DPRP 712- Removable Complete Dentures I Exam 1 Lecture Material
1/188
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
189 Terms
Consequences of tooth loss
residual ridge resorption, changes in intraoral structures, decreased masticatory function, loss of facial support and muscle tones
A removable dental prosthesis that replaces the entire dentition and associated structures of maxillae or mandible
complete denture/ complete removable dental prothesis
residual ridge resorption
non physiologic compression (under dentures) results in resorption
which arch has a faster residual ridge resorption by 4x
mandibular
Maxillary loss is in a ____ direction
vertical and palatal
mandibular loss is in a ________ and oriented along _____
vertical direction; cross sectional shape of mandible
Maxilla gets ______, mandible gets _____
shorter and smaller; shorter and wider
Masticatory performance of complete dentures
59%
goal of complete denture treatment
minimize affect of functional, aesthetic, and psychological compromises
T/F dentures over the decades will have more problems due to bone loss, muscle tone loss, less neuromuscular control, reduced saliva, thinning tissues
T
T/F you can eat corn on the cob or an apple with dentures
F- this will accelerate RRR
T/F Patient education is an important part of the denture sucess
T
Retention
resistance to displacement of denture base away from ridge
Support
resistance to vertical movement of denture base toward ridge
Stability
Resistance to horizontal or rotational forces
Primary stress bearing areas of the maxilla
palate, residual ridge
Primary stress bearing areas of mandible
buccal shelf and retromolar pad
Step 1 Complete Denture Treatment
With Patient- treatment plan and prelim impressions
Lab- Prelim casts and custum tray
Step 2 Complete Denture Treatment
With Patient- Border molding and final impressions
Lab- Master cast, record base, wax rim
Step 3 Complete Denture Treatment
With patient- Ear Bow and MMR
Lab- cast mount and teeth set up
Step 4 Complete Denture Treatment
