Old Midterm Review Sheet Material for the Final - Posterior Segment & Ocular Disease Spring 2026
1/148
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
149 Terms
-liquefaction
-condensation
-atrophy of the hyaloid
What are the age-related changes that occur in the vitreous?
-the slow development of floaters
-an occasional flash
Age related changes in the vitreous will lead to what?
true
True or False:
Age related changes to the vitreous can lead to a PVD?
flashes (or maybe floaters when the PVD nears completion)
As a PVD progresses, you can get an increase in ________
The vitreous begins to move more and because floaters previously near the retina become more visible
Why can a PVD lead to flashes and floaters?
an increase in floaters and/or possibly a complaint of one large floater
A complete PVD is often accompanied by what:?
Weiss (Vogt) ring
THE one large floater secondary to a PVD
true
True or False:
If you have a sudden increase in floaters, and it is a shower of floaters, it could be a vitreous heme or occasionally a vitritis
1) Get to ora in EVERY QUADRANT
2) If no break, re-examine by 1/1/6 rule
3) Warn the patient to return if the symptoms continue to increase over what is found that day
What is the management plan if flashes or floaters are seen regularly and/or increasing?
1) Get to ora in EVERY QUADRANT
2) If no break, re-examine by 1/1/6 rule
3) Warn the patient to return if the symptoms continue to increase over what is found that day
