Life Support: Lecture 3:
1/83
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
84 Terms
Coronary Heart Disease
Chronic condition of plaque buildup (atherosclerosis) in the heart arteries
There is also acute coronary heart disease which is sudden acute events (like heart attack) caused by plaque rupturing or blocking blood flow
Atherosclerosis:
Cholesterol building up in the arteries forming plaque
This causes the arteries to narrow and have reduced blood flow
Risk Factors for Coronary Heart Disease
Family History and Unhealthy Lifestyle (Bad diet and exercise which lead to high cholesterol)
Stable Angina:
Early Stage of CHD and it is caused by partially narrowed arteries
In exercise narrow arteries don’t get enough blood to the heart muscle which leads to ischemia and is represented as chest pain
Ischemia
a critical condition where restricted blood flow to a tissue or organ causes a severe shortage of oxygen and nutrients (in this case heart muscle)
Unstable Angina
More severe than stable angina, now chest pain also occurs at rest due to narrower arteries and indicates that a heart attack may occur
Acute Myocardial Infarction:
Heart attack in which the coronary artery is blocked. If it becomes blocked no blood is ale to flow to the heart muscle (myocardium) (blood clot or plaque buildup)
How to Diagnose?
Chest Pain and Radiation of Pain to Left Arm and Jaw, Sweating, Nausea and Vomiting
Risk Factors of CHD:
Smoking, High BP (hypertension), High Cholesterol (hypercholesterolemia), diabetes, obesity, family history, CVD and pervious stable angina
Why do these factors cause for a risk of CHD?
These factors damage blood vessels which promotes atherosclerosis, or pre-existing coronary artery narrowing
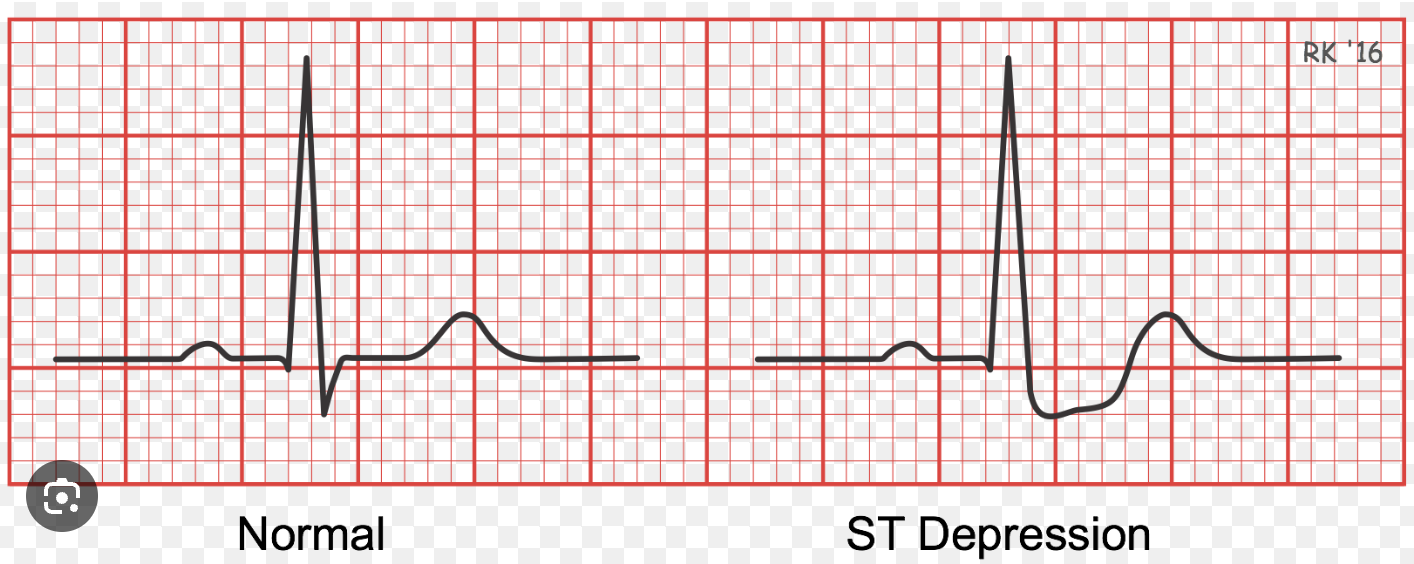
Electrocardiogram:
Measures electrical activity of the heart using P, QRS and T waves. Electrodes (leads) are placed on the patient and reflects how electrical impulses travel through the heart
Troponin Test:
Assesses if there is troponin in the bloodstream. This is helpful as troponin is only released when the heart is damaged, and therefore this blood test can show if someone is having a silent heart attack (ECG would not detect this)
