PHRX 4044 - Derm Exam #1 DR.A
1/122
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
123 Terms
describe non-melanoma
- malignant keratinocytes = SCC or BCC
- these are NOT melanocytes
- most common cancer in the US
describe melanoma
malignant pigment cells = melanocytes
what are the 5 general functions of the skin?
- protection
- antigen detection
- sensation
- synthesis of vitamin D
- thermoregulation
describe the cellular basis of the skin barrier
- epidermal cell properties
- contains cell-cell and cell-matrix connections and extracellular lipids
describe epidermal renewal and repair
- stem cell replication
- hyperprolifertaive pathologies
what are 3 skin adnexal structures?
- hair and sebaceous glands
- nails
- sweat glands
overall, describe the epidermis
- contains keratinocytes, melanocytes and langerhans cells
- basic structure and function from the keratinocytes
overall, describe the dermis
contains extracellular matrix proteins and diverse cell types:
- blood vessels
- glands
- nerve endings
- base of hair follicles
overall, describe the skin
- also called the integument
- largest organ
- has variable thickness
describe the composition of the skin
composed of 2 tissue layers:
- surface = cellular epidermis
- lower layer = mostly acellular dermis
what are 4 epidermal functions?
- protections from physical and chemical trauma and desiccation
- makes up 1/10 of skin thickness
- metabolic function = synthesis of vitamin D
- assists in antigen uptake via langerhans cells
describe the overall dermal functions
- sensation = support for nerve endings
- blood vessels = nutrient supply for epidermis and dermis and thermoregulation via dilation and constriction
what are the 3 main epidermal cell types?
- melanocytes = MCs
- langerhans cells = LCs
- keratinocytes = KCs
describe the presence of melanocytes
- make up 5% of epidermal cells
- have a clear cytoplasm
- there is 1 melanocyte for every 10-20 basal keratinocytes
what is the overall function of melanocytes?
produce melanin
describe melanin production, delivery. digestion and accumulation
- production stimulated by endocrine and paracrine signals at the melanocortin receptor
- delivered and phagocytyized by KCs
- partially digested by KC lysosomes
- accumulates over KC nucleus
- scatters and absorbs UV light
describe how variations in cell density exist across body surfaces
- regional concentrations of MCs = nevus or mole
- ABCDEs of moles = asymmetry, boarder, color, diameter, elevation
- changes in ABCDE may indicate malignancy
what cell type provides immune functions to the skin?
langerhans cells
describe the presence of langerhans cells
- makes up less than 5% of cells in epidermal layer
- have irregular shape
how are langerhans cells produced?
- bone marrow derived
- migrate from circulation across basement membrane into epidermis
describe how langerhans cells function as part of the immune system
- phagocytize and process low MW antigens
- exposure to antigen will trigger migration of LC to regional lymph nodes
- LCs breakdown antigens and present them to other immune cells in lymph nodes
- large SA of skin provides increased opportunity for antigen detection and initial processing
describe the presence of keratinocytes (KCs)
- most abundant epidermal cell type
- make up about 90-95% of cells in epidermis
describe how upper epidermal layers show body spite specification in response to pressure/friction
- mostly due to changes in thickness of cornified layer
- have a possible clear layer = stratum lucidum which is tightly packed squames seen in high frictional areas such as palms and soles
describe the 2 types of melanin and describe them
- eumelanin = brown/black
- phaeomelanin = red/yellow
- ratio between the 2 will determine pigmentation, eumelanin is more photo protective
describe the increase of melanin
- both eumelanin and phaeomelanin will increase in response to UV light
- triggered by MSG binding membrane melanocortin receptor
overall, how does the epidermal pigmentation occur?
occurs due to the combination of the following?
- MSH levels
- MSH receptor activity
- melanin production
describe vitiligo
- condition characterized by localized progressive loss of pigmentation
- occurs due to autoimmune destruction of melanocortins (MCs) and is often associated with other autoimmune disease
what are the 4 keratinocyte layers in the epidermis?