What is the management of a preretinal heme that is thought to be D/T TRACTION?
1) ERM
2) Preretinal Heme
3) Breaks (Holes and Tears)
4) Retinal Detachment
What are the conditions that can be caused by vitreoretinal traction?
Going to occur before a complete PVD or within 4-6 weeks after the complete PVD (posterior hyaloid will still be attached at the vitreous tails for a few weeks)
The disorders d/t vitreoretinal traction will usually occur when?
-MUST REFER IF flashes/floaters, OR a large edema ring >1DD, or encroachment 2DD past the equator towards the posterior pole
-Can monitor atrophic holes in 1 year unless referral criteria are met
-Monitor operculated holes in 6 months unless referral criteria are met
Management plan for retinal holes?
MUST REFER
Management plan for retinal tears?
rhegamatogenous RD
What is the most common form of retinal detachment?
from a tear or break in the retina
What is a rhegamatogenous retinal detachment d/t?
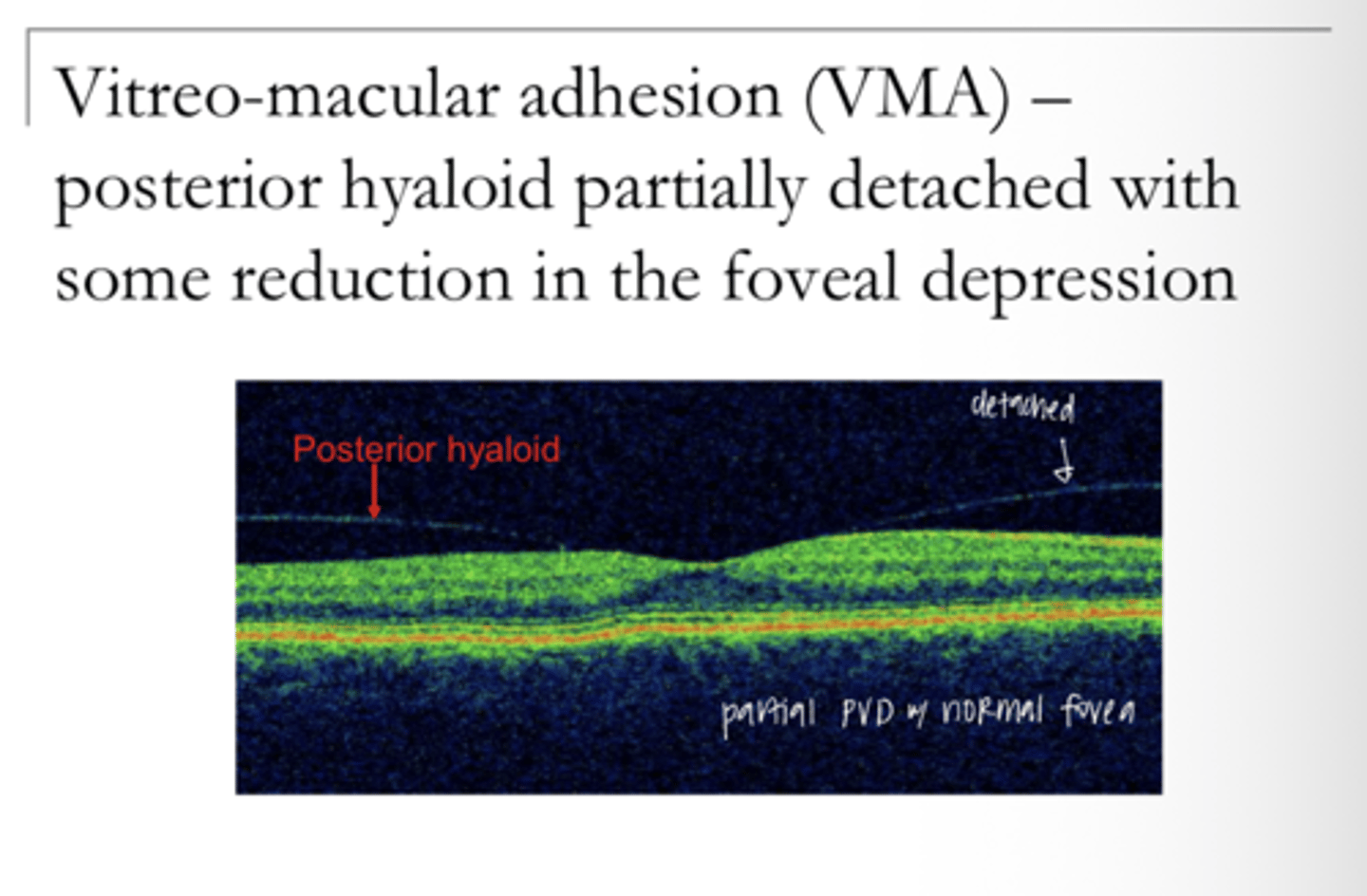
Imcomplete detachment of the hyaloid from the retina (hyaloid still attached at the macula) with no macular distortion
Describe Vitreomacular Adhesion (VMA)
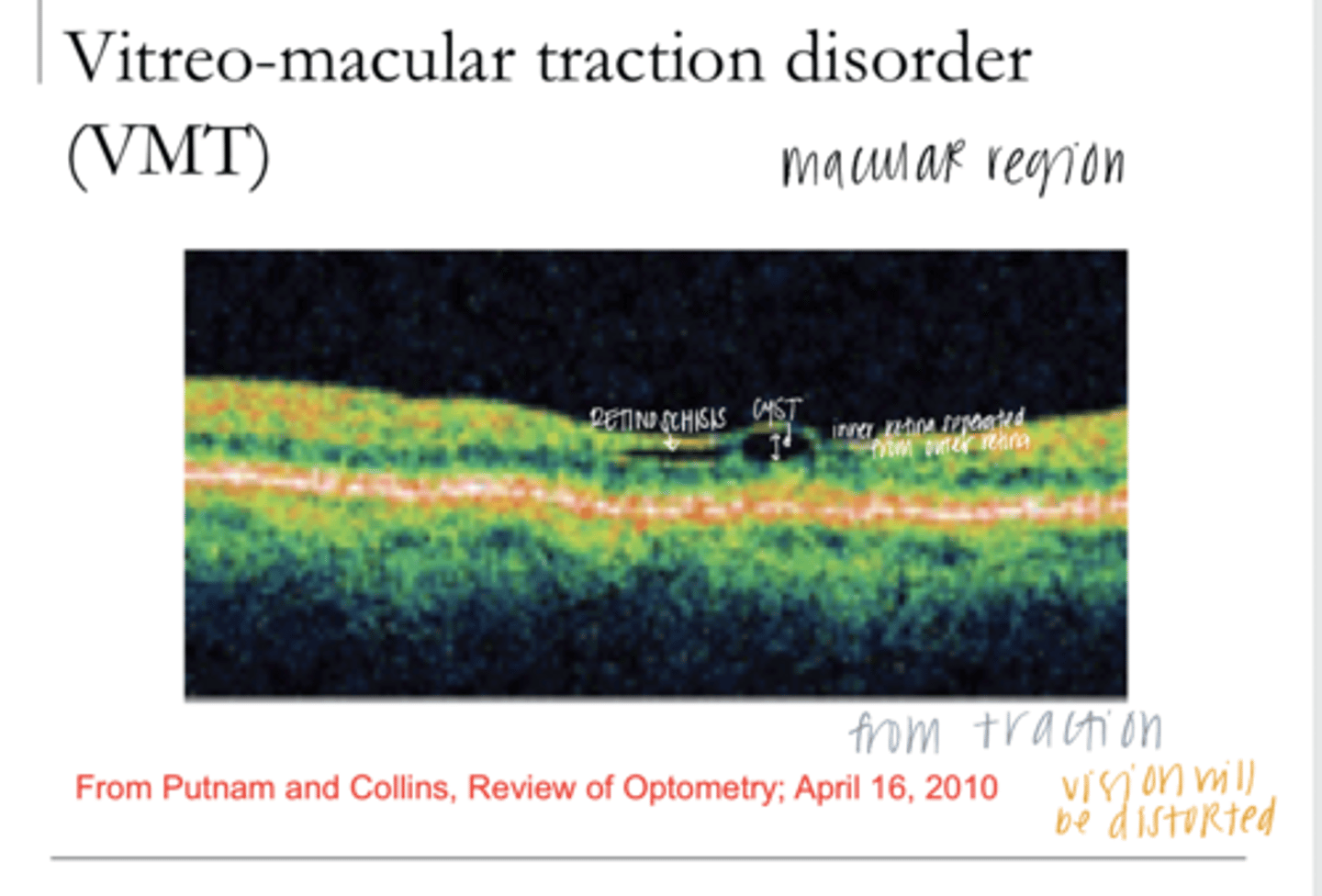
Incomplete detachment of the hyaloid with distortion of the macula (potentially a macular cyst which is technically a localized retinoschisis)
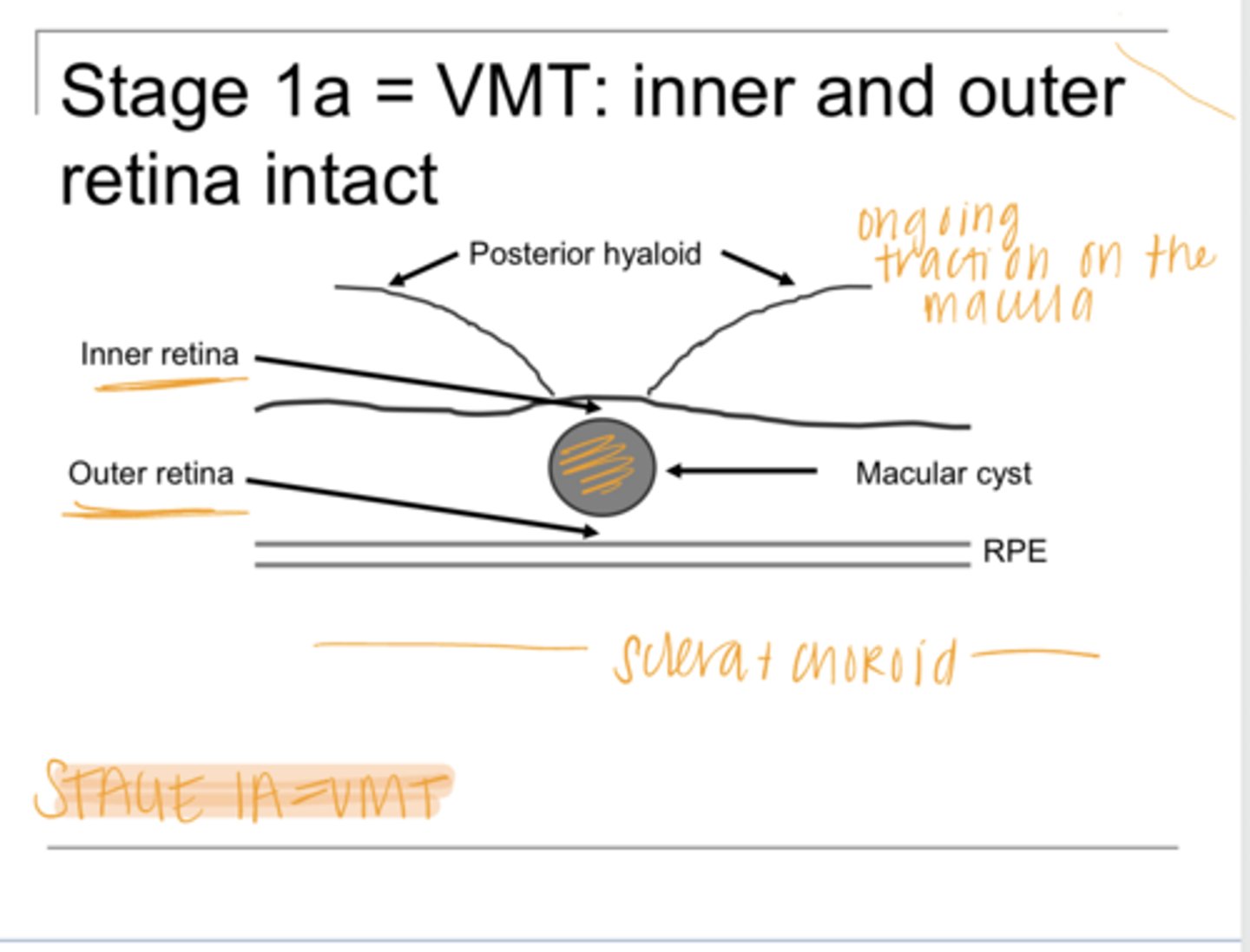
Describe Vitreomacular Traction (VMT)
anterior-posterior separation of the inner and outer retina
With VMT, there is _____ separation of the retina, Where?
