Basal Ganglia
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
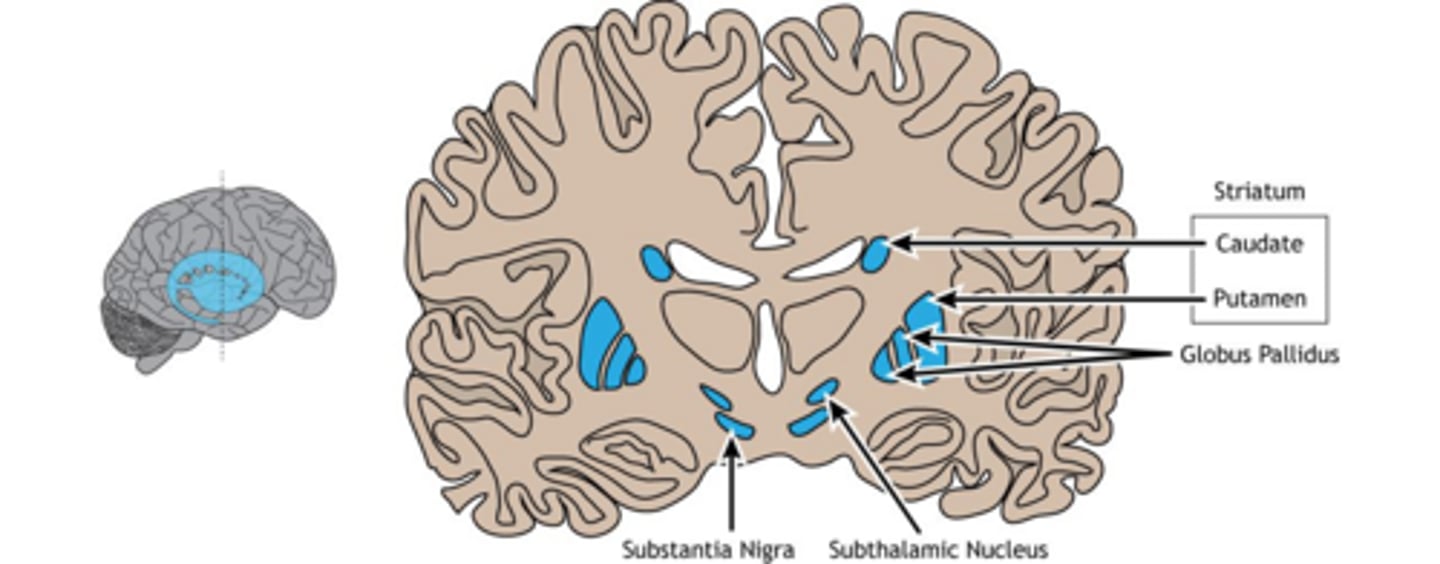
Which structures comprise the striatum?
The caudate nucleus and the putamen.
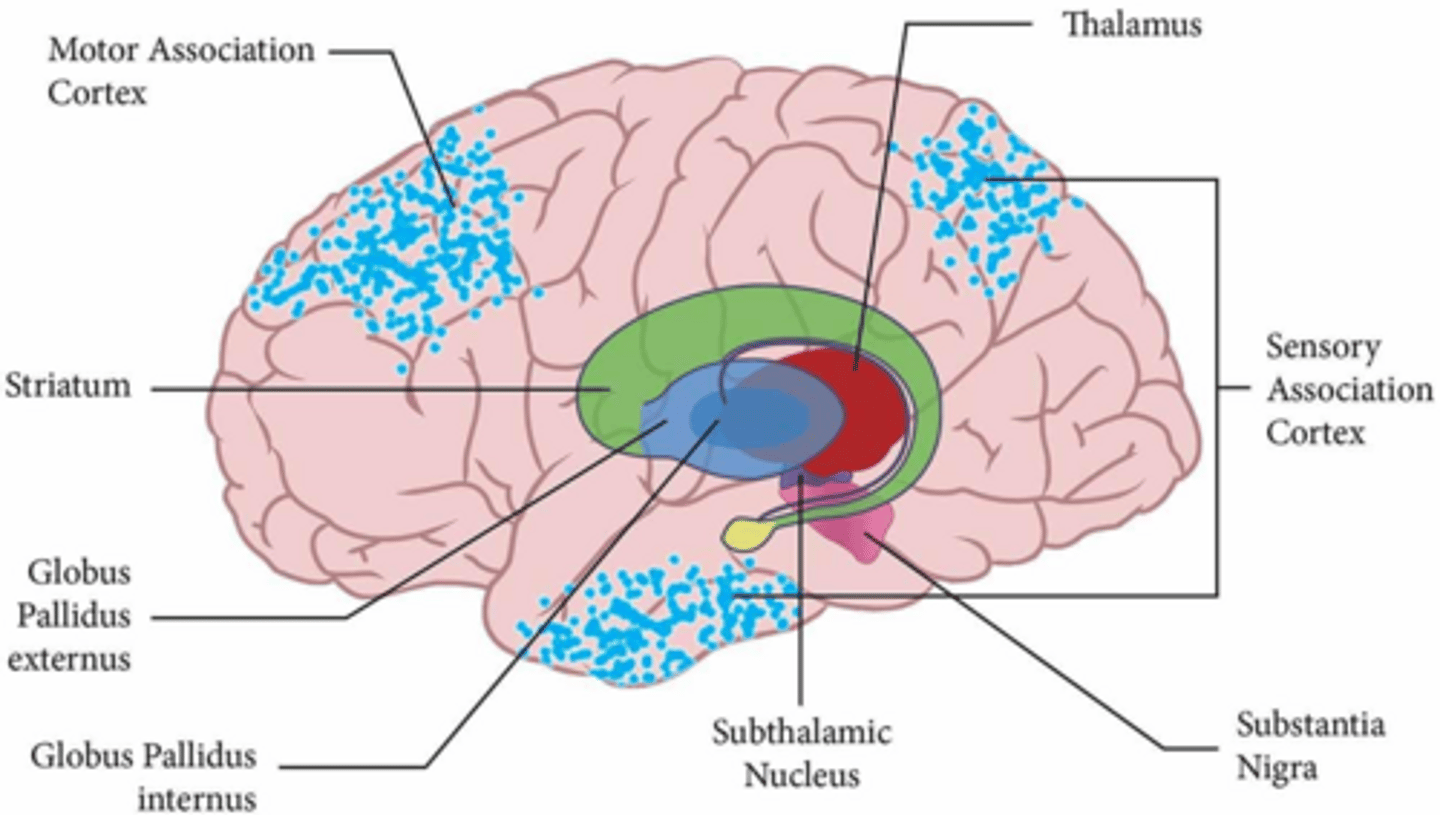
What is the primary function of the substantia nigra pars compacta?
It produces dopamine, which is essential for motor learning and reinforcing successful movement patterns.
What is the primary role of the indirect pathway in the basal ganglia?
To inhibit movement and suppress unwanted or competing motor patterns.
What is the primary role of the direct pathway in the basal ganglia?
To facilitate movement by disinhibiting the thalamus.
What is the mnemonic for the direct pathway's function?
DO IT (Direct = Output/Initiation).
What is the mnemonic for the indirect pathway's function?
INHIBIT IT.
What are the four classic clinical signs of Parkinson's disease (TRAP)?
Tremor, Rigidity, Akinesia/Bradykinesia, and Postural Instability.
What is the hallmark gait symptom of Parkinson's disease involving short, rapid steps?
Festination.
What is 'en bloc' turning in Parkinson's disease?
Turning the body as one rigid unit with minimal trunk and head dissociation.
How does dopamine affect the direct and indirect pathways?
Dopamine excites the direct pathway (via D1 receptors) and inhibits the indirect pathway (via D2 receptors), resulting in a net promotion of movement.
What is the primary pathophysiology of Parkinson's disease?
Loss of dopamine-producing neurons in the substantia nigra pars compacta, leading to decreased direct pathway activity and increased indirect pathway activity.
What is the primary pathophysiology of Huntington's disease?
Degeneration of medium spiny neurons in the striatum, leading to a loss of the indirect pathway and subsequent hyperkinesia (chorea).
What are common PT interventions for Parkinson's disease?
External cueing (visual/auditory), LSVT BIG, treadmill training, balance training, and dual-task training.
