Scapula mobilizations
1/47
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
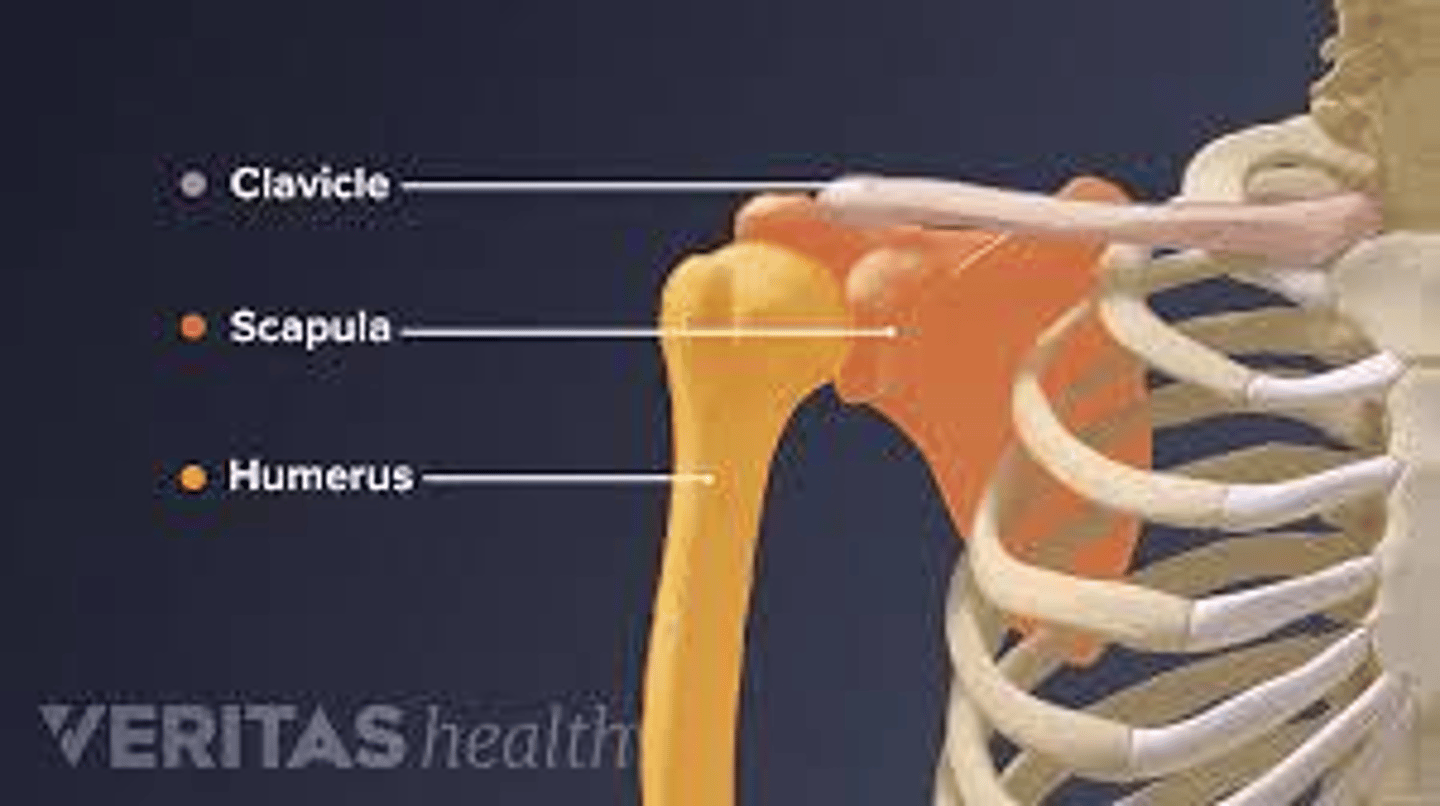
What are the three articulations of the scapula?
The clavicle, the humerus, and the posterior ribs.
