1: Disorders of the eyelids
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
anterior blepharitis
chronic inflammation of the eyelash and follicle and its associaated gland
can be due to infection, infestation or inflammation such as staphylococcal bacteria, demodex mites or seborrheic
very common in population and most age groups
symptoms are typically worse in the morning
what is blepharitis often caused by
meibomian gland dysfunction. blovkage of gland pores can result in inflammation, sometimes complicated by bacterial infection
risk factors of anterior blepharitis
skin conditions such as rosacea, oily skin, dandruff, or sebhorric dermatitis
posterior blepharitis ( mixed blepharitis )
atopia/allergenic
eyelid mites and lice
make upuse and CLs use
environment being cold or dry, use of air con or open fires
some meds eg cancer drugs or topical drugs
systemic disease eg diabetes
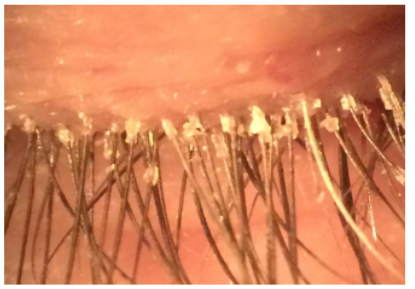
clinical presentation of anterior blepharitis
might include crusting at the lash base and erythematosus of the lid margin. it can become a chronic condition that required periodic treatments with hot packs, lid scrubs and antibiotic ointment.
symtopms of anterior blepharitis
variable and unreliable: poor correlation between signs and symtoms
tend to get flares of remission and exacerbation eg comes and goes in waves
discomfort and eye rubbing
worse on awakening, crusty feeling in eyelashes and around the eyelids
associated with dry eye and wet eyes
burning and grittiness
mild photphobia
signs of anterior blepharitis
bacterial:
hard scales and crusting and collarettes
mild papillary conjunctivitis
lash loss, notching of margin, trichiasis
seborrheic:
hyperaemic and greasy crusting of lashes
posterior blepharitis involvement
demodex:
mites seen and cylindrical dandruff and collarettes
papillary conjunctivitis and red eye
treatments of anterior blepharitis
depends on the type as to what treatment is given
not alays effective but contols symptoms effectively
warm compress and eye bag
lid cleaning
tea tree oil lid wipes
antibiotics- topical ointments and oral doxycycline
novel treatments such as ciclosporin, light therapies
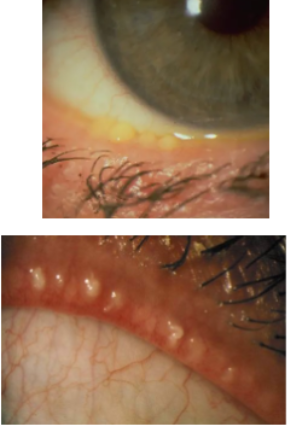
posterior blepharitis/ meibomian gland dysfunction
posterior lid inflammation, and typically due to meibomian gland dysfunction
glands either do not produce good enough meibum/oil or stop producing oil. This is typically down to th increase in melting point of these oils, meaning they can cause blockage and increased risk of infection and inflammation
increases tear film evaporation, and symptoms of dry eye like irritation, reflex tearing
is chronic and requires regular management

symptoms of posterior blepharitis
tend to get flares of remission and exacerbation eg comes and goes in waves
discomfort and eye rubbing
associated dry eye and watery eyes
burning and grittiness
mild photophobia
signs of posterior blepharitis
capping on glands seen, oils appear more firm and yelow
glands may also e recessed or plugged; notching
hyperamia and telangiectasia around posterior lid margin
pressure onto the lids causes secretion to be thick like toothpaste
tear flm very oily or foamy and unstable
tear break up time is very short
treatments of posterior blepharitis
warm compress and eye back ; 2x a day for 5 mins
omega 3 and 6 supplements
eyelid massage and lid treatments such as BlephEx
lifestyle changes ; blinking exercises , optimising VDU and use of heaing
eye drops / lubricants foir when needed and gels for the evening
if sevre, antii inflammatory meds

