Abomasal disorders
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
what is the abomasum? what does it do? anatomical location?
the “true stomach”, which produces and secretes juices required for digestion, located along the ventral midline
What are some abomasal diseases, categorized by their effect?
Outflow alteration
Displacement
LDA, RDA, volvulus
No displacement
impaction, intraluminal obstruction, extramural mass
loss of wall integrity
Ulceration
bleeding ulcers (type 1 and 2), perforating ulcers (type 3 and 4)
fistula
LDA
How common is it? what happens?
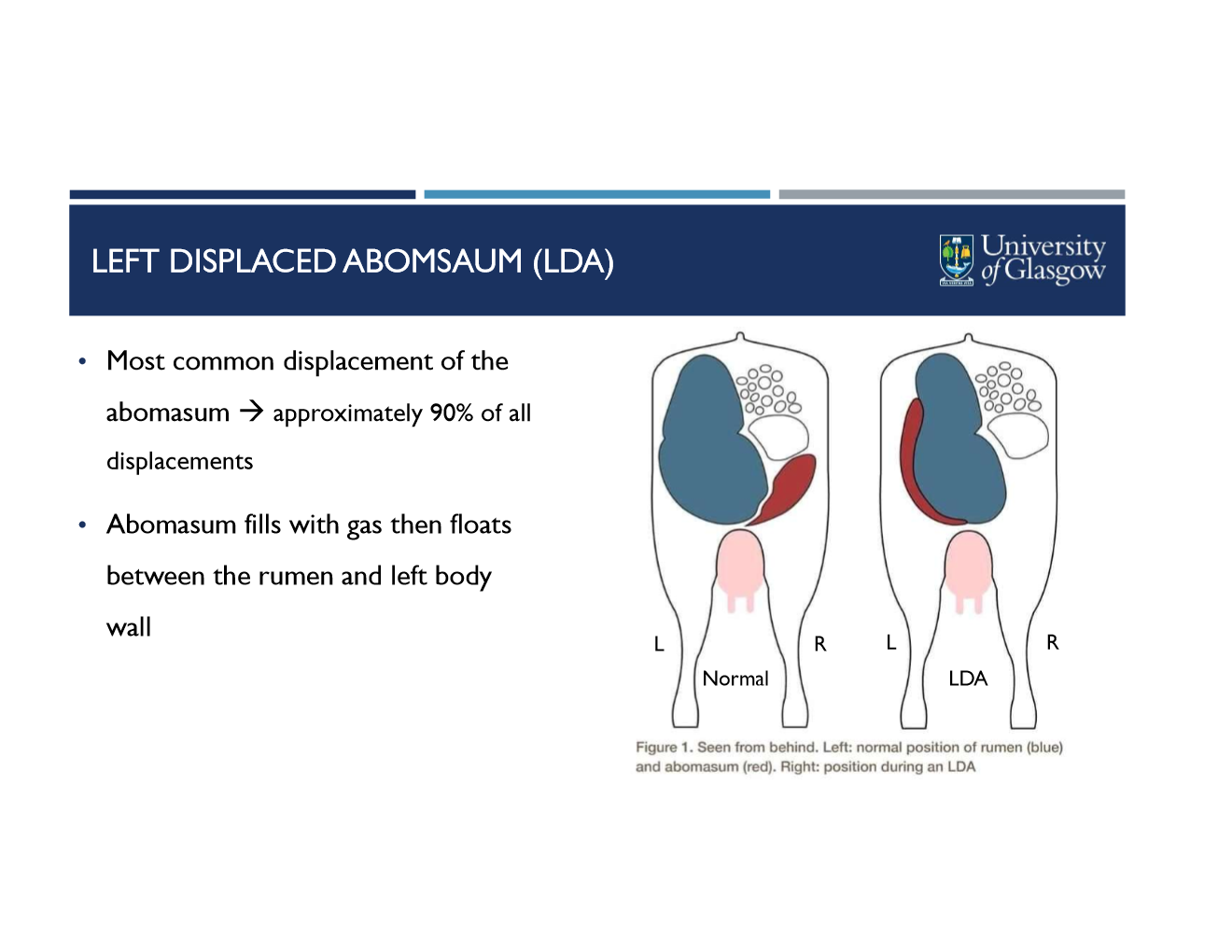
most common displacement (90% of all)
abomasum fills with gas then floats btwn rumen and left body wall
What are the cow and management risk factors of LDA?