- basal layer = stratum germinativum
- spinous layer = stratum spinosum
- granular layer = stratum granulosum
- cornified layer = stratum corneum
describe the basal layer (stratum germinativum)
- mitotic in normal epidermis = only layer that is mitotically active
- migrates into wound to cover site
describe the spinous layer (stratum spinosum)
- cells are post mitotic
- contains many cell-cell attachments via desmosomes that are responsibly for spiny histology
- desmosomes lend to much of the epidermal structural strength
describe the granular layer (stratum granulosum)
- keratin proteins aggregate to make granules
- nuclei breakdown and lipids are extruded
- other specialized proteins are x linked = results in increased mechanical resistance
describe the cornified layer (stratum corneum)
- cells cease metabolism
- cells flatten into discs called squames which are eventually lost
- 3-4 weeks from basal to cornified layer
describe epidermal structure
resembles brick and mortar
- structure derived from keratinocytes
- 2 biochemical phases exist in granular and cornified layers
- hydrophilic brick = proteins in cells cross linked together
- hydrophobic mortar = lipids in extracellular space
describe the epidermal chemical barrier
- slows transit of water soluble and lipid soluble compounds
- advantages and disadvantages = lessens dehydration of underlying tissue and entry of toxins BUT it also restricts cutaneous drug delivery
describe the epidermal physical barrier
desmosomes between cells will provide structural integrity and strength
what does the pilosebaceous unit consist of?
- hair shaft
- hair follicle
- sebaceous gland
describe the epidermis above the hair follicle
thin but serves as a protective layer
describe the hair follicle
- lined with keratinocytes that are associated with sebocytes
- sebocytes make sebum (oil under skin)
describe the location of sebaceous glands
- located throughout the epidermis except the palms and soles
- face and scalp have the highest density and size variation
- empties into supper hair follicle
what stimulates sebum production?
androgens
describe secretion from sebaceous glands
via a halocrine process
- the entire cell breaks down to release contents into the ducts that empty into the hair follicle
describe the mitotic process of sebocytes
- sebocytes are constantly going through mitosis
- replicating cells at the gland perimeter replace the cells lost during secretion
what happens if there is an over production of sebum?
the opening closed and becomes an acne lesion
describe acne
involves sebocytes and keratinocytes
- hyper secretion and hyperprolifertaion will block ducts and/or hair follicle
what is an example drug used to treat acne?
Accutane = 13-cis retinoic acid
describe how Accutane works
- decreases KC proliferation to keep hair follicle opening clear
- decreases sebum production
describe the hair growth cycle
- ranges from a few months to years depending on the specific body site
- scalp has an extending growth cycle
overall, describe normal epidermal keratinocyte replication
- cells build physical strata and functional barrier
- physical requirement to maintain a lifetime replacement of upper layer via normal turnover and wound healing
overall, describe keratinocyte stem cells in the epidermis. what are the 2 types?
replicating cells that will help replace lost cells
- interfollicular stem cells
- follicular stem cells
describe interfollicular stem cells
between hair cells
- normal site or replication in basal layer only
- responsible for routine replacement of epidermis and minor wounds
describe follicular stem cells
appears as a thickening that surrounds hair follicle
- important for healing or secondary burns
- progeny contribute to epidermis and hair
- fibroblasts in dermal pailla instruct bulge daughter KCs to follow hair KC maturation
describe the fate of follicular stem cells on a normal day to day basis
- one daughter cell stays as a stem cell
- the other daughter cell accumulates in dermal papilla and is triggered to make a different population of keratins which will eventually build the physical hair shaft
describe the fate of follicular stem cells if there is a wound
- if there is a wound, the interfollicular stem cells are lost
- daughter cells of the stem cells will move and cover the wounded dermis to recover a wound site via daughter cells from the bulge area
- important for physical or thermal injuries
what is a benign epidermal KC replication disease? describe its incidence
psoriasis
- fairly common and may have a genetic component
describe the presentation of psoriasis
varying severity
- symmetric, well demarcated plaques often on elbows, knees, scalp and lower back = due to hyperprolifertaion of keratinocytes
- red, inflamed, itchy
- the degree of hyper proliferation will vary = over proliferation causes pillars of keratinocytes
describe the histology of psoriasis (6 points)
- hyperproliferation
- hyperkeratosis = increase immature SC layers
- parakeratosis = nuclei retained in SC incomplete maturation
- SG may be reduced
- poor barrier function
- immune cells infiltrate
what are 2 possible precursors to keratinocyte malignancy (cancer)? what is important to note about them?
- actinic keratosis (AK)
- keratoacanthoma (KA)
theses examples are benign themselves
describe actinic keratoses (AK)
- chronic sun exposure
- chiefly on face, ears, forearms
- individual or multiple sites, scaly, red (flat)
- 20% turn into malignancy over 10-25 yrs
describe keratocanthoma (KA)
- usually 1 large nodule often same areas as AK
- rapidly growing
- often times will spontaneously regress and fall off over time
- some will develop malignancy later on at the same site
what are 3 possible therapies for precursors to KC malignancy (AK and KA)?