with patient- wax try in, adjustments, CR verification
lab- wax up and process dentures
Horizontal Jaw relation
centric relation
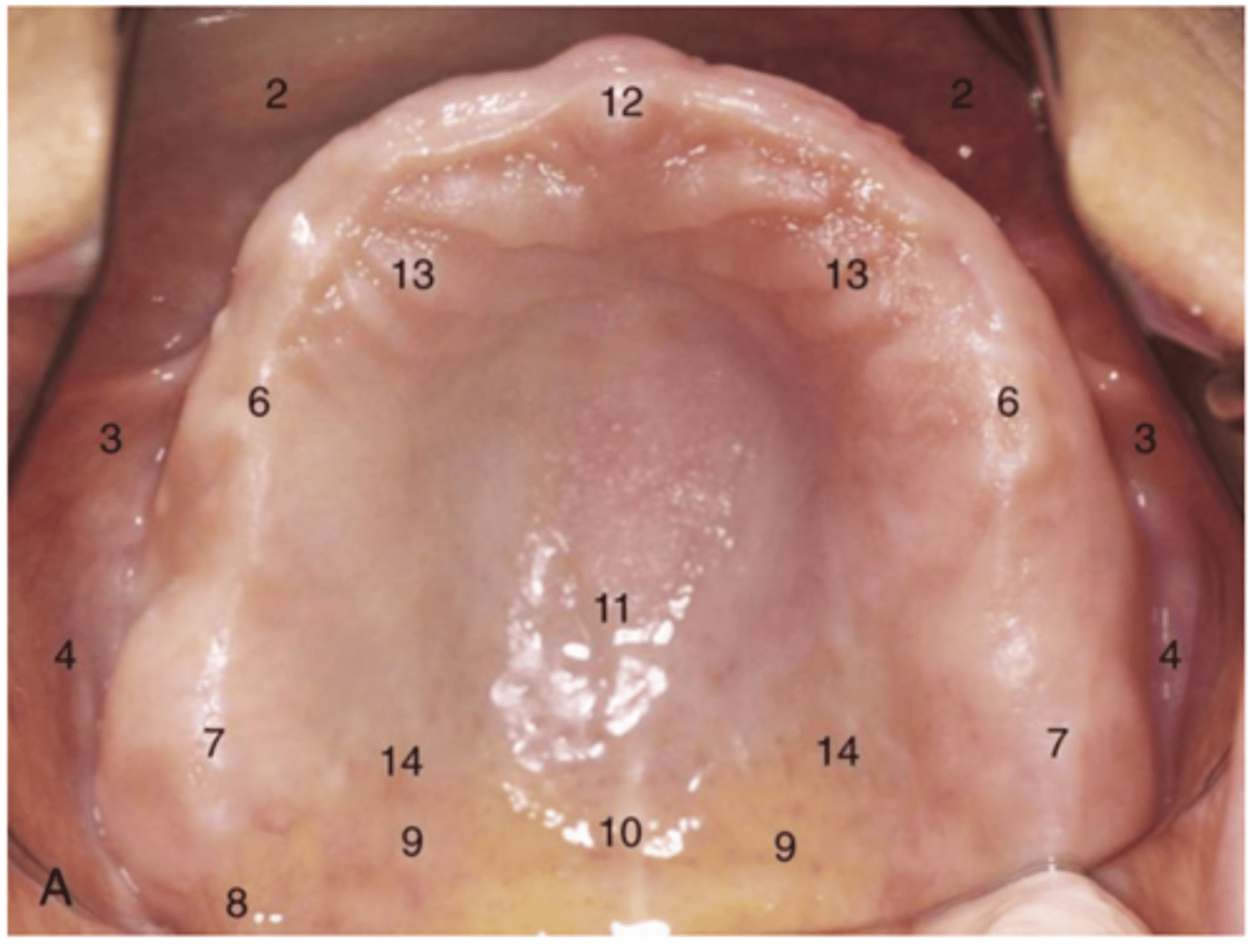
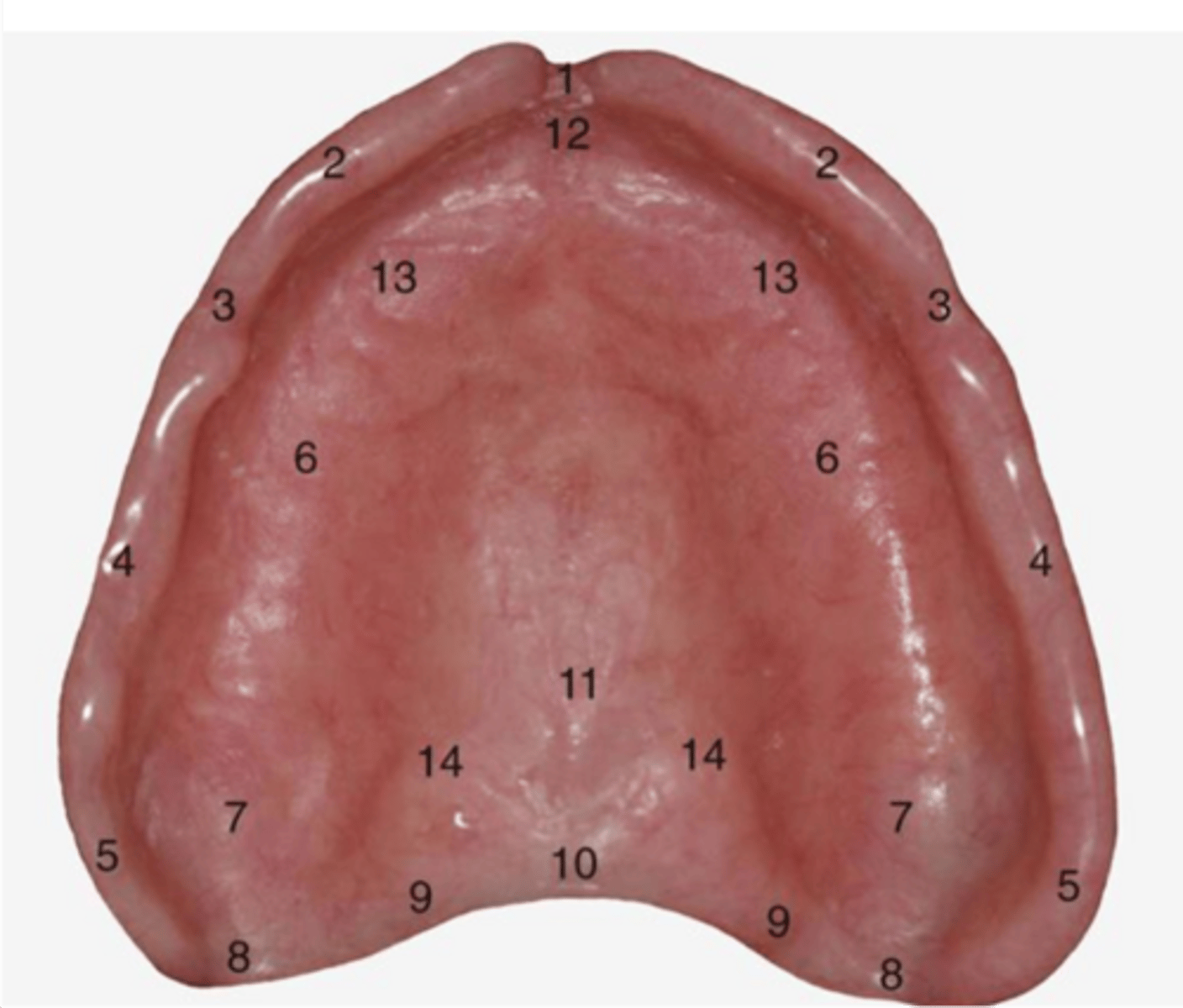
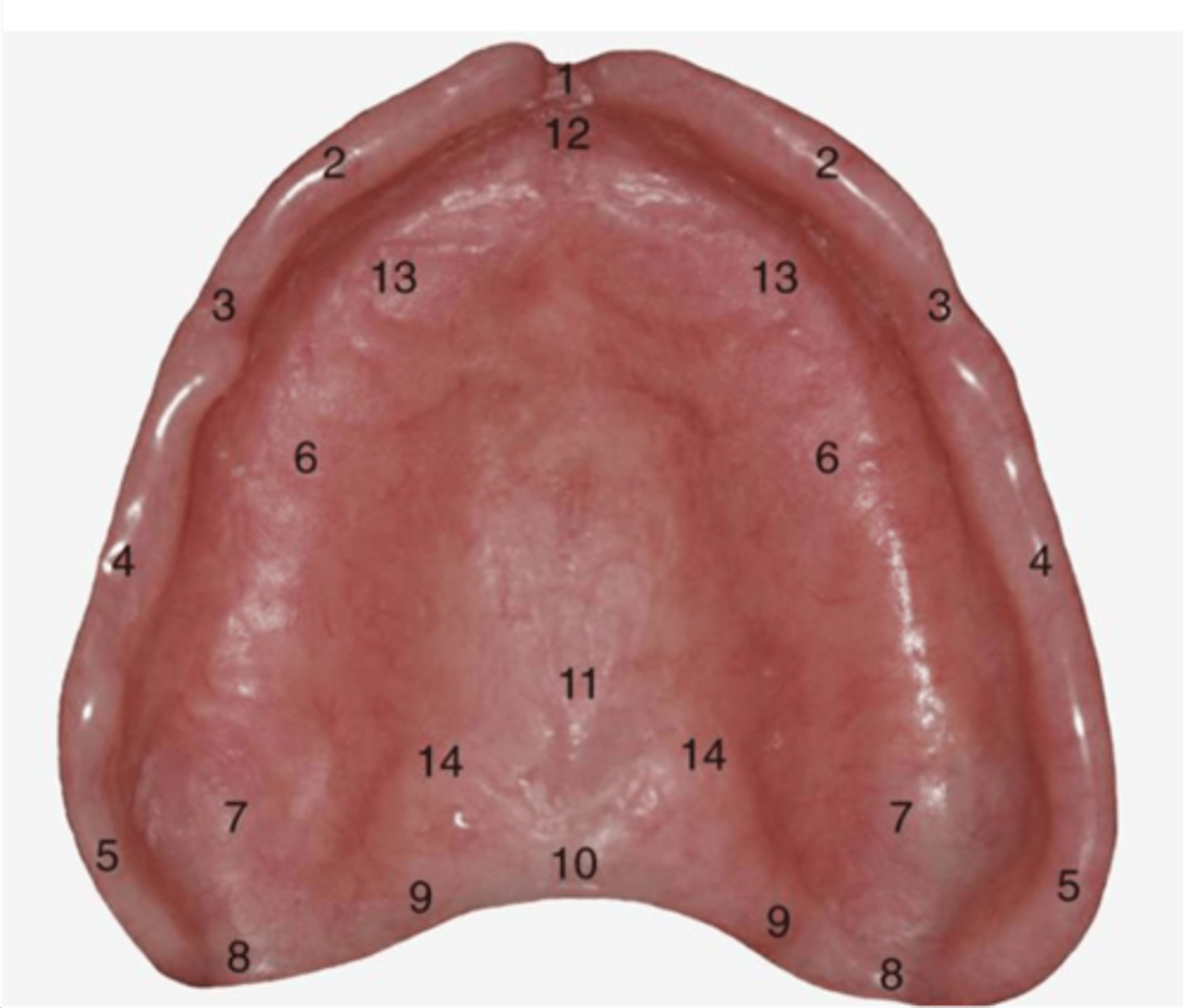
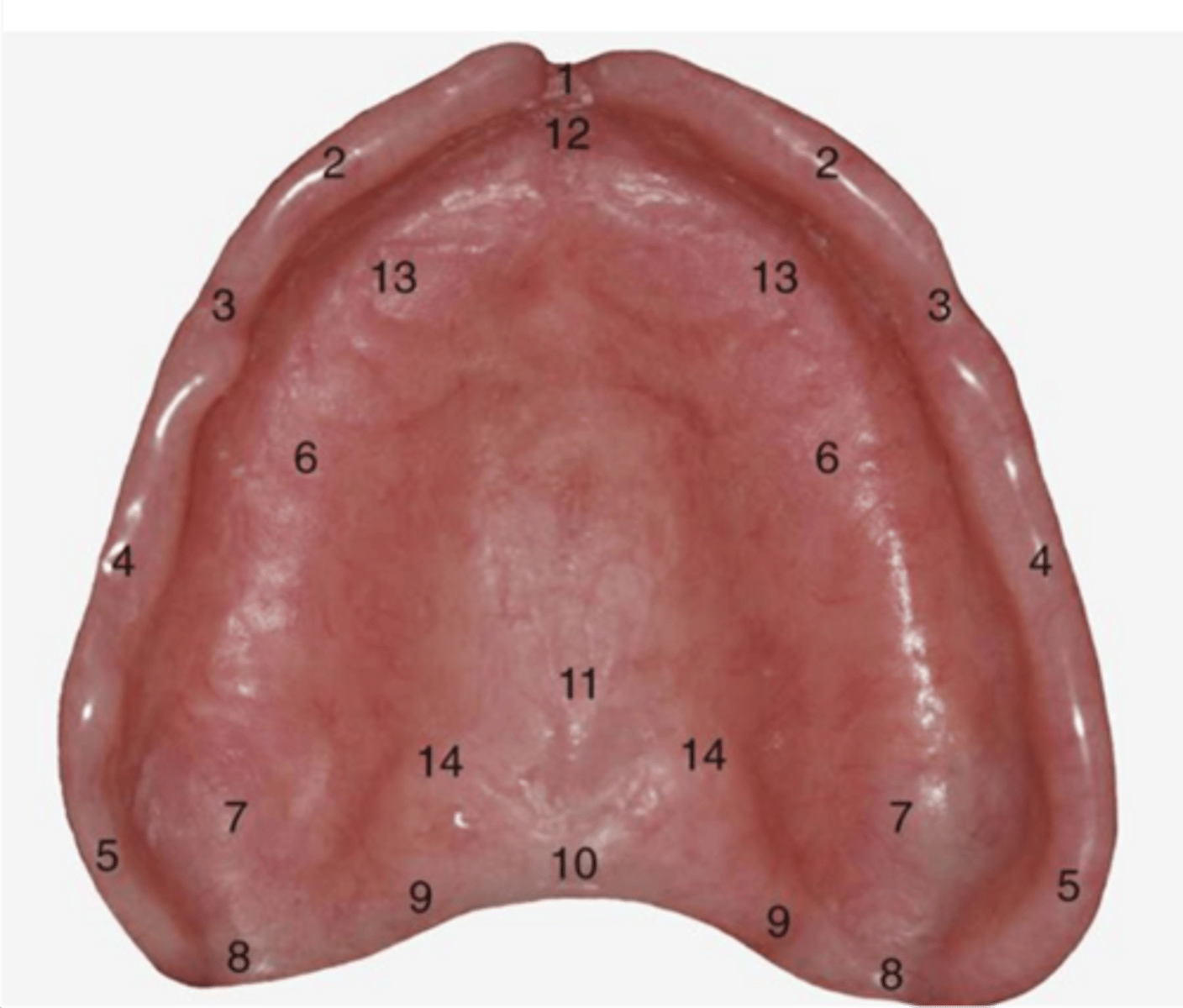
labial vestibule
2
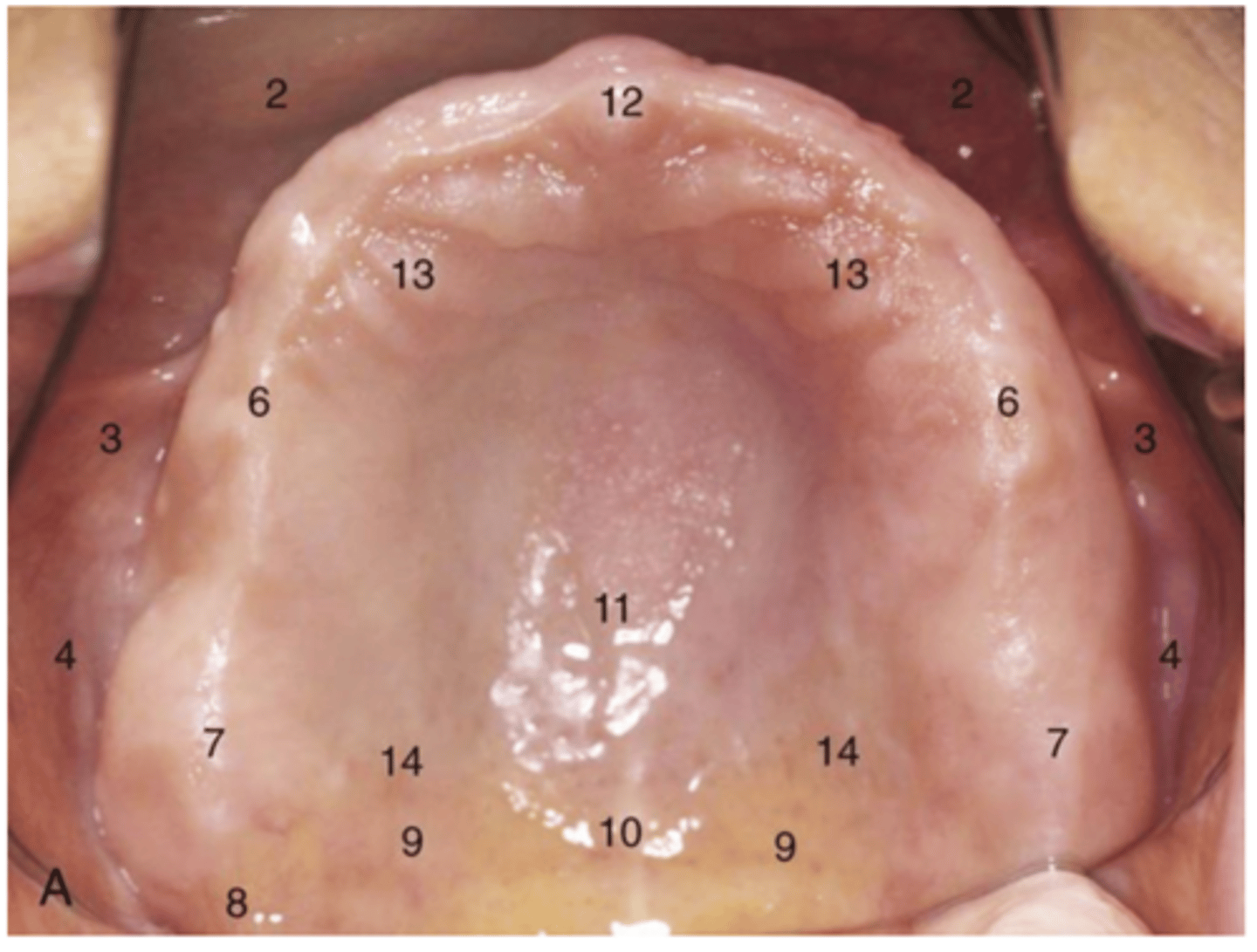
Buccal vestibule
4
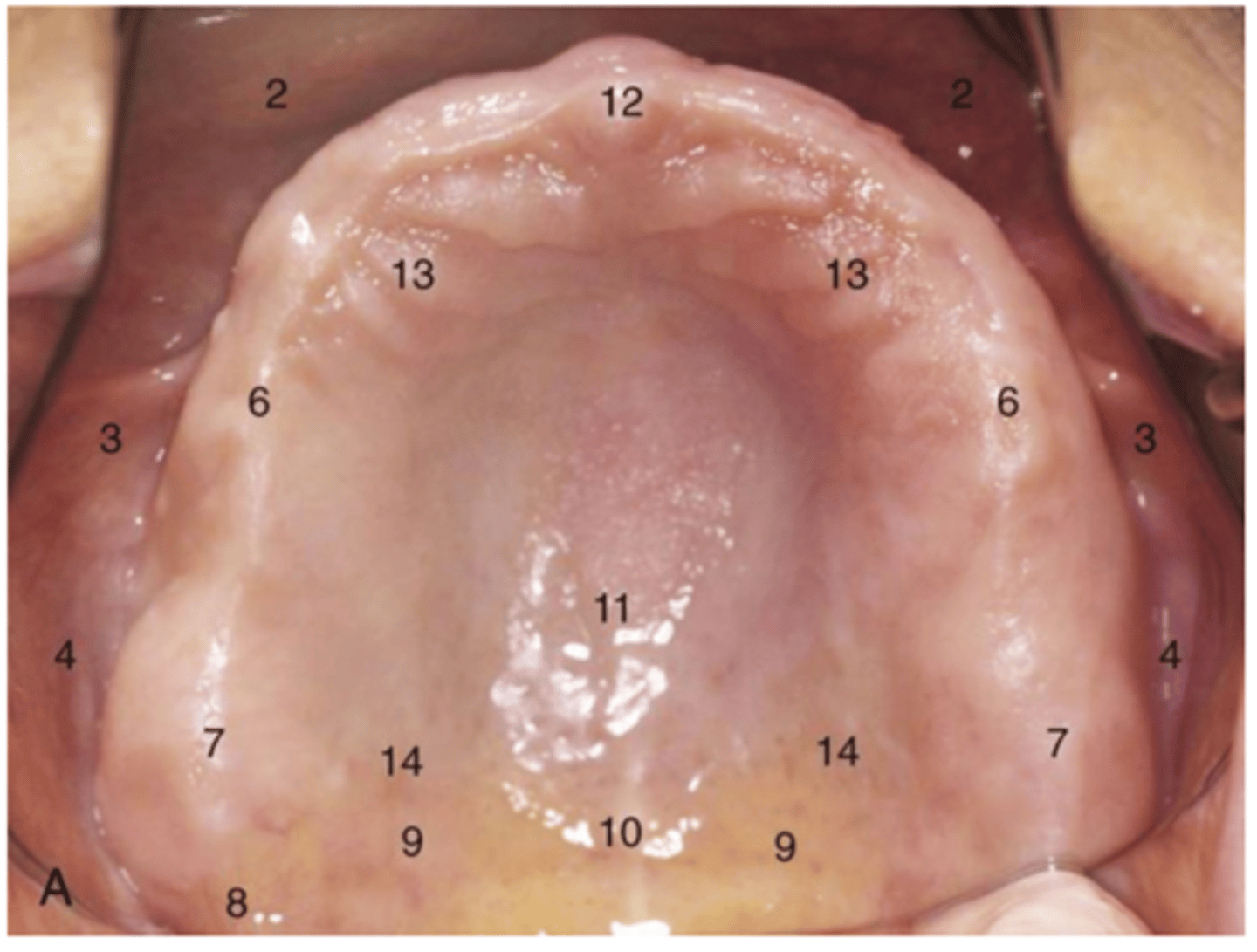
Residual Ridge
6
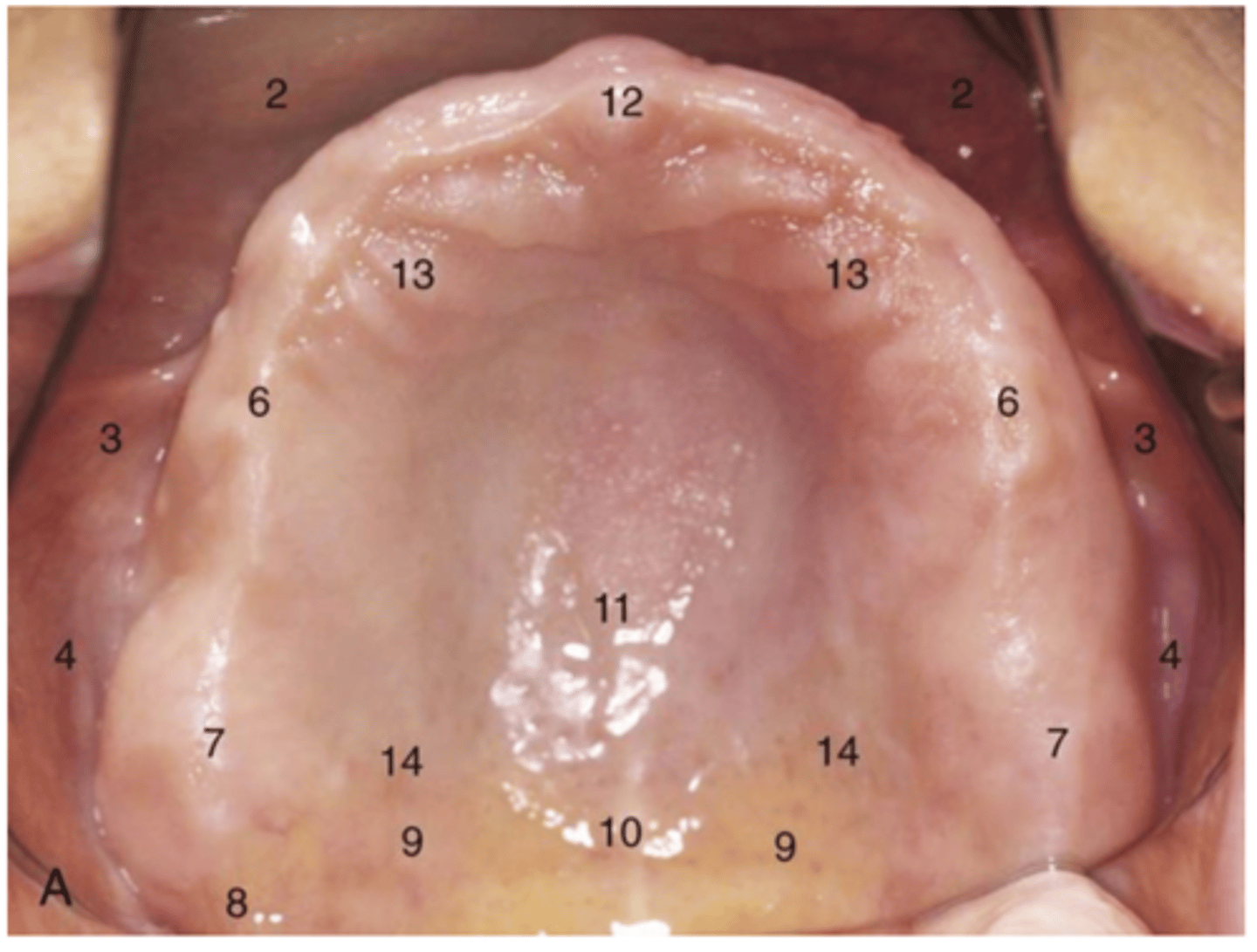
rugae
13
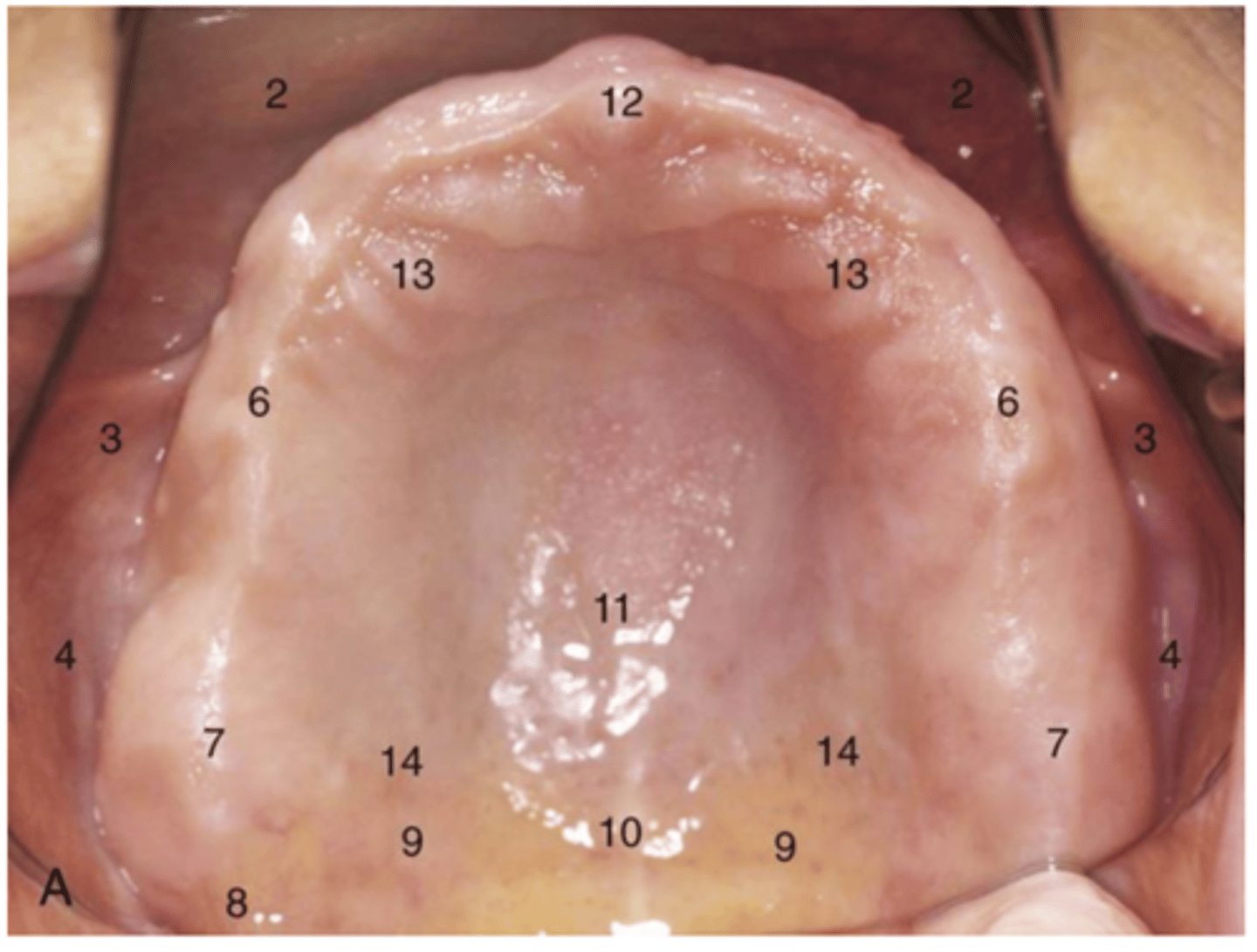
Buccal frenulum
3
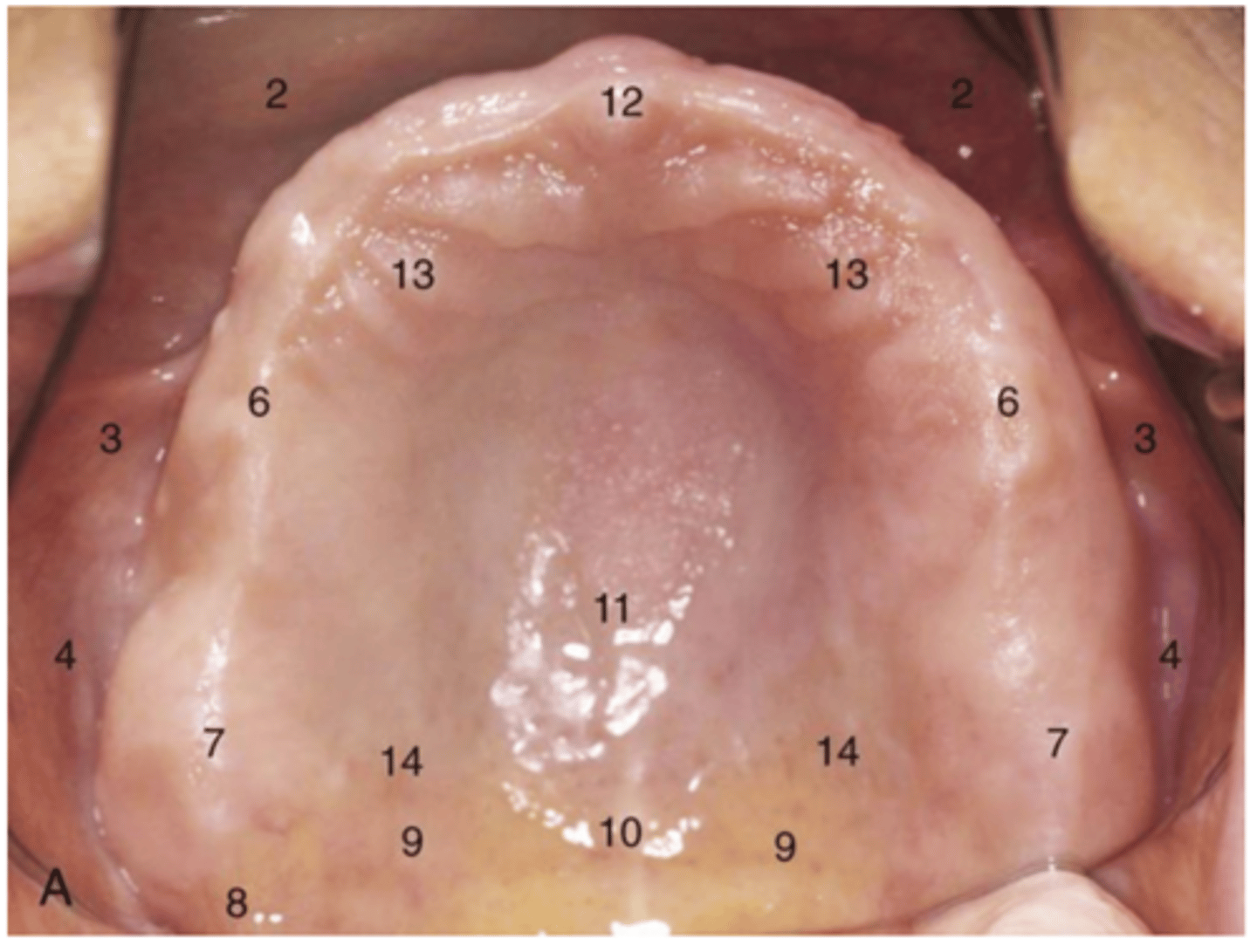
tuberosities
7
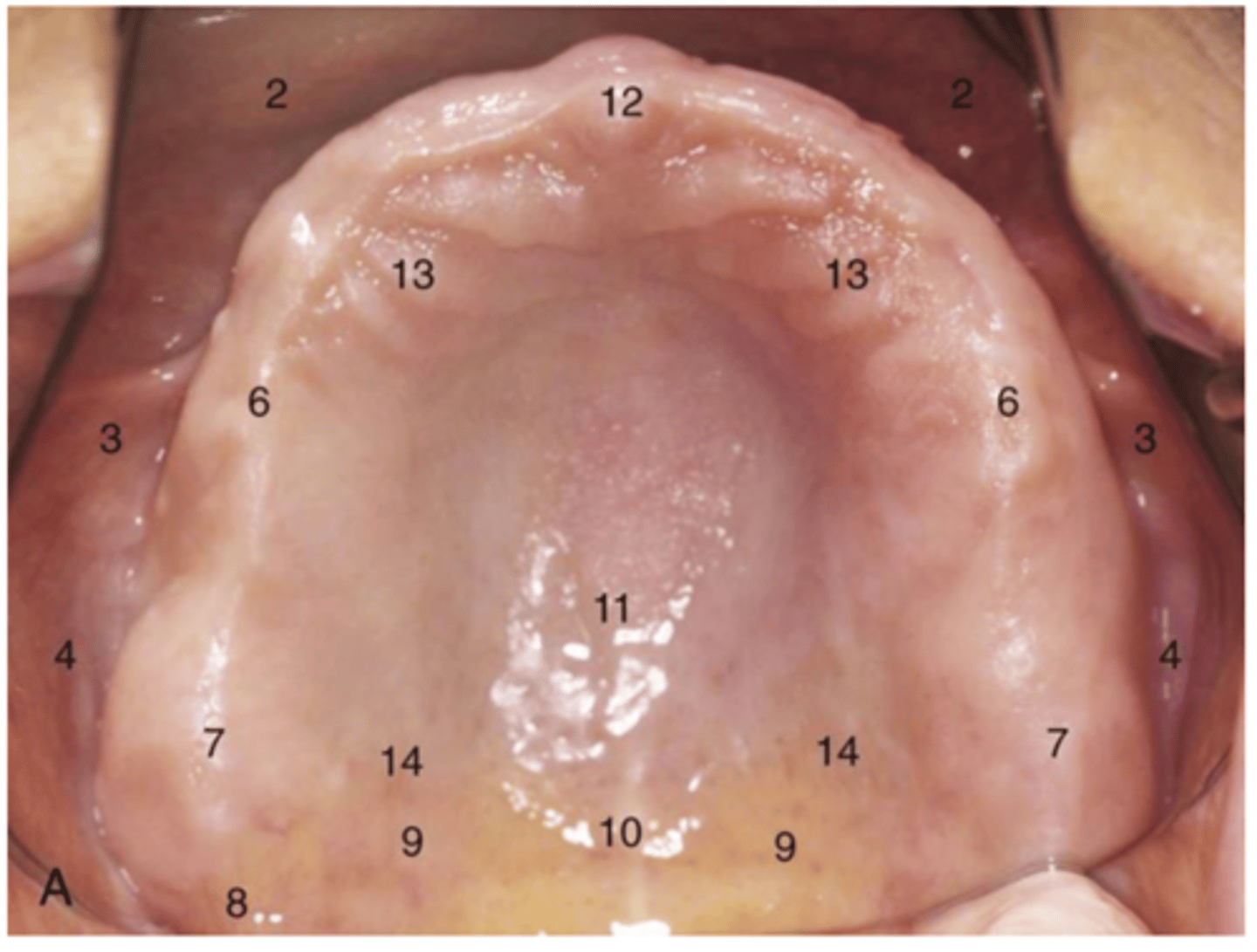
Incisive papilla
12
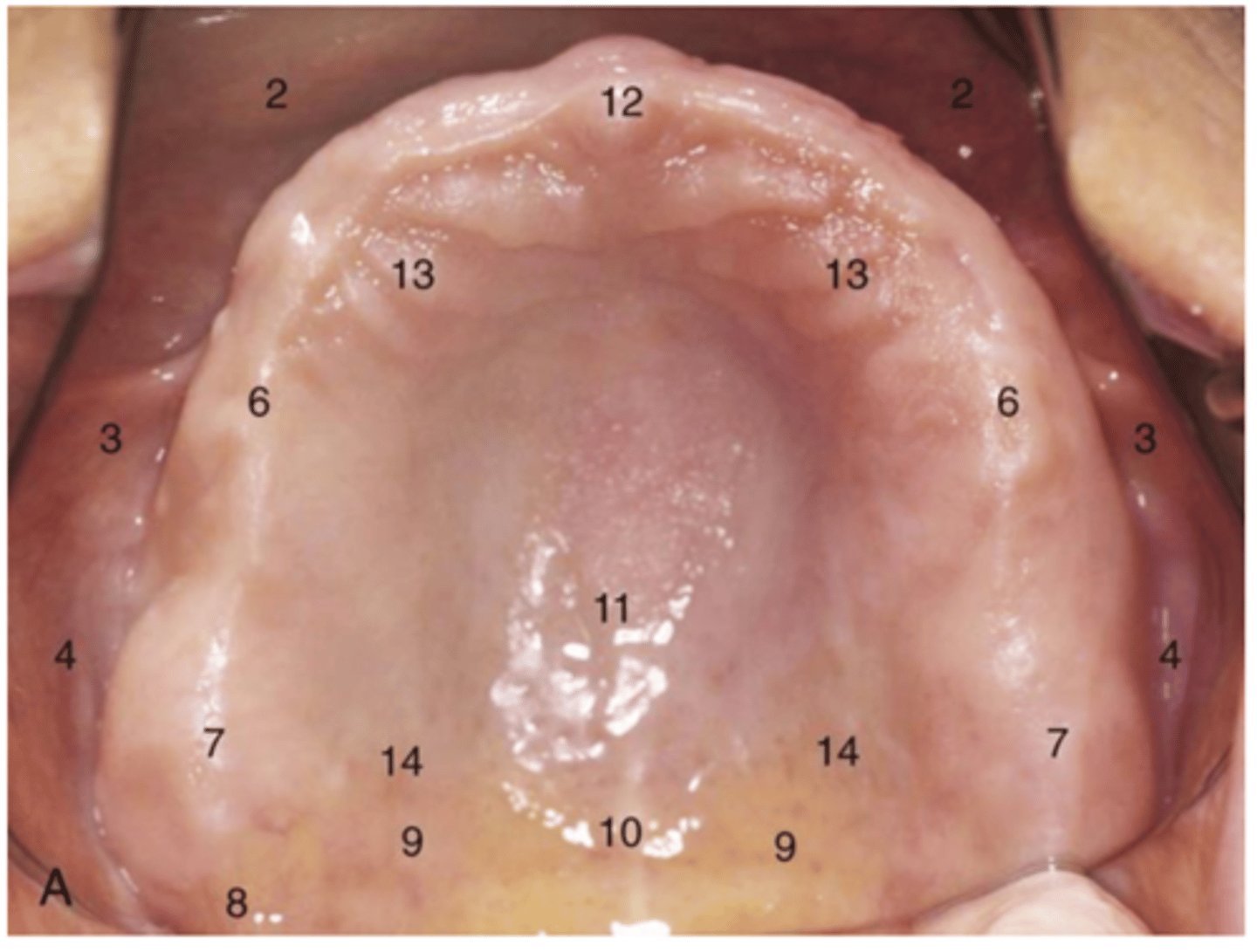
posterior palatal seal
9
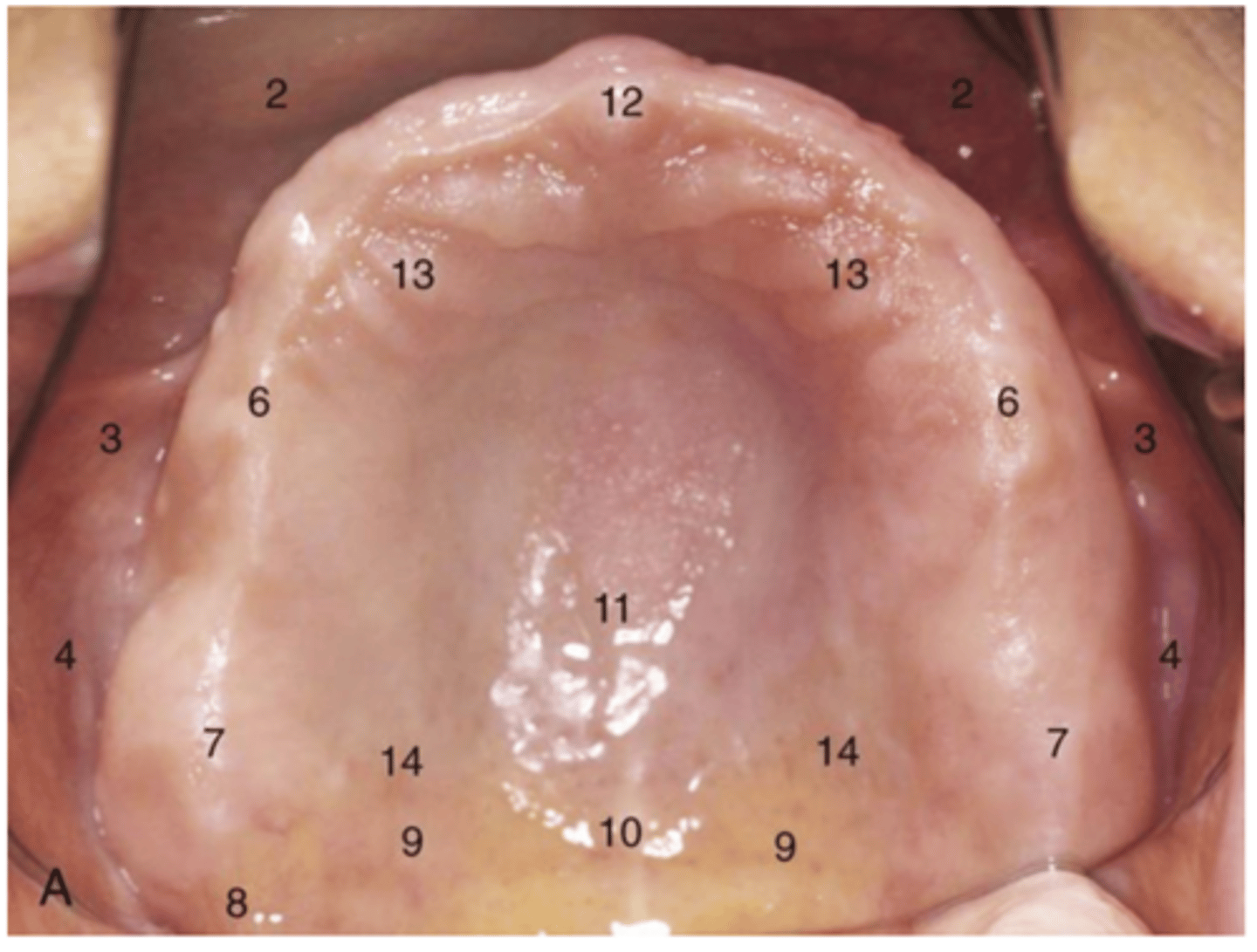
Junction of soft tissue over hard palate
14
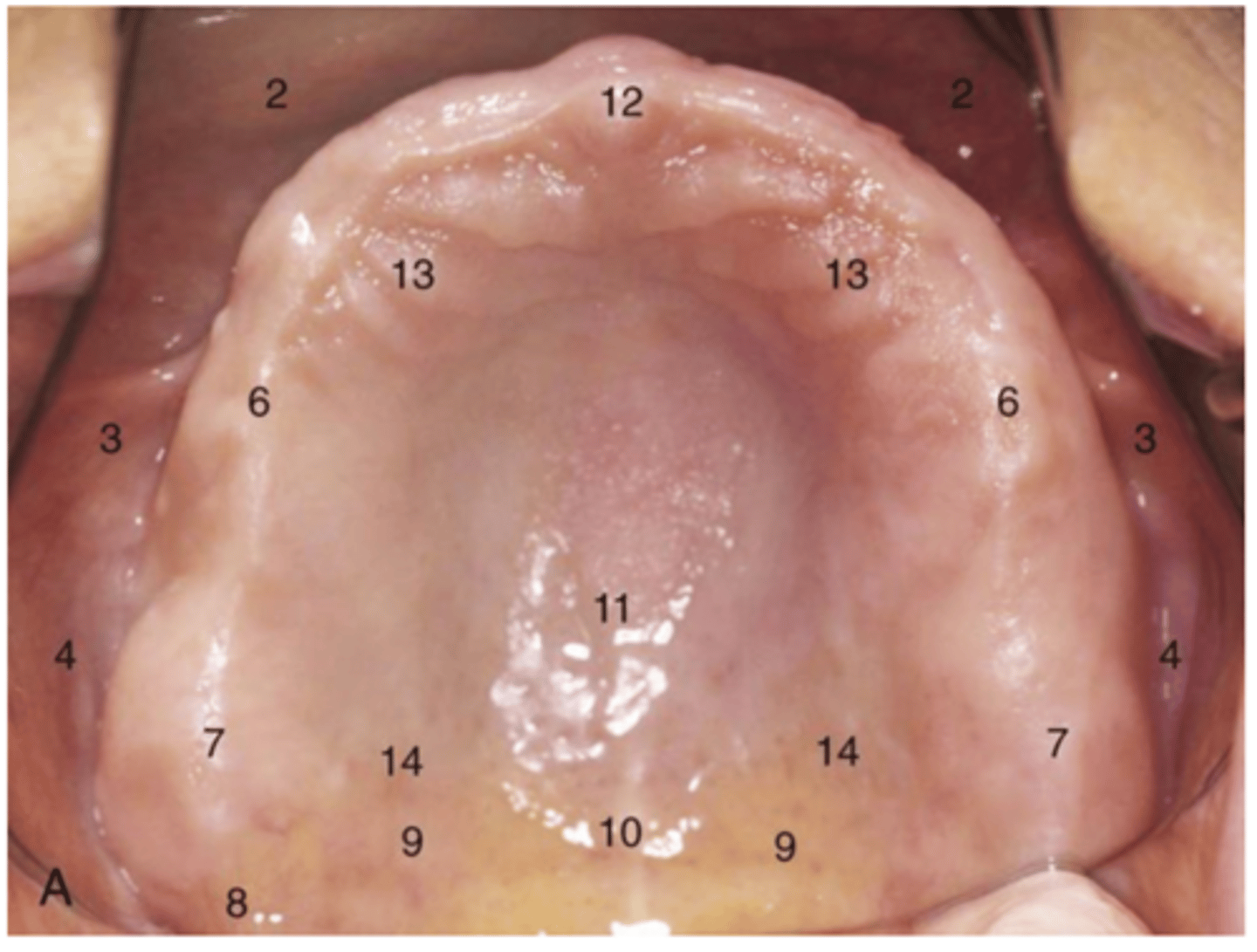
fovea palatine
10
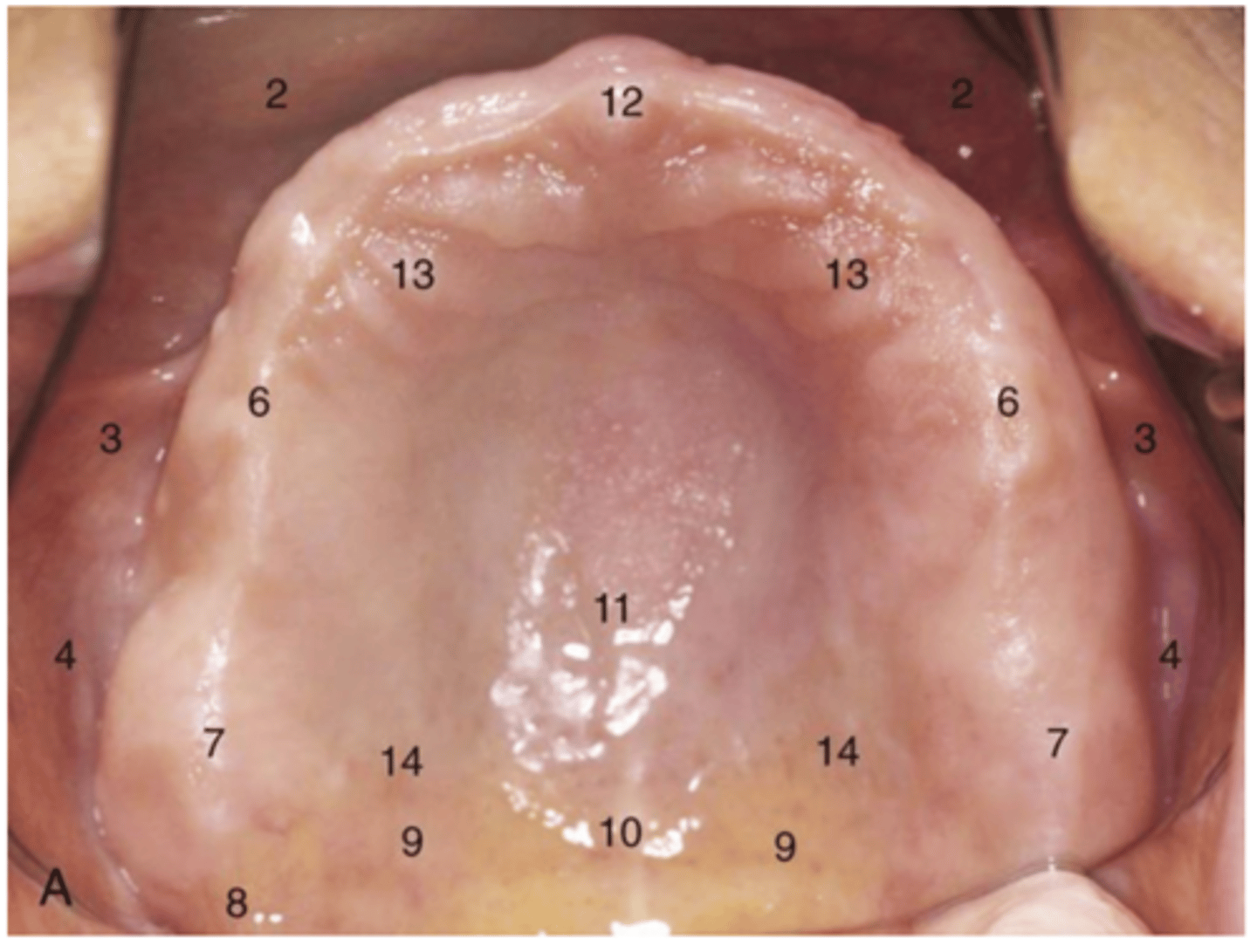
Hamular notch
8
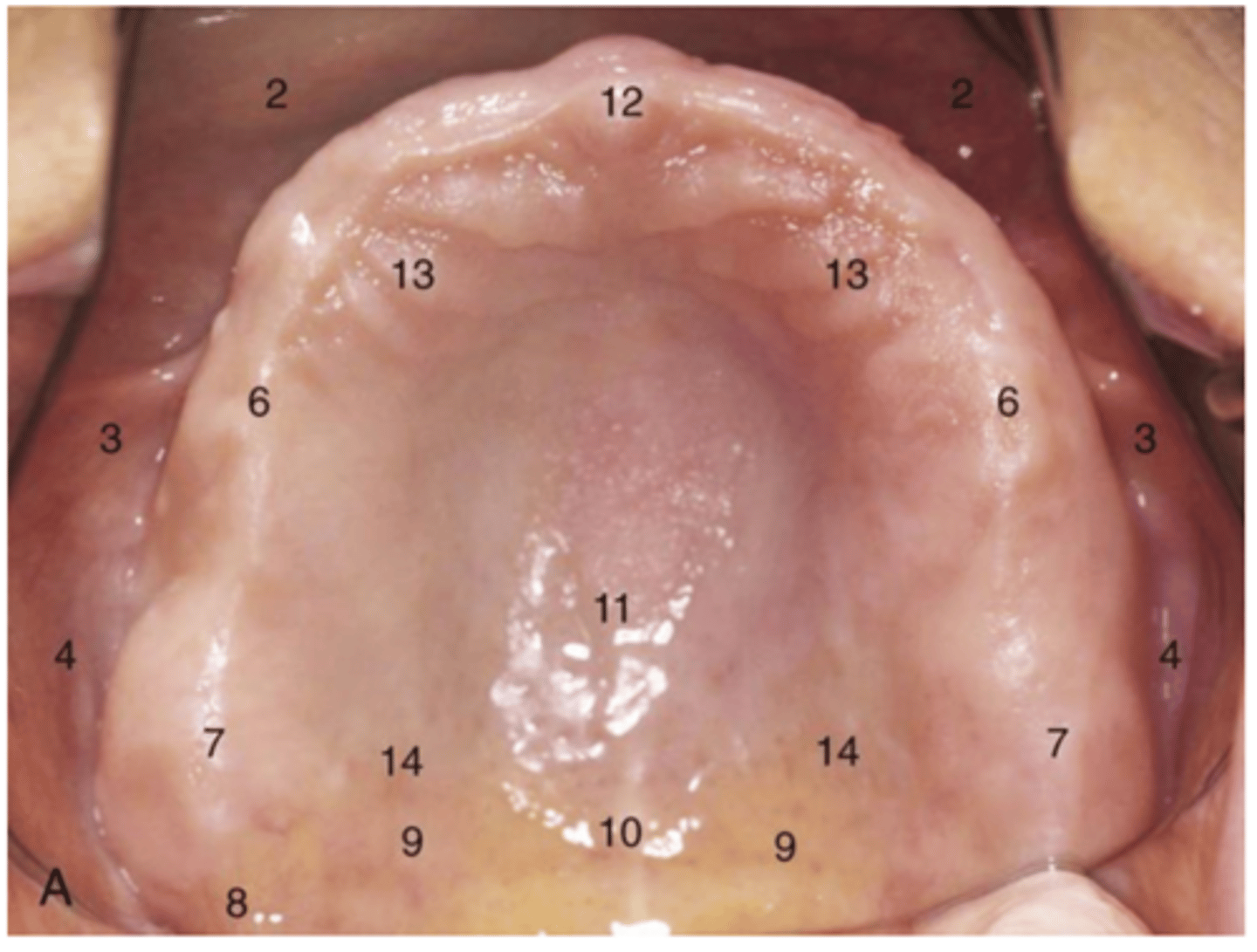
Median palatine raphe
11
Labial notch
1
labial flange
2
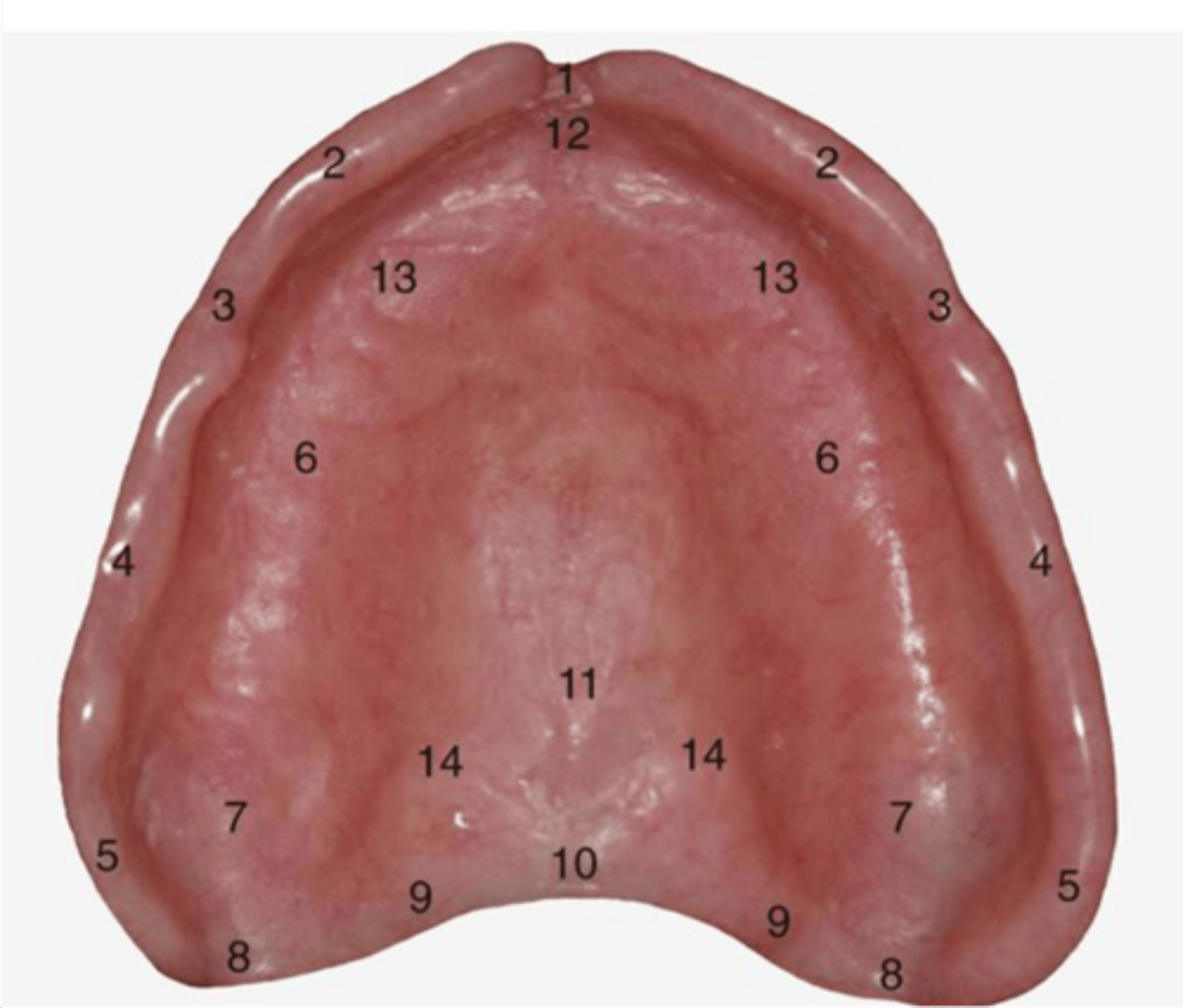