Ischemia and Infarction on ECG
Ischemia: Shows T wave inversion and ST depression
Treatment of CHD:
Stent Placement: Adding a stent into the artery to open a narrowed or blocked artery (minimally invasive)
Coronary Artery Bypass Grafting: Surgical procedure in which an artery of the legs or chest is used to create a new pathway for blood to reach the heart muscle
Better Lifestyle and Medication
Aortic Dissection:
The aorta has a tear in one of its three layers (intima) and blood enters the vessel wall which creates a false lumen (extra channel that shouldn’t exist)
This weakens the vessel and creates the risk of a rupture, this is dangerous as the aorta is a high pressure vessel and a rupture would cause massive internal bleeding reducing blood flow to organs
Type A Aortic Dissection:
Tear in the ascending aorta
Type I: ascending and descending aorta
Type II: only ascending aorta
Type A Aortic Dissection Treatment:
Immediate surgery is required, the part that is ruptured must be removed and replaces with a bypass tube
Type B Aortic Dissection:
Tear in the descending aorta
A tear leads to impaired blood flow to the kidney, intestines and lower body
Treatment for Type B Aortic Dissection:
First blood pressure control and rest
Surgery only if complications occur
How to Diagnose Aortic Dissection?
Acute severe pain in shoulder blades, chest or abdomen, Typical patient: man aged 60-70 years old
Can cause shock
Can be seen on a CT scan or echo
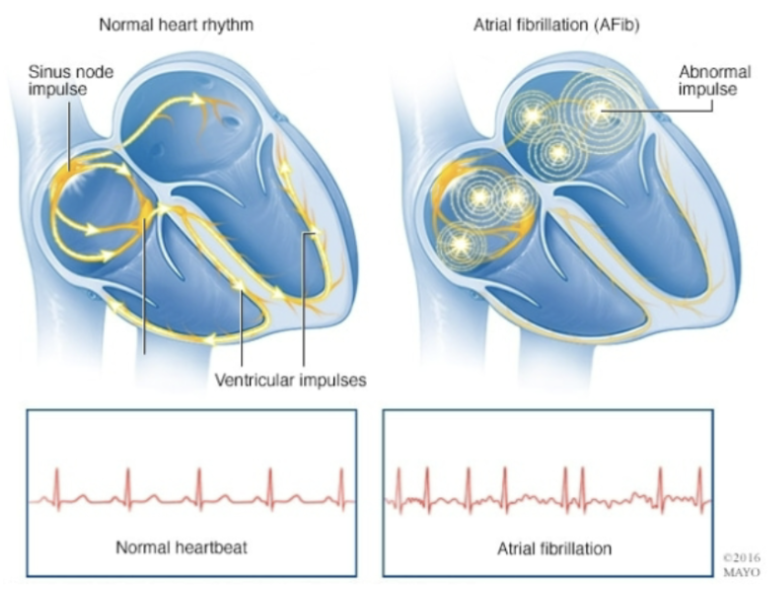
Atrial Fibrillation:
Multiple foci in the artia rapidly fire, therefore there is no sign pacemaker (SA Node) and atria does not contract properly it only fibrillates
The Effect of Atrial Fibrillation on Ventricles
The ventricles receive irregular signals as well and therefore leads to an irregular rhythm
The ventricles do not fill properly with blood due to the irregular and fast rhythm and no effective atrial contractions occur
↓ Ventricular filling, ↓ Cardiac output, ↓ Blood flow to brain
How is Atrial Fibrillation represented on a ECG?
