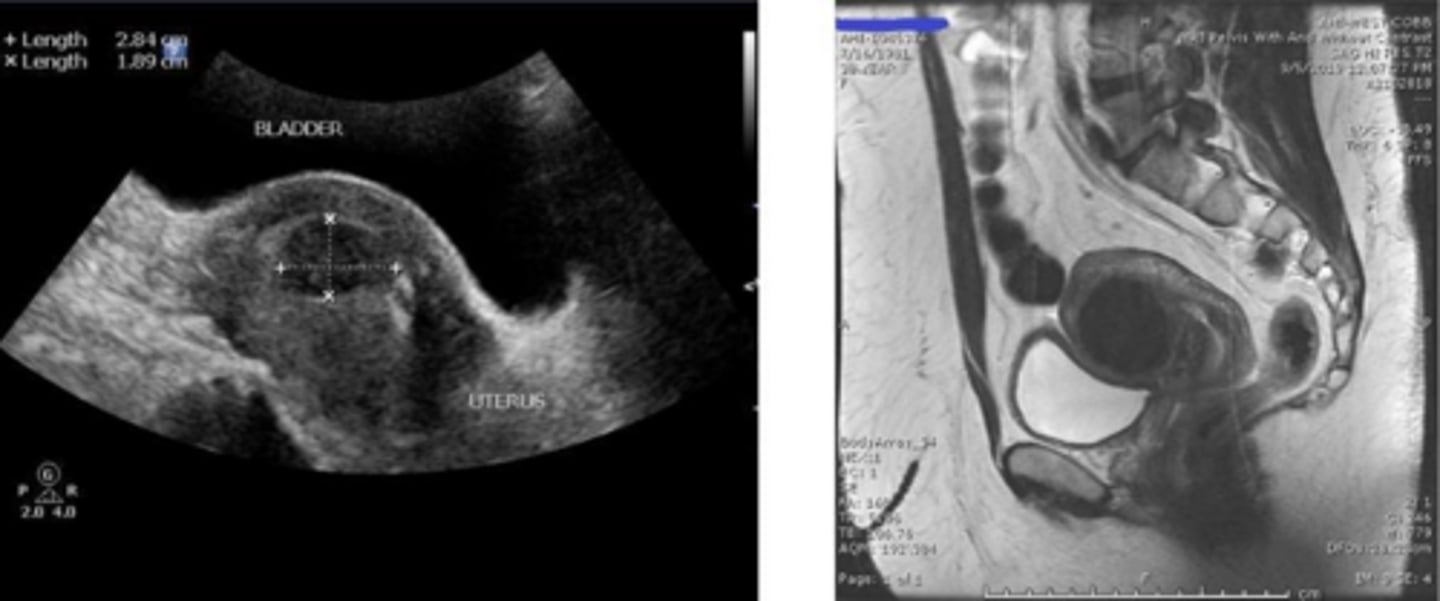
What is the first-line and gold-standard imaging modality for diagnosing uterine fibroids?
Pelvic ultrasound (transvaginal and transabdominal).
When is Saline Infusion Sonohysterography (SIS) indicated for the evaluation of uterine fibroids?
Best for visualizing submucosal fibroids and cavity distortion.
When is MRI typically indicated for the evaluation of uterine fibroids?
It is reserved for surgical planning (e.g., myomectomy) or when malignancy is suspected.
Why is a CBC often ordered for patients with symptomatic uterine fibroids?
To evaluate for iron-deficiency anemia resulting from chronic heavy menstrual bleeding.
What is the first-line medical management for symptomatic uterine fibroids?
Hormonal contraceptives (combined or progestin-only), with IUDs being most effective for reducing blood loss.
What is the clinical role of GnRH agonists/antagonists in fibroid management?
They suppress the HPO axis to shrink uterine size and increase hemoglobin levels, typically used as pre-surgical preparation.
What are the indications for surgical management of uterine fibroids?
Severe anemia, chronic pain, acute torsion, significant symptoms, or rapid growth in post-menopausal patients.