- surgery
- dermabrasion = physical sanding away
- laser resurfacing
what is an example of a medication that can be used as therapy for precursors to KC malignancy (AK and KA)? how would these medications work?
tirbanilbulin (topical)
- cause cells cycle arrest by targeting microtubules to cause a deficit in mitosis in cell = stop or slow growth
describe the incidence of keratinocyte NON melanoma
- 3 million cases per year but they are unevenly distributed by types
- 80% BCC vs 20% SCC
- there is a 95% cure rate for both if they are detected and treated early
when do most keratinocyte non melanoma cases occur?
- in pts older than 60
- since cancer is a time dependent accumulation of multiple mutations
what are 3 shared risk factors for BCC and SCC
- sun, indoor tanning, fair skin
- chemical exposure
- immunosuppression or compromised immune system may not remove tumor cells that would otherwise be recognized as non self
describe the presentation of basal cell carcinoma (BCC)
- pearly nodule
- central depression
- rolled edge
describe the histology of basal cell carcinoma (BCC)
- looks like immature or basal cells of epidermis
- slow growing and rarely metastasize
describe the etiology of basal cell carcinoma (BCC)
- induces DNA mutations
- p53 tumor supressor gene is most common
- normal p53 arrests cell cycle and allows time for DNA to repair but if it is mutated it can no longer arrest the cell cycle
- leads to accumulations of mutations which leads to overgrowth of these cells which can then invade into the dermis
describe the treatment therapy for basal cell carcinoma (BCC)
- no single method is ideal
- surgical excision, radiation, retinoids to suppress cell replication
describe the presentation of squamous cell carcinoma (SCC); both early and late stages
- early stage = indurated hardened, erythematous plaque
- late stage = ulceration and crusting often indicates invasion of underlaying tissue
describe the histology of squamous cell carcinoma (SCC)
- cells look like squame KCs
- irregular masses of proliferating KCs extend into dermis
- keratin pearls exist in differentiated tumors
describe the etiology of squamous cell carcinoma (SCC)
similar to BCC = sun exposure
describe the treatment therapy of squamous cell carcinoma (SCC)
- surgery, usually followed by radiation or chemotherapy
- ex = retinoids used to suppress replication if surgical removal has not captured all cells
describe the presentation of malignant melanoma
- relatively variable
- size shape color
- atypical ABCDE = asymmetry, boarder, color, diameter, elevation
what is important to note about diameter for malignant melanoma?
notable if diameter is more than 4-6 mm
what is important to note about color for malignant melanoma?
- dark does not necessarily mean malignant
- color variation is a red flag
- some mutated cells will lose their ability to generate pigment
what are 3 risk factors for malignant melanoma?
- fair skin and congenital nevi = moles
- family history of melanoma
- history of chronic sun exposure
describe treatment therapy of malignant melanoma
- excision of lesion and nearby uninvolved skin and evaluation of lymph nodes for possible spread
- surgical removal often followed with interferon to induce apoptosis
describe the organization and 3 cell types found in there dermis
- ECM proteins
- cell types = fibroblasts, macrophages and mast cells, endothelial cells
- 2 histological compartments = papillary and reticular dermis
describe extracellular matrix (ECM) proteins in the dermis