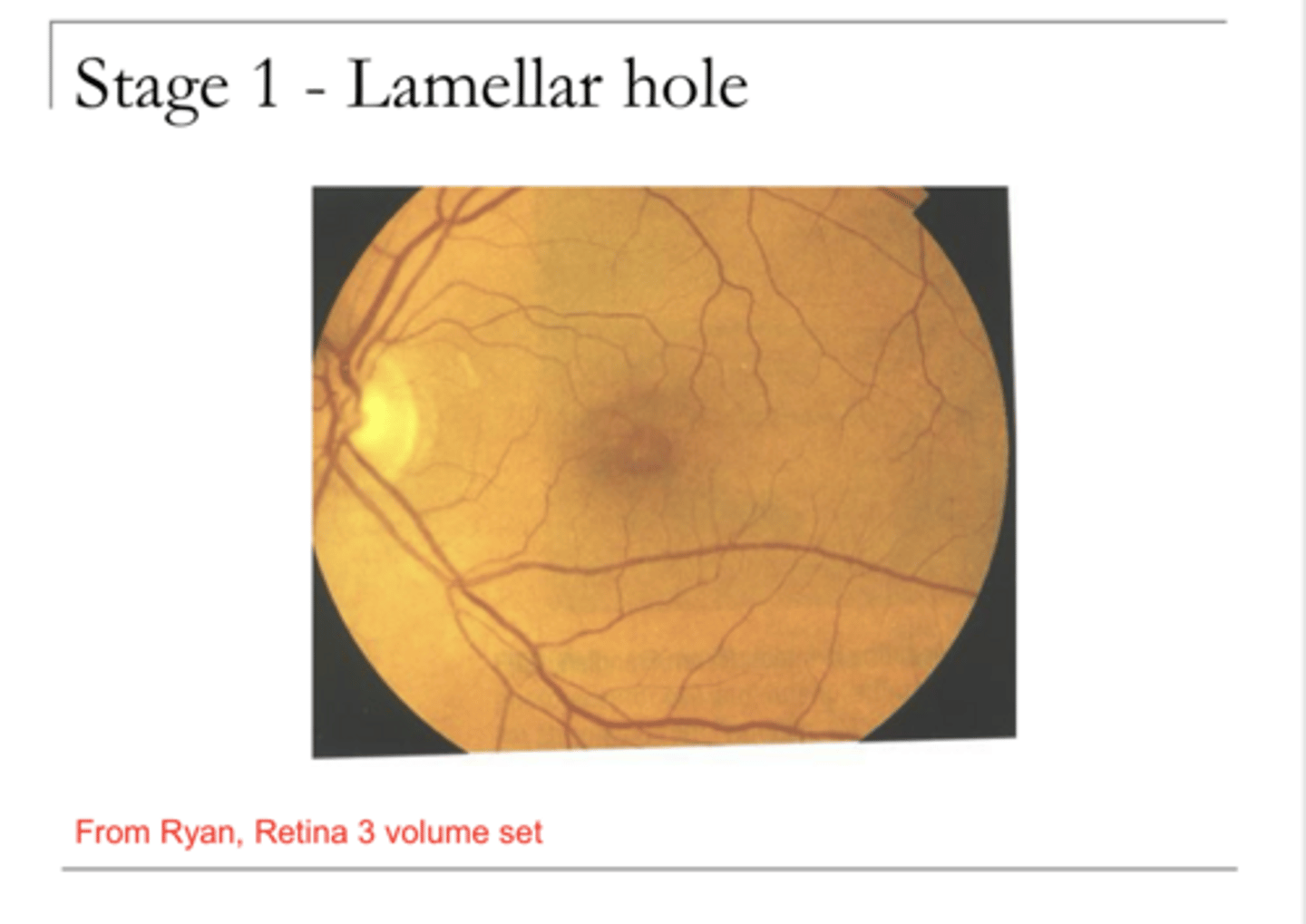
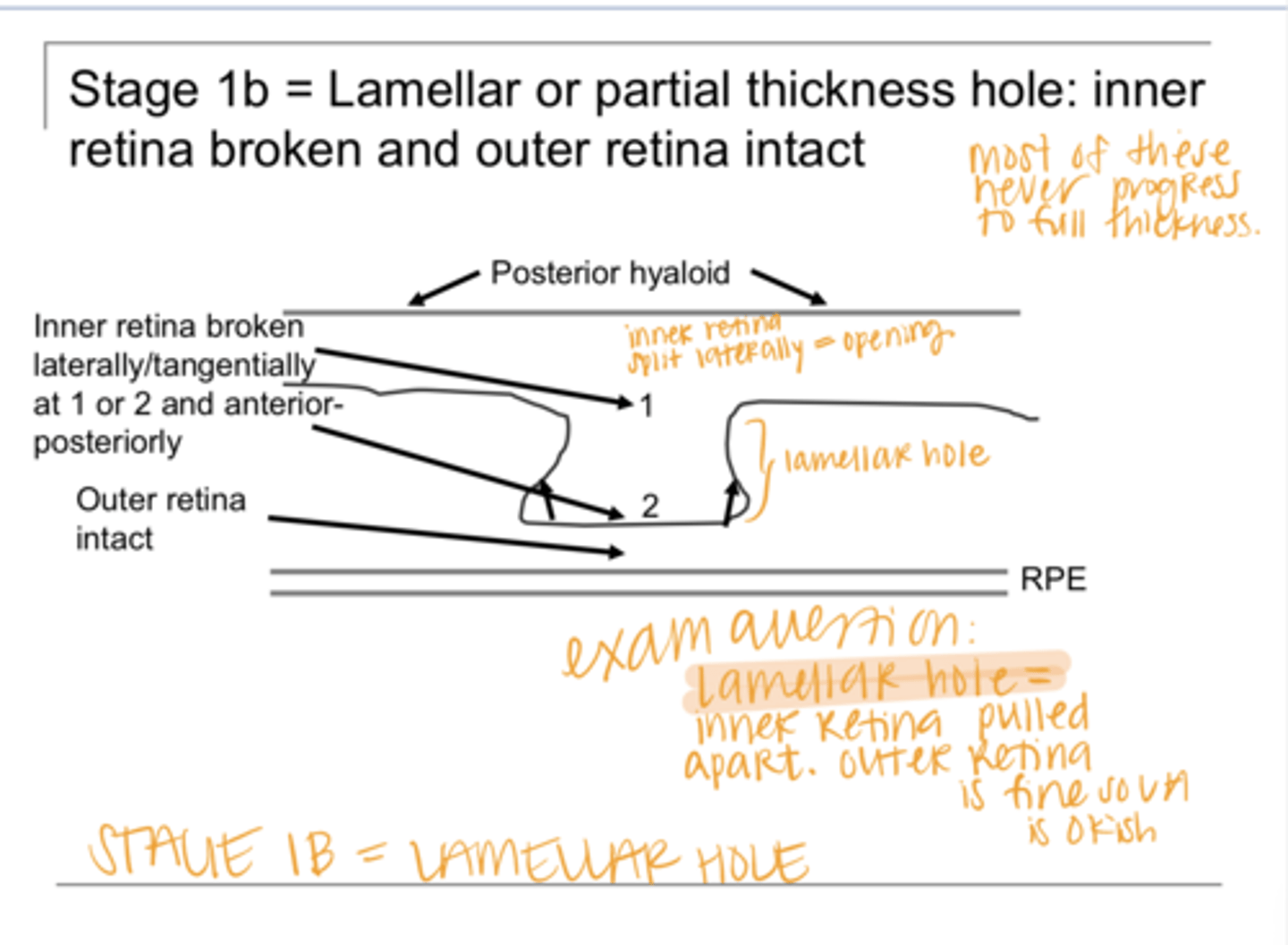
lateral break in the inner retina with an intact outer retina (may be a retinoschisis)
Describe Lamellar Hole
anterior-posterior separation of the inner and outer retina
With a lamellar hole, there is _____ separation of the retina, Where?
