Cow Qs
1/17
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
18 Terms
1. LDA - Left displaced abomasum
2. Empty rumen with large gas cap - rumen pings
Sunken eyes & skin tent = cow is dehydrated
Smelly vaginal discharge, open cervix & difficulty performing rectal = indicates infection (metritid)/retained placenta
High heart rate & resp rate - animal is in pain
Pings - indicative of gas collection, could be rumen pings (unlikely given symptoms)
From clinical signs think cow is suffering from LDA
What does each of the clinical signs mean?
Give your diagnosis based on clinical signs
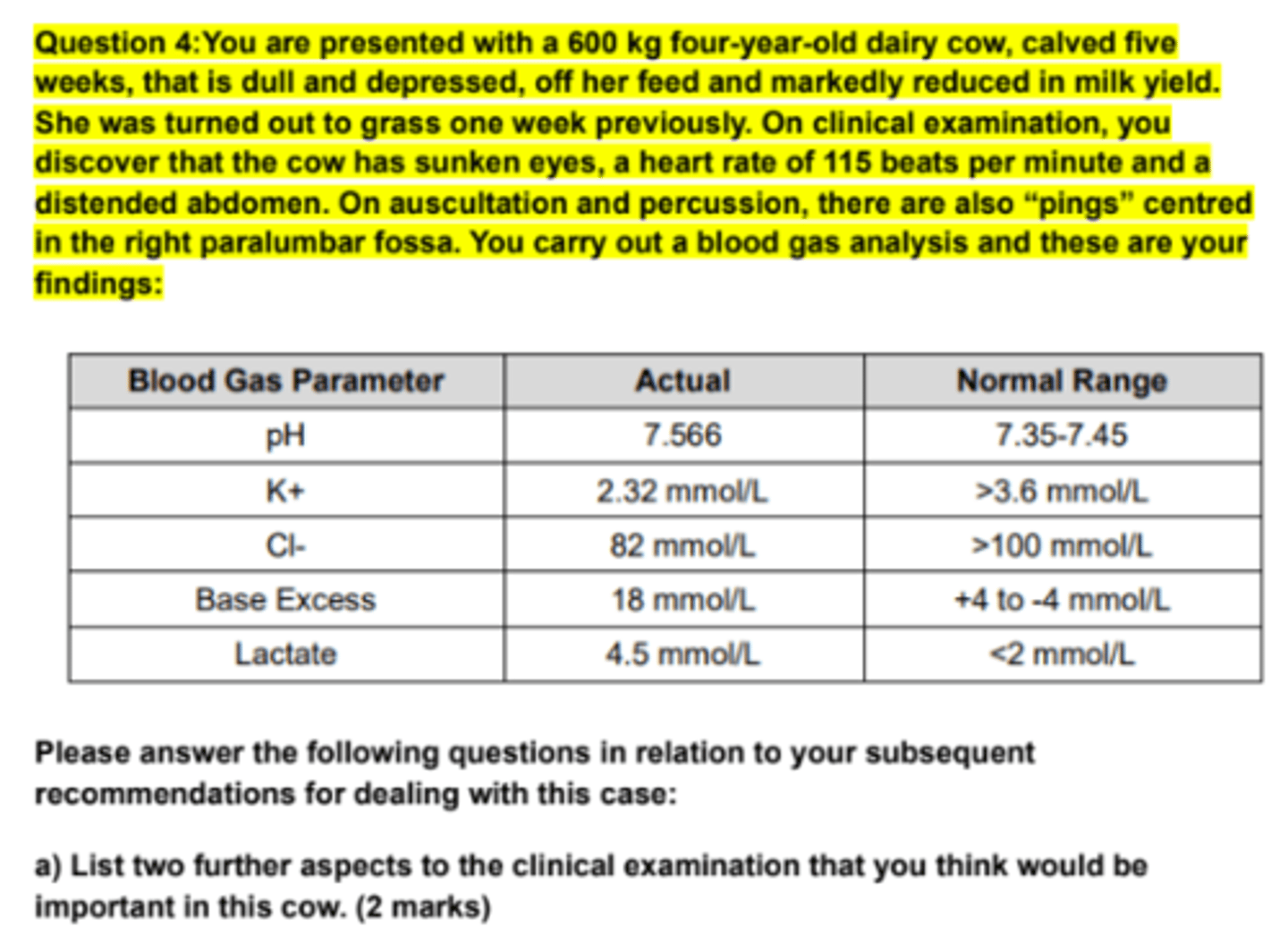
- Ultrasound
- Take a blood sample
- Ballottement and auscultation
What further clinical examination steps would be important to perform in order to
help with your diagnostic assessment? (2.5 marks)
- Liptack test to measure the pH of the aspirated fluid.
