test test
1/260
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
261 Terms
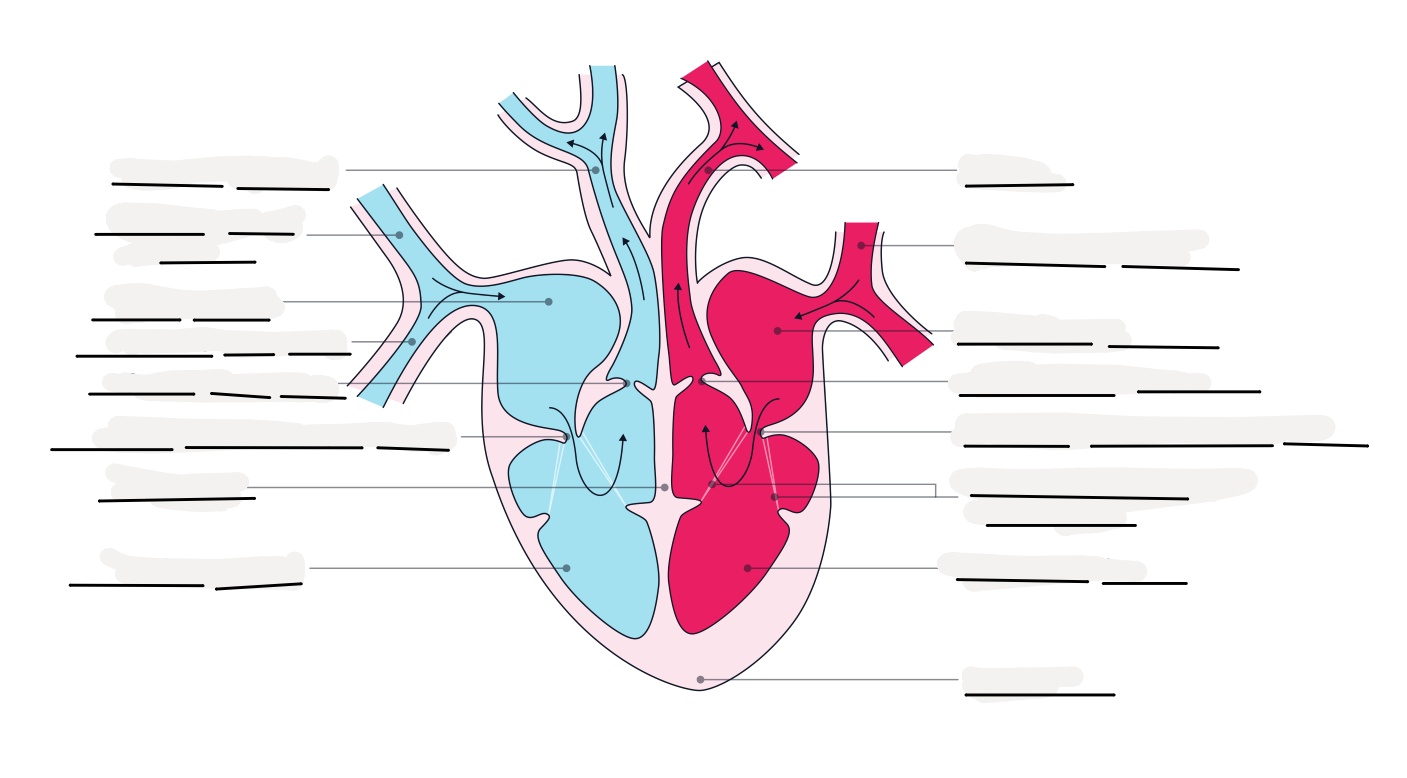
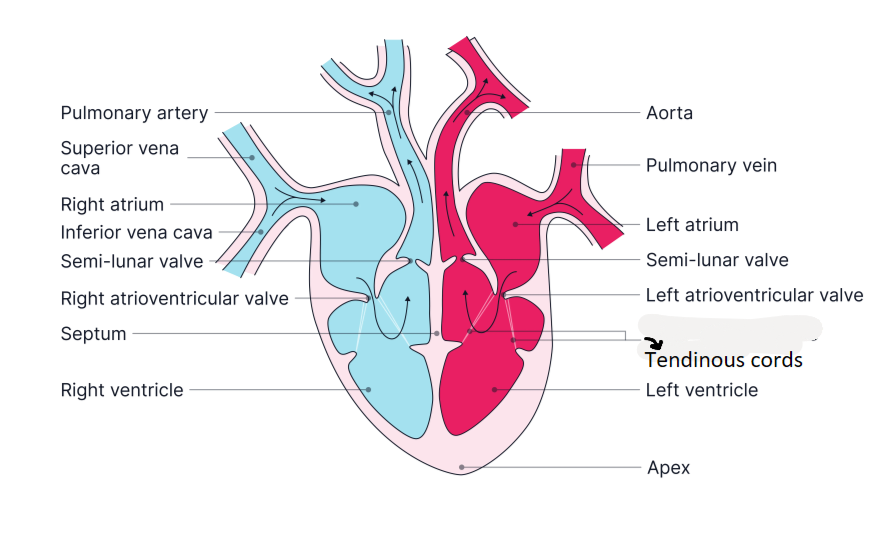
what is the heart made up of?
cardiac muscle
what is cardiac muscle?
a type of muscle that beats continually without tiring
what does the term myogenic mean in terms of the heart?
the capacity of the heart to generate its own electrical impulse, which causes the heart to contract
how many chambers is the heart made up of and what are they called?
