Phys final
1/90
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
91 Terms
Reticulocytes
immature RBCs
main Plasma proteins
albumin, fibrinogen, immunoglobins
albumin
plasma protein that drives osmotic pressure
Platlets
cellular fragments that come off of megakaryotes to aid platlet plug formation/coagulation
basophils
have granules with histamine (inflammation/allergies) and heparin (anticoagulant)
Blood cell formation
Lt-HSC → St-HSC → committed stem cells → specific cells
cytokine
cell-stimulating factor that helps differentiate blood cells
Erythropoiesis
production of RBCs in the red bone marrow when when stimulated by erythropoietin (released when blood O2 drops)
Anemia
decrease O2 delivery due to blood loss, RBC destruction, or decrease RBC production
polycythemia
an increase in hematocrit from sustained hypoxia/doping leading to increase blood viscosity, vascular resistance, and blood pressure
Fibrinogen
plasma protein that interacts with blood to increase viscosity
platelet plug formation
adhesion → activation → aggregation
intrinsic coagulation pathway
Factor XII → XIIa when exposed to platelets or a negative surface (collagen)
extrinsic coagulation pathway
Factor VII → VIIa when exposed to thromboplastin
final common coagulation pathway
Factor Xa + Va + Ca+ + phospholipids → prothrombinase
Thrombin
converts fibrinogen into fibrin which then traps blood cells (clot)
tissue plasminogen activator
activates plasminogen into plasmin which then breaks down clots
fibrinolysis
breakdown of clots via plasmin
Neutrophils
migrate to tissue to become macrophages
Phagocytosis
adherence→ destruction → respiratory burst
macrophages
destroy foreign material via phagocytosis
NK cells
non -specific killer cells that kill cells without a “self marker” and also enhance inflammatory response
antimicrobial proteins
interferons and compliment proteins
compliment proteins
form the membrane attack complex (insert pores in pathogens leading to cell lysis), promotes opsonization, amplify immune response
Interferons
released by infected cells and bind to neighbor cells to block viral reproduction, activates macrophages and NK cells
APCs
engulf and present foreign particles to T cells via MHC II proteins
dendritic cells
macrophages
B cells
MHC proteins
display self-antigens and present foreign antigens to T cells
MHC 1 - hold endogenous antigens and display to CD8 cells
MHC 2 - present to CD4 cells
Antibodies
binds to specific antigens to form antigen-antibody complex which inactivates and tags antigens for destruction for innate defenses
actions of antigen-antibody complex
neutralization (cover binding sites)
agglutination (clumps antigens)
precipitation (insoluble complex forms precipitate)
complement fixation
compliment fixation
antibodies bound to cells expose the compliment binding site leading to a change shape → cell lysis, enhance inflammation, opsonization
active humoral immunity
B cells encounter an antigen and produce antibodies
passive humoral immunity
antibodies acquired from and extrinsic source (serum injection/ moms blood through placental barrier)
CD receptors
assist cell-to-cell interactions
CD4 → MHC II
CD8 → MHC I
Humoral immunity
antigen activated B cells → plasma cells → antibodies
CD4 cells
create memory cells and differentiate into Th cells
CD8 cells
create memory cells and differentiate into Tc cells
Th cells