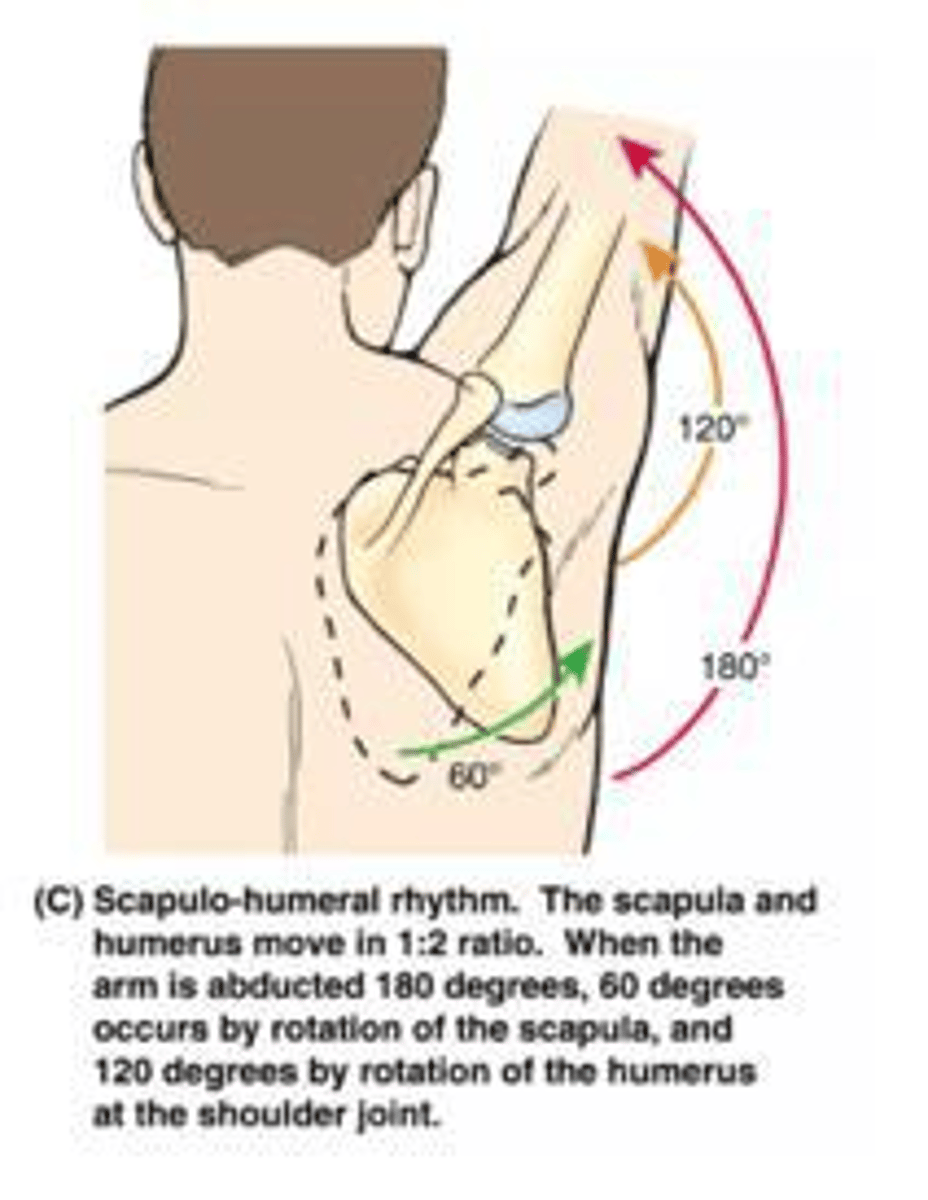
What is the generally accepted ratio for scapulohumeral rhythm?
1:2.
List the six movements of the scapula.
Elevation, depression, protraction, retraction, upward rotation, and downward rotation.
Which muscles are considered the primary scapular stabilizers?
Trapezius, serratus anterior, levator scapulae, rhomboids (major/minor), and pectoralis minor.
Which muscles are responsible for scapular elevation?
Upper trapezius and levator scapulae.
Which muscles are responsible for scapular protraction?
Serratus anterior and pectoralis minor.
What scapular movements occur during humeral abduction?