Buccal notch
3
buccal flange
4
Alveolar groove
6
incisive fossa
12
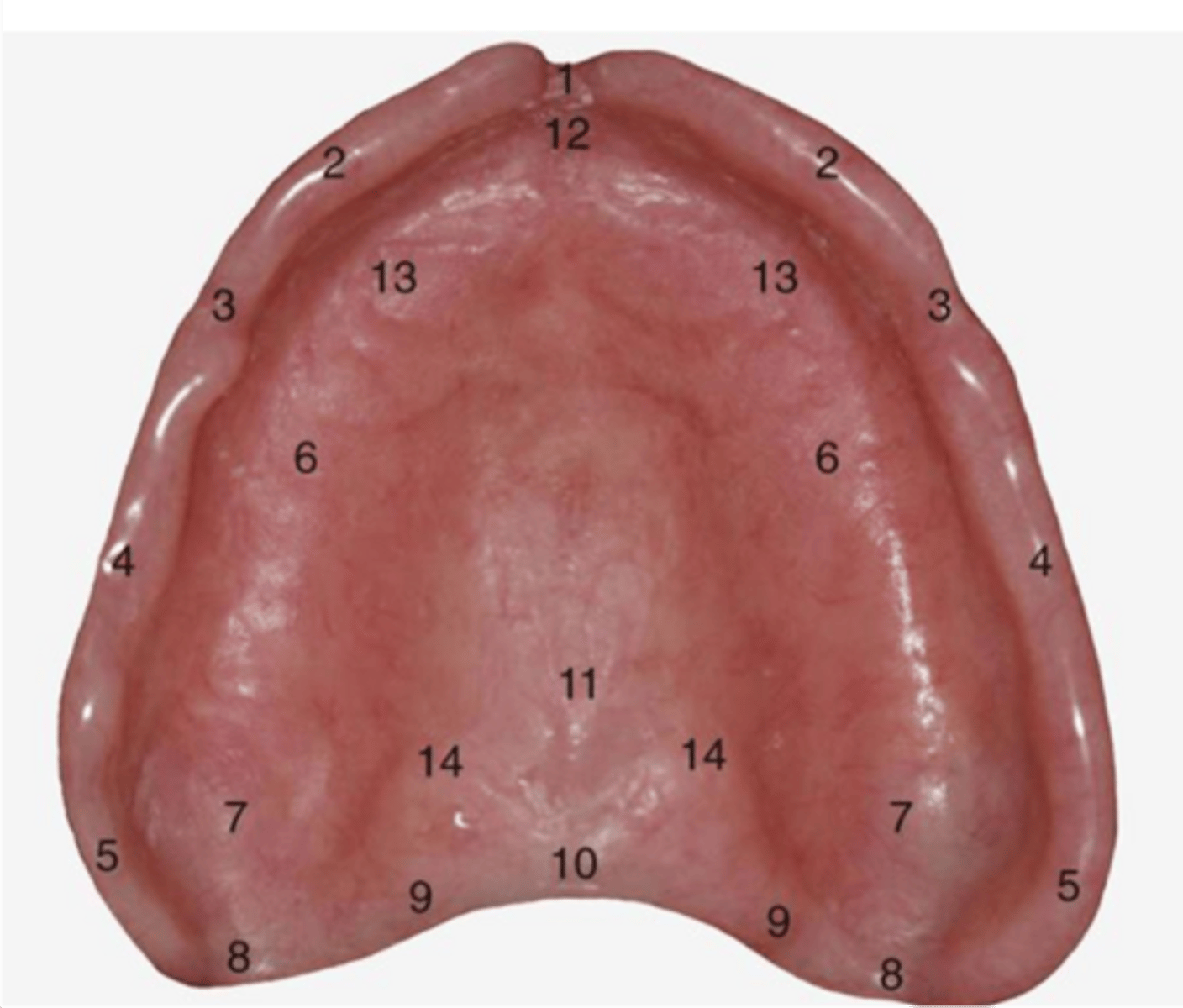
Coronoid contour
5
Inadequate width or height of this flange area is a problem when developing seal to hold maxillary denture up
coronoid contour
area of posterior palatal seal
9
posterior palatal seal makes a _____ outline
butterfly
pterygomaxillary seal in area of hamular notch
8
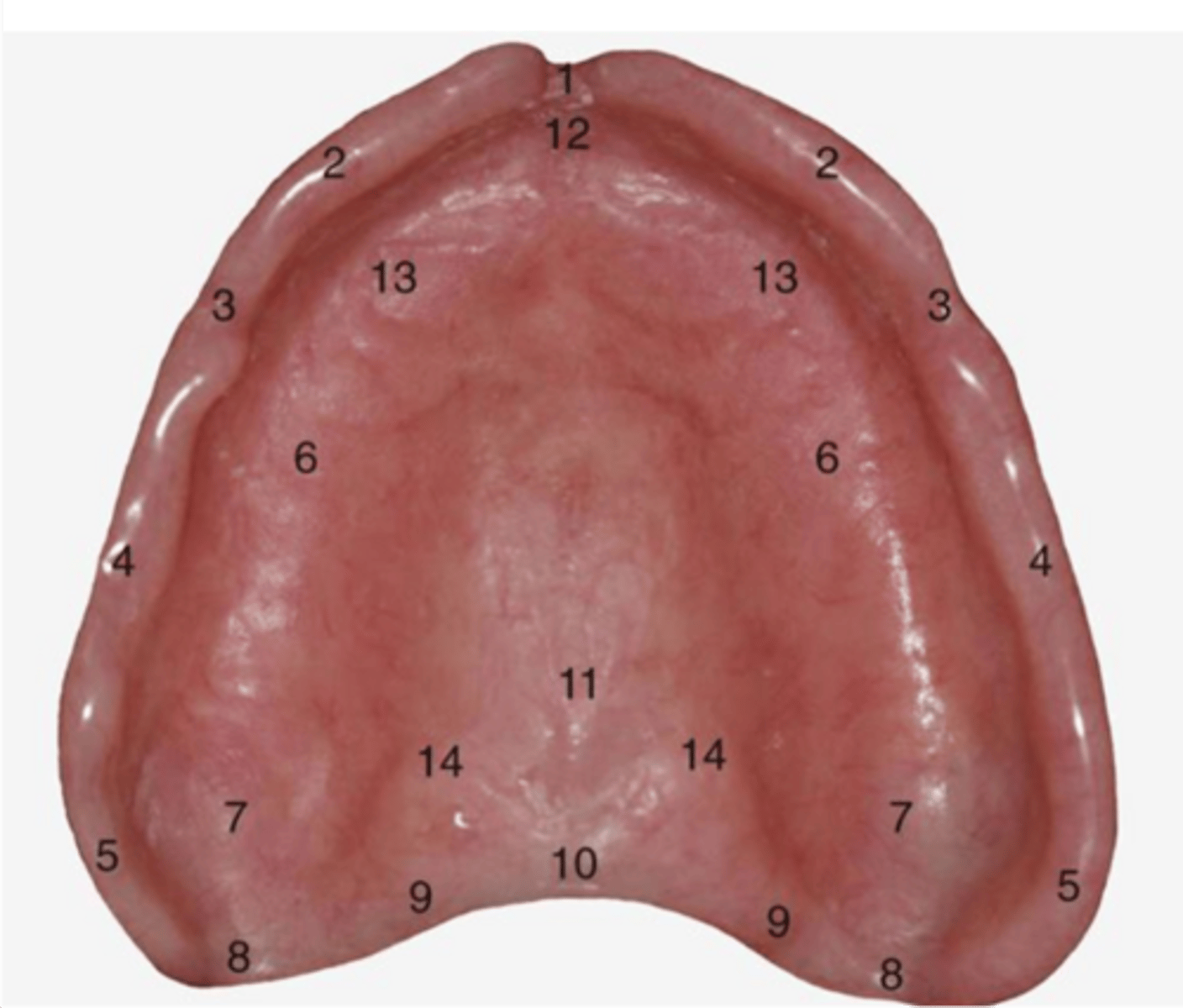
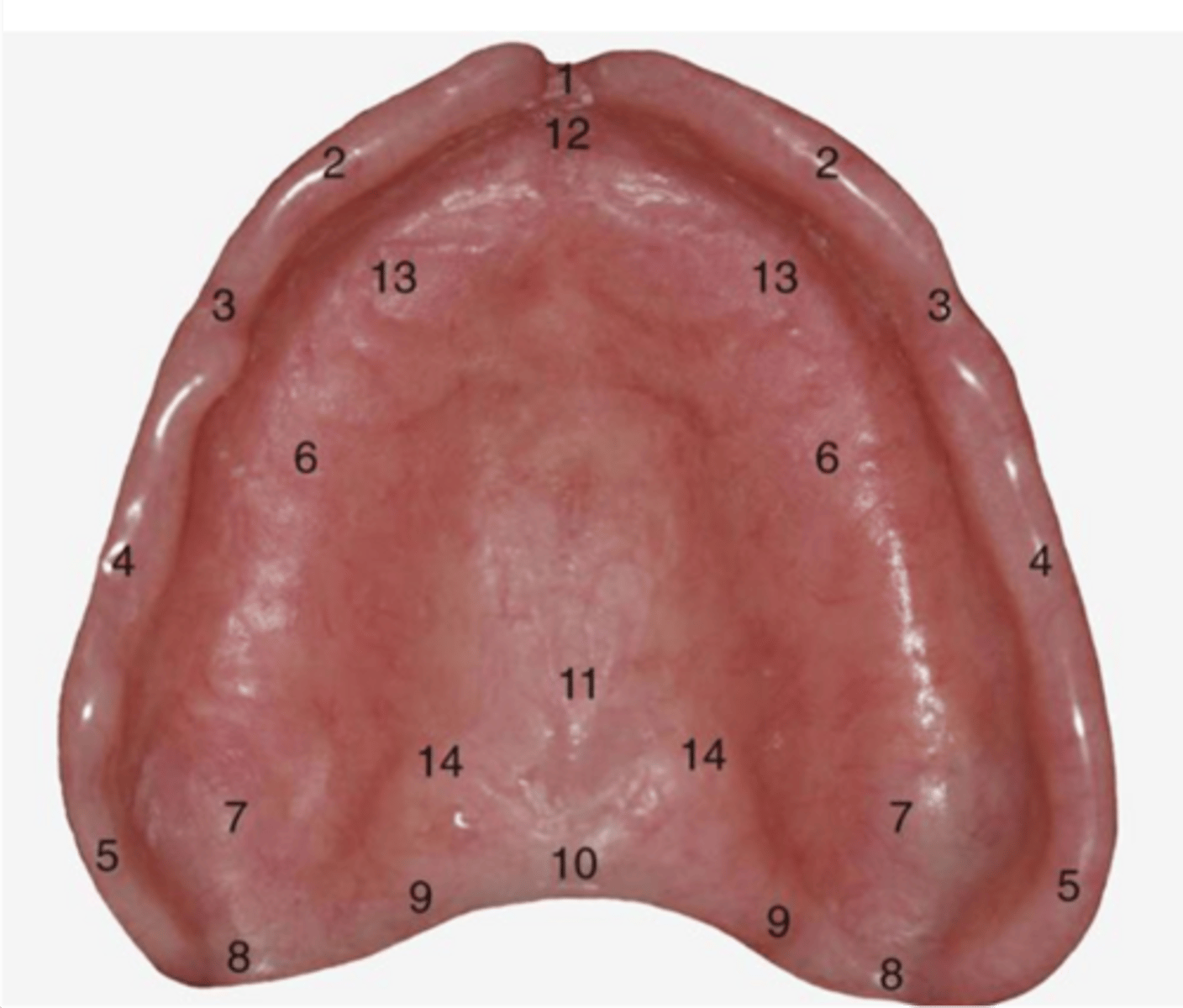
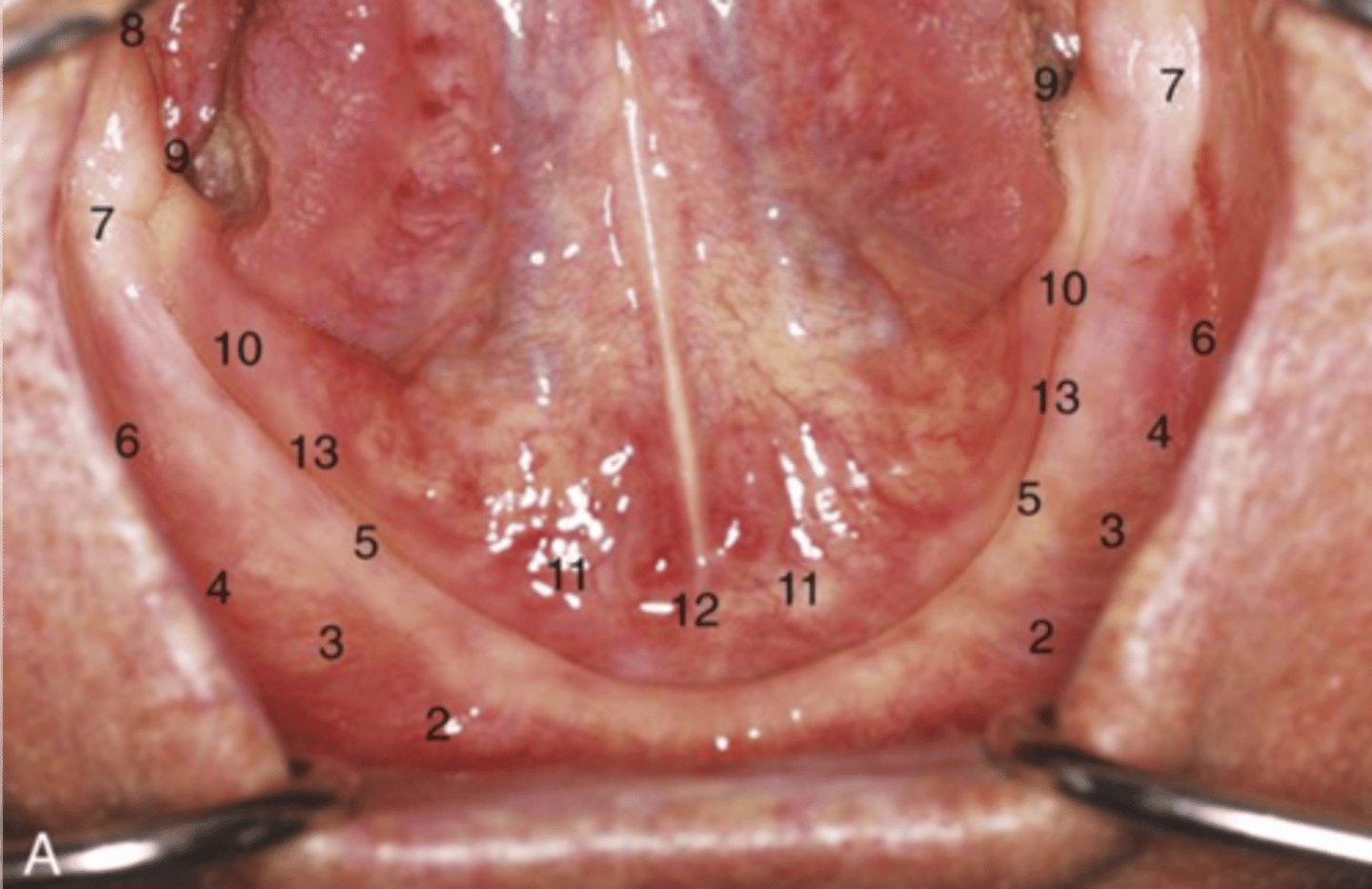
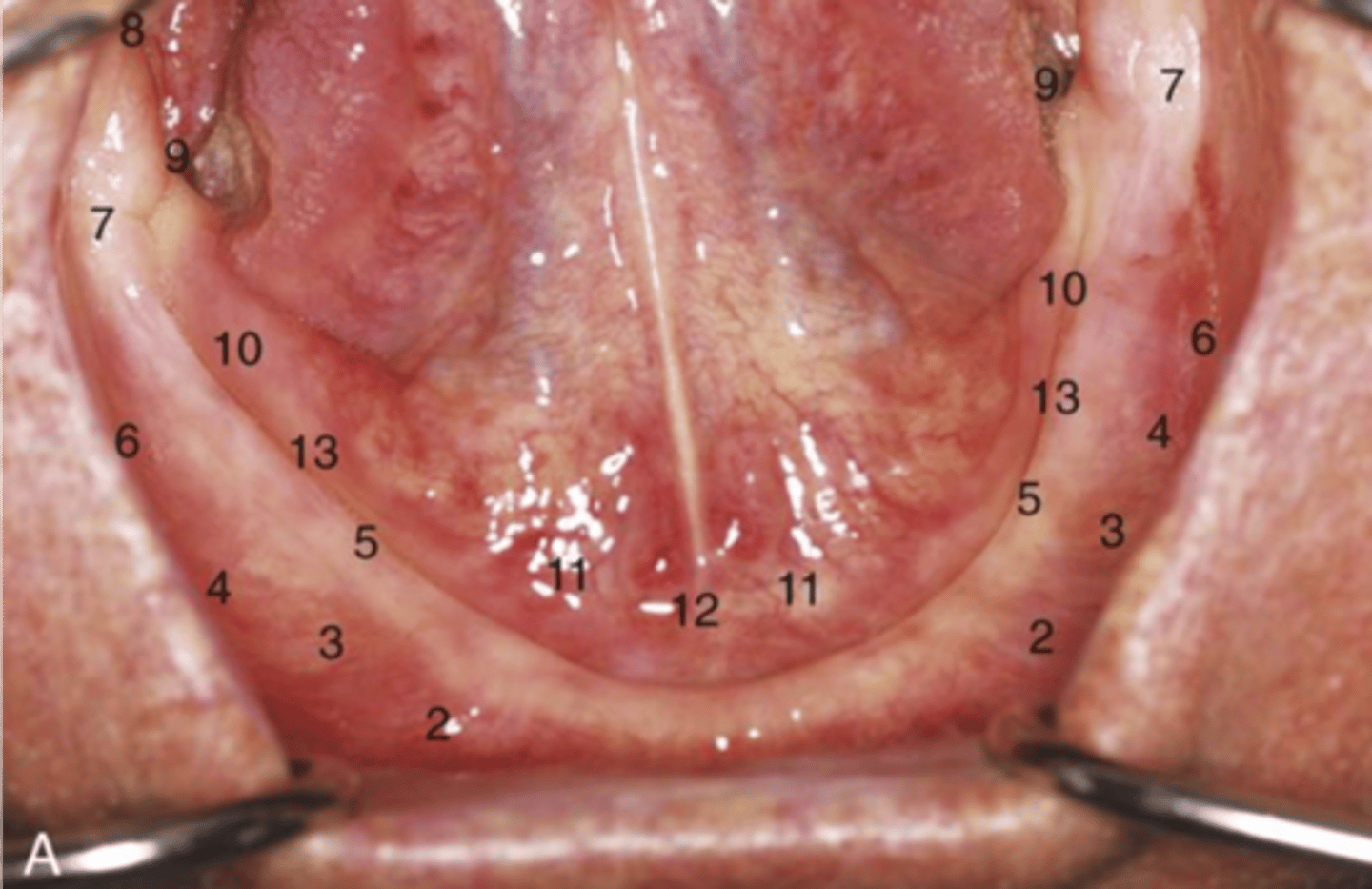
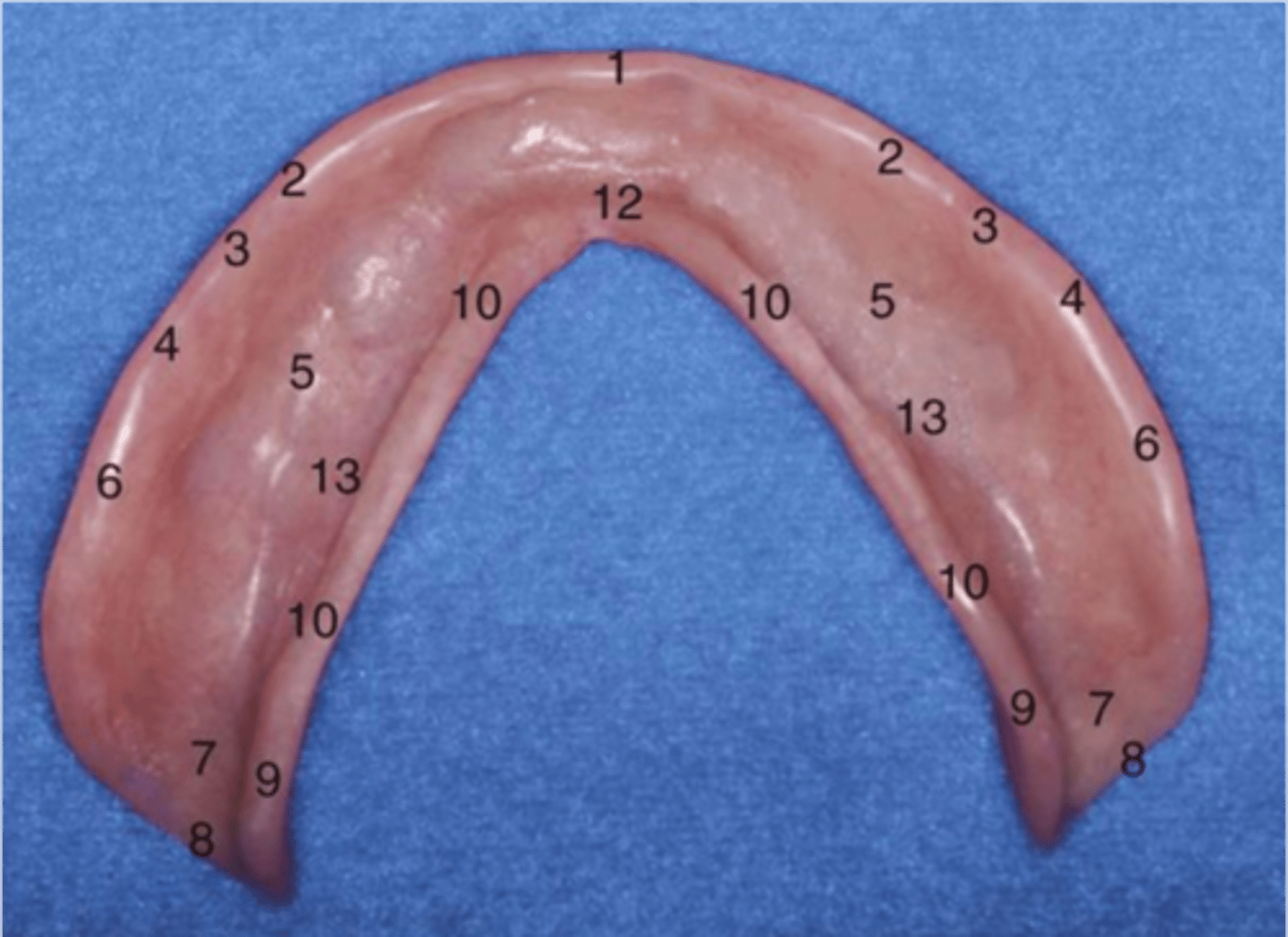
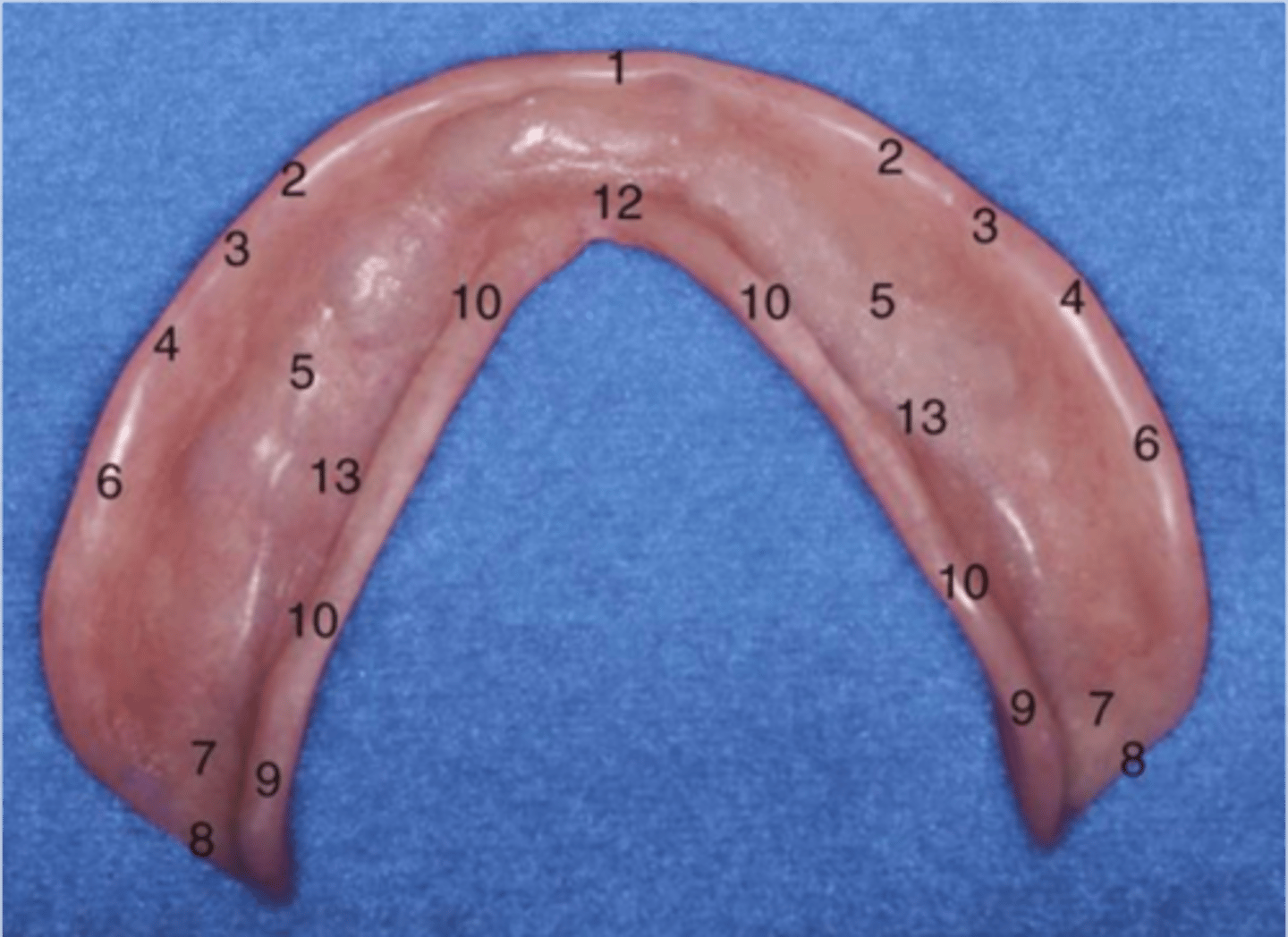
Labial vestibule
2
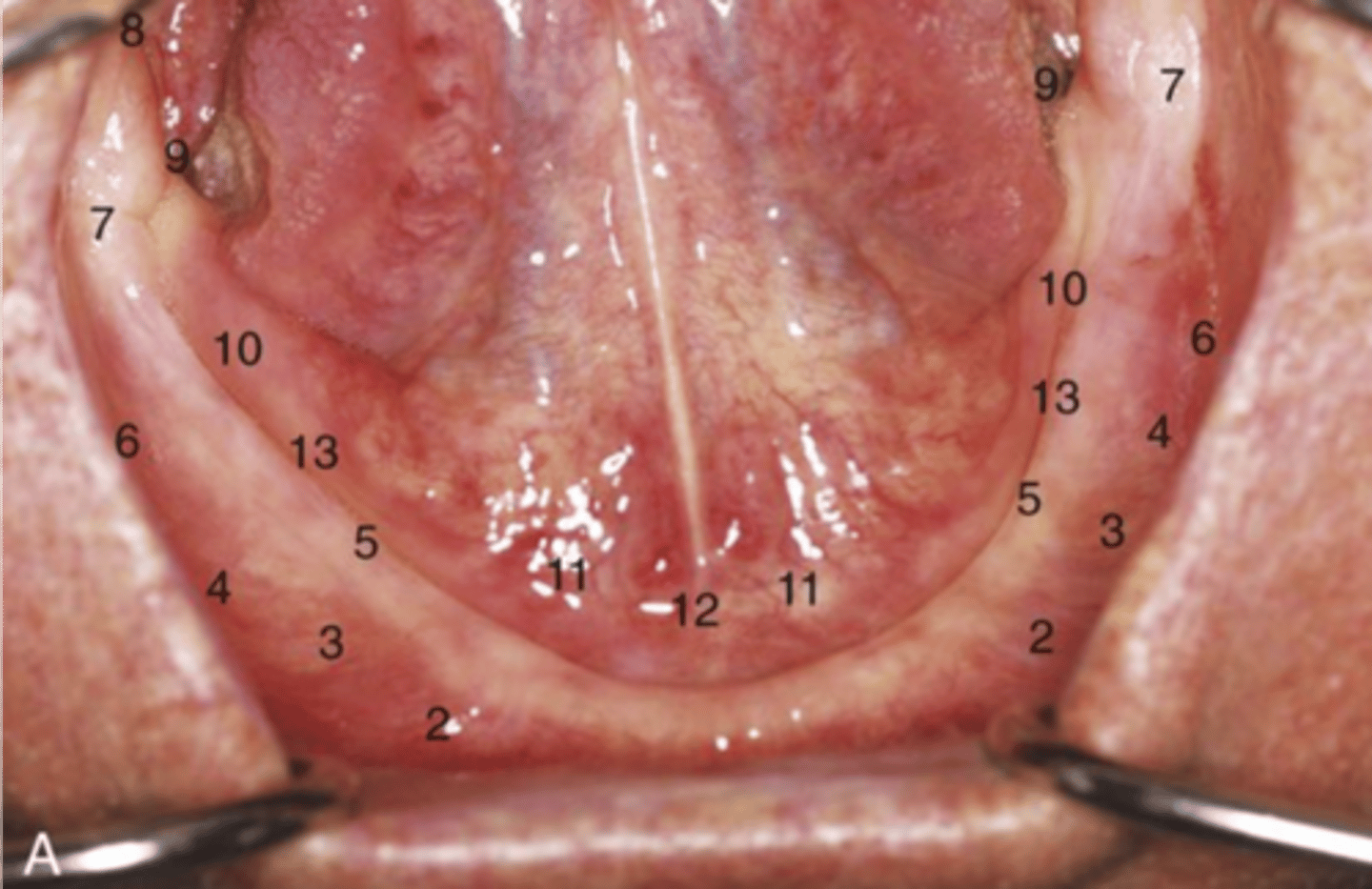
residual alveolar ridge
5
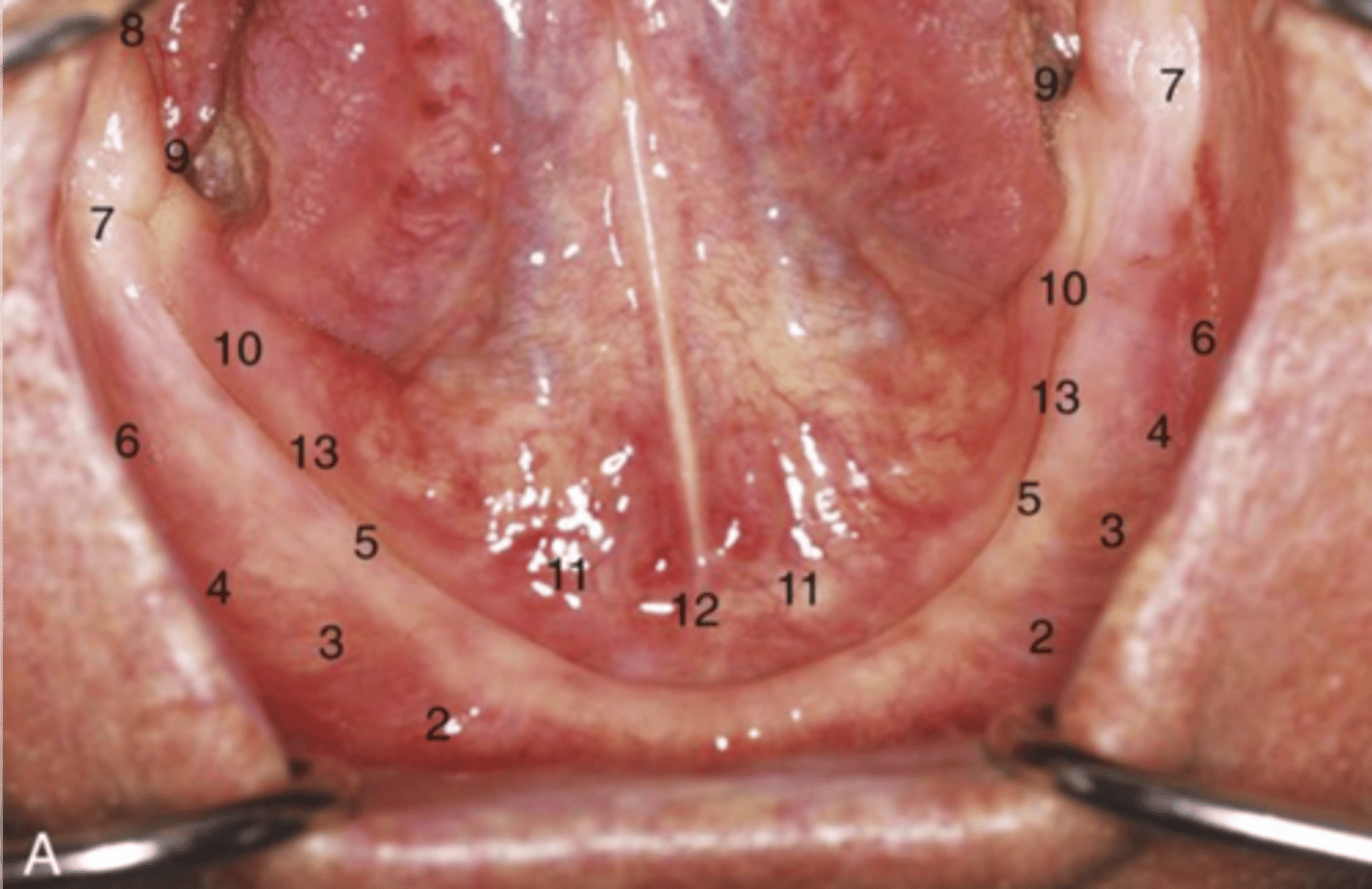
pterygomandibular raphe
8
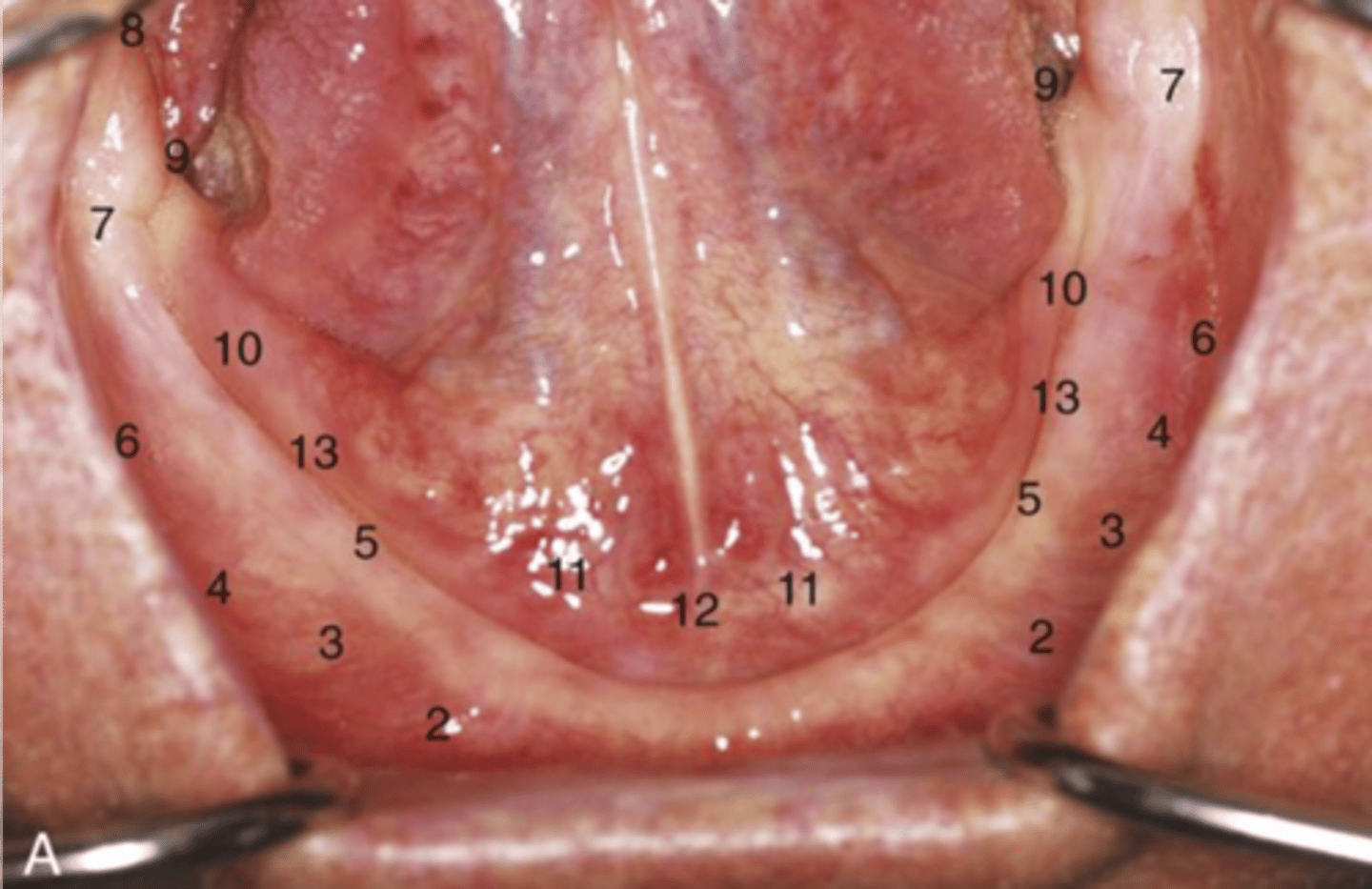
Buccal shelf
6
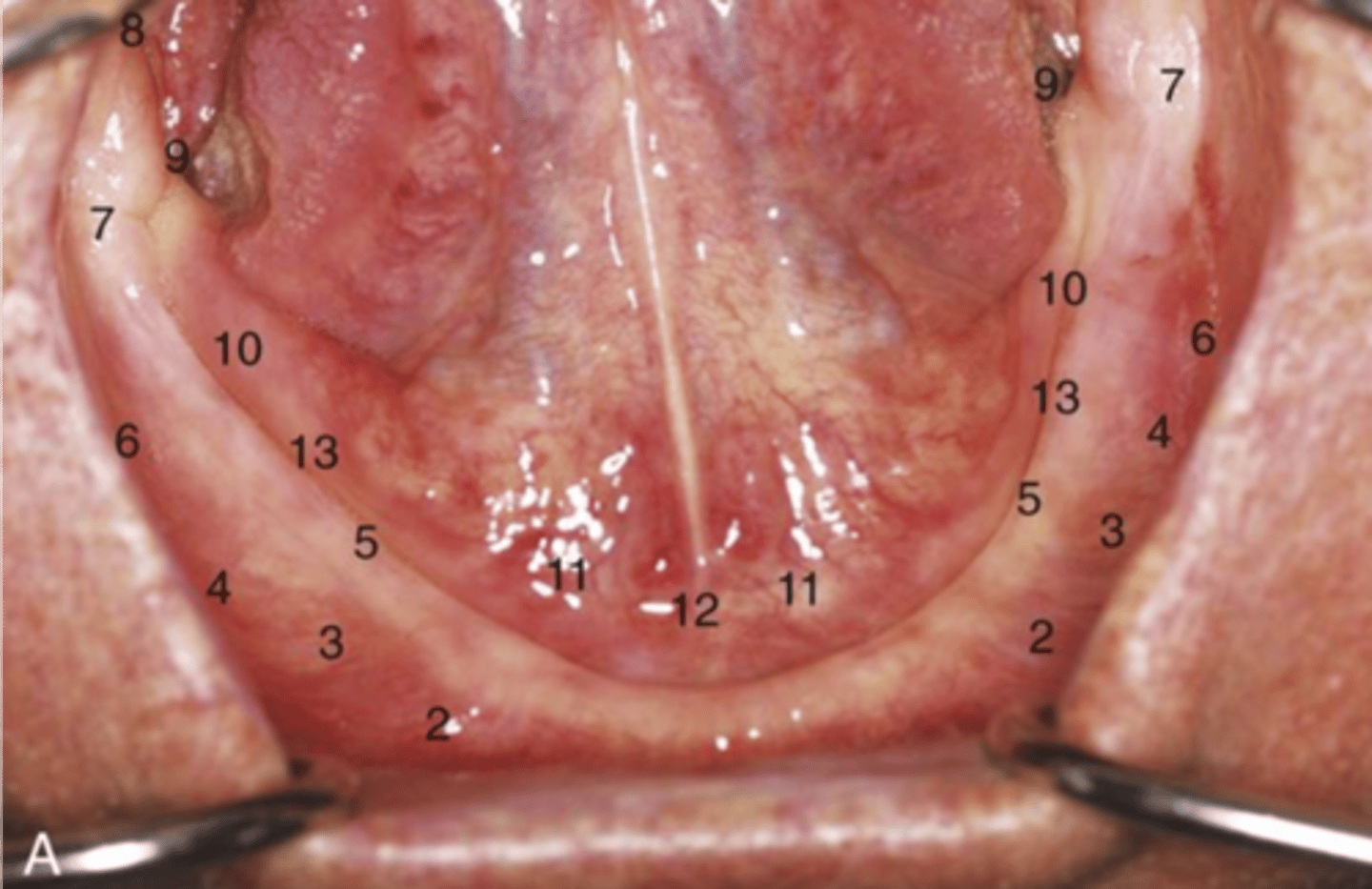
retromolar pad
7
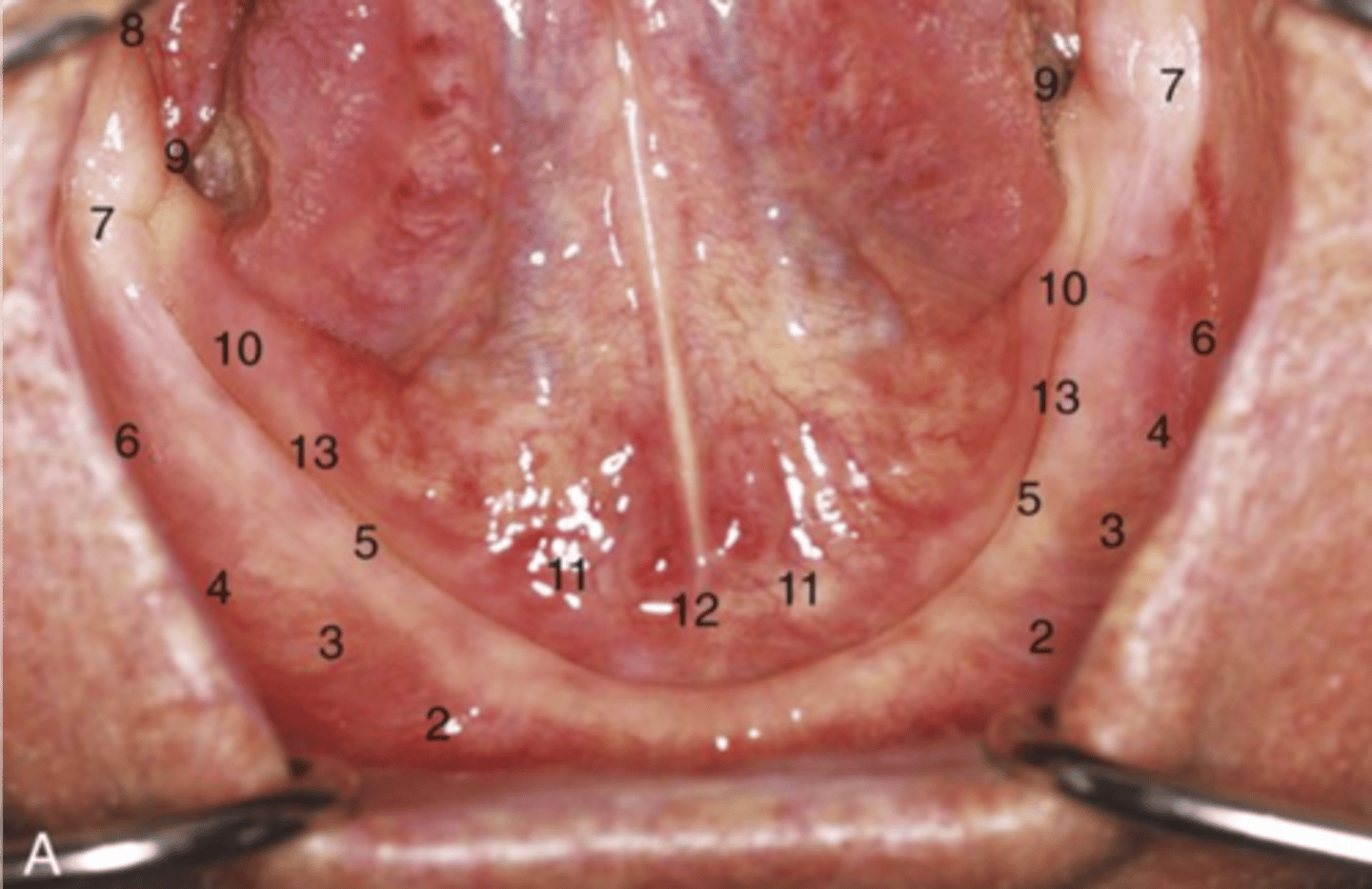
sublingual caruncle
11
An additional secondary support area is necessary on the mandible if