release cytokines → stimulate innate immune system
stimulate CD8 cells
stimulate B cells
Tc cells
kill cells by releasing perforins (create pores) and granyzymes (enter cell and stimulate apoptosis)
pressure flow relationship
there is a critical closing pressure of the vessels that must be overcome to allow blood flow
pressure resistance relationship
as resistance decreases driving pressure increases in a logarithmic curve
(veins are much more compliant than arteries)
compliance of vessels
the ability expand to hold a larger volume and therefore have less change in transmural pressure
Law of LaPlace
the equilibrium between collapsing force (tension) and the blowout force (transmural pressure) depends on vessel radius
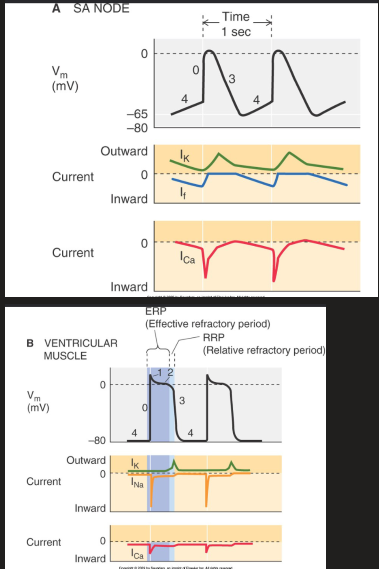
Heart depolarization
SA node → atrial muscle → internodal pathways → AV node → bundle branches → purkinje fibers → verticular muscles
Phases of heart depolarization
depolarizing upstroke - slow with Ca2+ (pacemakers), fast with Ca2+ and Na+ (contractile cells)
rapid repolarization (contractile cells) - inactivation of Ca2+ and Na+ currents
Plateau phase of ventricular muscle - continued Ca2+ and Na+ influx to lengthen refractory period
repolarization - outward K+ current
Diastolic potential - stable RMP (contractile cells), pacemaker potential (pacemakers)
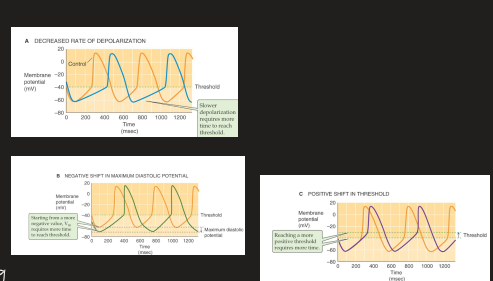
Modulation of pacemakers
decrease steepness of pacemaker potential
more negative diastolic pressure
more positive threshold
ECG Waves
P wave - atrial depolarization
QRS - ventricle depolarization
T - ventricle repolarization
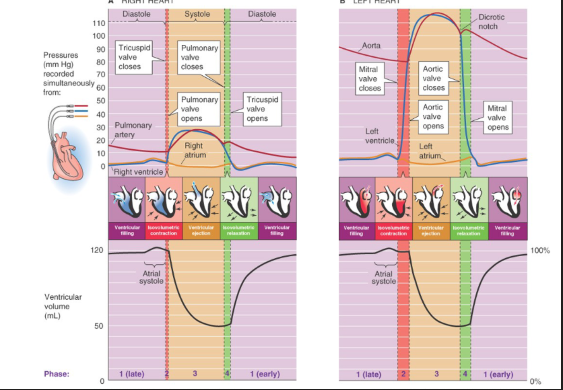
Cardiac cycle flow
Pulmonary veins/Vena cava → L/R Atrium → mitral/tricuspid valve open (AV) → L/R Atrium → Aortic/Pulmonary SLV open → outflow
Phases of cardiac cycle
ventricular filling→ isovolumetric contraction → ventricular ejection → isovolumetric relaxation
Starlings law
increased venous return → increased myocardial stretch → increased stroke volume
Factors affecting heart cardiac output
heart rate (filling time)
preload (starling law)
afterload (background aortic pressure)
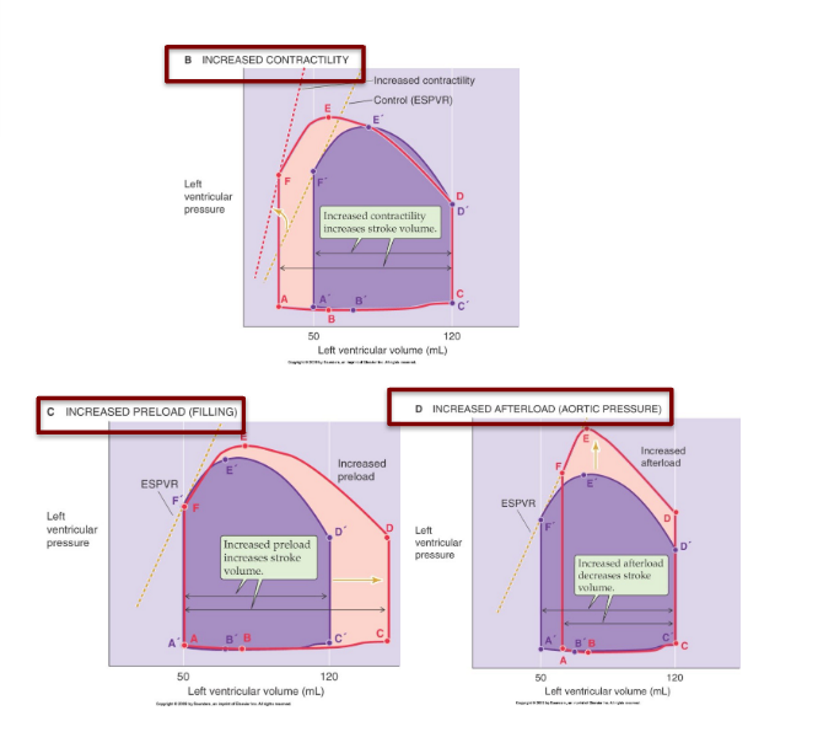
preload
the end-diastolic volume
afterload
pressure needed to open semilunar valve
Atrial baroreflex
increase blood pressure → stretch HP baroreceptors → decreased sympathetic stimulation → vasodilation → decrease BP
or
decrease BP → decrease stretch HP baroreceptor → increase sympathetic stim → vasoconstriction → increase BP
high pressure baroreceptors
located in carotid sinus/aortic arch
detect changes in atrial pressure
dominates unloading
low pressure baroreceptors
located in atrium
detect stretch → increase cardiac output
dominate loading
Respiratory sinus arrhythmia
correlation of breathing with heart rate due to bainbridge reflex
bainbridge reflex
increase venous return → increased pressure in atrium → increased stretch → increased sympathetic tone via vagus nerve → increased HR
cardiac response to exercise
mechanical
pumping muscle → increase venous return → increased SV/CO
chemical
increased metabolism → decrease pH → vasodilation → increased flow
partial pressures at different spots
Air
PO2 - 160
PCO2 - 0.3
Lungs
PO2 - 104
PCO2 - 40
Tissue
PO2 - 40
PCO2 - 45
daltons law
total pressure is the sum of gas partial pressure
Henrys law
concentration of dissolved has correlates to partial pressure of that gas