Upward rotation, posterior tilting, and external rotation.
What scapular movement is coupled with humeral internal rotation?
Scapular protraction (abduction).
What does the acronym SICK stand for in the context of scapular dyskinesia?
Scapular malposition, Inferior medial border prominence, Coracoid pain, and Kinesis abnormalities.
Which nerve injury is associated with a winging scapula?
The long thoracic nerve.
What is Snapping Scapula syndrome?
An audible or palpable clicking/grinding caused by the scapula rubbing against the rib cage.
Where is the inferior angle of the scapula typically located?
Close to the level of the T7 vertebra.
How do you locate the coracoid process during palpation?
1-2 finger breadths inferior to the lateral third of the clavicle, feeling for a hard, rounded, tender knob.
What is the purpose of scapular protraction/retraction manual techniques?
To improve reaching, pulling, and pushing activities, provide postural support, reduce guarding, and build trust.
What is the purpose of the Scapular Distraction manual technique?
To improve upward rotation of the scapula to facilitate better flexion/abduction of the shoulder.
In the side-lying position for scapular mobilization, where should the stabilizing hand be placed?
On the superior border or spine of the scapula.
What are the four PNF patterns for the scapula?
Anterior elevation, posterior elevation, anterior depression, and posterior depression.
Which muscle is associated with a soft tissue restriction in anterior elevation?
Latissimus dorsi.
Which muscles are associated with soft tissue restrictions in posterior depression?
Upper trapezius and levator scapulae.
What is the goal of active assisted upward rotation treatment?
To improve general mobility, proprioception, and positional tolerances of the scapula to improve shoulder AROM.