- Blood lactate
What further diagnostics, apart from the clinical examination, may help you in
reaching a diagnosis? (1.5 marks)
- Likely to have alkalosis
- High pH
- Base excess increased
What electrolyte and acid-base balance problems are likely in this case? (1 mark)
Vagal indigestion syndrome
Chronic
Acute or chronic condition?
Traumatic reticuloperitonitis, causes abscesses that interfere with motility
What is the most common cause of this syndrome in cows?
Peritoneal fluid analysis will support if peritonitis present, the total protein or nucleated cells will increase.
A lateral radiograph should be performed to identify if there is a foreign body present, or a reticular abscess.
An ultrasound of the abdomen (cranioventral) will indicate if focal
peritonitis is present and examine the reticular contraction rate.
For a definitive diagnosis, explorative surgery is required (left paralumbar fossa laparotomy and rumenotomy).
Describe how you would further investigate, using both clinical examination and
diagnostic techniques, whether this particular cause was a factor in this case? (4
marks):
I believe that the cow is suffering from Omasal transport failure due to traumatic reticuloperitonitis, which is type II vagal indigestion.
Left paralumbar fossa laparotomy and rumenotomy
will help to identify and remove any foreign materials present.
Antibiotic therapy and supportive therapy should be given after
the surgery.
Your investigations confirm that this syndrome was caused by the common factor
you suspected. What are the potential treatment options in such a case as this? (3
marks):
Ballottement
Rectal exam
Caecal dilation
Caecal torsion/volvulus
List two differential diagnoses for the abdominal problem with this cow. (2 marks)
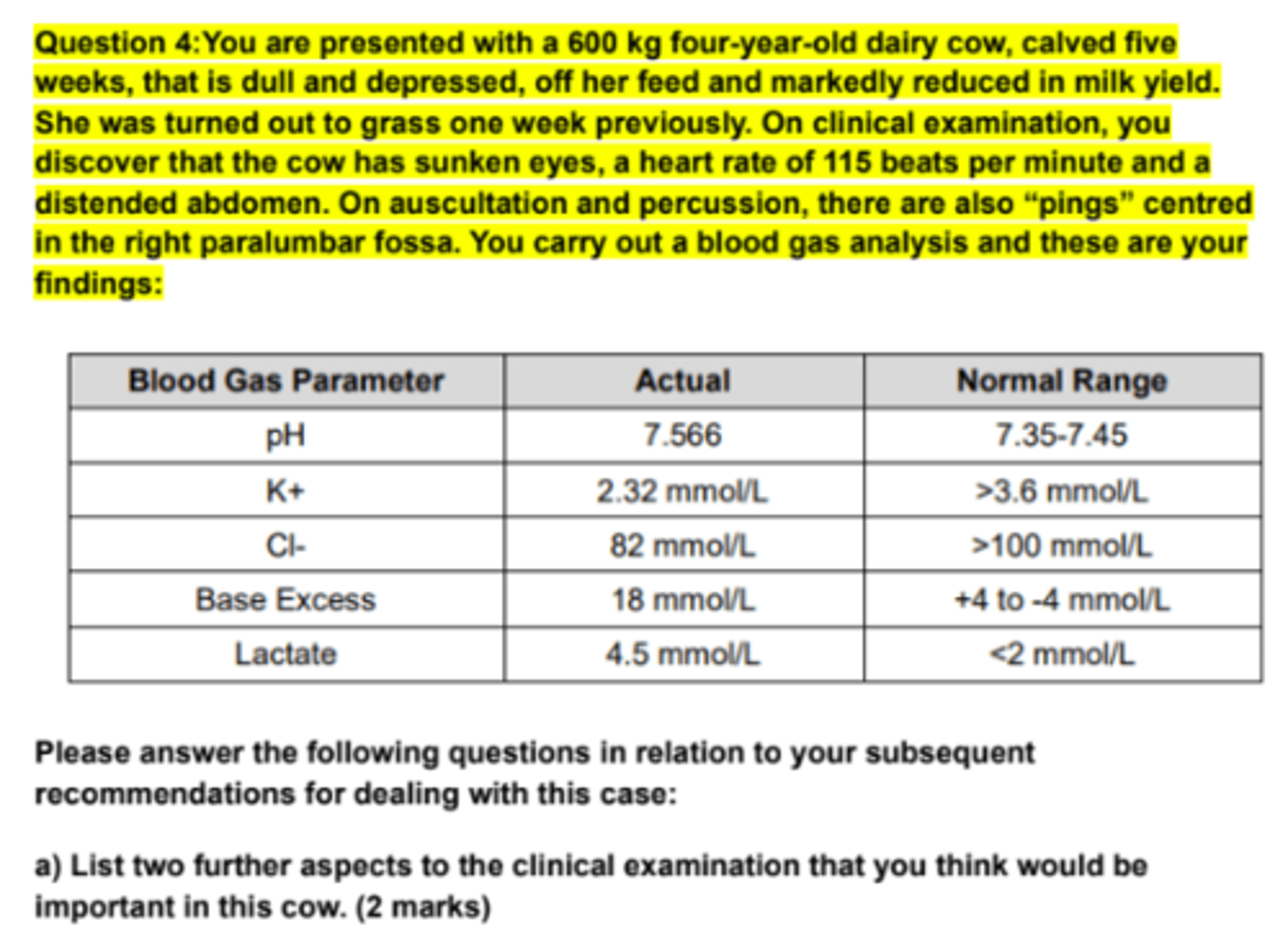
Hypocalcemic: The chloride is being sequestered in the abomasum leading to a drop of
negative ions in the blood.
BE: Bicarbonate is being produced by the kidneys to compensate for the loss of anions.
However this leads to a metabolic alkalosis.
Hypokalaemic: The metabolic alkalosis causes an exchange of K+ ions into the intracellular