there are genial tubercles
Buccal frenulum
3
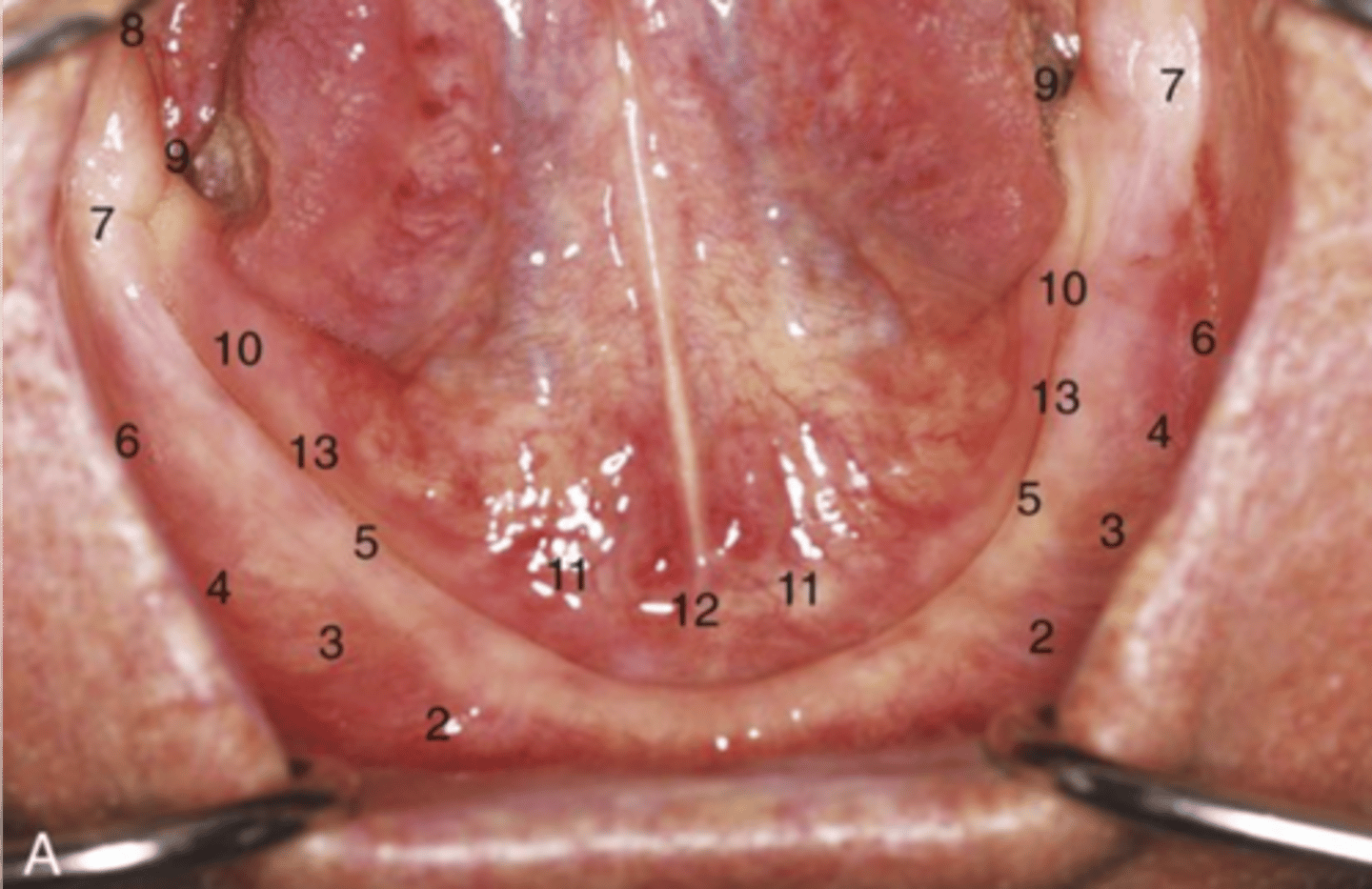
Premylohyoid eminence
13
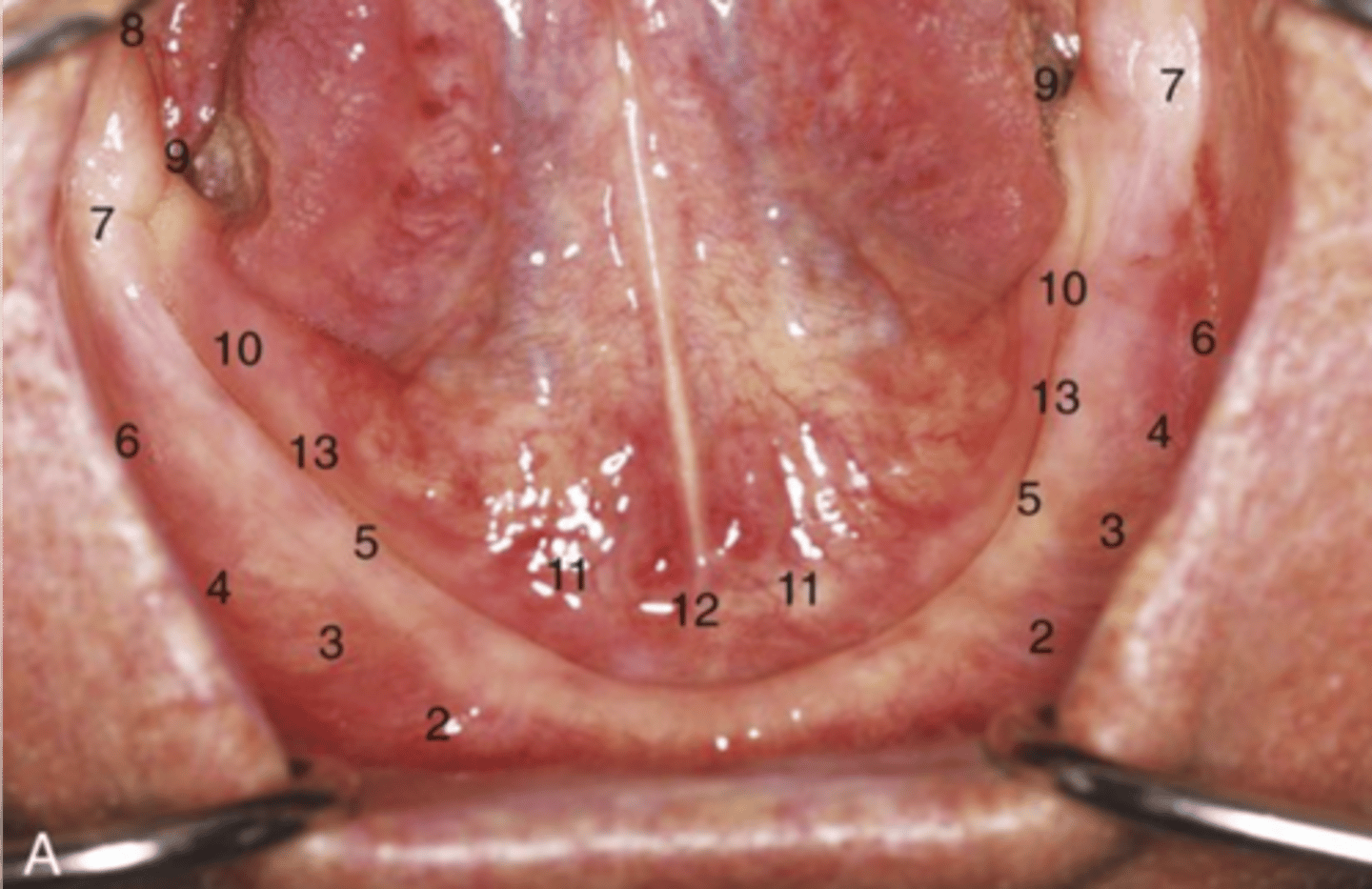
Relief zone for supporting a denture
premylohyoid eminence
retromylohyoid fossa
9
area critical to provide posterior retention of dentures on mandible
retromylohyoid fossa
Why does a mandibular denture gain retention in retromylohyoid fossa
the mandible has lingual bilateral undercuts
How do you insert a mandibular denture
initially more posterior to engage in retromylohyoid fossa and then sealing denture anteriorly last
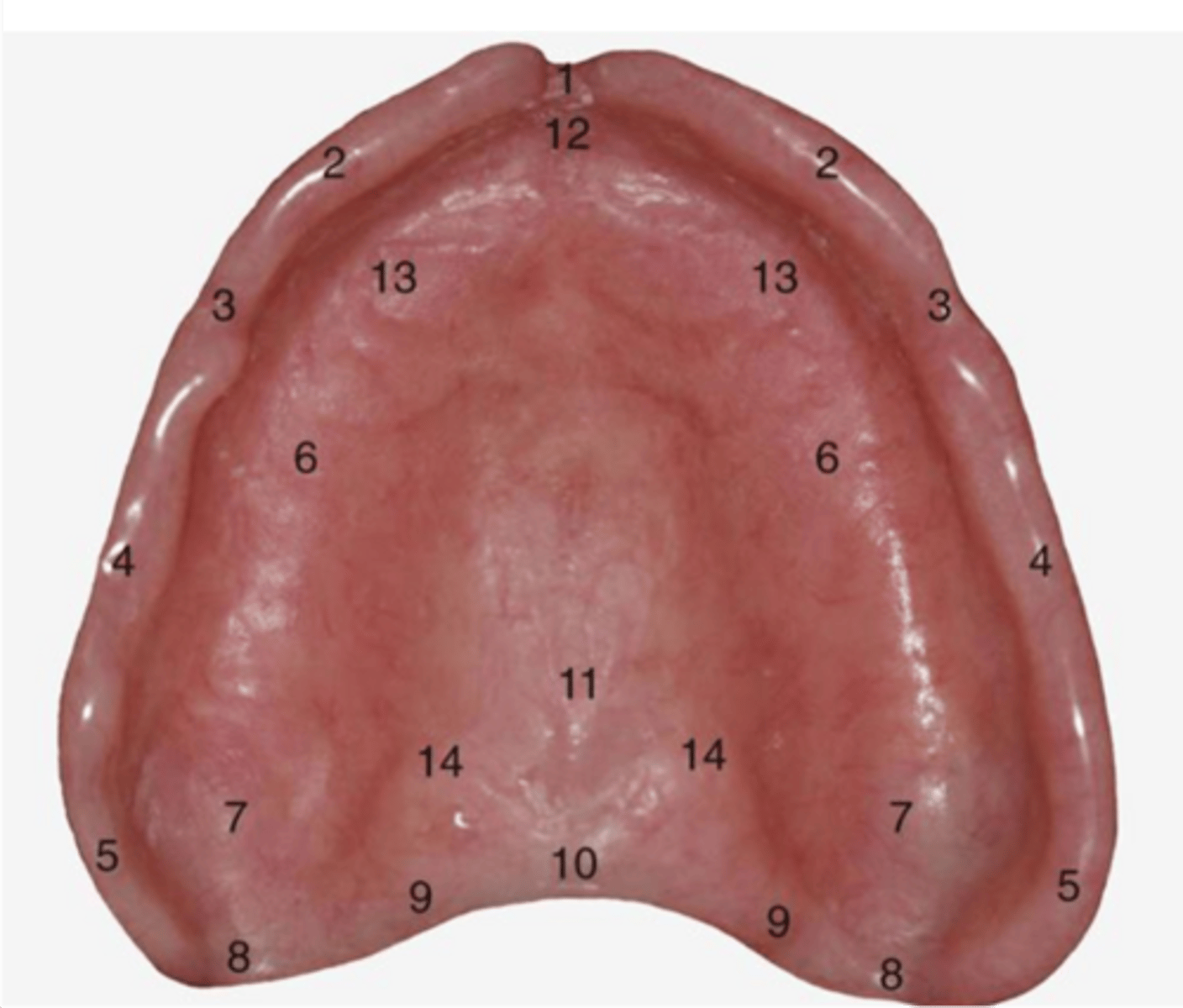
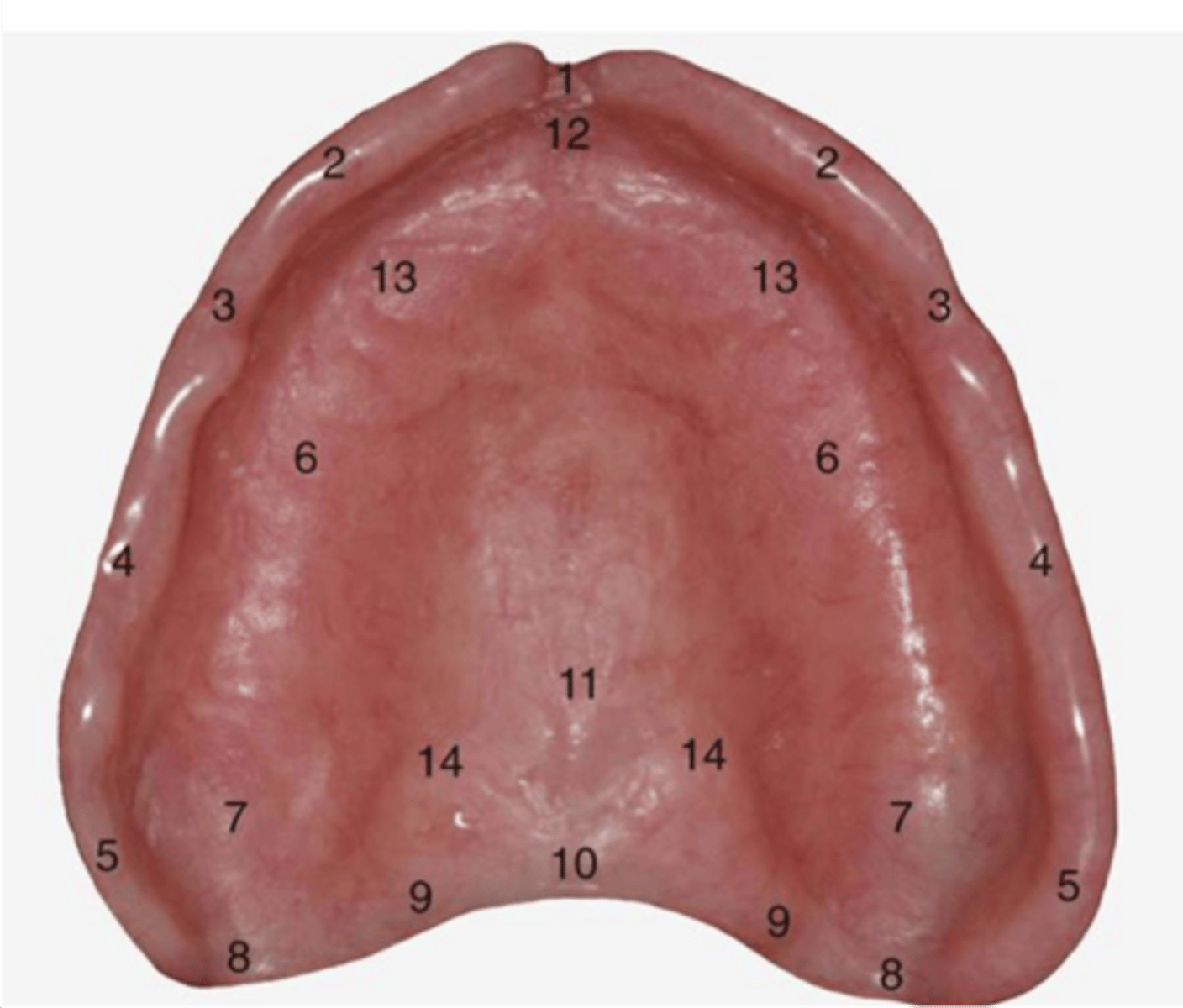
labial notch
1
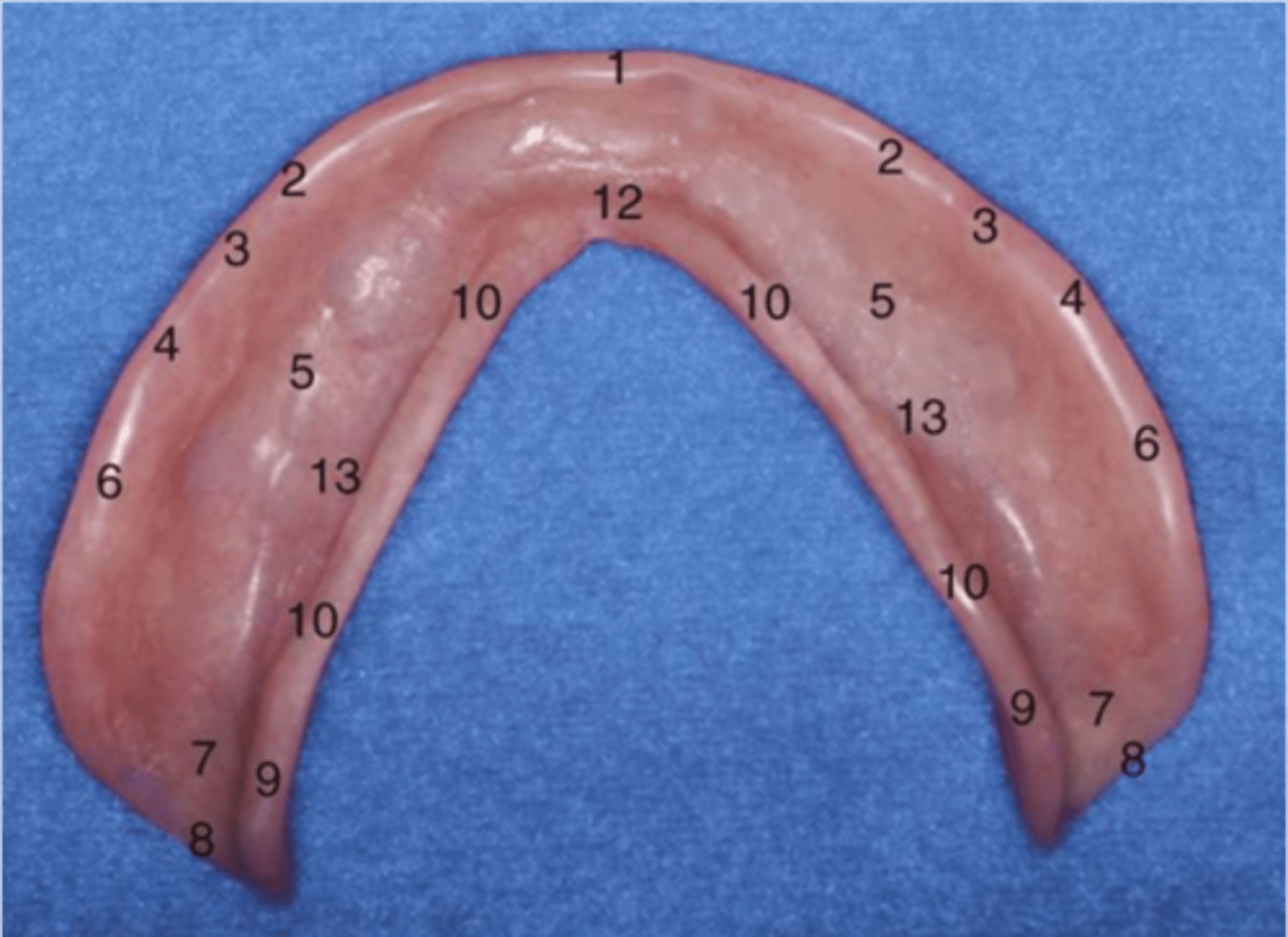
labial flange
2
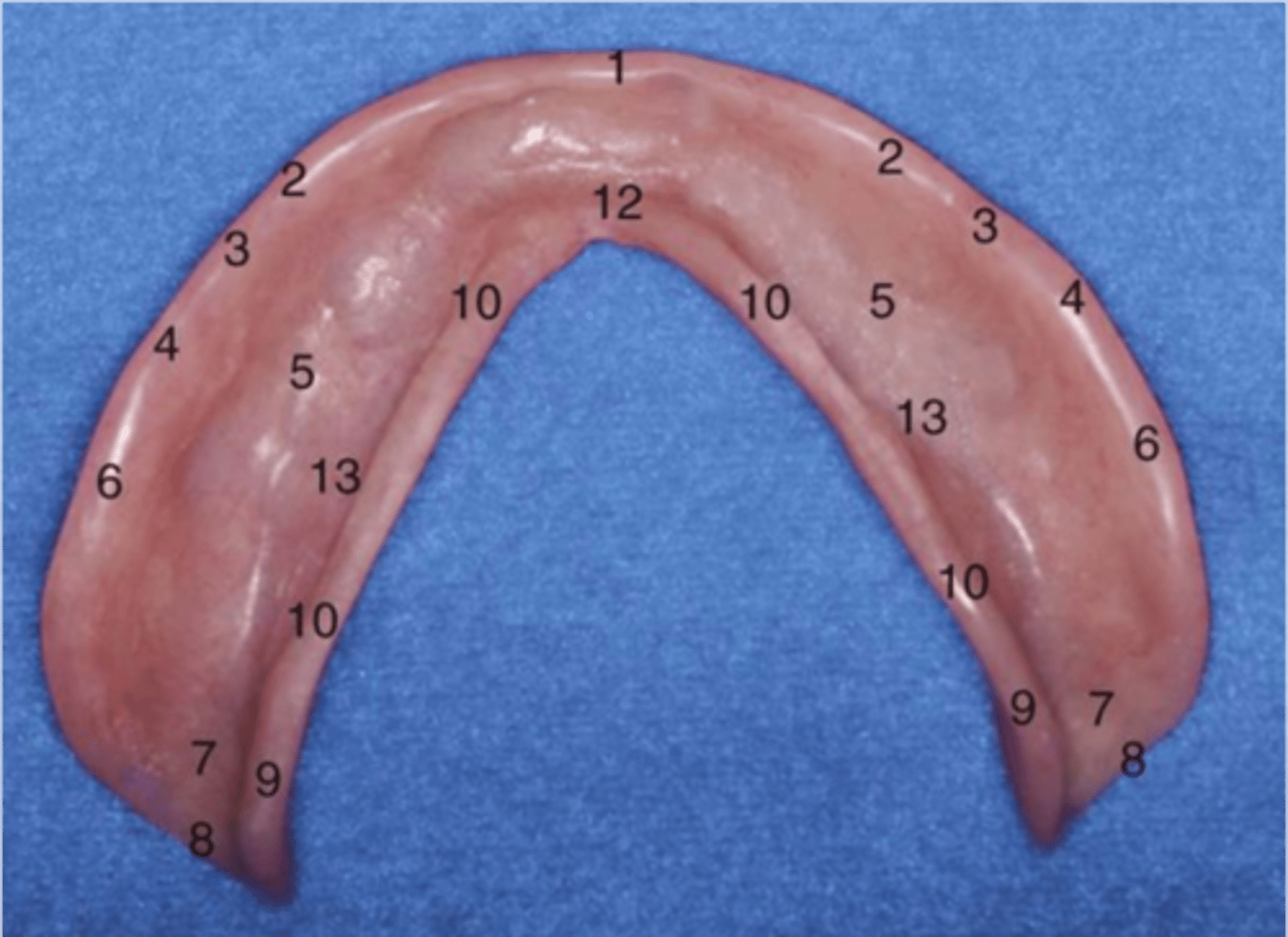
buccal notch
3
buccal flange
4
alveolar groove
5
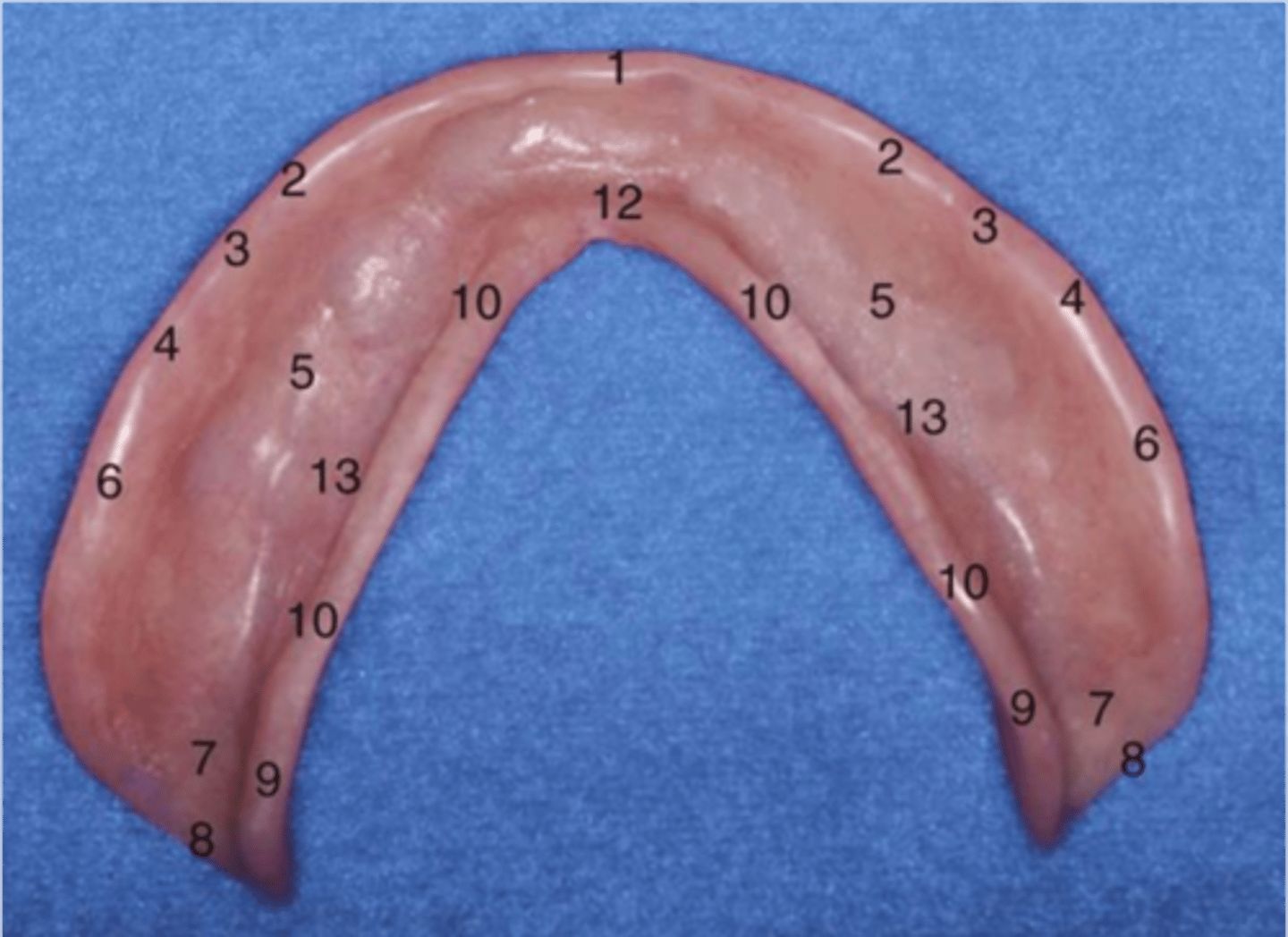
area of retromolar pad
7
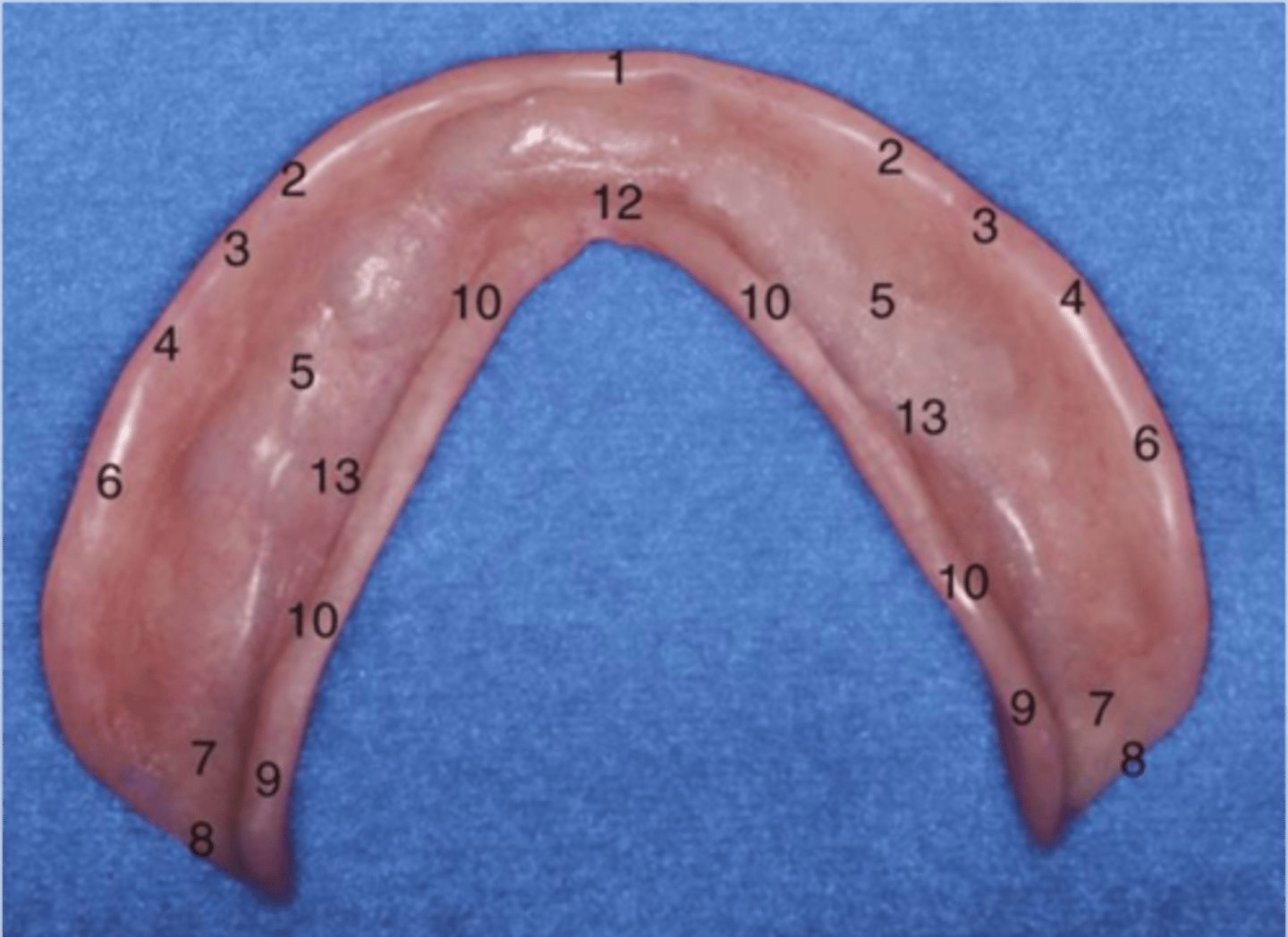
pterygomandibular notch
8
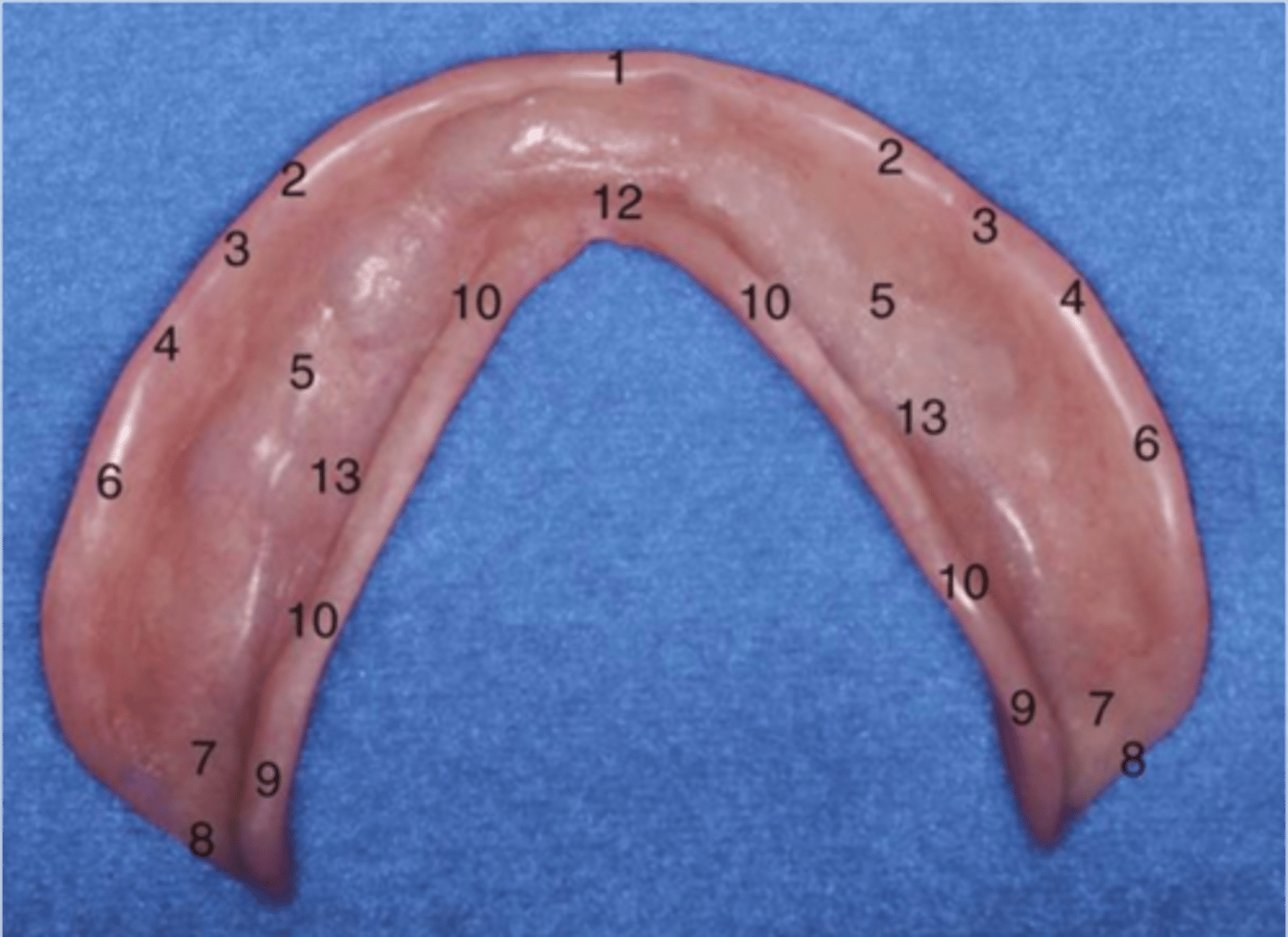
lingual flange
10