What is the correct patient positioning for scapular mobilization techniques?
Side-lying with neutral head, hips flexed, and ear aligned with the acromion and trochanter.
What is the progression for manual therapy scapular exercises?
Passive to active assistive to active to resisted.
What is the clinical significance of scapular humeral rhythm?
It allows for maximum motion of the upper extremity and provides shoulder stability.
What should be considered when addressing the scapula in exercise intervention?
Incorporating the core.
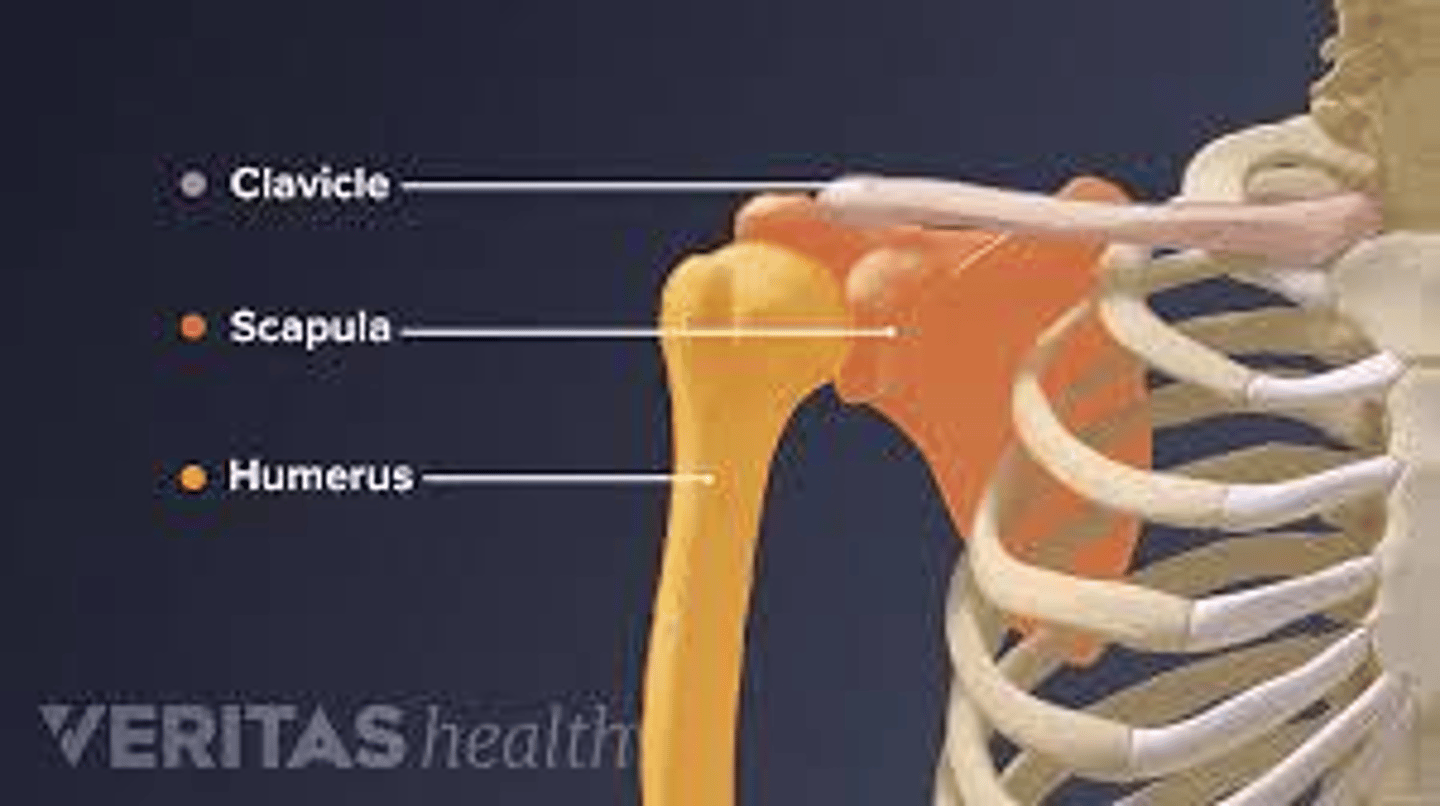
What are the three articulations of the scapula?
The clavicle, the humerus, and the posterior ribs.
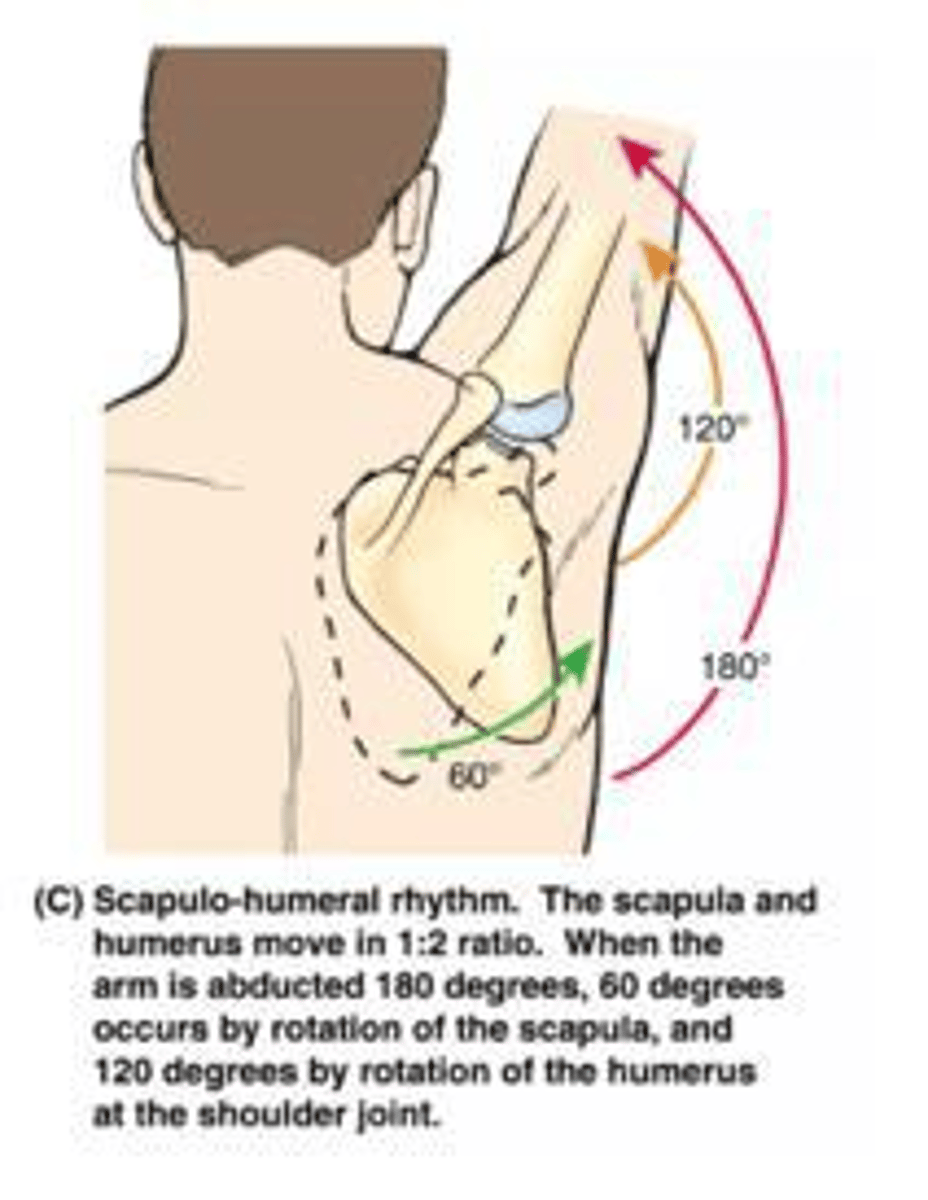
What is the generally accepted ratio for scapulohumeral rhythm?
1:2.
List the six movements of the scapula.
Elevation, depression, protraction, retraction, upward rotation, and downward rotation.
Which muscles are considered the primary scapular stabilizers?
Trapezius, serratus anterior, levator scapulae, rhomboids (major/minor), and pectoralis minor.
Which muscles are responsible for scapular elevation?
Upper trapezius and levator scapulae.
Which muscles are responsible for scapular protraction?
Serratus anterior and pectoralis minor.
What scapular movements occur during humeral abduction?
Upward rotation, posterior tilting, and external rotation.
What scapular movement is coupled with humeral internal rotation?
Scapular protraction (abduction).
What does the acronym SICK stand for in the context of scapular dyskinesia?
Scapular malposition, Inferior medial border prominence, Coracoid pain, and Kinesis abnormalities.
Which nerve injury is associated with a winging scapula?
The long thoracic nerve.
What is Snapping Scapula syndrome?
An audible or palpable clicking/grinding caused by the scapula rubbing against the rib cage.