Cow
breed- dairy (esp holsteins)
age- older cattle, less risk in primiparous/heifers
stage of lactation
57% occur 2 weeks postpartum
80% occur within 4 weeks
inc risk with production levels
concurrent disease
infectious disease (mastitis, metritis, enteritis, lameness)
metabolic disease (hypocalcemia, negative energy balance)
management
transition cow nutrition- reduced DMI or high concentrate intake during pre calving
transition cow environment- calving pen management, overstocking, poor feeding management
LDA
History and clinical exam findings?
history
reduced feed intake
drop in milk production
decline in rumination time
recent calving
concurrent postpartum disease
clinical exam
ping on auscultation and ballotement
dull demeanor
TPR normal (usually)
± abnormal feces or dehydration
LDA
Diagnostic techniques? how do you locate the site to auscultate?
DX techniques
abdominocentesis (where ping is located)
pH <3.5
No protozoa
Ultrasound
scan last 3 intercostal places
exploratory laparotomy
Auscultation
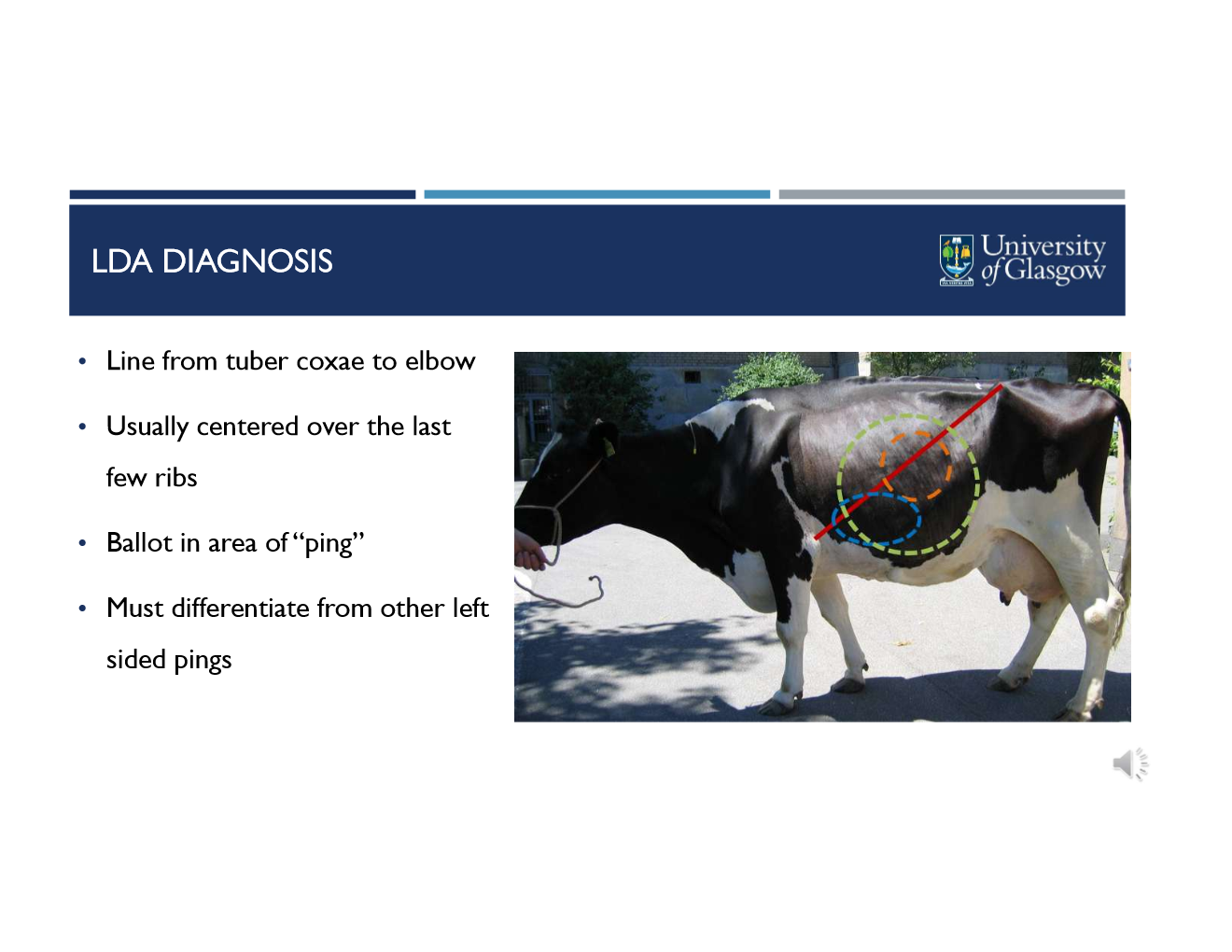
line from tuber coxae to elbow
usually centered over the last few ribs
ballot in area of “ping”
must differentiate from other left sided pings
LDA
what is the goal incidence rate in a herd? when should you investigate and what are you investigating in herd level cases?