What is the difference between A-delta and C fibers in pain transmission?
A-delta fibers transmit fast, sharp, localized pain; C fibers transmit slow, dull, aching, diffuse pain.
What is the primary ascending pathway for pain transmission?
The spinothalamic tract (anterolateral system).
What is the Gate Control Theory of pain?
The concept that non-painful input (touch, pressure) can 'close the gate' to painful input at the dorsal horn of the spinal cord.
Which brain structure is responsible for the emotional response to pain?
The anterior cingulate cortex.
Which brain structure is responsible for the location and intensity of pain?
The somatosensory cortex.
What are the primary neurotransmitters involved in descending pain modulation?
Endorphins (opioids), serotonin (5-HT), and norepinephrine.
What is central sensitization?
A condition where the CNS becomes hypersensitive to pain, often seen in chronic pain conditions like fibromyalgia.
What characterizes neuropathic pain?
Burning, shooting, or electric-like sensations, often associated with nerve damage.
What is referred pain?
Pain perceived at a location other than the site of the painful stimulus, caused by visceral and somatic sensory convergence.
What is the role of the subthalamic nucleus (STN) in the indirect pathway?
It excites the GPi, which in turn inhibits the thalamus, effectively suppressing unwanted movement.
What happens to the thalamus when the GPi is inhibited?
The thalamus is disinhibited (less inhibited), becoming more active and sending excitatory signals to the cortex.
What is the primary difference in onset age between Parkinson's and Huntington's disease?
Parkinson's typically has an onset >60 years, while Huntington's typically has an onset between 30-50 years.
What is the clinical clue for nociceptive pain?
A mechanical pattern (local, aching pain).
What is the clinical clue for nociplastic pain?
Diffuse, persistent pain often accompanied by fatigue and sleep issues.