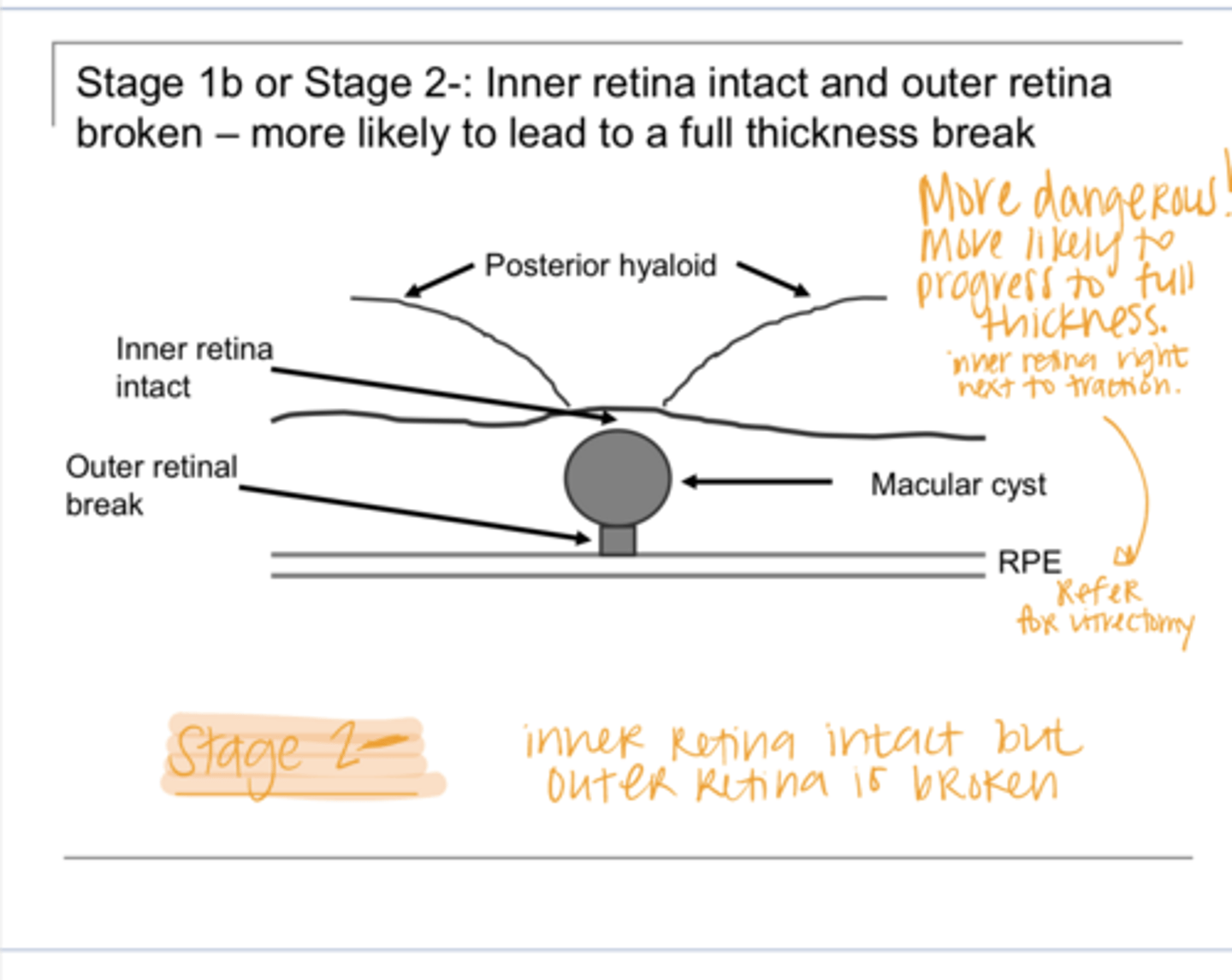
Lateral break in the outer retina with inner retina intact
Describe Stage 2- Macular Hole
Small (<400 micron) full thickness hole
Describe Stage 2 Macular Hole
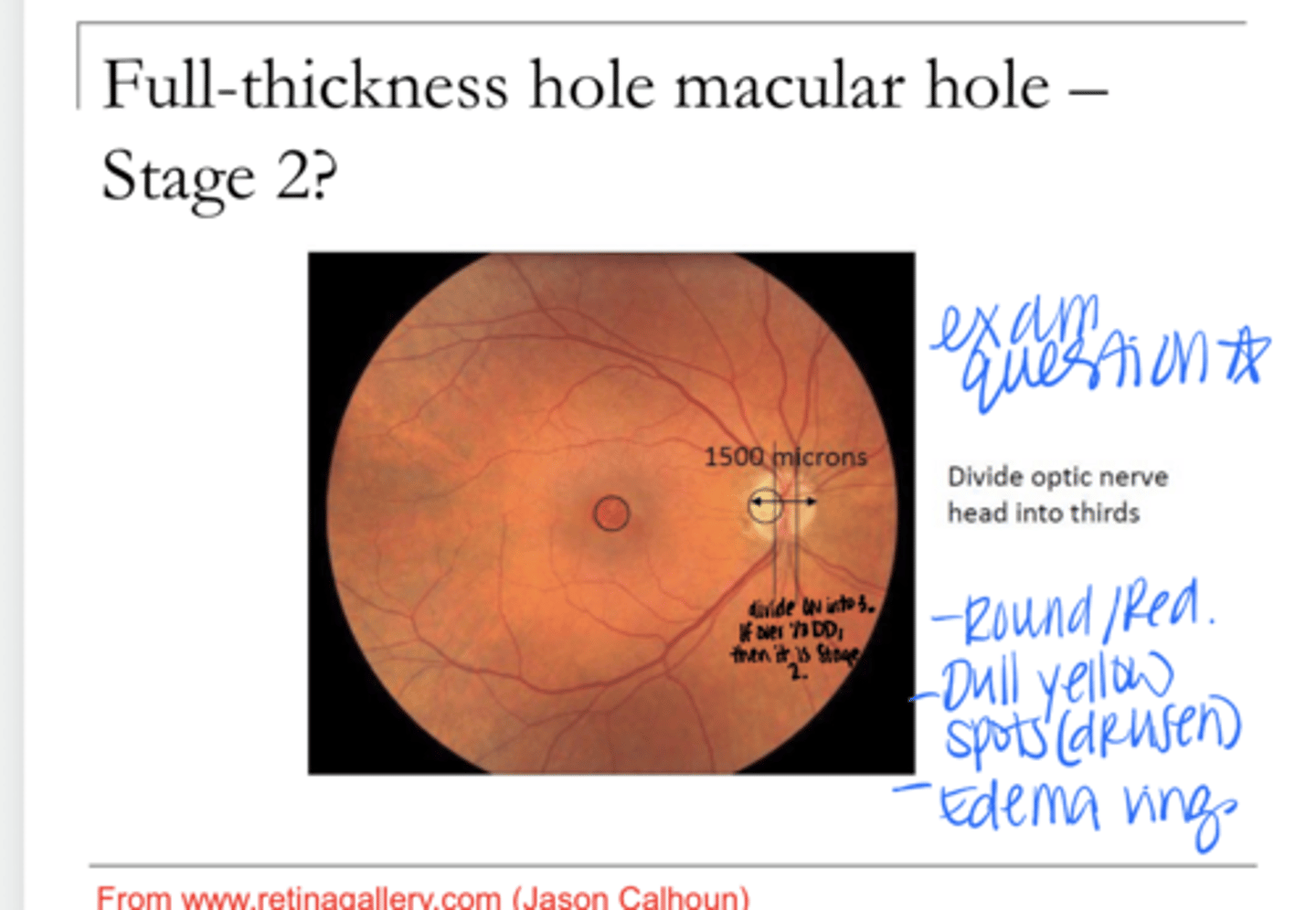