No regular P waves, and irregular signals lead to irregular rhythm on the ECG (tachycardia)
Symptoms of Atrial Fibrillation:
Dizziness, Collapsing, Tachycardia (leads to cardiac fatigue and heart failure → tachcardia-induced cardiomyopathy) and Palpitations
High BP (hypertension)
Treatment for Atrial Fibrillations:
Anticoagulants: In AF blood clots start to form due to blood pooling from irregular heartbeats and it also increases the risk of a stroke, Anticoagulants are used to prevent blood clots from forming and a stroke occurring
Medication: Rate/Rhythm control to lower the heart rate allowing for ventricular filling
Cardioversion: Electrical and Chemical
Electrical: two pads placed on chest and a shock is delivered to reset the heart to SA Node
Chemical: Use of antiarrhythmic drugs to convert rhythm back to sinus rhythm
Ablation: Insert a catheter into the heart and burn the spots that are signalling incorrectly so it goes back to sinus rhythm
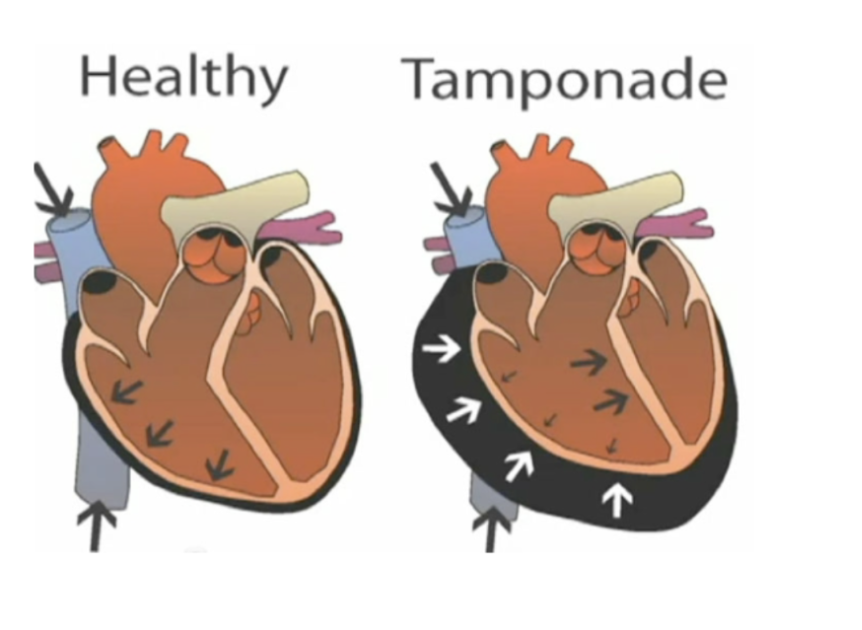
Cardiac Tamponade
Drastic drop in BP due to blood, fluid or pus filling up the pericardial sac surrounding the heart preventing it from filling properly
Science behind Cardiac Temponade:
After there is trauma to the heart, the pericardial sac fills up leading to the narrowing of the ventricles (and heart chambers)
This means that the heart cannot fill up properly in diastole leading to the blood being backed up into the veins (shown as bulging neck veins) (↓ Filling → ↓ stroke volume → ↓ cardiac output)
Since there is less blood pumped it leads to hypotension
Symptoms of Cardiac Temponade:
hypotension which causes tachycardia, leads to shock, respiratory distress
Occurs due to trauma in heart (stabing)
Muffles Heart Sounds in Stethoscope, Hypotension, Bulging Neck Veins
How to measure Cardiac Temponade:
Cardiac Ultrasound, X-ray on chest, ECG and CT-scan