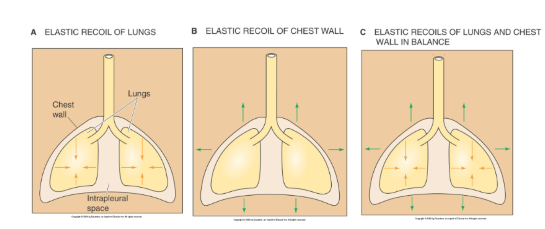
Lung vacuum
elastic recoil of lungs opposes the recoil of the chest wall to create a relative negative pressure → drawing air in
Insparation
Respiratory muscles contract → increased thoracic cavity volume → decreased thoracic cavity pressure → vacuum → air flow in
respiratory muscle
primary - diaphragm and intercostals
secondary - scalenes, neck and back, upper airway
Quiet expiration
elastic recoil of lungs / muscles relax → decrease thoracic volume → increase thoracic pressure → air flows out
Active expiration
abs, intercostals, and neck/back muscle forcefully contract to push air out
Atelectasis
punctured lung → Pip = Patm → no vacuum → alveoli collapse
fixed by increasing transpulmonary pressure
transpulmonary pressure
Ptp = Pa - Pip
alveolar surface tension
water on alveoli creates a collapsing force
surfactant
produced by alveolar type II cells to break the surface tension and allow alveoli to inflate
Infant respiratory distress syndrome
no surfactant → increased surface tension → lungs collapse
O2 transport in blood
dissolved in plasma
bound to hemoglobin
CO2 transport in blood
dissolved in plasma (minimal)
bound to hemoglobin (minimal)
Bicarbonate (majority)
Bohr effect
increased metabolic rate → increased temperature, CO2, H+, 2-3 DPG
Haladane effect
Hemoglobins ability to carry O2 in the blood is dependent upon O2
Fick’s law
rate of diffusion is affected by
molecular weight of gas (negative)
solubility of the gas (positive)
area of membrane (positive)
thickness of membrane (negative)
Factors affecting gas exchange
diffusion capacity (fick’s law)
partial pressure difference
transit time
Fick principle
VO2 = CO x (a-v difference)
Diffusion equilibrium
when Partieriole = Pblood
happens 1/3 down the capillary
Minute ventilation
VE = (VTidal - VDead Space) x Respiratory rate
characteristics of pulmonary circulation
low resistance
low pressure
high compliance
increase arterial pressure → decreased resistance
V/Q matching
the balance of ventilation and perfusion
If V is too high → alveolar air approaching atmospheric air
If Q is too high → alveolar air approaches venous air
Alveolar dead space ventilation
ventilation without perfusion
no blood flow to alveoli → ventilation increases
lungs compensated with bronchoconstriction and reduced surfactant → ventilation decrease
pulmonary shunt
perfusion without ventilation
Blood passes from right to left heart without becoming oxygenated
lungs compensate by shunting (redirecting) blood away from unventilated alveoli
Apnea
the cessation of breathing
occurs when sleeping if CO2 drops blow apneic threshold
central respiratory chemoreceptors
located in the brainstem
detect brain tissue PCO2/H+
control 70% of ventilation
peripheral respiratory chemoreceptors
located in carotid and aortic bodies
detect blood O2/CO2
control 30% of ventilation
Dorsal respiratory group
detect lung stretch/peripheral chemoreceptors and send the signal to the VRG
Ventral respiratory group
rhythm generating/integrating center
sets eupena (breaths/minute)
VRG → phrenic/intercostal nerves → inspiratory muscles
Pontine respiratory center
influence/modify the activity pf the medullary (timing) centers
influence the inspiration/expiration transition
response to increased arterial PCO2
increased arterial PCO2 → CRC/PRC detect → medullary respiratory centers → respiratory muscles → increase ventilation