target is <3% incidence
investigate if
overall anual LDA >2%, several cases in short time (cluster)
investigate- transition cow management and nutrition
LDA
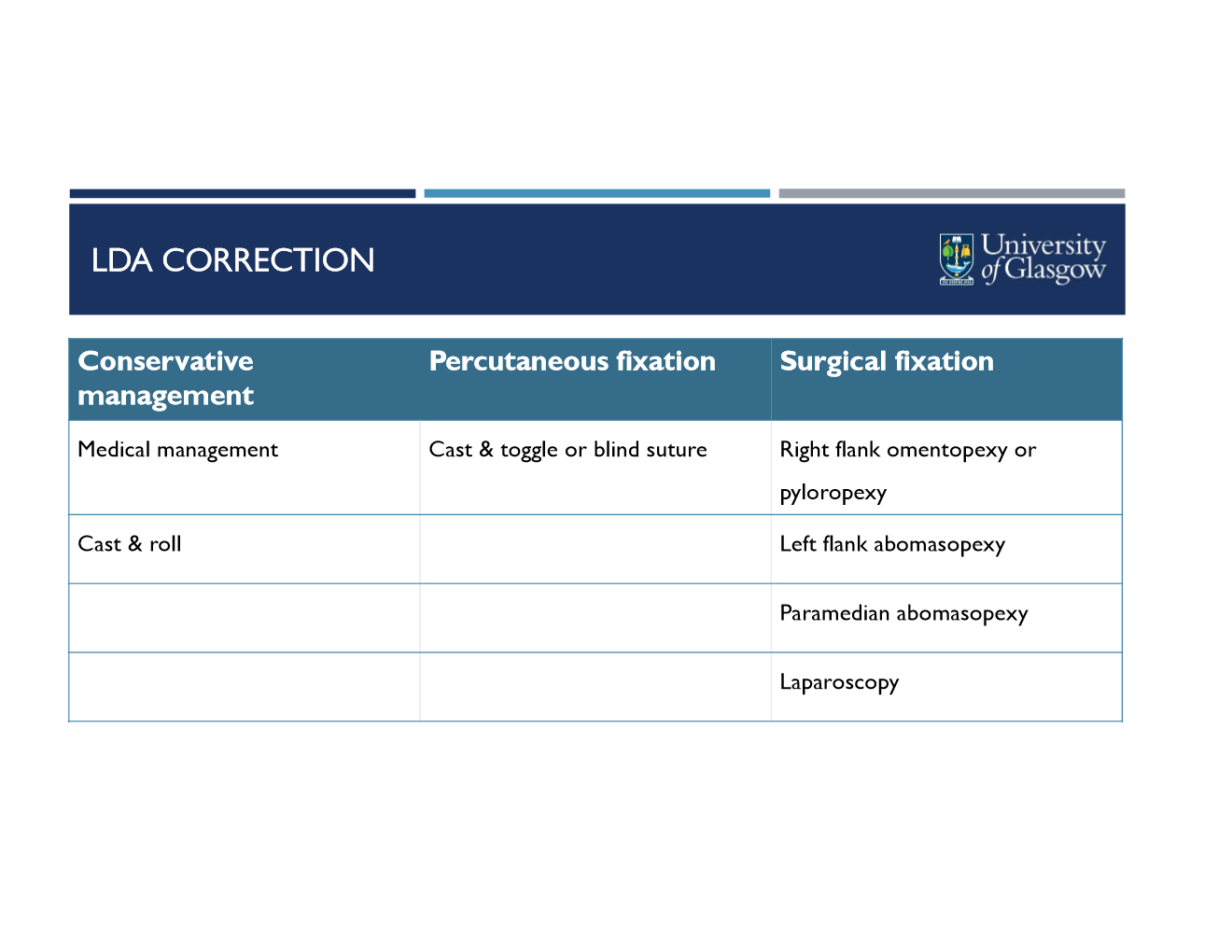
how is it corrected?
LDA
what are the steps to casting a cow?