2 atria (top 2 chambers), 2 ventricles (bottom 2 chambers)
how many sides does the heart have and what does each side do?
2 sides : Left hand side and Right hand side
RHS - contains deoxygenated blood which pumps to the lungs
LHS - contains oxygenated blood which pumps to the rest of the body
what are the 2 types of valves in the heart - and where are they in the heart?
atrioventricular - between the atria and the ventricles
semi-lunar - at the beginning of the aorta and pulmonary artery
what is the function of valves?
to prevent backflow of blood
do valves in the heart open one way or both ways?
only open one way
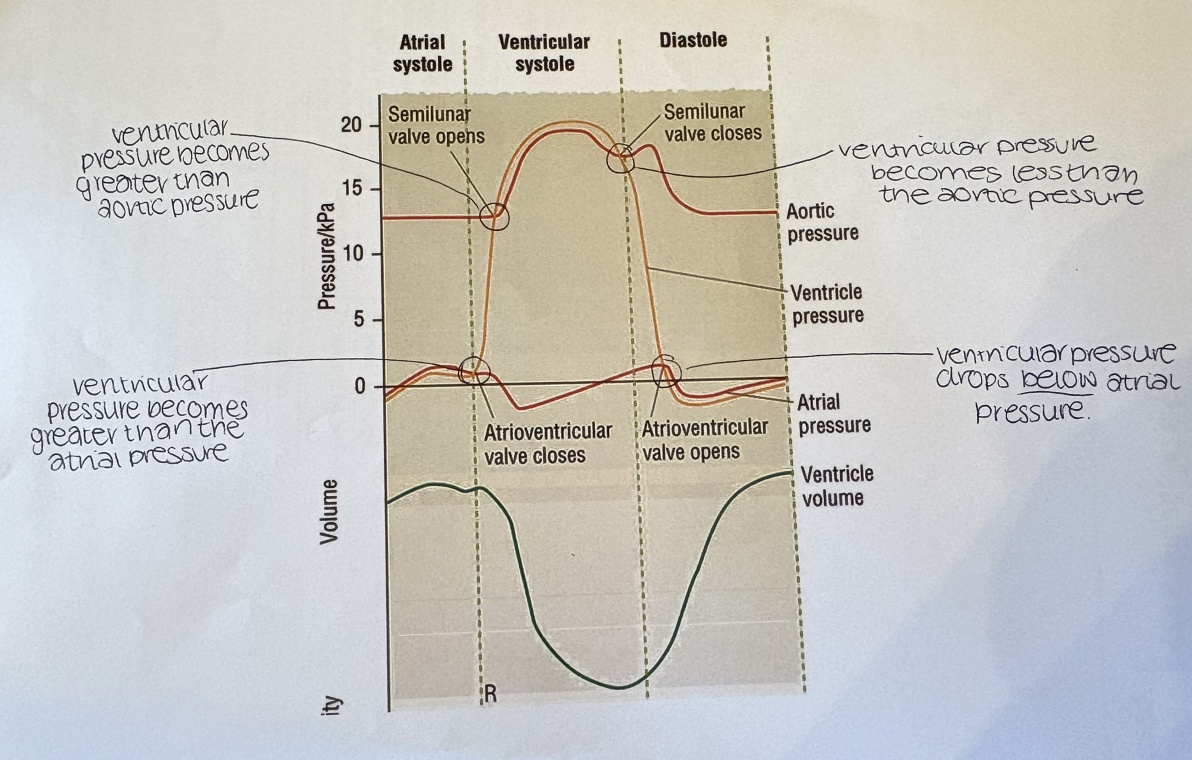
what determines if a valve in the heart is open or closed?
the relative pressure
if there is a higher pressure behind a valve it is forced open
if there is a higher pressure in front of the valve it is forced shut
what is the role of the tendinous cords in the heart?
to stop the valves inverting
what in the heart stops the valves inverting?
tendinous cords
where are coronary arteries situated?
over the hearts surface
what do the coronary arteries do for the heart?
they provide the heart with oxygen and glucose
what happens if one of the coronary arteries get blocked?
it may cause angina or a heart attack
what is the cardiac cycle?
the sequence of events that make up one heart beat
what are the 3 parts of the cardiac cycle?
atrial systole
ventricular systole
diastole
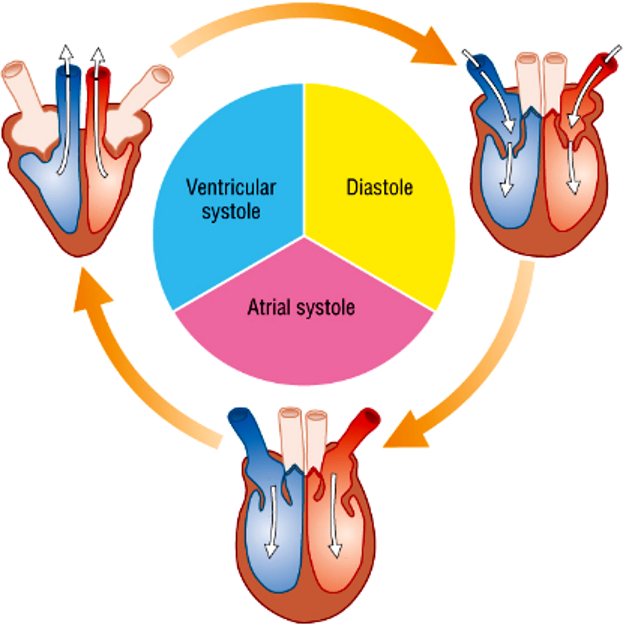
what happens during atrial systole?