mostly collagen, some laminin
describe fibroblasts in dermis
produce collagen and other ECM proteins
describe macrophages and mast cells in dermis
involved in peripheral immune function and some antigen processing
describe endothelial cells in the dermis
- walls of blood vessels
- sensory nerve endings
describe the papillary dermis
located right under the basal laminate
- undulating arrangement
- fine mesh of collagen fibrils
describe the undulating arrangement of papillary dermis
more contact area between epidermis and dermis per unit of surface provides stronger attachment
describe the fine mesh of collagen fibrils in the papillary dermis
- small vessels and capillary beds supply the dermis and epidermis
- sensory nerve endings
describe the reticular dermis
- dense collagen fibers
- contains nerves, base of hair follicles and sweat glands
describe the dense collagen fibers in the reticular dermis
- large blood vessels
- dilation and constriction will promote or restrict heat loss
describe 1st degree burns
mild sunburn
- damage within epidermis that is NOT blistering
- sunburn caused reddening but not blistering of the skin and damage is only to the upper layer s
- transient dermal erythema
- heals in 4-5 days with no scarring
describe 2nd degree burns
- blist fluid may separate epidermis from dermis
- painful = nerve endings viable
describe healing of 2nd degree burns
- heals in about 2 weeks
- regrowth via KCs within follicles, cells will migrate out to recover the area
describe 3rd degree burns (eschar)
burns below the hair follicle
- follicles and glands are destroyed, dermis may be lost
- injury depth kills nerves, so it is less painful than 2nd degree burn
describe the healing of 3rd degree burns less than 5 cm diameter
- heal from the edge
- can self heal can cover the wound via cells migrating in from the perimeter
describe the healing of 3rd degree burns more than 5 cm diameter
require grafting in order for skin to recover
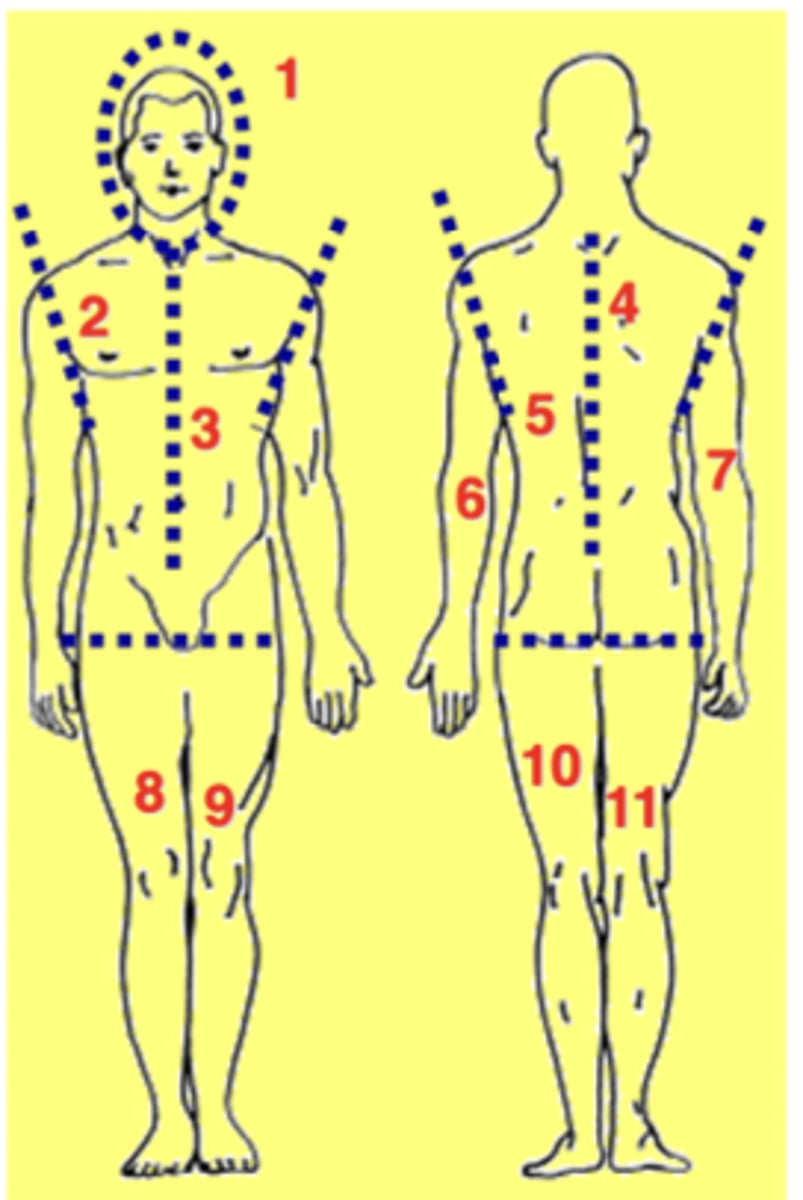
describe the rule of 9s for skin surface area
each of the following accounts for 9% of total skin SA:
- all of head and neck
- right anterior trunk
- left anterior trunk
- right posterior trunk
- left posterior trunk
- right arm
- left arm
- right anterior leg
- left anterior leg
- right posterior leg
- left posterior leg
- groin = 1% SA
when are burns considered critical?
- more than 25% of body has second degree burns
- more than 10% of body has third degree burns
- area affects the amount of of fluid loss and increases infection rate
what are the 4 phases of skin wound healing?
HIP-R
- hemostasis
- inflammation
- proliferation
- remodeling
what is a big takeaway to consider when observing the 4 phases of skin wound healing?
phases of healing will overlap each other to different extents and have presentation times that vary
describe the hemostasis phase of wound healing
- timeline = mins-hrs
- vasoconstriction occurs to cause platelet aggregation and blood clotting
- overlaps with inflammation so inflammation begins before hemostasis is completed
describe the inflammation phase of wound healing
- timeline = days-hrs /weeks
- early acute phase = vasodilation and capillary permeability chemotaxis of leukocytes
- late phase = macrophage infiltration
describe the proliferation phase of wound healing
- timeline = days-weeks
- proliferation of KCs, fibroblasts and endothelial cells
- synthesis and deposition matrix
- excess metric and fibroblasts lead to keloid (hypertrophic scar)