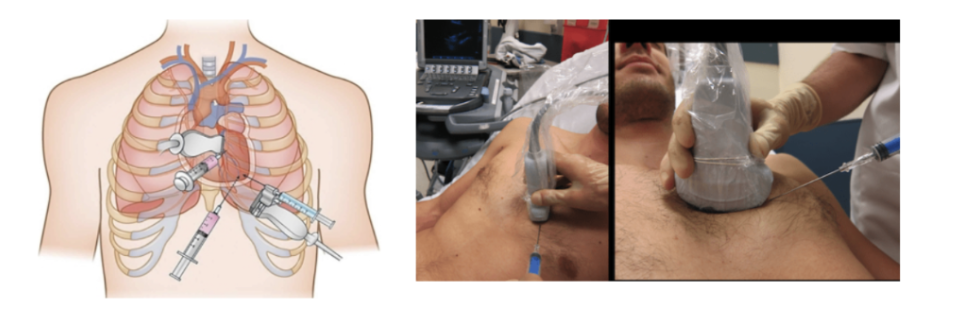
Treatment of Cardiac Temponade:
Pericardiocentesis: An ultrasound-guided needle insertion used to remove fluid/blood from the pericardial sac to relieve pressure
Resuscitative Thoracotomy: Opening the chest wall to gain access to the heart to control bleeding and relieve temponade
Heart Failure (Decompensatio Cordis)
Failure of the pump function of the heart leading to pulmonary edema
Pulmonary Edema:
condition characterized by excess fluid buildup in the lung's air sacs (alveoli), causing severe breathing difficulty and potential respiratory failure
Astma Cardiale:
severe breathing difficulty and potential respiratory failure
Causes of Heart Failure:
heart attack, hypertension, valve abnormalities, medication (chemotherapy), anemia and infection of the heart
Anemia:
occurs when your body lacks enough healthy red blood cells or hemoglobin to carry adequate oxygen to its tissues
Symptoms of Heart Failure:
Weight gain due to fluid retention and shortness of breath (usually at night when you lie down) due to the fluids, and fatigue, high BP (hypertension) and high respiratory rate (tachypnea)
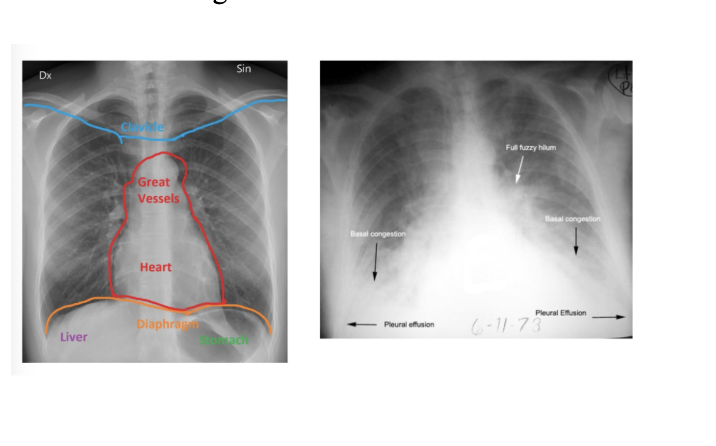
How can you test for Heart Failure:
Blood test, and X-ray of the chest
Normal lungs: dark (air-filled)
Edema: white (fluid-filled)
Treatment for Heart Failure:
Oxygen Therapy: High pressure in the hope that fluid is removed from lungs back into circulation, then eliminated via kidneys
Continuous Positive Airway Pressure (CPAP): Applies positive pressure, helps to keep alveoli open and push fluid out of alveoli back into circulation
Medication: Nitroglycerin and Diuretics:
Nitroglycerin: Opens blood vessels which reduces BP and fluid leakage (leads to vasodilation)
Diuretics: Removes excess fluids from the body, so blood volume decreases and therefore pressure which reduces pulmonary edema
..
..