The muscle in the atrial wall contracts (0.1s)
The atrial muscle wall is relatively thin and so the pressure generated is relatively small, as blood is only being pumped into the ventricles
The pressure in the atria is higher than in the ventricles, so this pushes open the atrioventricular valves
what happens during ventricular systole?
The ventricular muscle contract (0.3s)
The left ventricle muscle is thicker than the right and so creates more pressure and pumps the blood with greater force
Blood is pumped through the semi-lunar valves, which open
As soon as the pressure in the ventricles becomes greater than that in the atria, the difference in pressure forces the atrioventricular valves shut - the valves are held shut (do not flap open) because of tendinous cords holding them
what happens during diastole?
The heart muscle relaxes (0.2s)
The pressure in the ventricles drop
Blood in the arteries does not flow back because the semi-lunar valves shut
Blood from the veins flows into the 2 atria - some can flow through the atrioventricular valves into the ventricles as the atrioventricular valves are very slightly open
The blood is at very low pressure
fill in the gaps
which ventricle in the heart has a thicker wall and why?
the left as it has to pump blood further (around the body rather than to just the lungs)
left has a muscular wall that is around 5x thicker than the right
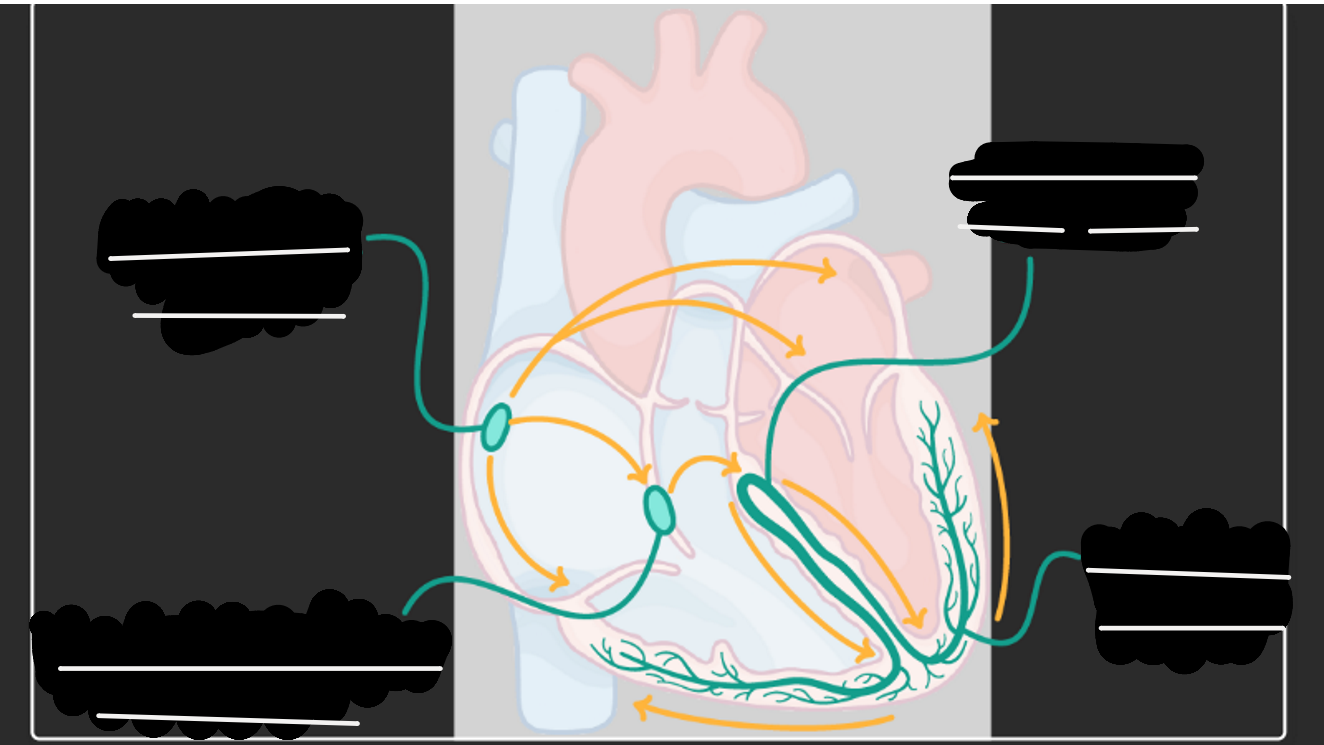
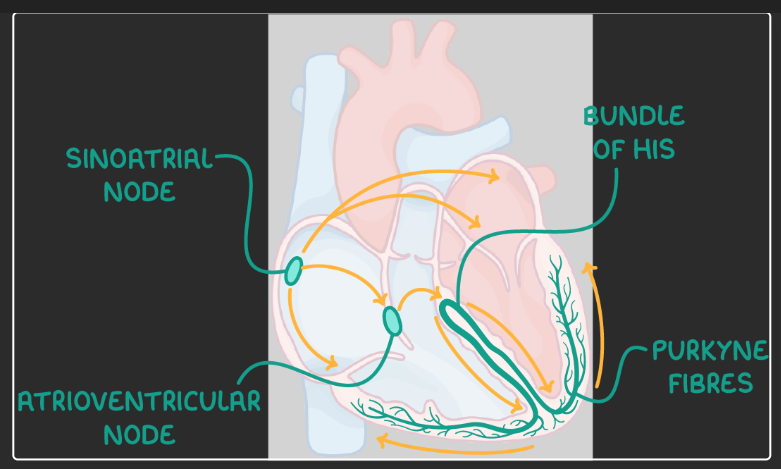
what is the order of the conduction system (nodes and systole/diastole)?