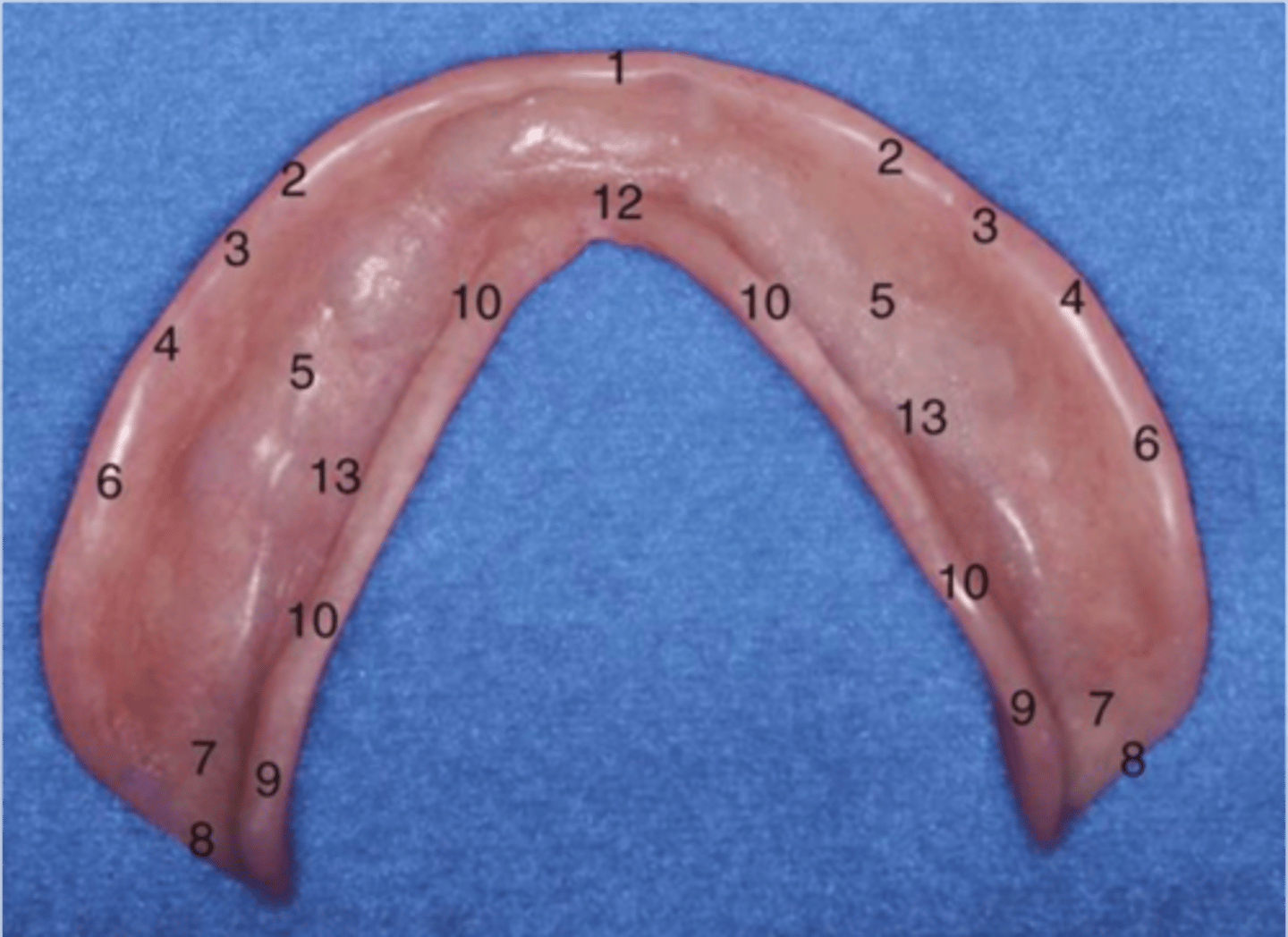
lingual notch
12
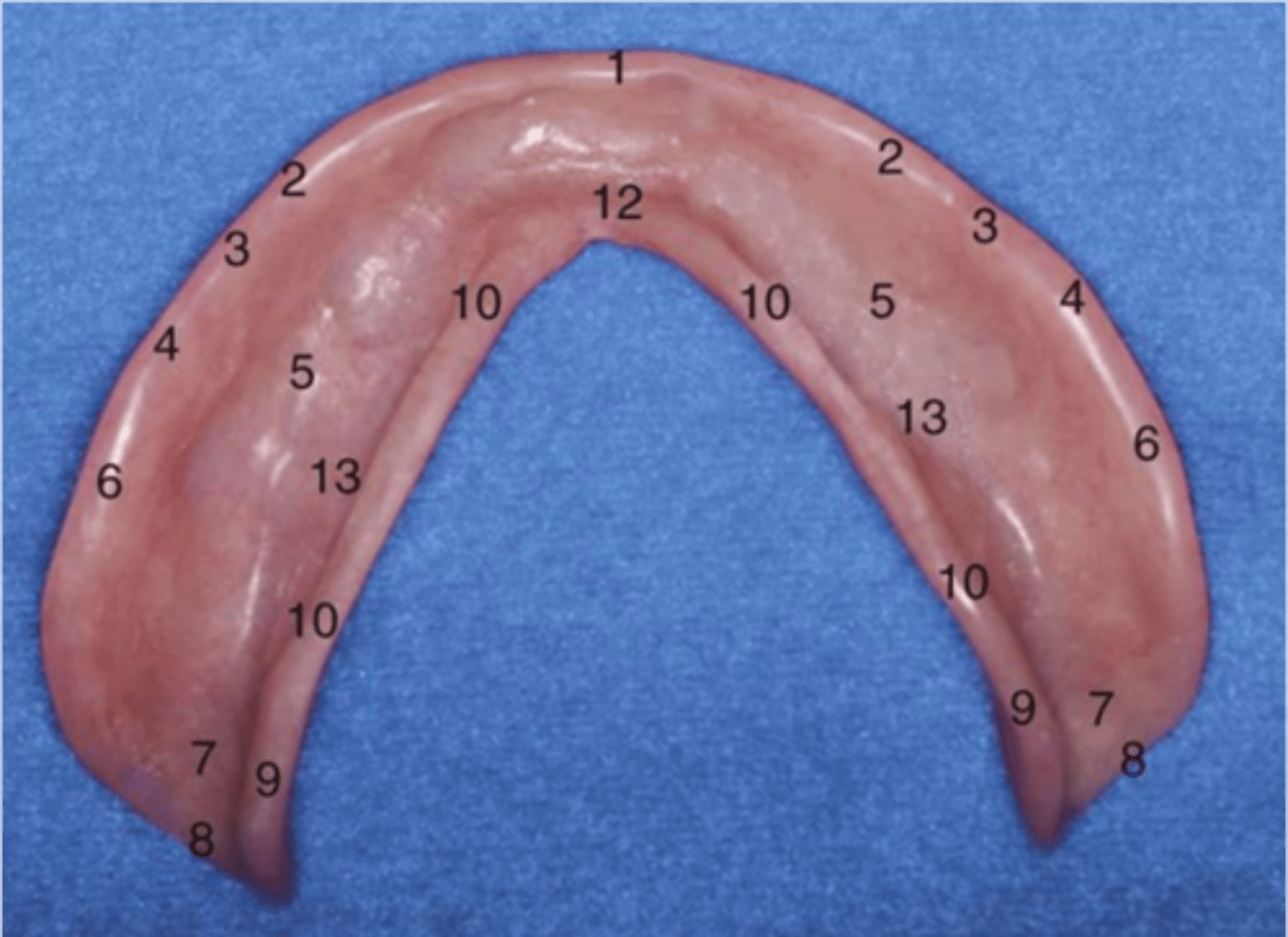
area of premylohyoid eminence
13
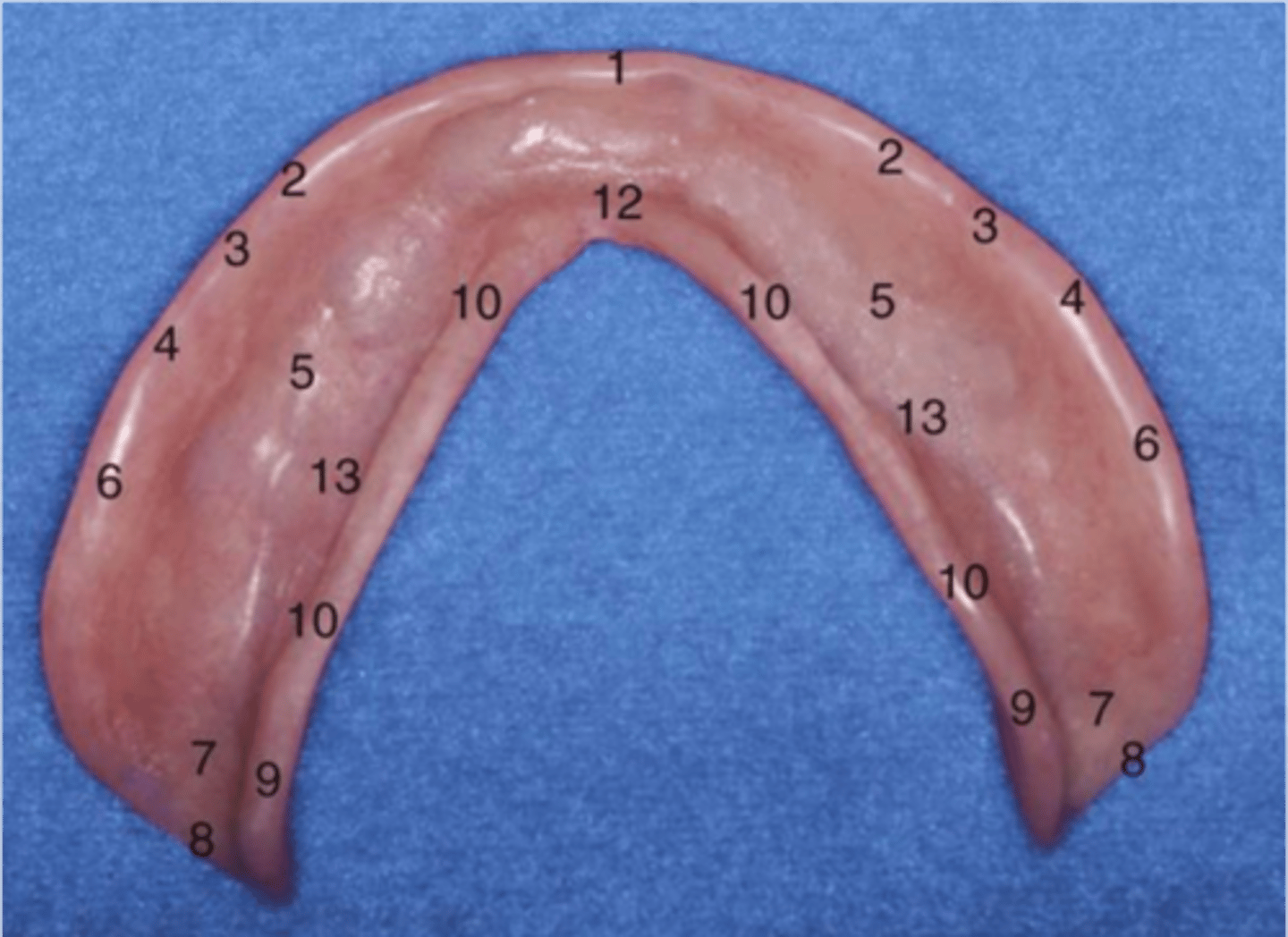
extension helps retain posterior of mandibular denture
posterior lingual flange
Intaglio surfaces
surface of denture facing tissues
Cameo surfaces
surface of denture exposed, with teeth
How do you obtain an accurate impression
impress healthy tissue, use properly fitting custom tray, select correct impression method and materials for the circumstance
T/F Tissue management comes after impressions
False
what is the key to an accurate impression
custum tray
Custom tray requirements
stable, rigid, extended, properly relieved
Anterior flabby ridge
hypermobility made obvious with movement toward suction tip. movable, hyperplastic fibrous tissue on the maxillary ridge, often causing poor denture stability, retention, and a lost peripheral seal
Relief
reduction or elimination of undesirable pressure or force
Maxillary custom tray will be used with what technique