Full thickness hole >400 microns; with vitreous still attached to the macula
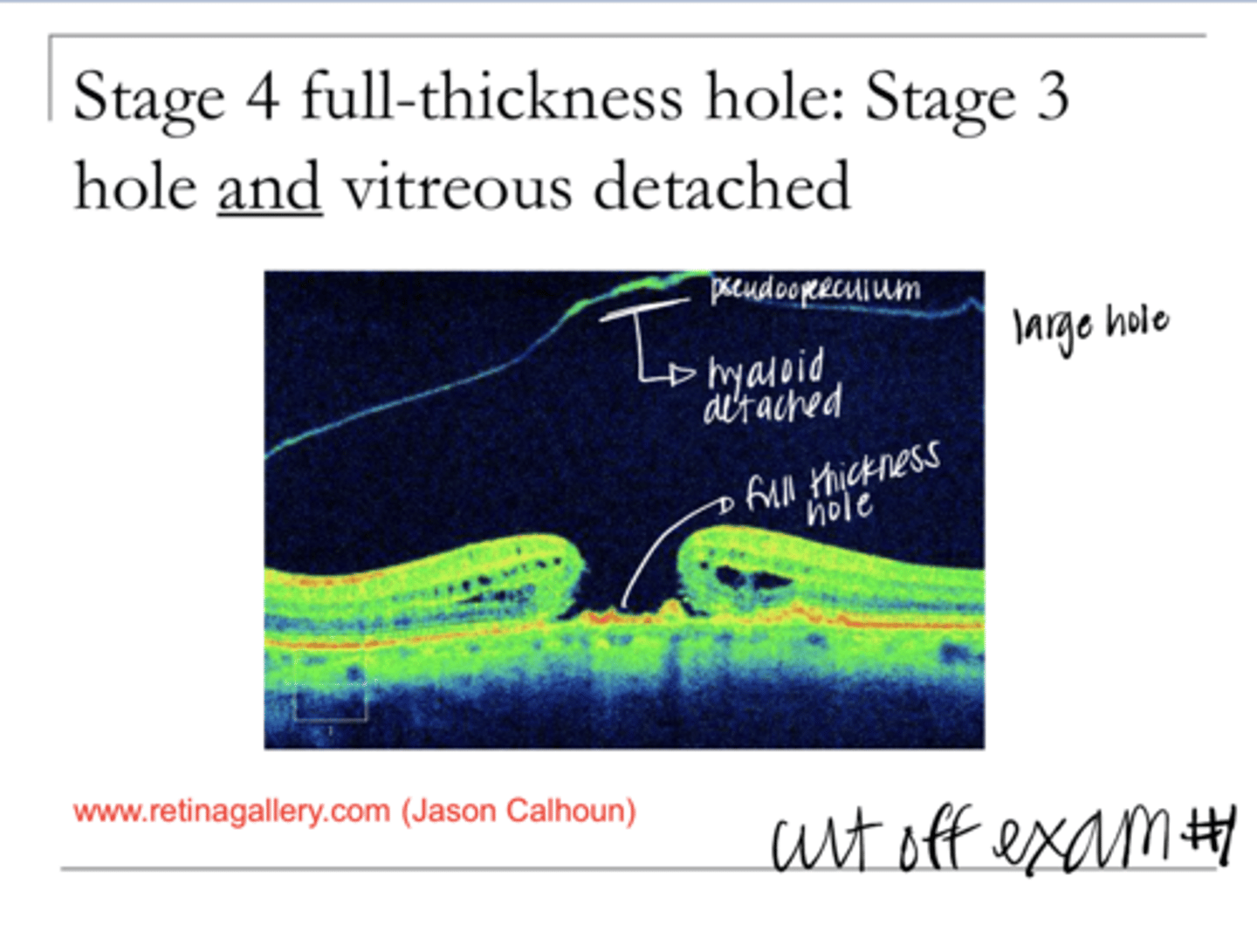
Describe Stage 3 Macular Hole
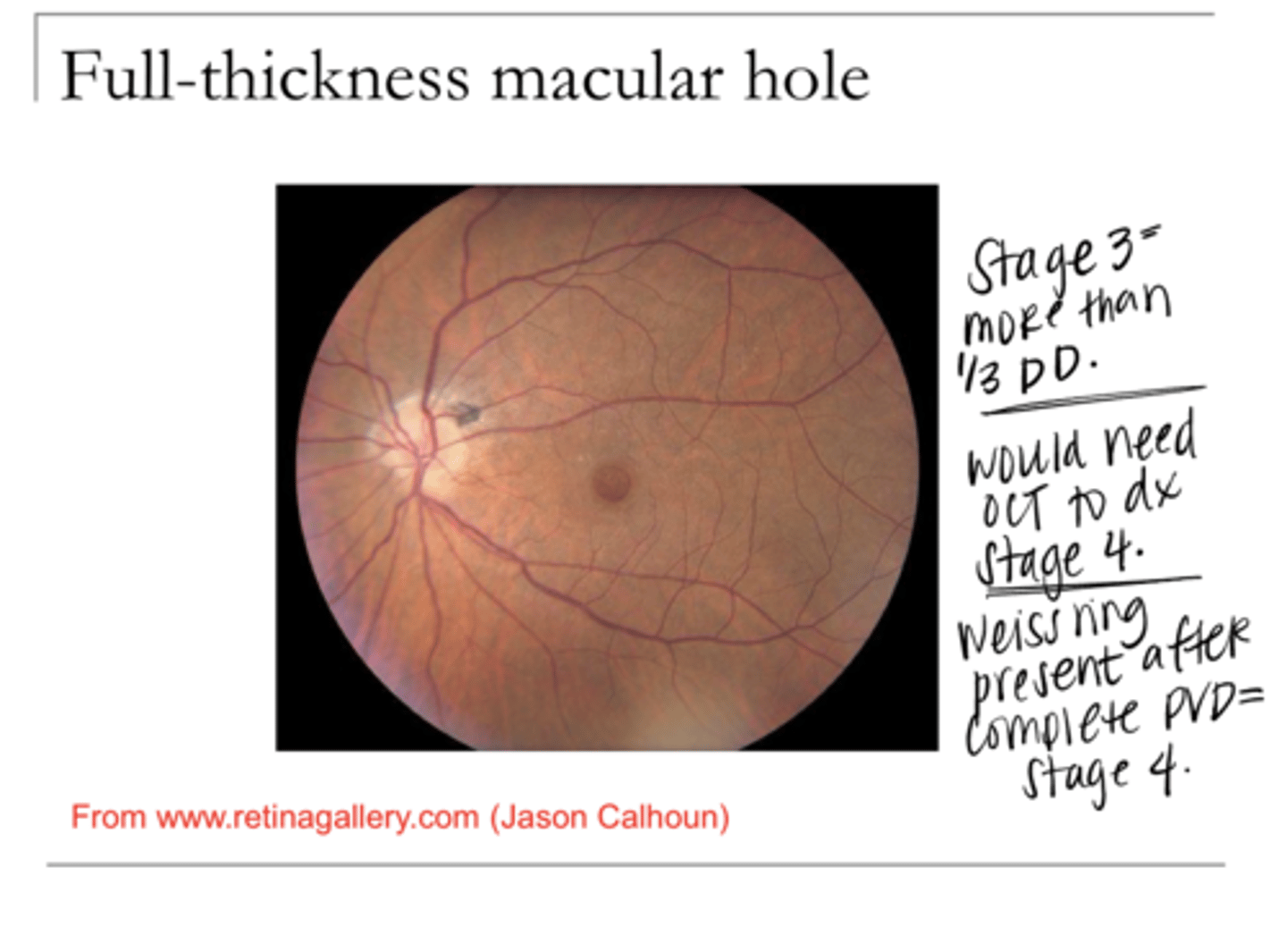
Full thickness hole >400 microns AND the