Shock:
a reduction in systemic perfusion causing inadequate tissue oxygen delivery to meet demand, resulting in anaerobic metabolism and the formation of lactic acid
Tissue Hypoxia:
tissues receive inadequate oxygen, preventing proper cellular respiration and ATP production
In shock this lactate accumulation is pathological due to tissue hypoxia
Reversible vs Irreversible Lactate Production
In the beginning phase it is reversible, but can rapidly turn irreversible and turn into organ damage/dysfunction, cell death and death
During physical exercise you also produce lactate but this is physiological and can therefore be reversed (not pathological)
What is oxygen delivery dependant on
Cardiac Output x Hemoglobin x Oxygen Saturation
Cardiac Output: Stroke Volume x Heart Rate
Hemoglobin: Found in red blood cells and carries/delivers oxygen
Oxygen Saturation: Percentage of hemoglobin that is bound to oxygen
Pneumonia:
When the alveoli fills up with pus and fluid so it impairs gas exchange, therefore there is a low oxygen saturation
CO is high, but Hb is normal and SaO2 is low
What are the different types of Shock?
Hypovolemic (Hemorrhagic and Non-Hemorrhagic)
Obstructive
Distributive
Cardiogenic
Symptoms of All Shock
Tachycardia: ↓ cardiac output or ↓ volume so the body compensates with increasing heart rate
Hypotension: due to loss of blood or sepsis (response due to infection)
Pale, White and Clammy skin
Confusion: Not enough oxygen to the brain
Lactic acidosis and oliguria
Fast and weak pulse, Fast and shallow breathing
Stages of Shock
Initial, Compensated, Decompensated/Progressive and Refractory
What is the Initial Stage of Shock
Mean arterial pressure decreased less than 10 mmHg. Compensation is effective. No visible changes. The first stage of shock is hard to detect
What is the Compensated Stage of Shock
Body’s primary goal is to maintain blood flow to heart and brain through vasoconstriction (release of epinephrine) and shunting blood to vital organs. Anaerobic metabolism begins to occur. The body maintains perfusion by decreased peripheral blood flow, tachycardia to maintain cardiac output, tachypnea. Distal pulses become weak skin will present as pale, cool, and diaphoretic, and blood pressure initially seems normal. Capillary refill is delayed. Normal BP does NOT rule out shock as the heart rate increases before BP drops
Perfusion:
the delivery of oxygen-rich blood and nutrients to the body's tissues and organs via the circulatory or lymphatic systems
Decompensated/Progressive Stage of Shock
Inability of the body to sustain adequate perfusion. As hypoxia develops the patient becomes confused and disoriented; as blood pressure decreases, distal pulses become difficult to locate. Patient presents with flat neck veins, pale, cool, clammy skin, hypotension, and oliguria (reduced kidney perfusion)
Hypoxia:
dangerous condition where your body, or a part of it, doesn't receive enough oxygen to function properly, and therefore sending someone into a confused state
Refractory/Irreversible Stage of Shock
Impending death as the body is no longer able to adjust for the extreme blood loss; tissue perfusion is negligible, allowing for cellular necrosis due to lack of adequate oxygen tension. Heart function continues to decline becoming slow and irregular; multi-system organ failure occurs.
Diagnosis Through Imaging
Usually can just be diagnosed through symptoms however we can test for lactic acidosis (through inadequate tissue oxygenation by lab studies)
>4 mmol/L
Overall Treatment Goals for Shock:
Maximise cardiac output (fluids, blood, vasopressors) and increase oxygenation (intubation or non invasive ventilation)
Oxygen delivery is needed to increase Cardiac output (CO), Hemoglobin (Hb) and Oxygen saturation (SaO₂) and decrease agitation, fever and work of breathing
What is Hypovolemic Hemorrhagic Shock?
Acute hemorrhage causing rapid reduction in blood volume (red blood cell mass and plasma)
↓ Blood volume → ↓ cardiac output → ↓ oxygen delivery
Causes of HHS?