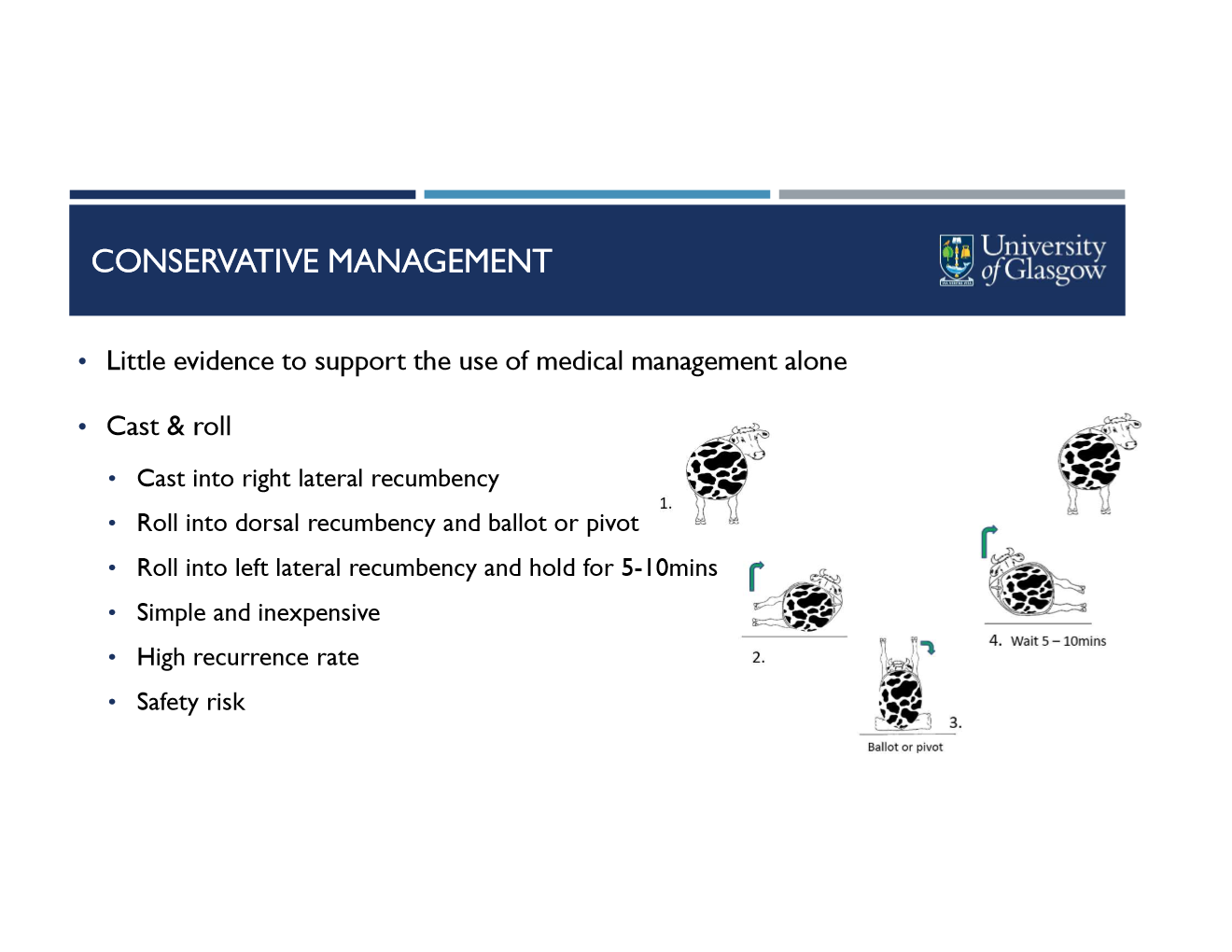
cast into right lateral recumbency
roll into dorsal recumbency and ballot or pivot
roll into left lateral recumbency and hold for 5-10 mins
it is conservative management!
simple and inexpensive
high recurrence rate
high recurrence rate
safety risk
LDA
How would you conduct a percutaneous fixation?
cast into dorsal recumbency
clip and surgical scrub from sternum to umbilicus
instill 10-20ml local anesthetic at surgical sites
one hand caudal to sternum
one hand cranial to umbilicus
both to right of midline (avoid mammary vein)
identify ping (while in dorsal recumbency still)
insert trocar at caudal site, push toggle through then clamp suture end to hold
move 10cm up to cranial site and repeat process
tie both suture together loosely
leave one hands width btwn suture and body wall (risks necrosis if too tight)
roll cow clockwise into sternal recumbency
LDA
what are pros and cons of percutaneous fixation?