vitreous is detached from the macula (but can still be attached elsewhere)
Describe Stage 4 Macular Hole
usually in the periphery
Unifocal CHRPE Location in the Retina
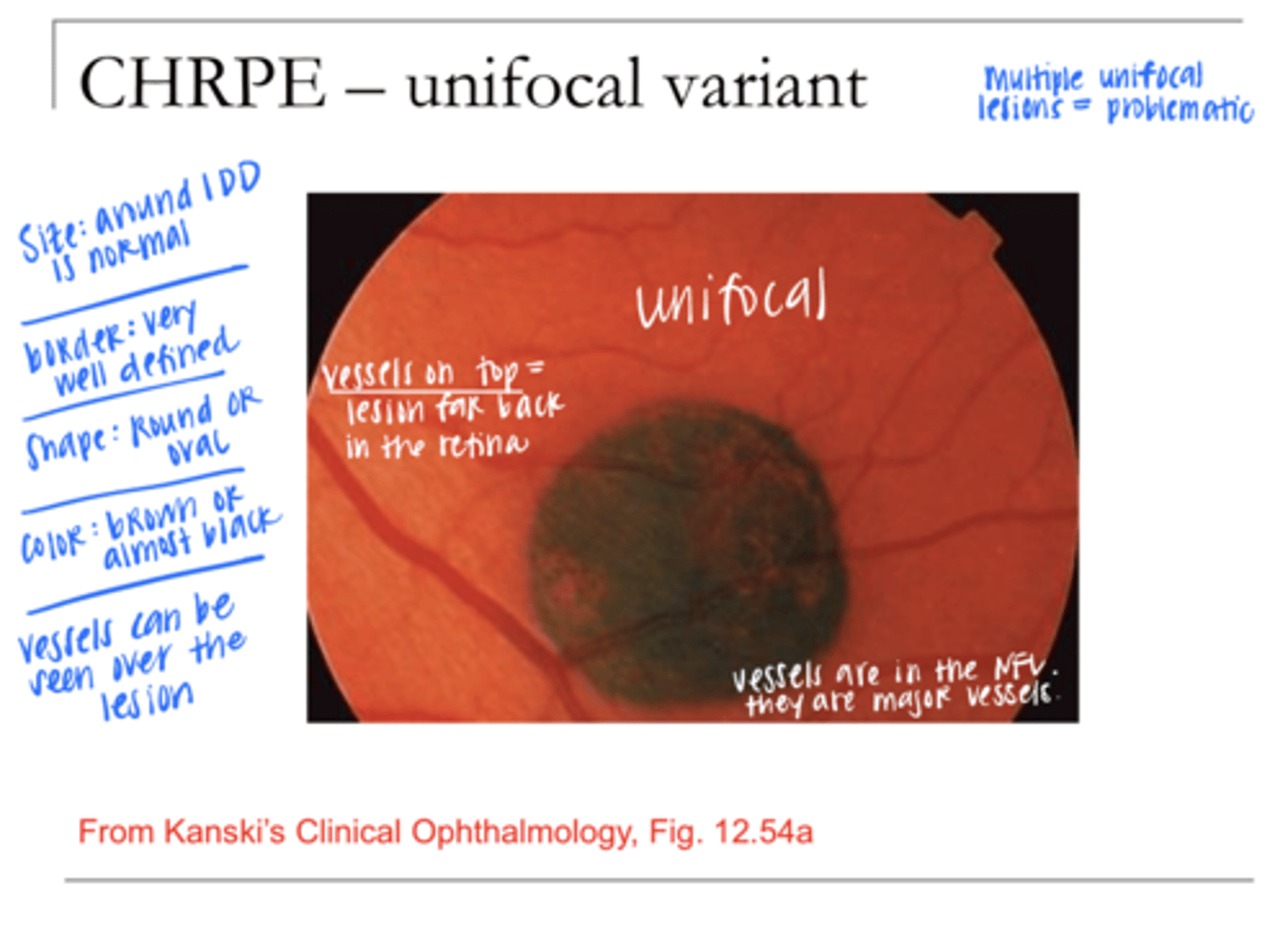
Usually <2DD in size