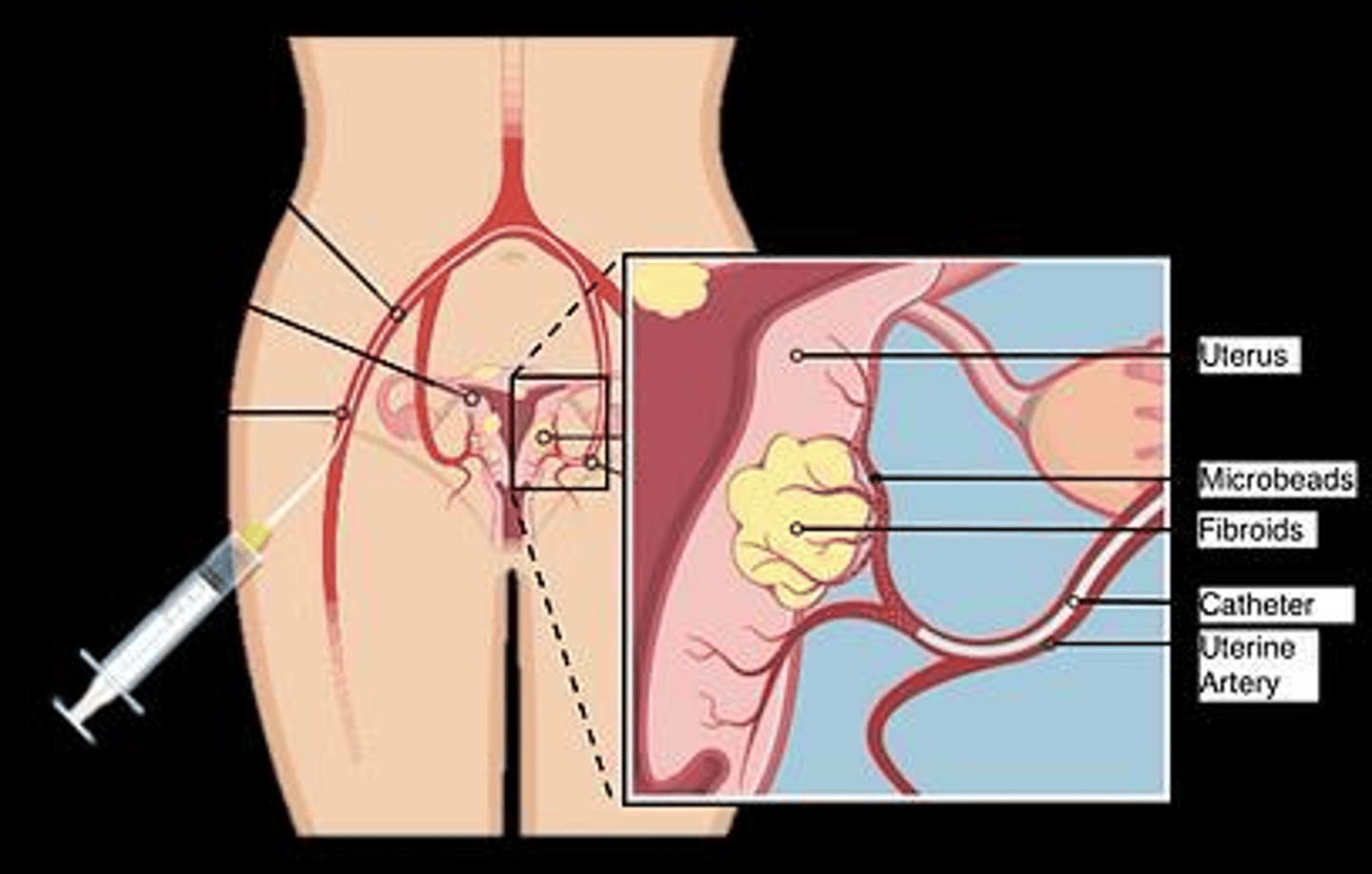
What is Uterine Artery Embolization (UAE) and why is it generally avoided in some patients?
It is a minimally invasive procedure that cuts off blood supply to fibroids; it is generally avoided in patients desiring future pregnancy.
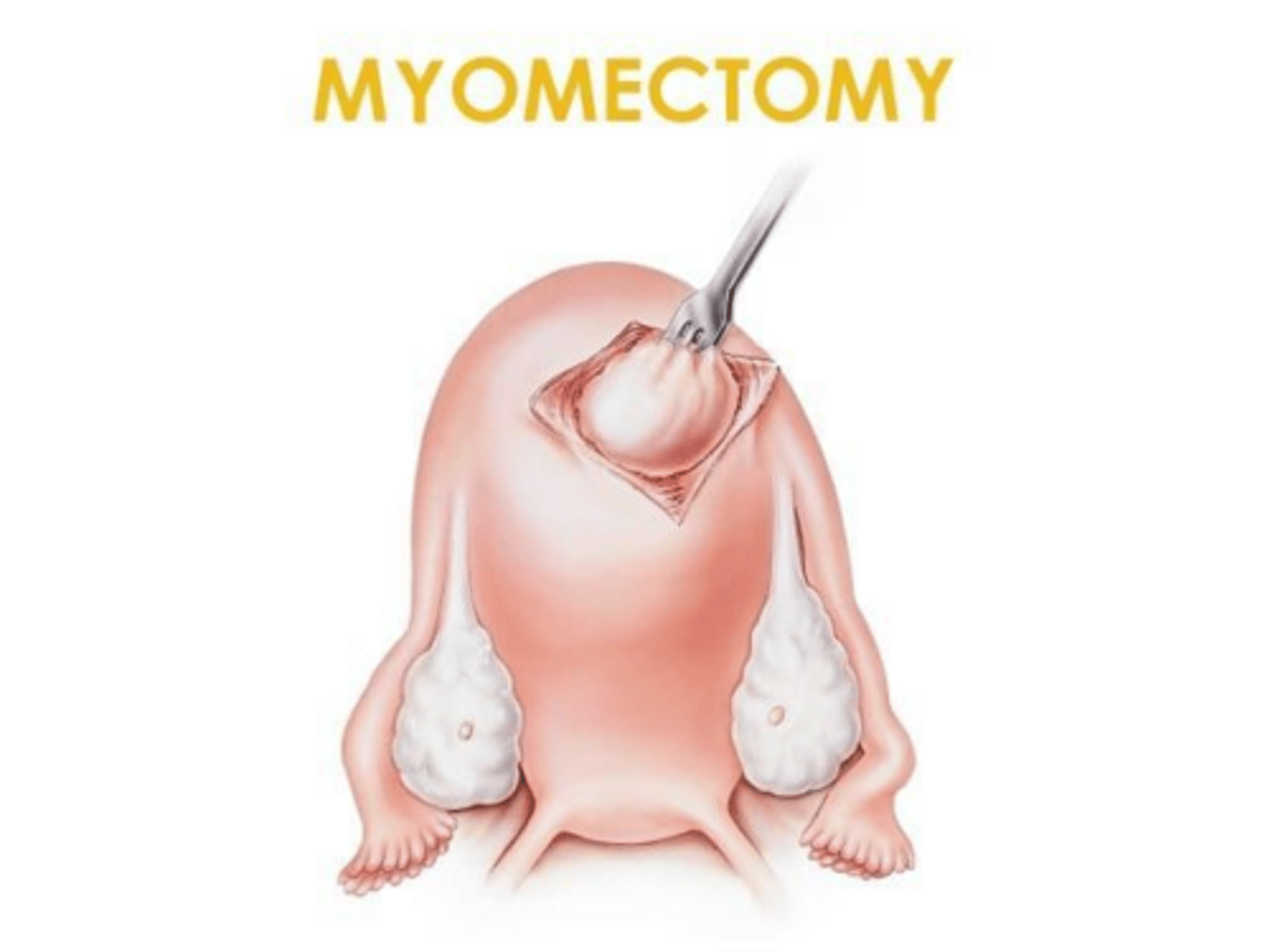
What is a myomectomy?
A surgical procedure involving the removal of fibroids only, preserving the uterus. Treatment of choice for patients desiring pregnancy.
What is the only definitive treatment of fibroids?
Hysterectomy.
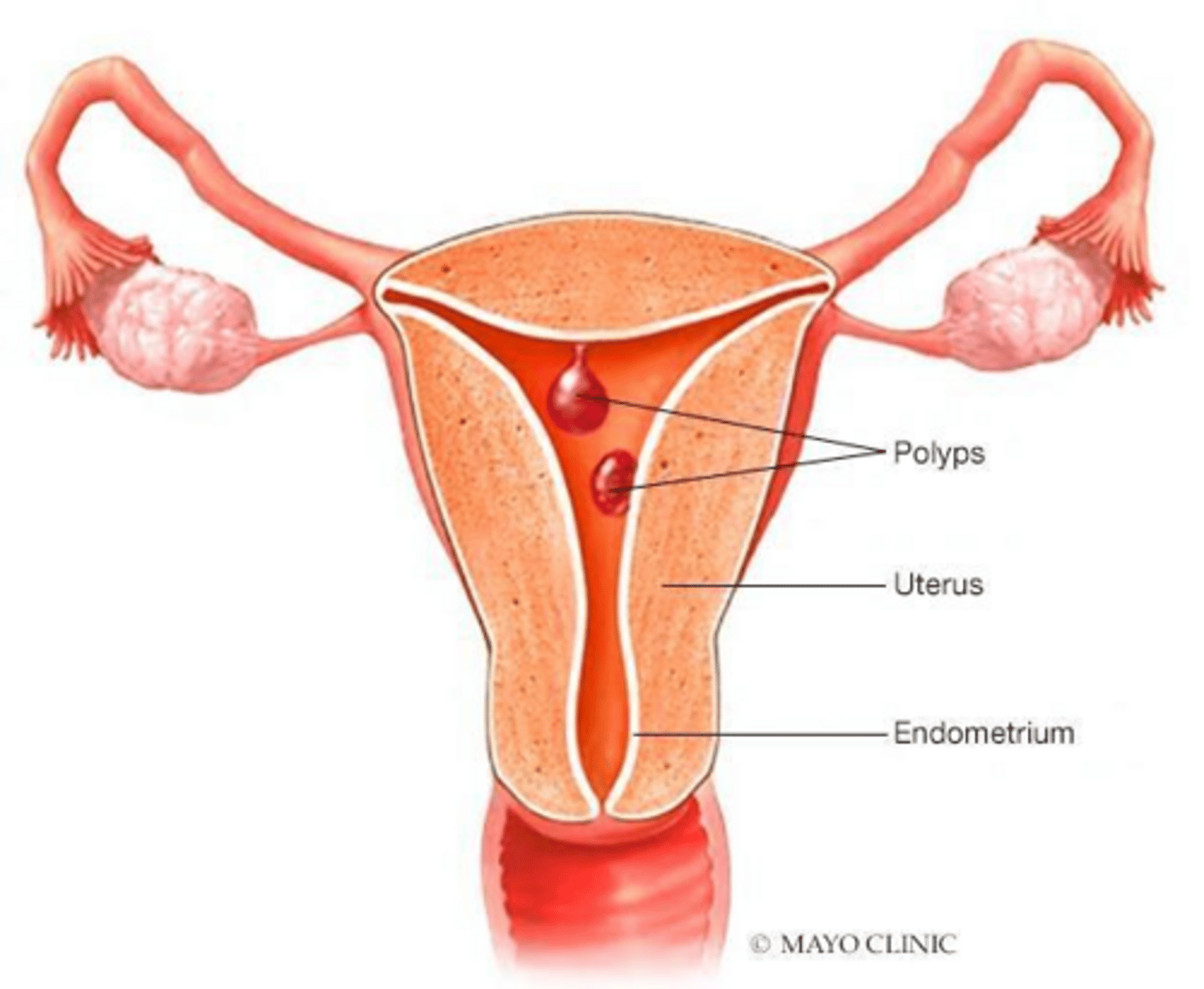