There is a brief break where no impulse is generated allowing blood to enter the atria.
The sino-atrial (SA) node initiates the impulse which is transported through both atria where it is received by the atrio-ventricular (AV) node.
This causes atrial systole.
Blood is ejected out of both atria and into the ventricles.
The AV node delays the impulse briefly then releases it onwards to the bundle of his.
The bundle of his splits the impulse down the left and right bundle branches where they reach the Purkyne fibres.
Once the impulses reaches these fibres both ventricles will contract causing the blood to be ejected into the circulatory systems.
It then repeats.
fill in the gaps
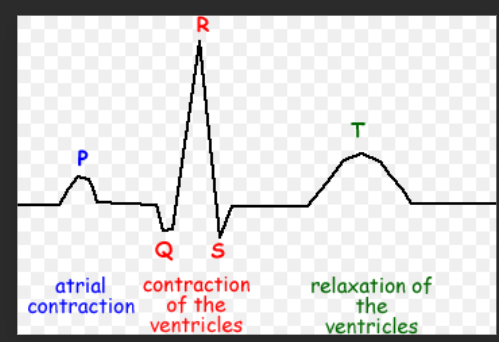
on a graph to show the cardiac cycle what do the letters P, Q, R, S and T show?
P = atrial systole - SA node generates a wave of excitation which passes across the atrial walls leading to atrial systole
Q, R and S = Ventricular systole - wave of excitation passes down the bundle of his and up the Purkyne fibres in the walls leading to ventricular systole
T= diastole - both atria and ventricles contract leading to diastole
Then there is a refractory period after contraction which means that the heart is unable to contract for a brief time
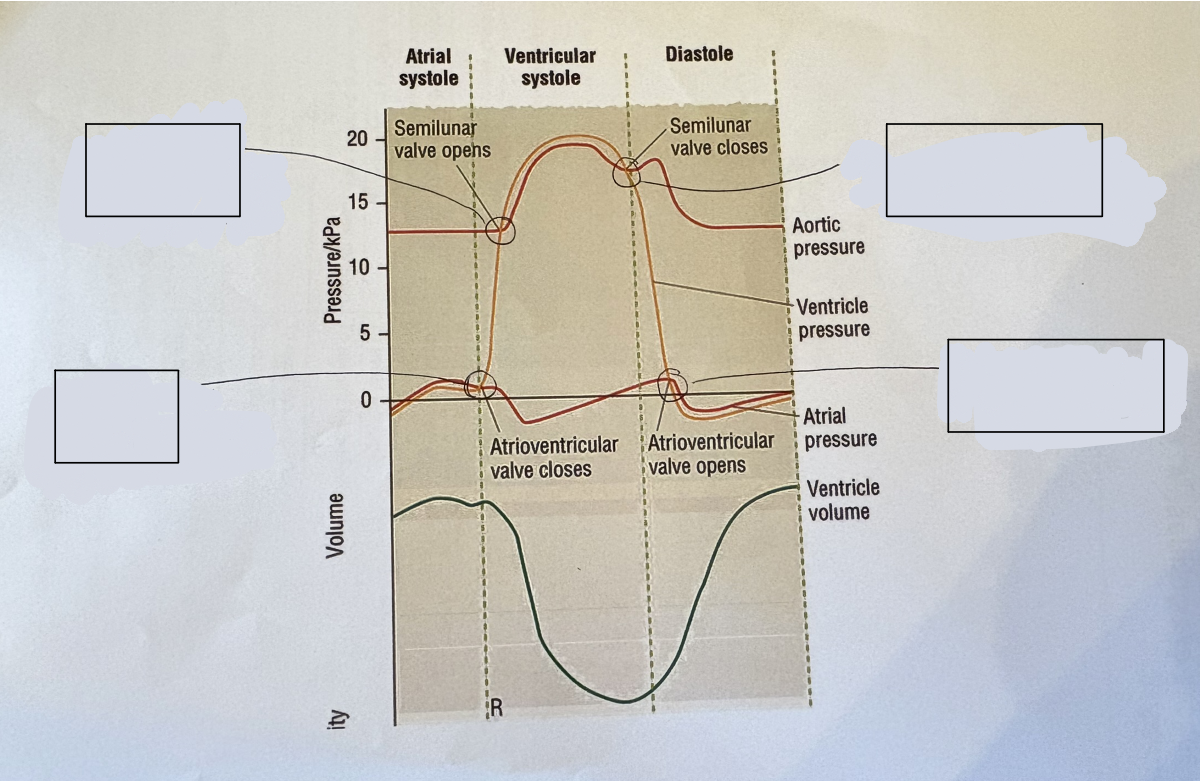
what should go in the gaps to describe the graph?
how many molecules of haemoglobin does each erythrocyte contain?
about 280 million molecules of haemoglobin
what is haemoglobin?
soluble globular protein
made of 4 polypeptides
each polypeptide contains a haem group
each haem group binds to one oxygen, so one haemoglobin molecule can bind to 4 oxygen molecules
each haem group contains an iron ion at the centre
what is the haem groups role in blood?
responsible for the red colour
site of oxygen transport
has an affinity for oxygen (each haem group can hold one oxygen molecule (O2)
what is cooperative binding?