Advantages
quick and easy, minimal specialist equipment, inexpensive
Disadvantages
safety risk (casting and rolling)
labour (+2 staff)
risk of ventral fistula formation
blind technique soooo risk of incorrect fixation
wrong abomasal position
fix to other viscera
→ obstructions or peritonitis
LDA Surgery
What medications for surgical correction?
broad spectrum antibiotics
NSAID
Calcium
± fluid therapy
LDA Surgery
what is involved in pre-op prep?
adequate restraint
regional anesthesia
line block, inverted L, paravertebral (proximal or distal)
surgical clip and prep
LDA Surgery
What occurs in the right flank approach?
standard prep, anesthesia, and right flank incision
explore abdomen
Locate then deflate abomasum
using left arm, reach caudally around the rumen to find the abomasum (between rumen and body wall)
palm needle and tubing then insert at an angle to defate
reposition abomasum
reach cranioventrally and locate the omentum/pylorus
pull gently towards incision
Omentopexy
locate the “sow’s ear” in omentum
locate abomasum and position pexy 3-5 cm from pylorus
suture a wide vertical section of omentum
include omentum in peritoneum and transversus muscle suture
use appropriate suture material
Pyloropexy
suture muscular part of pylorus to incision site (don’t enter pyloric lumen)

LDA Surgery
what are advantages and disadvantages of right flank approach?
advantages
standing animal
no assistants needed
good access for abdominal exploration
ensures correct fixation of omentum or abomasum
disadvantages
more difficult technically
more invasive surgery (risk of infection in wound or peritoneum)
risk of recurrence if pexy fails
wrong position
omentum too friable
risk of pyloric stenosis (pyloropexy)
LDA Surgery
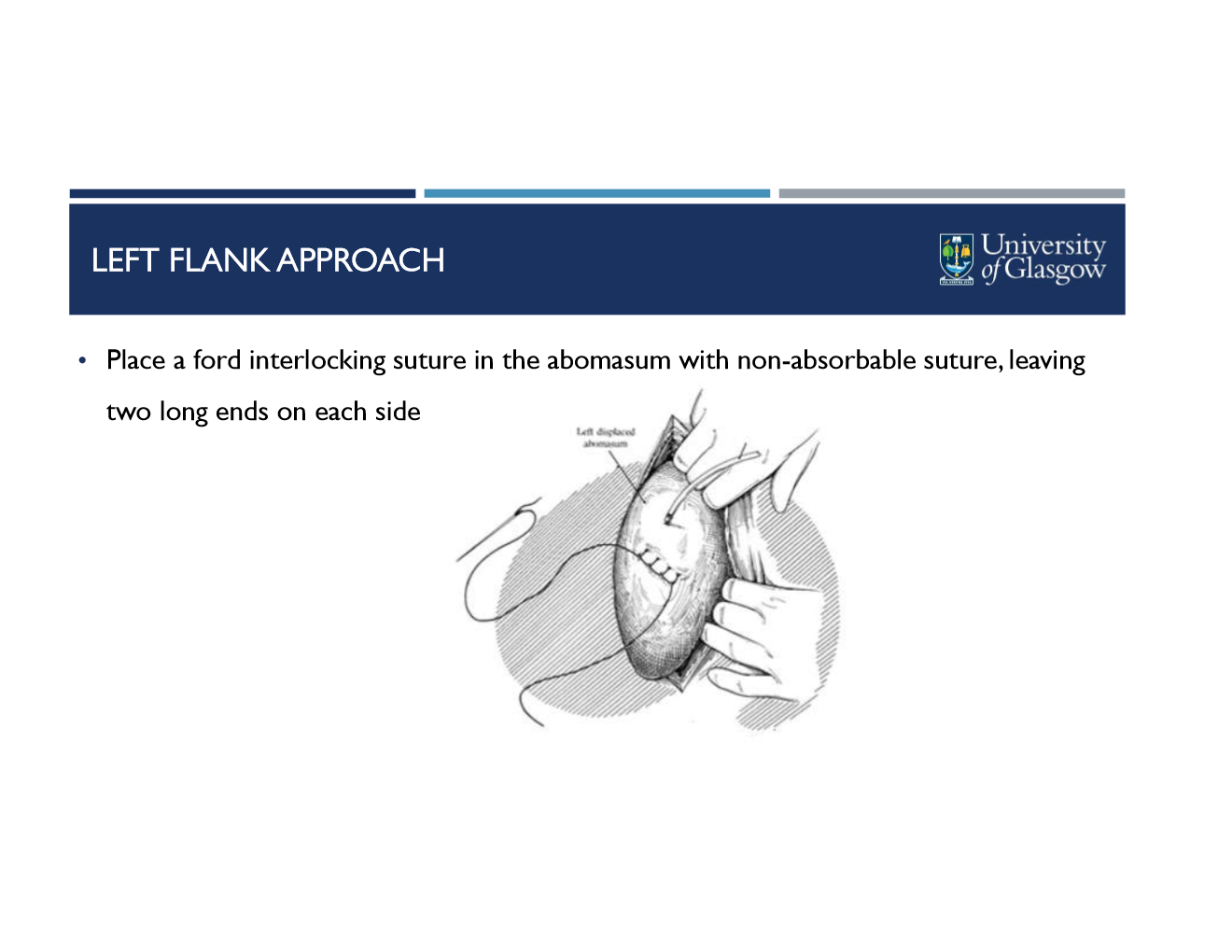
What occurs in the left flank approach?