Unifocal CHRPE Size
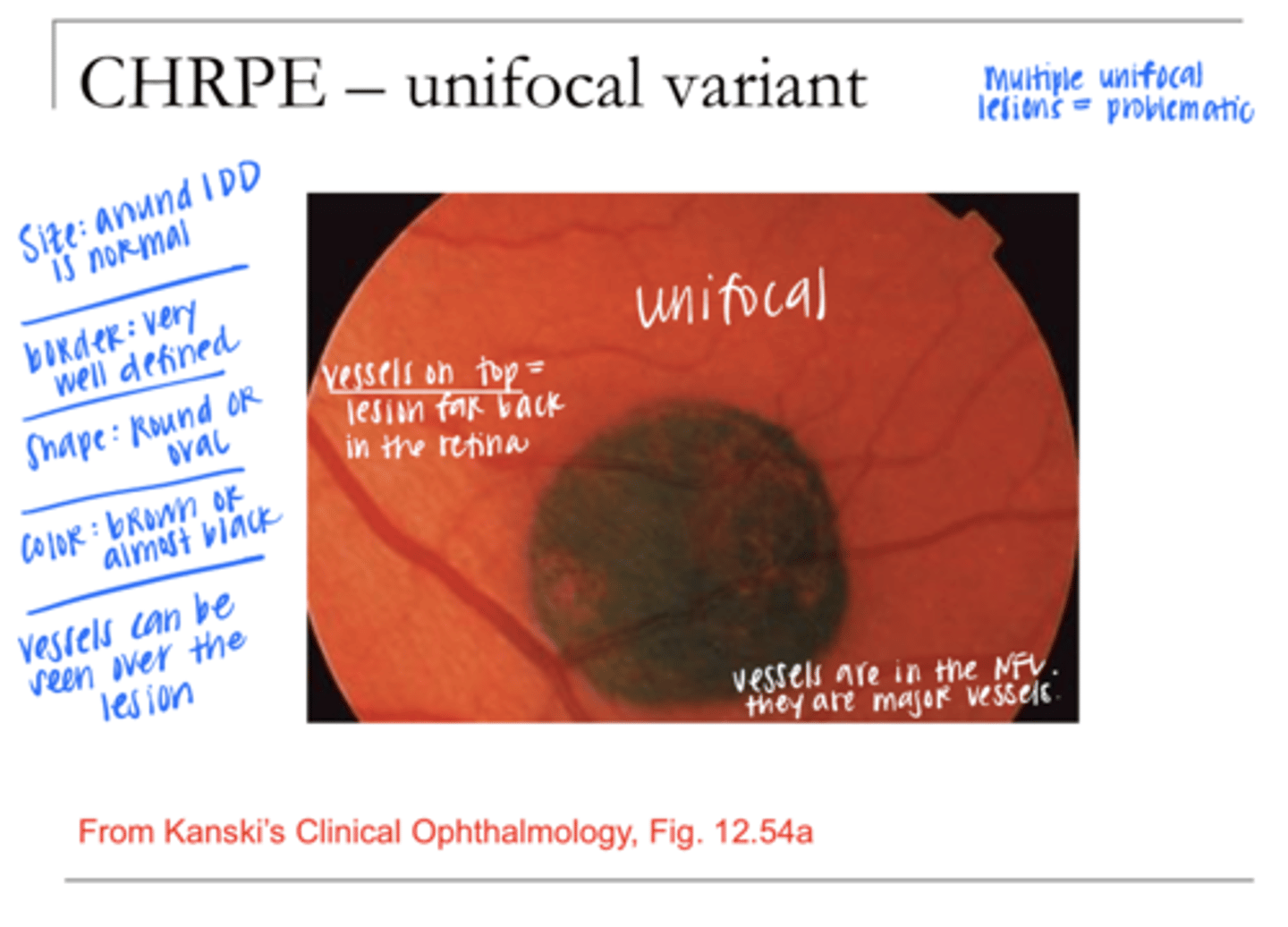
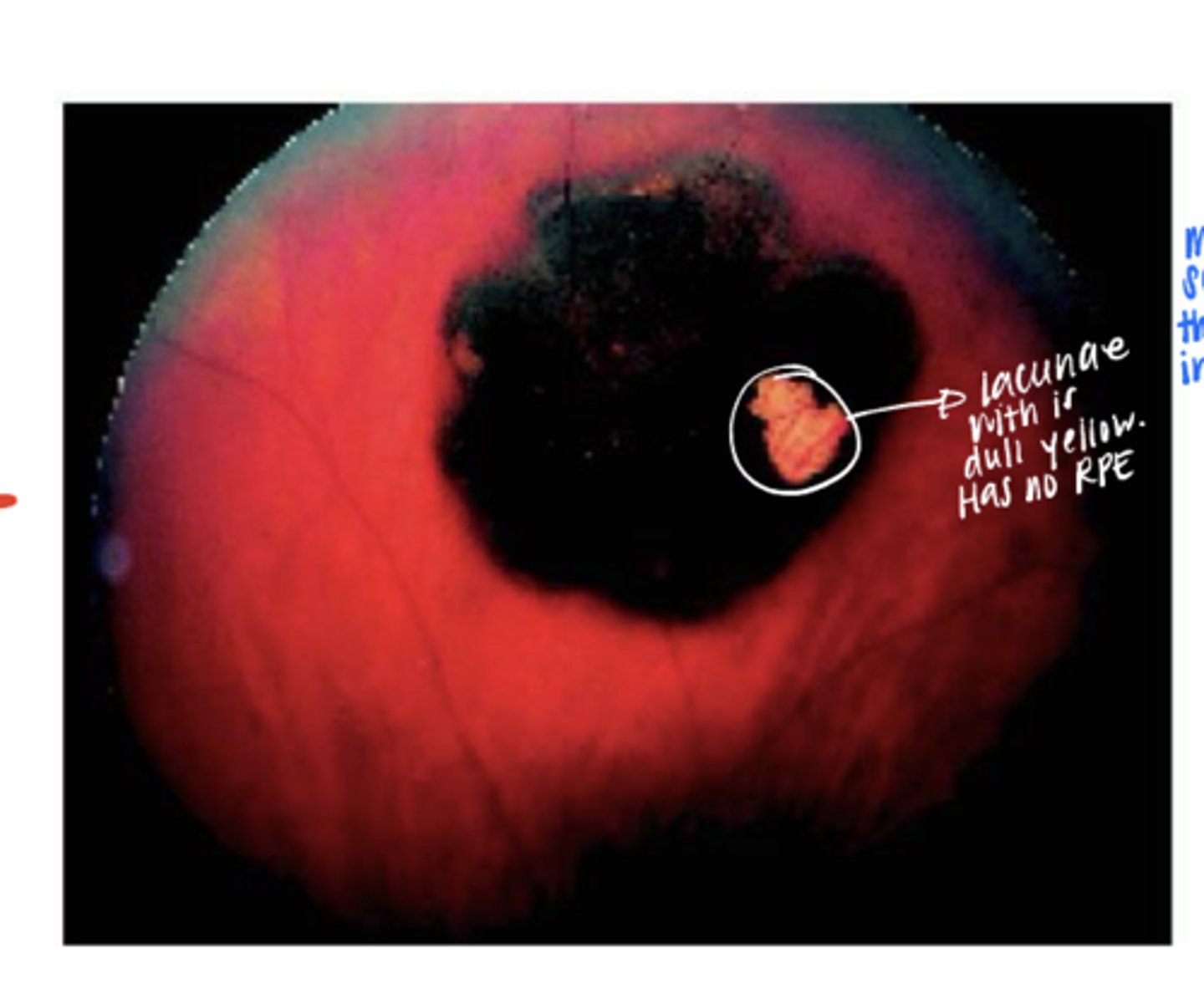
Dull yellow lacunae
What may appear with a Unifocal CHRPE?
<2DD
What is the typical size of a nevus?
Benign
Is a nevus benign or malignant?