When one oxygen molecule binds to haemoglobin (Hb), it changes the tertiary structure (shape) of the Hb
This conformational change makes it easier for additional oxygen molecules to bind (increasing affinity)
Therefore, each oxygen binds more readily than the last → this is cooperative binding
As soon as oxygen diffuses into an erythrocyte, it is rapidly bound to Hb
This helps maintain a steep diffusion gradient for oxygen from alveoli to blood until Hb becomes saturated
what is the formula of oxyhaemoglobin that is fully associated?
HbO8
What determines whether haemoglobin takes up or releases oxygen?
Haemoglobin takes up or releases oxygen depending on volume (or partial pressure) of oxygen present
what is partial pressure of oxygen measured in?
KPa
When does haemoglobin bind more readily to oxygen and when does it release it?
haemoglobin binds more readily to oxygen in high partial pressure of oxygen (in the lungs)
releases oxygen more readily in low partial pressure of oxygen (in respiring tissues)
What is the maximum amount of oxygen a haemoglobin sample can combine with defined as?
The maximum amount of oxygen with which haemoglobin sample can combine is given a value of 100%
How does haemoglobin’s affinity for oxygen vary with partial pressure of oxygen?
Haemoglobin has a high affinity for oxygen where the partial pressure of oxygen is high (the lungs)
but a low affinity for oxygen where the partial pressure of oxygen is low (respiring tissues e.g. muscles)
What effect does a small change in ppO₂ have on haemoglobin saturation
A small change in the ppO2 makes a significant difference to the saturation of Hb with O2
What does ppO₂ stand for?
ppO2 is shorthand for partial pressure of oxygen
what is the Bohr shift?
The Bohr shift is the rightward shift of the oxygen dissociation curve caused by increased CO₂ (and lower pH), which reduces haemoglobin’s affinity for oxygen so it releases more oxygen to respiring tissues.
what does the oxygen dissociation curve show?
Relationship between % Hb saturation and pO2
what is cooperative binding?
Binding of one O2 increases Hb affinity for more O2
How does fetal Hb differ from adult Hb?
fetal haemoglobin has a higher affinity for oxygen than fetal haemoglobin
why is it good that fetal haemoglobin has a higher affinity for oxygen than adult haemoglobin?
It means that at low ppO2 oxygen dissociates from the adult haemoglobin and diffuses across the placenta and binds to the fetal haemoglobin because fetal haemoglobin has a higher affinity for oxygen than adult haemoglobin
is there high or low ppO2 at the placenta and why?
there is low ppO2
because the placenta is a respiring tissue
allows for oxygen to be dissociated from adult haemoglobin and bonded to fetal Hb
On the oxygen dissociation curve is the fetal Hb curve to the left or the right of the original one?
left
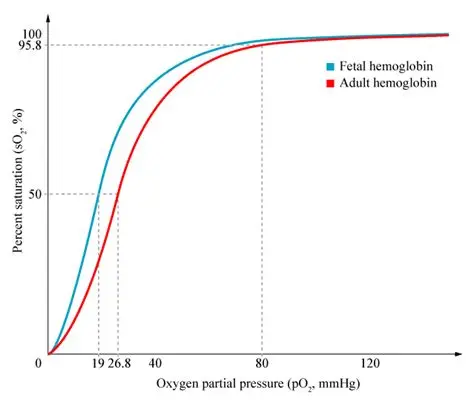
at what ppO2 will fetal Hb bind to oxygen?
at the same ppO2 that adult Hb releases O2
what happens to the fetal Hb once the baby is born?
new erythrocytes will contain adult Hb
erythrocytes live for approx. 120 days
after 6 months, all erythrocytes will contain adult Hb
what causes cooperative binding?
conformational change in haemoglobin
what shape is the oxygen dissociation curve?
S shaped
where in the body has a high ppO2 and where has a low ppO2 and hat does this cause?
High ppO2 at the lungs - causes Hb to have a high affinity, Hb becomes saturated
Low ppO2 at respiring tissues - causes Hb to have a low affinity, Hb releases oxygen
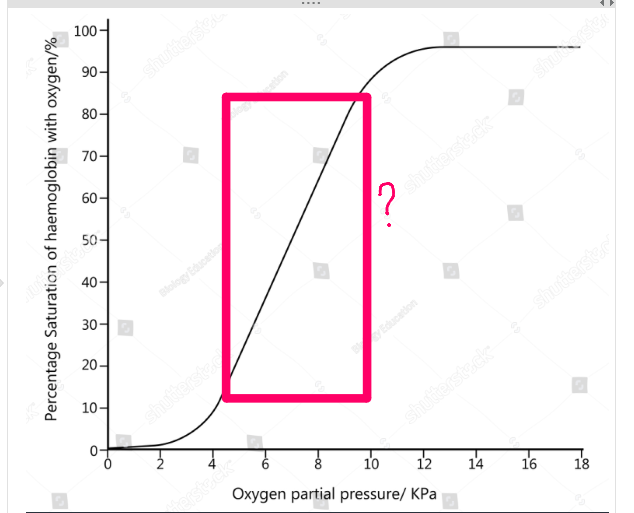
what does the steep middle section of the oxygen dissociation graph show?