fluid to stabilize blood pH. This ionic transfer rapidly leads to hypokalaemia.
Describe the major electrolyte and acid-base changes that are apparent on the
blood gas analysis of this cow as outlined in the table above. (1 mark)
increases in plasma L-lactate are most commonly caused by
poor systemic tissue perfusion because of dehydration, shock, endotoxemia, or a
combination of these conditions, as well as local hypoperfusion such as splanchnic
ischemia and abomasal necrosis seen in cows with abomasal volvulus
Comment on the blood lactate concentration as outlined in the blood gas analysis
results. (2 marks)
Correct hypocalcemia
increase fibre length
Decrease concentrates
Describe your post-op medical management of this cow.
Changes
Grossly
Microscopically
How does it cause diarrhoea?

Type-2 ostertagiosis: Fecal sample or pepsinogen in serum
Johne's disease (paratuberculosis): Serology (ELISA but low sensitivity) or fecal culture
(Herrold's egg yolk medium)
For each of these diseases give one diagnostic test that might assist in their
diagnosis ante-mortem.
The parasite causes the abomasum to take on a "moroccan leather"/ "cobblestone"
appearance in heavy infections. This appearance is due to the worms feeding and the
individual lesions they create eventually coalesce and give the abomasum this rough texture.
These lesions may be accompanied by a rise in pH (6-7). This means pepsinogen will no
longer be converted to pepsin as it requires a much lower pH (2.5-5). This results in the
subsequent leaking of pepsinogen across the damaged epithelium that will lead to increased
plasma levels. Adult Ostertagia can also cause hypersecretion of pepsinogen compounding
the issue. The increased pH also stimulates the production of gastrin which will cause
inappetence.
In severe cases such as above oedema is usually marked and can extend over the
abomasum and into the small intestine and omentum causing the ascites and oedema.
Why an 18 month-old bullock/steer with chronic abomasitis due to ostertagiosis
develops dependent oedema, ascites and inappetence? (pathology)