Where is the inferior angle of the scapula typically located?
Close to the level of the T7 vertebra.
How do you locate the coracoid process during palpation?
1-2 finger breadths inferior to the lateral third of the clavicle, feeling for a hard, rounded, tender knob.
What is the purpose of scapular protraction/retraction manual techniques?
To improve reaching, pulling, and pushing activities, provide postural support, reduce guarding, and build trust.
What is the purpose of the Scapular Distraction manual technique?
To improve upward rotation of the scapula to facilitate better flexion/abduction of the shoulder.
In the side-lying position for scapular mobilization, where should the stabilizing hand be placed?
On the superior border or spine of the scapula.
What are the four PNF patterns for the scapula?
Anterior elevation, posterior elevation, anterior depression, and posterior depression.
Which muscle is associated with a soft tissue restriction in anterior elevation?
Latissimus dorsi.
Which muscles are associated with soft tissue restrictions in posterior depression?
Upper trapezius and levator scapulae.
What is the goal of active assisted upward rotation treatment?
To improve general mobility, proprioception, and positional tolerances of the scapula to improve shoulder AROM.
What is the correct patient positioning for scapular mobilization techniques?
Side-lying with neutral head, hips flexed, and ear aligned with the acromion and trochanter.
What is the progression for manual therapy scapular exercises?
Passive to active assistive to active to resisted.
What is the clinical significance of scapular humeral rhythm?
It allows for maximum motion of the upper extremity and provides shoulder stability.
What should be considered when addressing the scapula in exercise intervention?
Incorporating the core.