small increase in ppO2 causes a large increase in Hb saturation
explain what happens as oxygen binds to one Hb molecule
first O2 molecule takes a while to bind
when the O2 does bind, it changes the shape of the Hb molecule
once the shape has changed the next 2 or 3 O2 molecules bind much more quickly
the final O2 molecule sometimes takes a while to bind to the Hb
once the final O2 molecule has bonded to the Hb, the Hb is fully saturated
this is cooperative binding
what happens to the oxygen dissociation curve during exercise?
the curve shifts to the right because:
when muscles are respiring faster (when you are exercising), more CO2 is produced
this lowers the affinity of Hb for O2 at the exercising muscles, meaning that the Hb releases more O2, which is then used by the muscles for faster aerobic respiration
this is the Bohr shift
what is the effect of CO2 on the the oxygen dissociation curve?
as partial pressure of CO2 rises (amount of CO2 increases), Hb gives up oxygen more easily
this is known as the Bohr effect/shift
the curve shifts to the right
in what scenario may the oxygen dissociation curve undergo the Bohr shift?
in active tissues with a high partial pressure of CO2 (during exercise)
what are the 3 ways that carbon dioxide is transported from the tissues to the lungs? (incl. % of each)
5% dissolves in the plasma
15% combines with Hb to form carbaminohaemoglobin
80% is converted to HCO3– ions in erythrocyte cytoplasm
Describe how carbon dioxide is transported from respiring tissues in the blood, including the role of erythrocytes and haemoglobin
At respiring tissues, CO₂ diffuses into erythrocytes
CO₂ + H₂O → H₂CO₃ (carbonic acid) in cytoplasm, catalysed by carbonic anhydrase
H₂CO₃ dissociates into H⁺ and HCO₃⁻ ions
HCO₃⁻ diffuses out into plasma; Cl⁻ diffuses into RBC to maintain electrical balance (chloride shift)
Hb binds H⁺ to form HHb (haemoglobonic acid), acting as a buffer and preventing pH changes
Binding of H⁺ causes Hb to release O₂, which diffuses to respiring tissues
Continuous removal of CO₂ (as HCO₃⁻) maintains a steep diffusion gradient into RBCs
Explain how carbon dioxide is released from the blood in the lungs, including the role of haemoglobin and carbonic anhydrase
This produces CO2 which diffuses out of rbc into the alveoli
At respiring tissues, CO2 diffuses into erythrocyte
CO2 reacts with H2O in erythrocyte cytoplasm to from H2CO3 (carbonic acid) - the enzyme carbonic anhydrase speeds up this reaction
H2CO3 dissociates into H+ ions and HCO3- ions
These HCO3- ions diffuse out the rbc into the plasma
to maintain electrical balance chloride ions (Cl-) diffuse into the rbc - known as chloride shift
Hb in rbc bonds with the free H+ ions to form Haemoglobonic acid (HHb) to act as a buffer (stop pH in blood changing)
to accept the H+ ions, the haemoglobin has to release its oxygen - this oxygen diffuses out the rbc and to the respiring tissues
removing CO2 and converting it to HCO3- ions maintains the steep conc
what is this HCO3−
hydrogen carbonate ions
what is one reason it is good that the heart is myogenic?
it prevents the body wasting resources on maintaining the basic heart rate
what do Electrocardiograms (ECGs) do?
they can measure electrical excitation through the heart as a way of recording what happens as it contracts
this recording of the electrical activity of the heart is called an electrocardiogram (ECG)
how is an electrocardiogram done?
electrodes are stuck painlessly to clean skin to get good contacts needed for reliable results
signal from each of the electrodes is fed to the machine which produces an ECG
Does an ECG measure the direct activity of your heart?
No they measure tiny electrical differences un your skin which can result from the electrical activity of the heart
what are ECGs used for?
they are used to help diagnose heart problems
if someone is having a heart attack, recognisable changes take place in the electrical activity of their heart which can be used to diagnose the problem and treat it correctly and fast
What letters are used to represent the different stages shown on an ECG?