What are endometrial polyps?
Benign overgrowths of endometrial glands and stroma that form focal lesions in the uterine cavity.
What is the most common symptom of endometrial polyps?
Abnormal uterine bleeding. Though usually found incidentally!
How are endometrial polyps diagnosed?
Transvaginal ultrasound, confirmed with hysteroscopy and biopsy.
What is the management for symptomatic or postmenopausal endometrial polyps?
Polypectomy via hysteroscopy.
How is post-menopausal bleeding (PMB) defined?
Any vaginal bleeding occurring 12 months or more after the last menstrual period.
What is the clinical rule regarding post-menopausal bleeding?
Post-menopausal bleeding is considered endometrial cancer until proven otherwise.
What is the most common cause of post-menopausal bleeding?
Endometrial or vaginal atrophy.
What is the first step in PMP bleeding evaluation?
Characterize bleeding, assess risk factors and perform a pelvic exam.
What is the first-line diagnostic test for evaluating post-menopausal bleeding?
Transvaginal ultrasound to measure endometrial strip thickness.
What endometrial strip thickness (EMS) measurement has a high negative predictive value for cancer?
An EMS of 4mm or less. Greater than 4mm requires TISSUE BIOPSY!!
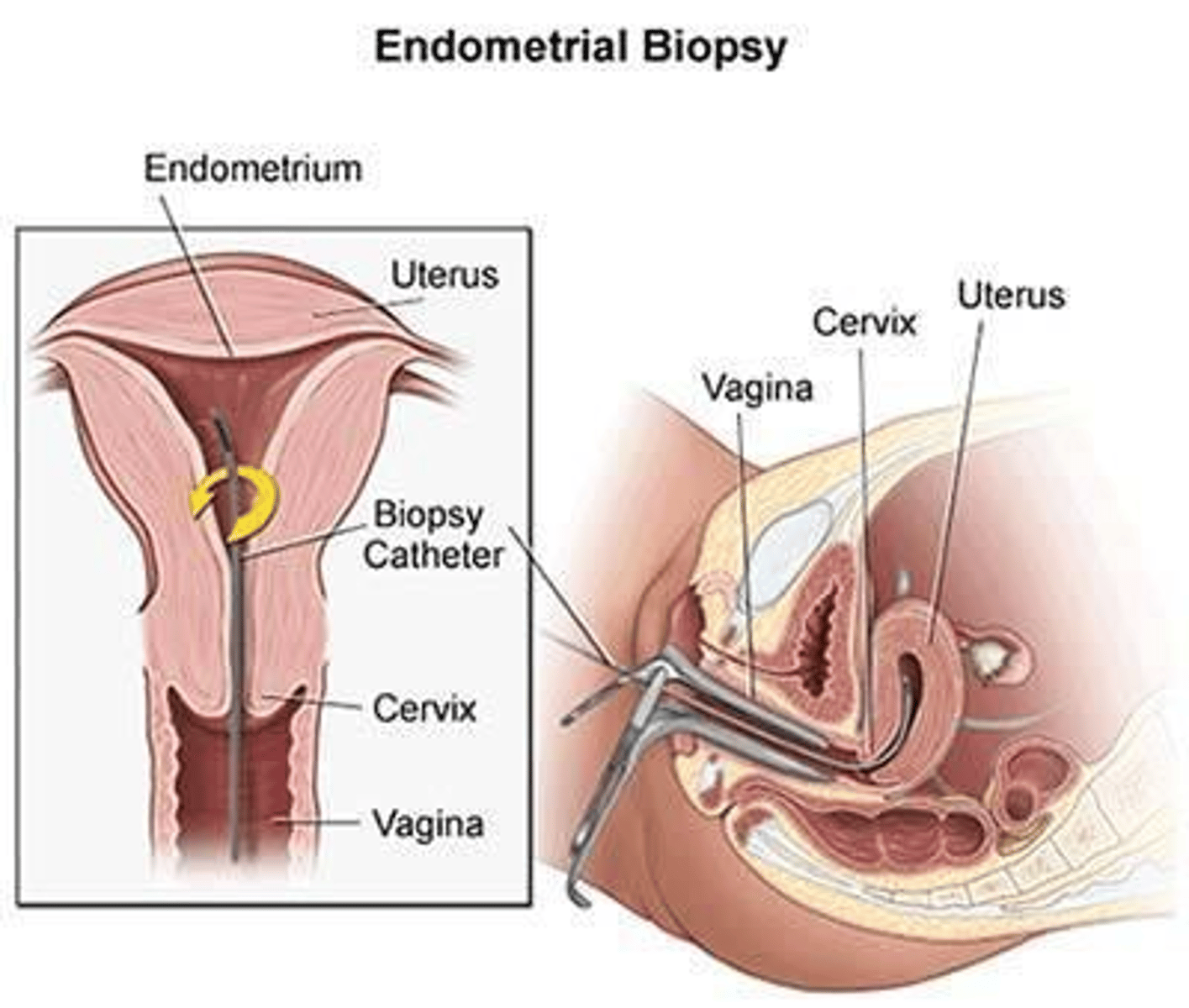
What is the preferred first-line tissue sampling?
Office EMB
What is the gold standard for uterine cavity evaluation if an endometrial biopsy is negative or shows hyperplasia?
D&C (dilation and curettage) with hysteroscopy.
Which GYN malignancy is the most common in the United States?
Endometrial cancer.
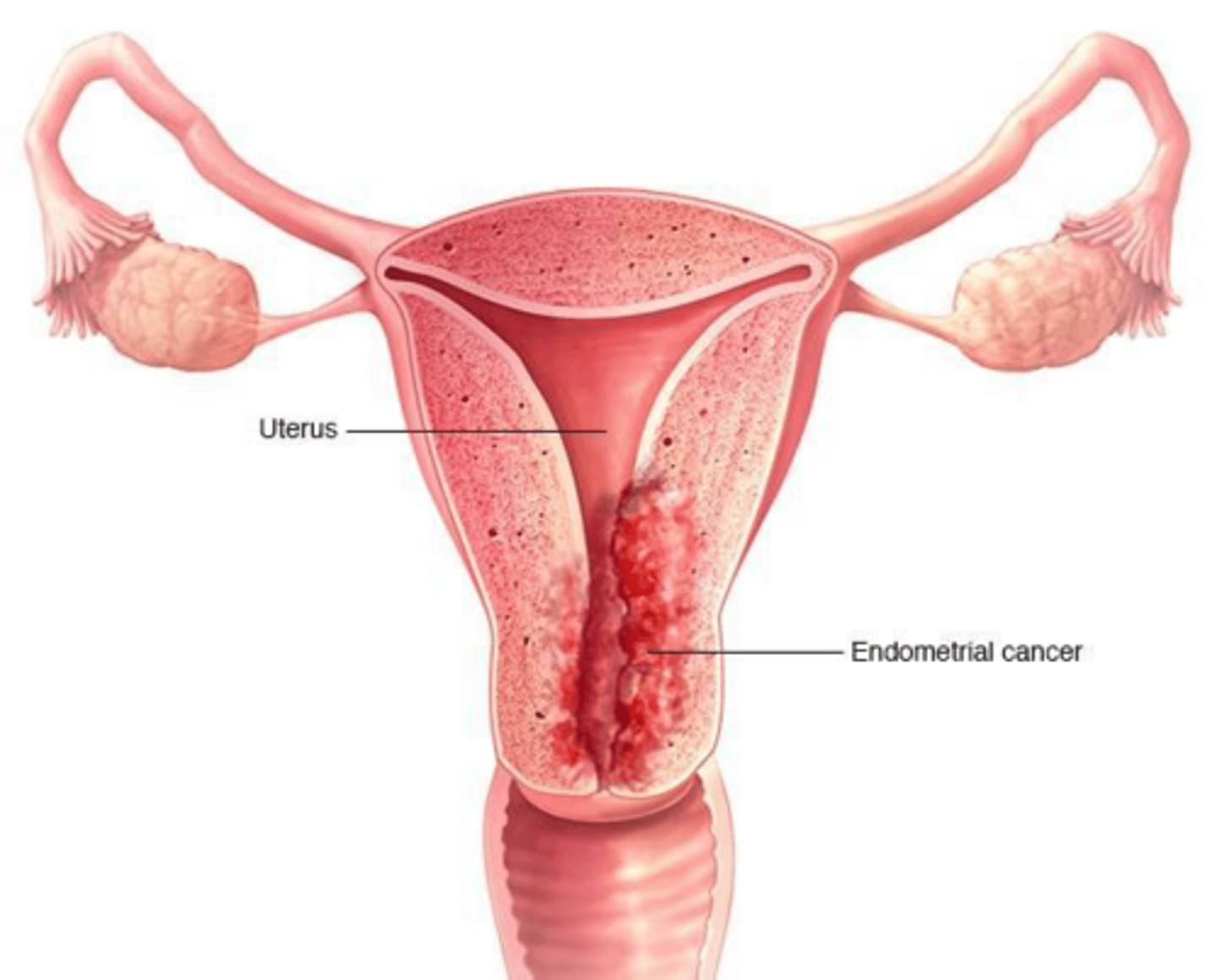
What is the 'Golden Rule' of endometrial cancer pathogenesis?