External (trauma) or internal bleeding (abdominal aortic aneurysm, GI sources, blunt trauma, fractures, arterial or venous injury, ectopic pregnancy)
High Risk leeding Areas: Thorax, Abdomen, Pelvis and Upper Legs (Femur)
Treatment for HHS:
Volume Resusitation (isotonic fluid to increase volume)
Blood Transfusion
If BP is low and actively bleeding (90/60) you want to go to a lower BP than normal because then the body has just enough blood flow to work normally (100/60 rather than 120/80). This prevents further bleeding and dislodging clots
What is Non Hemorrhagic Hypovolemic Shock:
There is no bleeding but loss of fluids (diarrhea or dehydration) 9 Non-hemorrhagic hypovolemic shock arises when volume intake is insufficient to make up for volume losses)
↓ Plasma volume → ↓ Cardiac output → ↓ oxygen delivery
What are the Causes of NHHS
Inadequate fluid intake (tea and toast)
Excessive output: renal diuresis (diabetes insipidus), gastro-intestinal losses, Insensible losses (skin, respiratory), third space (burns, pancreatitis, peritonitis)
Metabolic derangements (hyperglycemia, inborn error of metabolism)
How can it be diagnosed as NHHS?
Sodium levels are elevated,
Hemoglobin/hematocrit are elevated due to hemoconcentration
Creatinine is elevated (renal function is decreased)
Treatment for NHHS:
Oxygenation and Ventilation
Isotonic fluid resusitation
What is Cardiogenic Shock
Characterized by reduced cardiac output (heart cannot pump enough blood) resulting in decreased oxygen delivery to the tissues
↓ Cardiac output → ↓ oxygen delivery despite normal volume
What are the Causes of Cardiogenic Shock?
Myocardial Infarction that is due to ischemia
How can Cardiogenic Shock be Diagnosed in Hospitals:
Clinical: chest pain, shortness of breath, syncope, oliguria, altered mental status, hypotension, tachy-or bradycardia, peripheral edema.
ECG: ischemia or arrhythmias
Chest-X-ray: pulmonary congestion
Laboratory: elevated troponin levels
Treatment for Cardiogenic SHock
Ensure adequate oxygenation and ventilation
early revascularization with PCI (remove plaque), coronary bypass surgery, or thrombolytics ( dissolve blood clots)
What is Obstructive Shock?
ccurs when extra cardiac obstruction impedes cardiac filling (reduces preload) or impairs cardiac output (increased afterload).
Causes of Obstructive Shock
Cardiac Temponade
Pulmonary Embolism: Blood clot trapped in the artery restricting oxygen and blood flow
Tension pneumothorax: Air is trapped in the chest so it compresses lungs and great veins (vena cava) due to increase in intrathoracic pressure
Symptoms of Obstructive Shock
Jugular Vein Distention: neck veins popping out
Blood clots in the veins
Treatment for Obstrucitve Shock:
Pericardiocentesis (Tamponade) → drain excess fluid from the pericardium
Relief of tension (Pneumothorax)
Thrombolysis (Pulmonary Embolism) → clot breakdown
What is Distributive shock:
a medical emergency where severe blood vessel dilation (vasodilation) and leaky capillaries cause a dangerous drop in blood pressure
therefore blood "spreads out” and does not reach organs effectively
eg. Anaphylactic and Septic shock
Causes of Distributive Shock
Sepsis
Anaphlaxis
Hypothermia: Rapid external heat causes the peripheral blood vessels to open up suddenly, sending this cold, acidic blood back into the core circulation, overloading the already strained heart.
Neurogenic shock
Pulmonary Embolism
Part of Obstructive Shock
It comes from a blood clot in one of the pulmonary arteries in the lungs causing restriction of blood flow/shortness of breath
Hypovolemic Shock Symptoms (End):
Low BP, High Pulse, High Respiratory Rate, Vasoconstriction, Pale and Cold
Cardiogenic Shock Symptoms (End):
Low BP, High and Weak Pulse, High Respiratory Rate, Vasoconstriction, Pale and Cold
Obstructive Shock Symptoms (End):
Low BP, Vasoconstriction, High Pulse, High Respiratory Rate, Pale and Cold
Distributive Shock:
Vasodilation, High or Low BP, High or Low Pulse Rate, High or Low Respiratory Rate, Normal/Red and Warm