P, Q, R, S and T
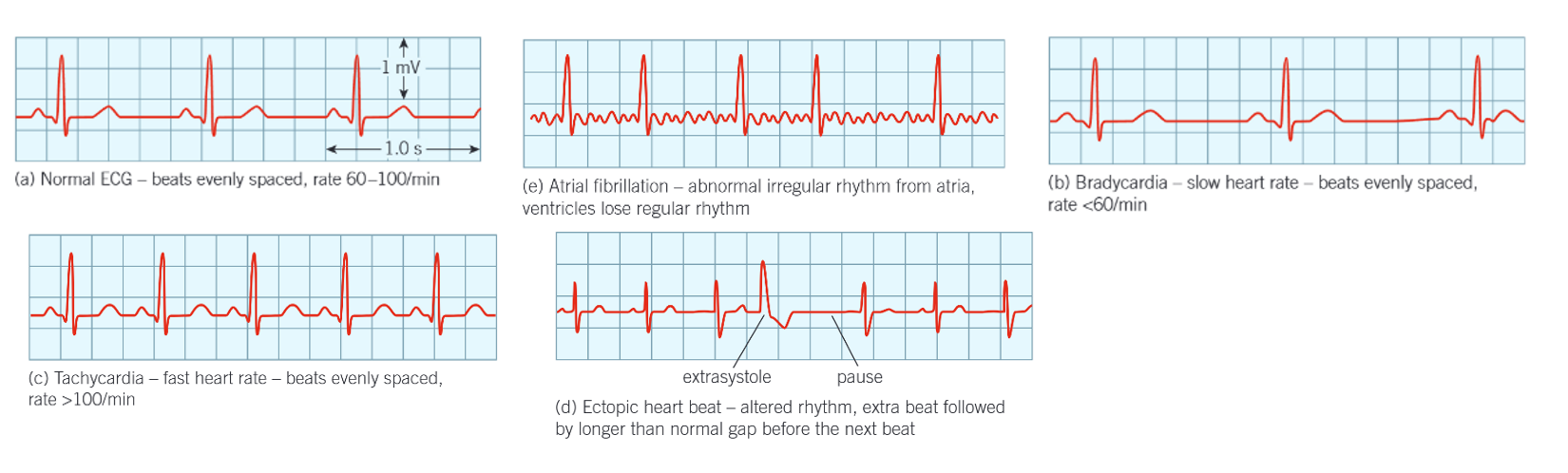
what is tachycardia?
when a heart beat is very rapid - over 100 bpm
when is tachycardia normal?
it is often normal when:
you exercise
have a fever
if you are frightened or angry
if tachycardia is abnormal what may it be caused from?
problems in the electrical control of the heart
may need to be treated by medication or surgery
what is bradycardia?
when heart rate slows down to below 60 bpm
why do lots of people have bradycardia?
because they are fit
training makes the heart muscle grow so it can beat slowly but more effectively
what may people with bradycardia need?
severe bradycardia can be serious
may need an artificial pacemaker to keep the heart beating steadily
what is an ectopic heartbeat?
extra heartbeats that are out of the normal rhythm
are ectopic heartbeats normal?
most people have at least one ectopic heartbeat a day
they are usually normal but can be linked to serious conditions when they are very frequent
what is atrial fibrillation?
an example of arrhythmia, which means abnormal rhythm of the heart
Rapid electrical impulses are generated in the atria
Small, unclear P wave or T wave
They contract very fast (fibrillate) up to 400 times a minute
However, they don’t contract properly and only some of the impulses are passed on to the ventricles, which contract much less often
As a result the heart does not pump blood very effectively
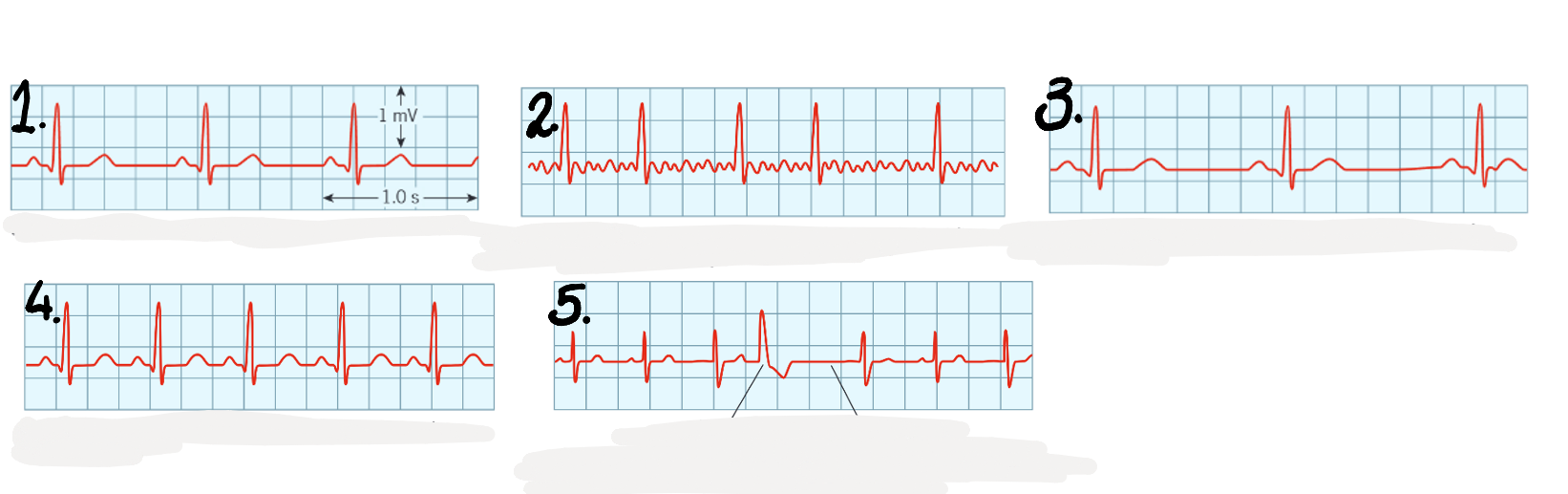
which ECG is which different type of heart beat? how do you know?
normal ECG
atrial fibrillation
bradycardia
tachycardia
ectopic heartbeat
what affects blood pressure in the arteries?
varies as the ventricles contract
effected by the diameter of the blood vessels
how is blood pressure measured (traditionally)?