selective pressure impression technique
Where do you relieve
areas not well equipped to deal with pressures exerted by prosthesis
Selective pressure technique
relief wax for secondary stress areas, and no relief wax in primary stress bearing areas
Custom trays should be ____ short of vestibule depth
2-3 mm
T/F you can proceed with border molding without checking tray extension and adjusting as needed
false
If the tray border does not feel smooth to _____, then it is far too sharp for the patients mucosa
finger tip
Over extended tray
tissue distortion during impression leading to unstable denture
Under extended tray
insufficient extension to denture bearing areas leading to lack of retention
What is paramount about border molding to achieving a good outcome
ability to record necessary range of function
most difficult area to record clinically when border molding
mandibular posterior lingual vestibule of retromylohyoid fossa
border molding
shaping of border areas by functional or manual manipulation of tissue to duplicate contour and size of vestibule
Purpose of border molding
establish accurate flange length and border thickness, achieve retention through border seal (maxillary)
materials used for border molding
green stick compound
Overheating green stick will
vaporize volatile components
Prolonged immersion of green stick in hot water
leach out volatile or soluble components and alter physical properties
what increases flow of green stick
wet kneading
what results in distortion of tissues being recorded in border molding
not adequately softened compound
T/F excessive wet kneading can increase flow qualities of hardened material at mouth temperature to a point where distortion may occur upon removal
T
Where should you start border molding
buccal flange
Mucostatic impression
non pressure technique of recording tissue in passive state with mouth open
is it possible to have true mucostatic impressions
no, except scanning
what impression material would you use for mucostatic impression technique
low or extra low viscosity- ZOE and impression plaster