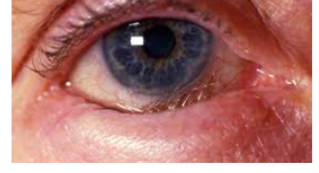
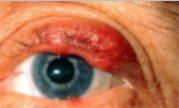
ectropion
associated with aging due to horizontal eyelid laxity
everson of eyelid
common cause of which loss of muscle tone
as lid margin falls away from its position agaainst the globe. the lacrimal punctum is no longer in position to drain tears from lacrimal lake.
epiphora
overflow of teas onto the cheel , may occur, cauing maceration of delicate skin in this area
ectropion symptoms
exacerbation of any ocular surface discomfort or diease
poor cosmesis
tarsal plate becomes inflamed, thickened and keratinised
corneal scarring and epithelial defects
epiphora
management of ectropion
initial magament may be topical lubricants and lid hygeince, but in time most reqire srgert for treatment, where the ld can be excised and pulled together to tighten. routine referral is indicated
entropion
inversion of the lid margin, usually bottom lid
may result from spasm of the orbicularis oculi muscle causing the lid margin to turn inwards. this inward turning puts the eyelashed in contact with the globe and can cause corneal abrasion.
scarring of the lif after trauma can also cause entropion
also polapse of orbital fat into lower lid can cause
synptoms of entropion
stinging. itchy , severe pain and potophobia
signs in ectropion
trichiasis, deep and perfuse corneal staining, red eye, epiphoria, inflamed lids
requires more urgent treat,ent and referral 2/52 due to severity
can try bandage CLs, chemodenervation
end result is surgery and should be prioritised
lash disorders
trichiasis: eyelashes growing in abnormal directoion , usually into the eye, toward the palebral fissue
distichiasis : additional rw of eyelashes
eyelashes loss and drop out
contact with the cornea can cause irritaation and painful abrasions and can lead to ulceration

chalazion
localised, non infectious and sometimes painless swelling of a meibomian gland, often caused by an obstructed duct. the gland may extrude its secretion into surrounding tissue, setting up a grabulomatous inflammation.
most common on top lid due to number of meibomian glands