A manual sphygmomanometer (cuff + mercury manometer) is placed around the upper arm
Cuff is inflated to occlude the artery, stopping blood flow to the lower arm
Stethoscope placed over the brachial artery at the elbow, cuff pressure slowly released
Pressure at which first tapping sounds (Korotkoff sounds) are heard = blood just forced through during ventricular contraction → systolic pressure
Measured as height of mercury column (mmHg) at this point
As pressure continues to fall, sounds become normal/disappear when blood flows freely even during ventricular relaxation → diastolic pressure
Normal reading ≈ 120/80 mmHg
what is the more recent way of measuring blood pressure?
digital sphygmomanometer is often used - same principles apply, stethoscope is simply built into the cuff applied around the arm
what is the main transport medium of the human circulatory system?
blood
what is tissue fluid important for?
the exchange of substances between the blood and the cells
what is lymph?
a third liquid which is also part of the complex system that makes up the circulation of the body
what is blood made up of?
plasma
erythrocytes (rbc)
leucocytes (wbc)
platelets
what % is each component of the blood?
55% plasma
44% erythrocytes
1% wbc and platelets
what are platelets?
fragments of large megakaryocytes found in the red bone marrow
they are involved in blood clotting
what is the yellow liquid in blood?
plasma
what does plasma carry?
dissolved glucose and amino acids
mineral ions
hormones
the large plasma proteins including albumin (important for maintaining the osmotic potential of the blood), fibrinogen (important in blood clotting) and globulins (involved in transport and immune system)
platelets
rbc (which carry oxygen and give the blood the red appearance)
many different types of wbc
one of the functions of blood is transport, this includes transport of…
Oxygen to, and carbon dioxide from, the respiring cells
Digested food from the small intestine
Nitrogenous waste products from the cells to the excretory organs
Chemical messages (hormones)
Food molecules from storage compounds to the cells that need them
Platelets to damaged areas
Cells and antibodies involved in the immune response
how does blood help with the maintenance of the body?
keeps a steady body temp
acts as a buffer, minimising pH changes
how is oxygen, glucose and carbon dioxide exchanged between the blood and respiring tissues?
by the tissue fluid
in the capillary beds where blood pressure is low and blood flows slowly
what is hydrostatic pressure?
The pressure exerted by the blood against the capillary walls
where is hydrostatic pressure high and low and what causes hydrostatic pressure?
caused by the heart pumping blood
High at arteriole end
Decreases along the capillary
during the formation of tissue fluid at the arteriole end of the capillary is there a higher hydrostatic pressure or oncotic pressure and what does this cause?
higher hydrostatic pressure
forces tissue fluid to move out of the capillaries through the gaps in the endothelial cells
this process is called ultrafiltration
when tissue fluid leaves the capillary what doesn’t leave with it and why?
Blood cells and plasma proteins are too large to leave so they remain in the blood plasma
why is there a higher hydrostatic pressure at the arteriole end of the capillary?
Blood enters the capillary directly from an arteriole
It has just come from the heart under high pressure
no fluid has been lost yet to the capillary
why is there a low hydrostatic pressure at the venule end of the capillary?
a large amount of fluid has left the blood, reducing volume and so reducing pressure
why is the oncotic pressure still high at the venule end of the capillary?
there are still plasma proteins in the blood plasma
at the venule end of the capillary is there more oncotic pressure or hydrostatic pressure and why? and what does it cause?
more oncotic pressure than hydrostatic pressure
hydrostatic pressure has decreased as fluid has left the blood plasma
oncotic pressure has remained as there are still plasma proteins in the blood plasma
causes water to move back into the blood by osmosis
how much of the tissue fluid reabsorbed back into the blood? and what happens to the rest?
around 90%
the other 10% joins the lymphatic system
what is a step by step of how tissue fluid is formed?
blood enters the capillaries from the arterioles
the blood is at high hydrostatic pressure(5.4KPa) because it has been pumped directly from the heart and no fluid has been lost yet
there is oncotic pressure (3.3KPa) due to the plasma proteins in the blood plasma though this is lower than the hydrostatic pressure
This forces fluid to move out the capillaries through the gaps in the endothelial cells - this process is called ultrafiltration
the fluid that leaves forms tissue fluid containing water, oxygen, glucose and ions
plasma proteins and blood cells remain in the blood plasma as they are too big to leave
at the venule end of the capillaries, hydrostatic pressure has decreased (to 2.1KPa) as lots of fluid has left the blood
oncotic pressure remains high (3.3KPa) as the plasma proteins could not leave the capillary
this means that oncotic pressure is now larger than hydrostatic pressure so water moves into the capillary by osmosis down a water potential gradient
not all tissue fluid returns - 10% drains into the lymphatic system
what is tissue fluid?
Fluid similar to blood that does not contain plasma proteins or blood cells (therefore similar to plasma without the plasma proteins)
what does the tissue fluid do when it has been forced out of the capillaries?
tissue fluid contains dissolved nutrients (e.g. glucose) and oxygen
the tissue fluid bathes the cells
exchange of has and nutrients occurs across the cell surface membranes