Unopposed estrogen stimulation of the endometrium. Chronic stimulation of the endometrium by estrogen without stabilizing/sloughing effect of progesterone leads to hyperplasia and potential malignancy.
Why is obesity a risk factor for endometrial cancer?
Adipose tissue contains aromatase, which converts adrenal androstenedione into estrone (peripheral estrogen).
How does Tamoxifen increase the risk of endometrial cancer?
It acts as an estrogen agonist on the uterine lining.
What is the primary non-hormonal genetic risk factor for endometrial cancer?
Lynch syndrome.
What are the characteristics of Type 1 (estrogen-dependent) endometrial cancer?
Arises from hyperplasia, associated with obesity/metabolic syndrome, low-grade endometrioid histology, and generally favorable prognosis.
What are the characteristics of Type 2 (estrogen-independent) endometrial cancer?
Arises spontaneously in an atrophic uterus, not associated with obesity, high-grade serous or clear cell histology, and aggressive prognosis.
Are there routine screening recommendations for endometrial cancer in average-risk women?
No, there is no routine screening indicated.
Why is a Pap smear not an effective screening tool for endometrial cancer?
It is designed for cervical cancer and is not a reliable tool for detecting endometrial malignancies.
What is the cardinal symptom of endometrial cancer?
Abnormal uterine bleeding.
What is the primary method for determining the official stage of endometrial cancer?
Surgical staging, which requires a pathologist to examine tissues removed during surgery.
What is the standard surgical management for Stage IA endometrial cancer?
Total Abdominal Hysterectomy & Bilateral Salpingo-Oophorectomy (TAH-BSO).
What is the standard management for Stage II endometrial cancer?
TAH-BSO plus pelvic/para-aortic lymphadenectomy, often with adjuvant radiation therapy.
What is the standard management for Stage III endometrial cancer?
Surgical debulking followed by combination chemotherapy and/or radiation.
What is the standard management for Stage IV endometrial cancer?
Palliative surgery, systemic chemotherapy and immunotherapy, or hormonal therapy.
What are the two most important prognostic factors for endometrial cancer survival?
Depth of myometrial invasion and the presence of lymph node metastasis.
Where do most endometrial cancer recurrences occur?
Locally (vaginal vault or pelvic side walls) or distantly (lungs/liver).
What is the recommended surveillance schedule for endometrial cancer in the first 2-3 years post-treatment?
Clinical exams (including speculum and rectovaginal exams) every 3-6 months.