standard prep and anesthesia for left flank
clip, prep, and mark ventral abdomen (20cm caudal to sternum)
left flank incision more cranial and ventral
visualize, exteriorize, and decompress abomasum
place ford interlocking suture in greater curvature of abomasum with non-absorbable suture, leave two long ends on either side
pass each long end thru ventral abd wall- 5 cm apart
push abomasum ventrally while assistant pulls gently on sutures then ties ends
LDA Surgery
what are advantages and disadvantages of left flank approach?
advantages
standing animal
good access to abomasum (can treat adhesions or ulcers if needed)
ensures direct fixation of abomasum
best technique in pregnant animals (more space)
disadvantages
technically mroe difficult
requires assistant
risk of ventral fistula formation
risk of damage to milk vein
LDA Surgery
what occurs in the paramedian approach?
cast into dorsal recumbency
clip and surgical scrub from sternum to umbilicus then local anesthetic line block
15 cm long incision to the right of midline about 10 cm caudal to sternum
suture the serous and muscular layers of abomasum of peritoneum/internal rectus abdominis layer
do not penetrate abomasal lumen
LDA surgery
what are advantages and disadvantages of paramedian approach?
advantages
easy relocation of abomasum
good access to abomasum (treat adhesions or ulcers)
disadvantages
safety risk with casting and rolling
risk of ventral fistula formation
risk of wound breakdown with subsequent herniation
contraindicated in pregnant cows
LDA surgery
what are advantages and disadvantages of laparoscopic approach?
Advantages
high success rate
quick procedure
minimally invasive
small wound
quick post-op recovery
visualize placement of toggles and position of abomasum
Disadvantages
specialist equipment needed
cost, maintenance
further training required
higher cost to farmer
RDA and RAV
How common is it? what happens?
less common than LDA
abomasum fills with gas and floats dorsally along right body wall (RDA)
RDA can flip across its long axis to form a volvulus (RAV)
volvulus may include omasum in severe cases
RDA and RAV
What are the risk factors?
higher risk in postpartum cattle
iatrogenic after rolling for LDA
RAV always thought to be consequence of uncorrected RDA
RDA and RAV
how do you diagnose them? clinical signs?
RDA history and clinical signs same as LDA
“ping” on auscultation, usually more cranial than LDA
differentiate from caecal/rectal gas
RAV more severe clinical signs
signs of colic
inc HR and RR
shock and endotoxemia signs
palpable distended viscus behind last rib
RDA surgery
How do you correct it surgically? prognosis?
they are surgical emergencies which must be corrected immediately
only right flank approach appropriate!