chalazion
when incerting the lid, the tarsal surface will not be smooth as expected but have a irregular nodule or cobblestone like appearance
risk factors include prior blepharitis, meibomian gland dysfunction, and those that have sebhorreic dermatitis or rosacea
can resolve spontaneously but can take a ew months
management of chalazion
reassure px and advise them to use an eye bag or some hot compress for at least 5 mins
sometimes lid massage lightly with findgers can help with the swelling
managment has 40% sucess rate
after 4 weeks, referral may be possible. HES will either use steriod injection to reduce inflammation or perform surgical excision.
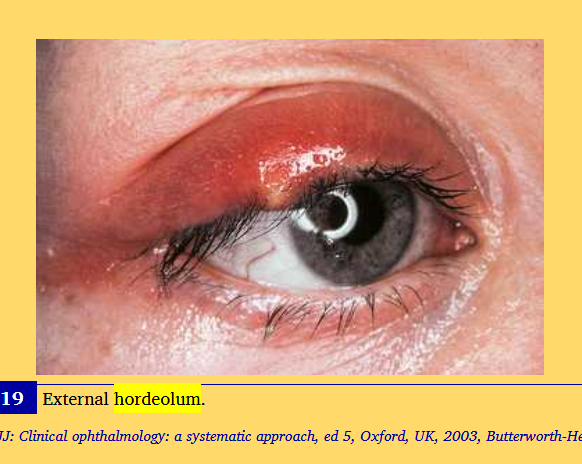
hordeolum
stye
acute inflmmation of an eyelid gland, usually caused by staphylocci
an infected zeis or moll gland is called an external hordeolum or common stye
a localised infection of a meibomian gland usually drains from the inside surface of lid thus called an internal hordeolum
external hordeolums are of the glands of zeis. more prominent anteriorly and on naked eye observation
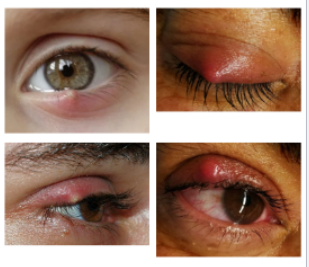
symptoms of hordeolum
because theyre infected, can be painful and filled with mucopurlent pus
anterior and posterior form a nodular mass and a large redder amount of inflammation than a chalazion
pain, tenderness, swelling and a burning sensation
more painful for an internal hordeolum
management of hordeolum
to soften the coagulated material and allow it to drain
most likely to resolve spontaneously in a fortnight so it may be bezt to monitor and refer it if it doesnt resolve in 3 weeks
if it doesnt resolve in 3 weeks, antibiotics may be prescribed as it may inctease the risk of cellulitis
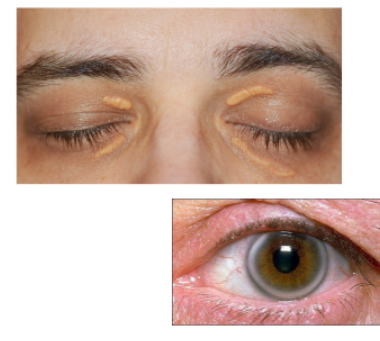
xanthalasma
raised plaques that may look nodular and have a yellow like tinge
accumulation of lipid under the skin
not symptomatic although px can findit cosmetically unappealing
often idiopathic, although 1/3 of px with it tend to have an arcus and high blood lipids/cholesterol
typically medial and bilateral but asymmetric
more frequ in older px , rare in those under 50
management of xanthalasma
is to reassure px and to refer to GP non urgently for lipid evaluation blood test if not done recently
treatment is surgical and only cosmetic as it has a high rate of recurrence
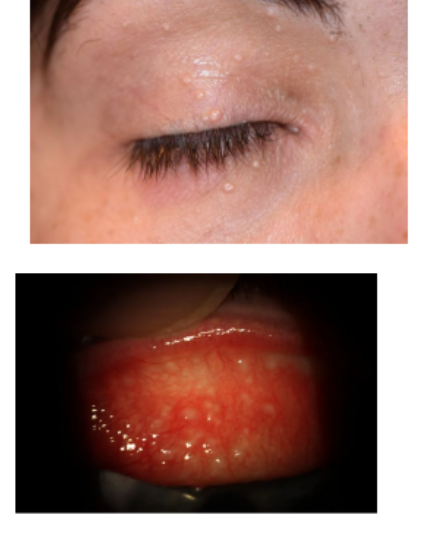
mollescum contagiosm
type of virus that can infect skin, giving pink/flesh coloured bumps that can have a central crater
usually in clusters but can be in isolation. can be found around the body
rarely symptomatic but if any infection enters the eye it can cause viral conjunctivitis like symptoms with follicles on the tarsal conjunctiva
discharge if popped is watery
tends to get worse before bettem but relsoves spont over the course of a couple months
management mollescum contagiosm
reassure px
refer if doesnt get better after 1-2 years but no treatment usually necessary, just adivse on hygeine and reduction of transmission
treatment can unclude removal and cauterisation
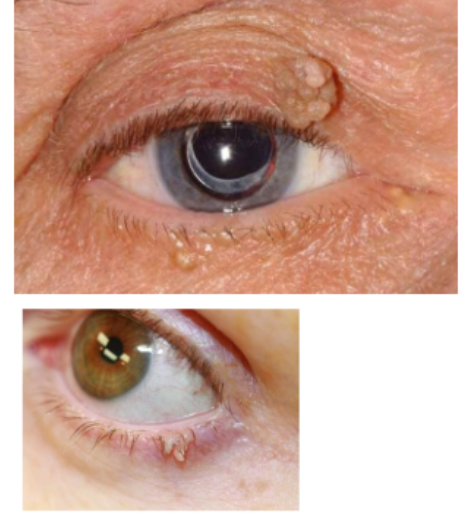
squamous papilloma
commonly referred to as a skin tag and can occur around the body , including genit tongue eyelid and face 7more common around body in obese people but no real aetiology/ risk factor increase for those with eyelid ones
can be brownish or flesh coloured and has larger viewable size and can appear nodular and/or finger like with its projection
most common when people get older
minimal risk treatment is only cosmetic, and is surgical excision
tumours
benign or malignant
benign is abnormal but noncancerous collection of cells that may or may not be progressive in its size. dont use terms like tumor in front of px until certain
when investigating a lump or bump or anything unusual in the eye, we want to ensure we can rule of the risk of it being malignant.
if malignant: invade local tissue, spread and grow, progresses and invades adjacent tissue
most eyelid lesions are benign, which dont metastasis

malignant tumors
malignant lesions tend to ulcerate ie cause a breakage or cratering of the skin
malignant tend to not be painful to touch and dont feel tender to px
malignant tend to be firm to the touch
tend to not be different colour
malignant tend to be irregular and asysmetric
malignant invade and destroy tissues eg uvea, retina
causes tellangiectasia : can see blood vessels on the face
can have rolled translucent margins that are shiny and whitish in appearance known as pearly borders
can sometimes have feeder vessels, ie cause blood supply to look aggravated

basal cell carninoma
most common form of skin cancer.
associated with sun exposure so more common in those liviing in sunny climates
associated also wit older people around 60s
very variable, clinical appearance but can have an ulcerated centre, pearly margins, raised edges
progression takes a long time eg 5 years and metastases are rare, worth asking px to look at their older photos and try to assess change
can be invasive and locally destructive so still requires referral

squamous cell carcinoma
second most common form of malignancy
difficult to diffrentiate betwween BCC and SCC , it depends on which layer of the skin it originates from,- this comes from a more internal layer making it more likely to spread and grow
appears more like hard scaly dead skin than BCC however it is not easy to diagnose
requires more urgent referral for confirmation 2/52, but as it is difficult to distinguish this is why we referral all suspect malignancy inclduding BCC urgently as to ensure that we do not delay potential care if scc is present