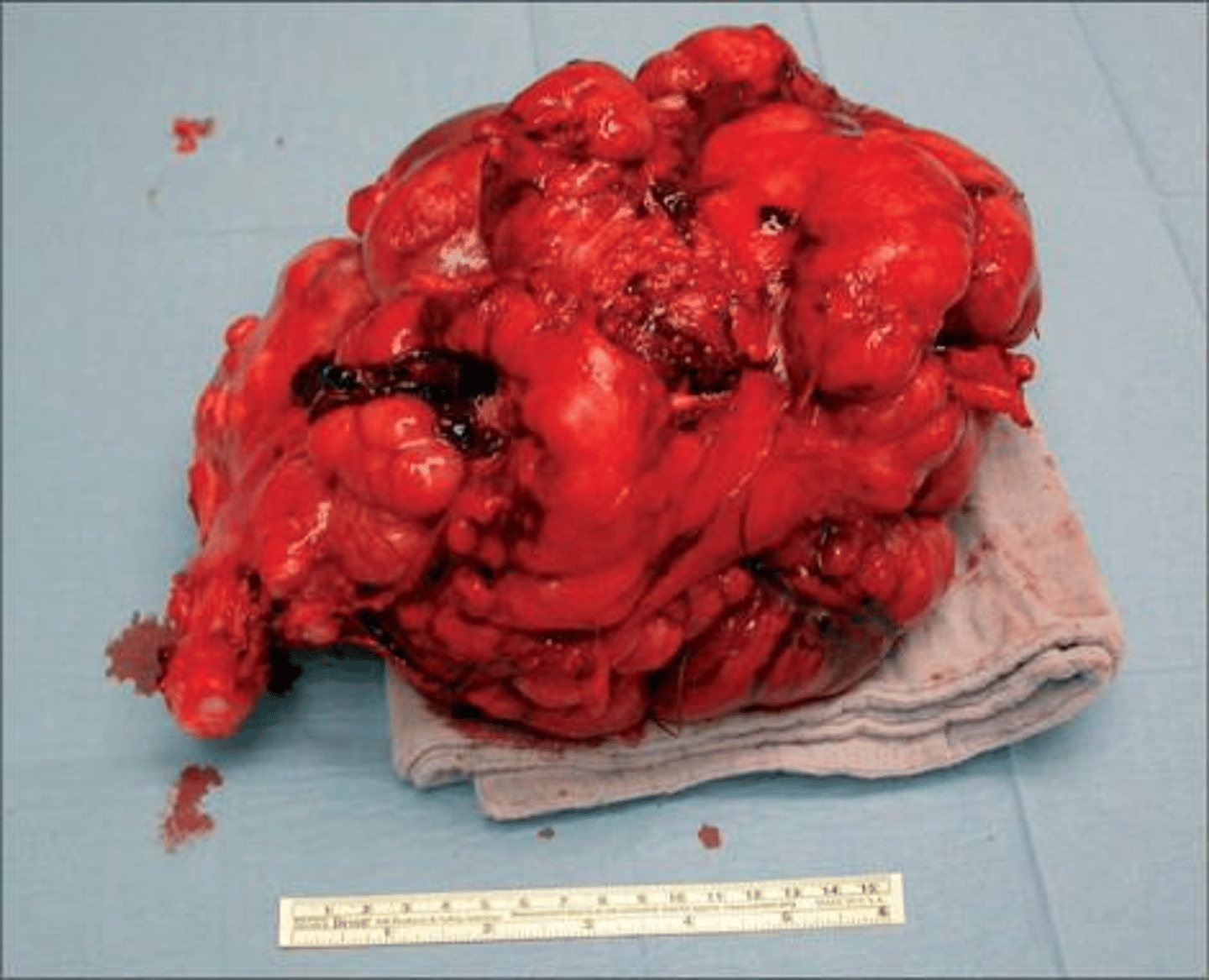
What are the primary characteristics of uterine sarcoma?
Rare (<5%), highly aggressive, arises from mesenchymal tissue, and carries a high risk of early metastasis.
What is the classic presentation of a uterine leiomyosarcoma?
A bulky mass that continues to enlarge after menopause, often accompanied by post-menopausal bleeding or pelvic pain.
What is the definition of Gestational Trophoblastic Disease (GTD)?
A spectrum of premalignant and malignant disorders arising from abnormal fertilization leading to proliferation of trophoblastic tissue.
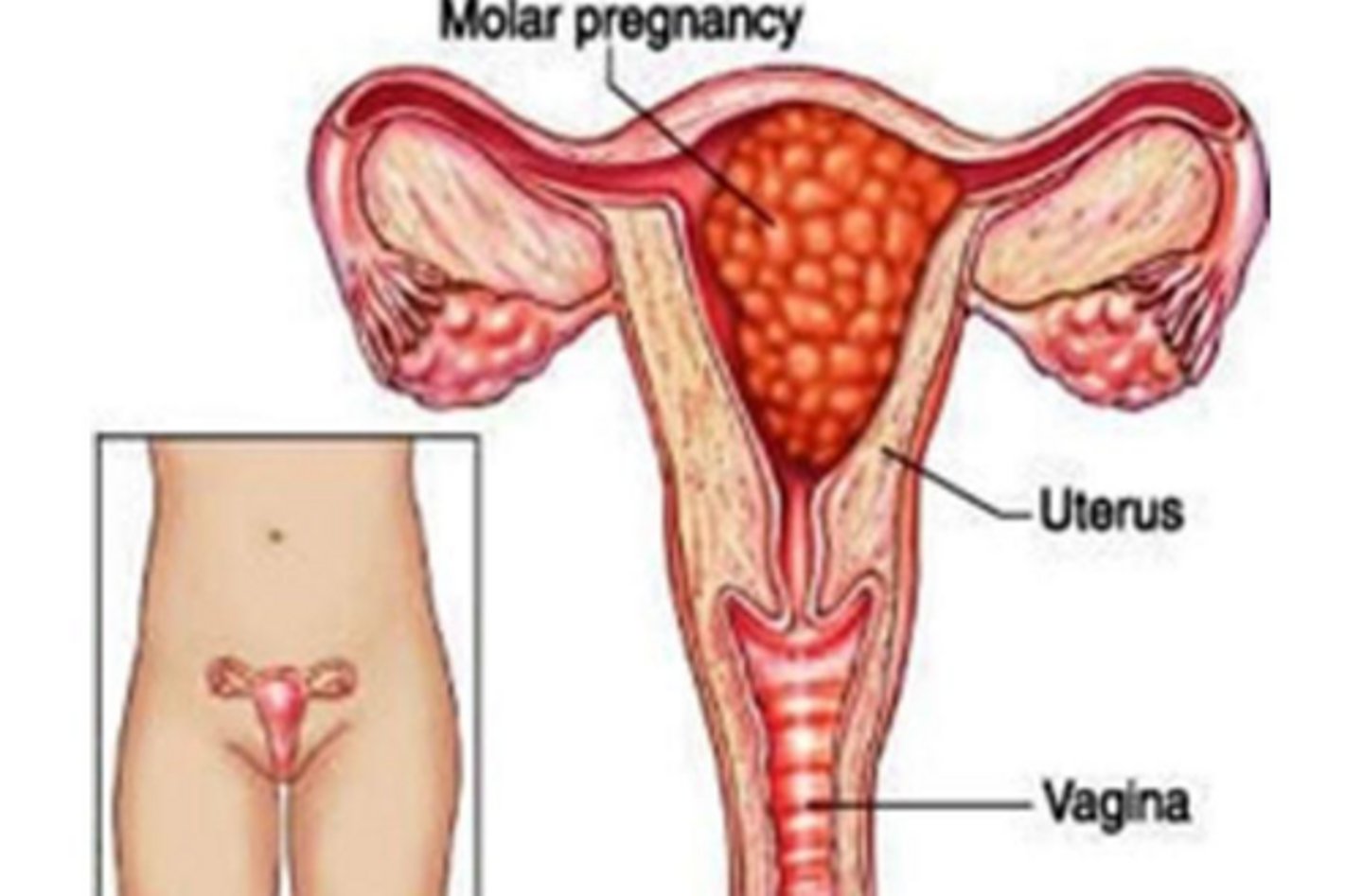
What is the most common type of GTD?
Hydatidiform mole, AKA molar pregnancy.
What is the pathogenesis of a molar pregnancy?
"Genetics of error" disease and is divided based on how the misfire in fertilization occured; either complete or partial.
What is the pathogenesis of a complete hydatidiform mole?
A "blank" egg (no maternal DNA) is fertilized by one sperm that duplicates its DNA.
What is the genetic composition of a complete hydatidiform mole?
46, XX or XY (all paternal DNA, maternal DNA is absent).
What is the pathogenesis of a partial hydatidiform mole?
A normal egg is fertilized by 2 sperm simultaneously.
What is the genetic composition of a partial hydatidiform mole?
69, XXX, XXY, or XYY (triploid, consisting of one maternal and two paternal haploid sets). Has fetal tissue but non-viable.
Which type of molar pregnancy has a higher malignant potential?
Complete hydatidiform mole (15-20% risk vs 0.5-5% for partial).
What are the three components of the classic clinical triad for molar pregnancy?
Vaginal bleeding in the first trimester, size/date discrepancy (uterus larger than expected), and extremely high b-hCG levels.