pre-sx is same as LDA
prognosis
good in simple displacement (RDA)
reduced with volvulus
very poor if volvulus includes omasum or reticulum
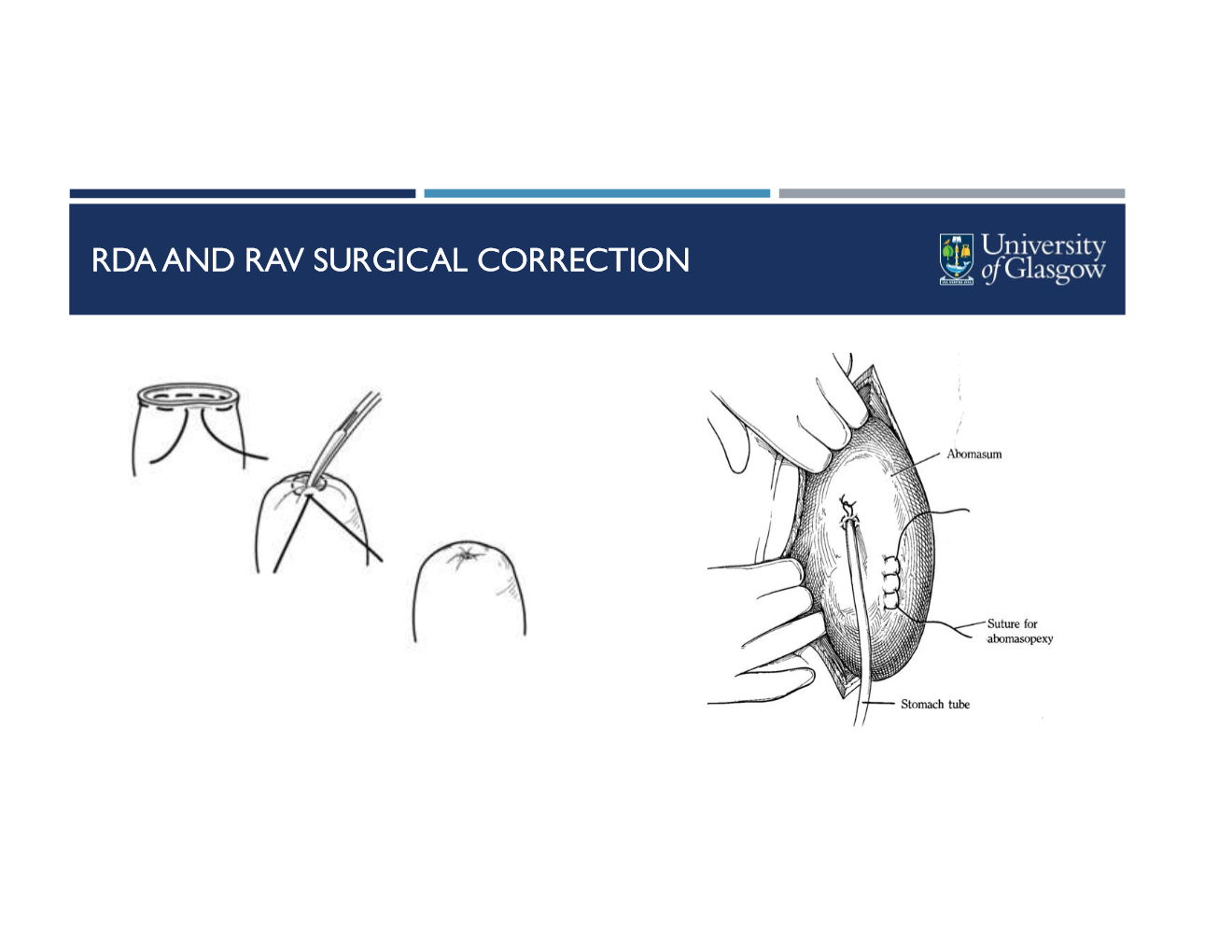
RAV surgery
how do you know its RAV? what are the additional steps (after all RDA steps)
follow grater omentum to abomasum, RDA is deflated and corrected as with LDA
place purse string suture in abomasum
stab incision into center of suture and instert tube
syphon fluid out
remove tube and pull purse string closed
correct volvulus
standard omentopexy
What are causes of abomasal impaction?
dietary
fibrous diet low in protein and energy
heavy ingestion of sand
poor water availability
non-dietary
abomasal hypomotility in postpartum dairy cattle
any cause of reduced abomasal outflow
vagal nerve damage
traumatic reticulopericarditis
what are clinical signs, diagnostic techniques, and treatment for abomasal impaction?
nonspecific clincal signs
inappetence, abdominal distension, reduced feces production or diarrhea
dx on feeding hx, abomasal ultrasound, or exploratory laparotomy
treatment
correct dehydration and electrolyte imbalances
mineral oil once daily (3-5 days)
surgical emptying of abomasum
what is the pathogenesis of abomasal ulceration?
production stress (early lactation and peak production)
management related stress
high acid, high energy diet
concurrent disease
no current link to use of NSAIDs in cattle
also seen in milk fed calves
what are the 4 types of abomasal ulceration and their definitions? clinical signs?
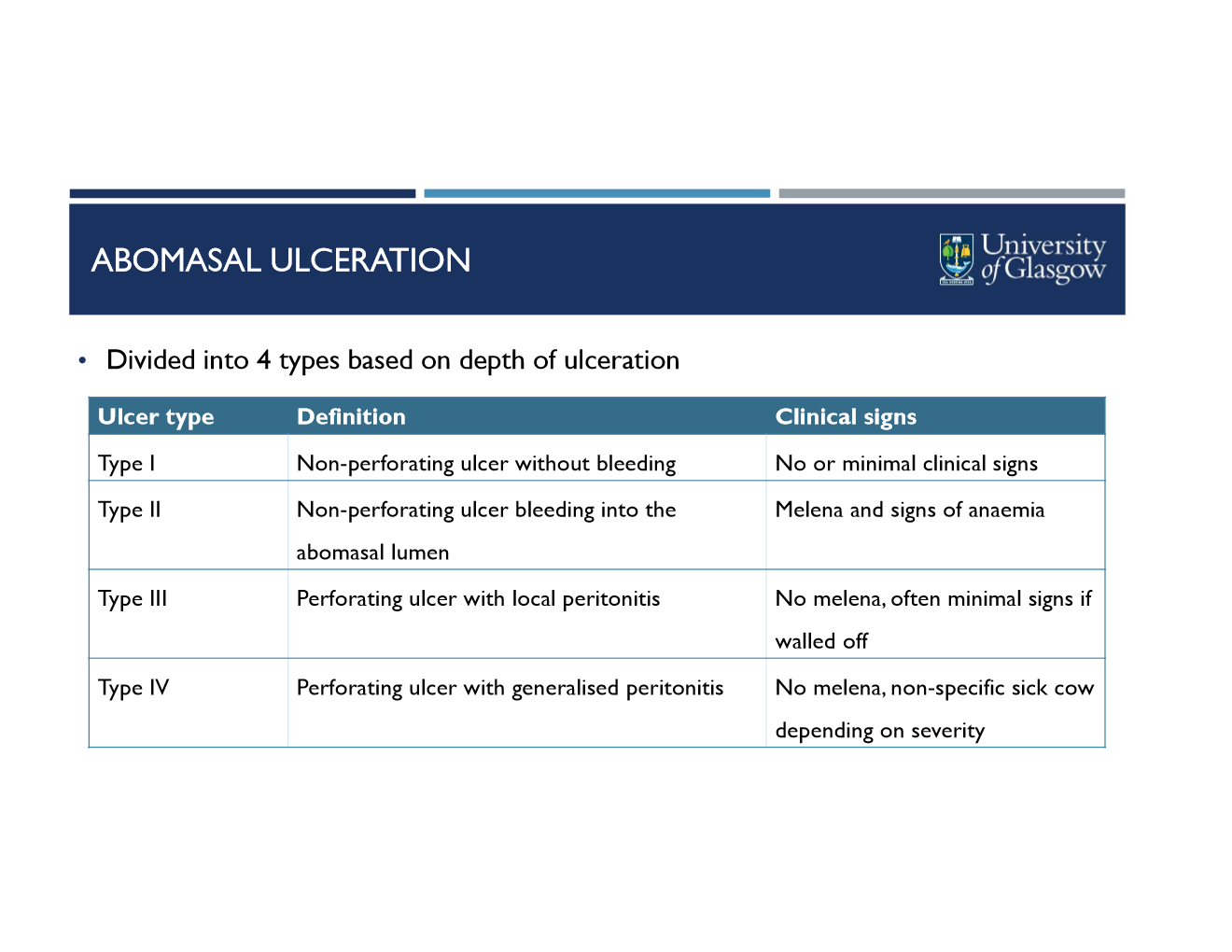
how do you diagnose abomasal ulceration?
clinical signs (melena, anemia)
fecal occult blood test
hematology and biochem
low PCV and total protein (type 2)
inflammatory response (type 3 and 4)
ultrasound ventral abdomen ± abdominocentesis
exploratory laparotomy
how do you treat abomasal ulceration?
high fiber diet
supportive therapy
blood transfusion (type 2)
oral antacids (magnesium oxide, aluminum hydroxide)
cimetidine, ranitidine
omeprazole (but not licensed in food producing UK animals)
Surgery (type 3 or 4)
abomasal fistula
how does it occur?
what are treatment options?
infrequently develops following abomasopexy
intraluminal suture placement allows leakage of abomasal content and weakening of incision
Treatment
supportive medical therapy to stabilize
surgical resection