What is the most common symptom of a molar pregnancy?
Painless vaginal bleeding; often dark brown discharge or expulsion of grape-like vesicles.
What are 2 severe symptoms a woman might experience during a molar pregnancy?
Hyperemesis gravidarum (due to extreme b-hCG) and early-onset preeclampsia (before 20 weeks)
Why might a patient with a molar pregnancy present with hyperthyroidism?
Because b-hCG is a structural analog to TSH and can stimulate the thyroid gland.
What are theca lutein cysts in the context of molar pregnancy?
Bilateral, enlarged ovaries (>6cm) caused by excessive hCG stimulation.
What is the first step in a molar pregnancy workup?
Quant. b-hCG. Will be EXTREMELY elevated (>100,000) with complete mole, mildly elevated in partial mole.
What is the characteristic ultrasound appearance of a complete mole?
A 'snowstorm' or 'grapes' appearance due to hydropic villi, with no fetal tissue.
What is the characteristic ultrasound appearance of a partial mole?
A 'Swiss cheese' placenta with fetal tissue present.
Why is a baseline chest X-ray mandatory in the workup of a molar pregnancy?
To rule out lung metastasis, as choriocarcinoma is highly hematogenous.
What is the immediate management for a diagnosed molar pregnancy?
Suction Dilation & Curettage (D&C) and administration of RhoGAM if the mother is Rh-negative.
What is the required surveillance protocol for b-hCG following molar pregnancy evacuation?
Weekly measurements until undetectable, then monthly for 6-12 months.
Why is strict contraception required for 6-12 months after molar pregnancy treatment?
To prevent a new pregnancy from raising b-hCG levels, which would mask the potential return of malignancy (Gestational Trophoblastic Neoplasia).