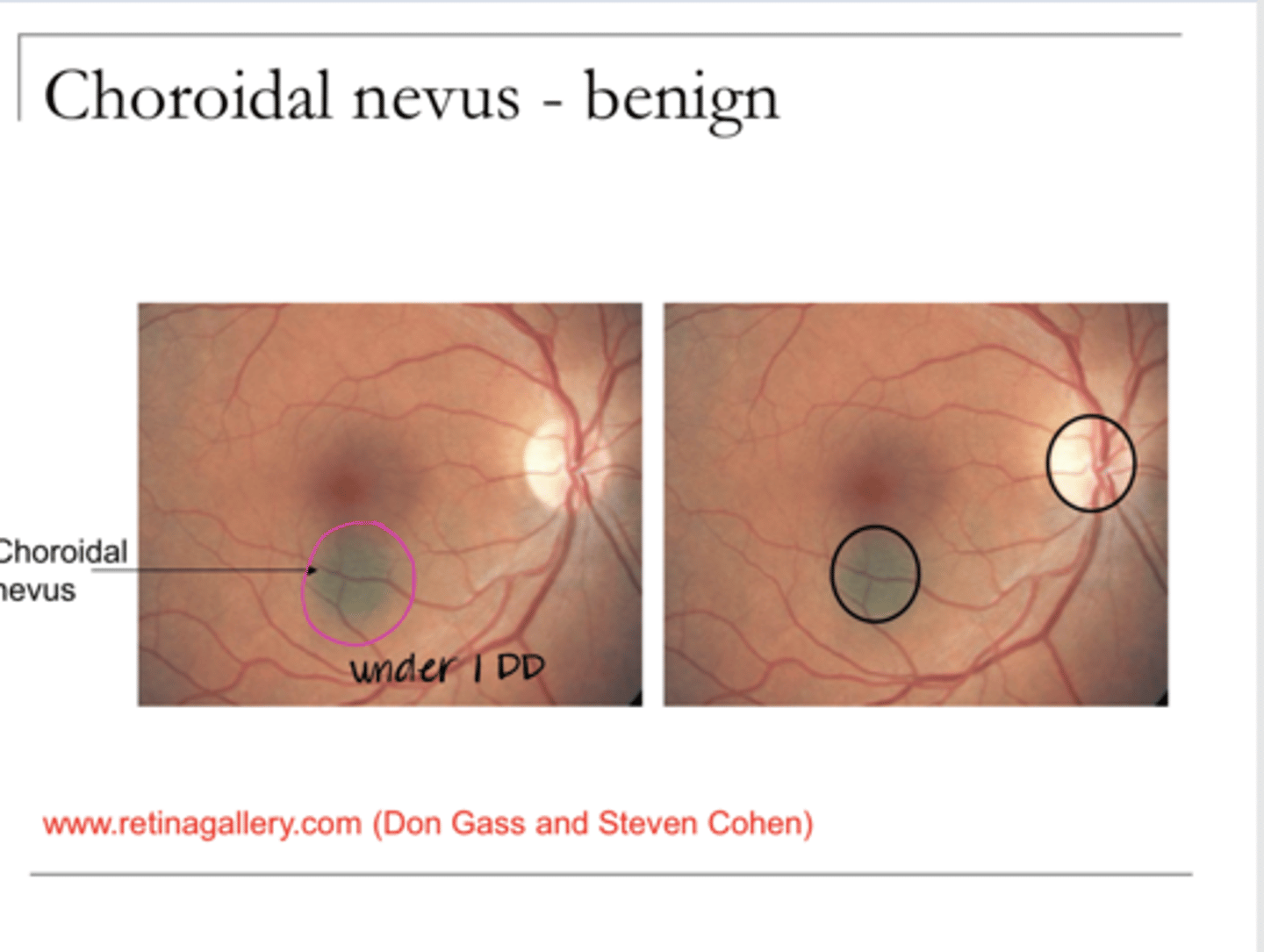
5
A nevus of >_____DD is malignant until proven otherwise
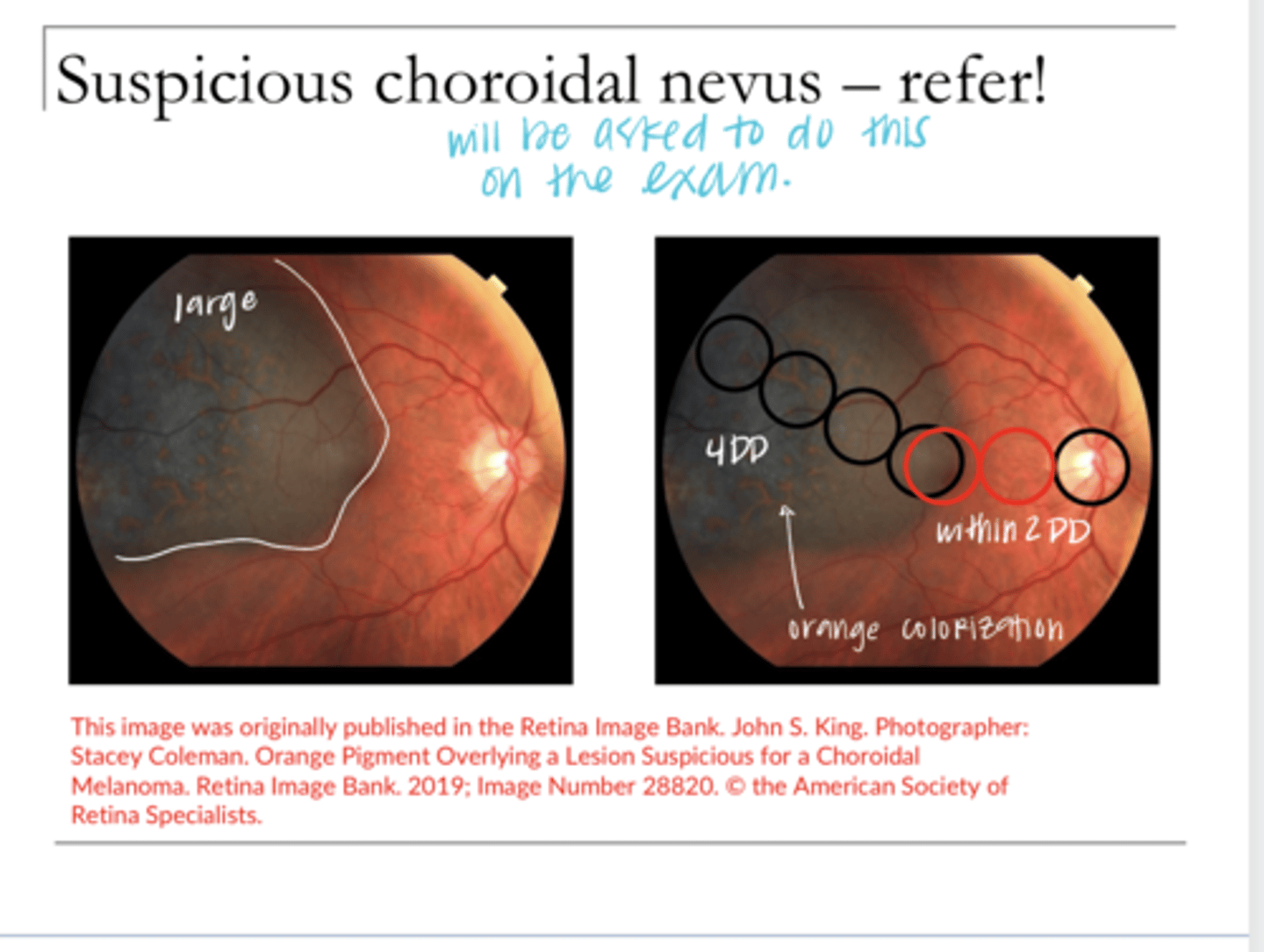
TFSOM-UHHD
Look at the size, Look for changes in Color (orange = bad) Border, Elevation, Serous Detachment, Thickness >2mm
How to diagnose malignant melanoma?
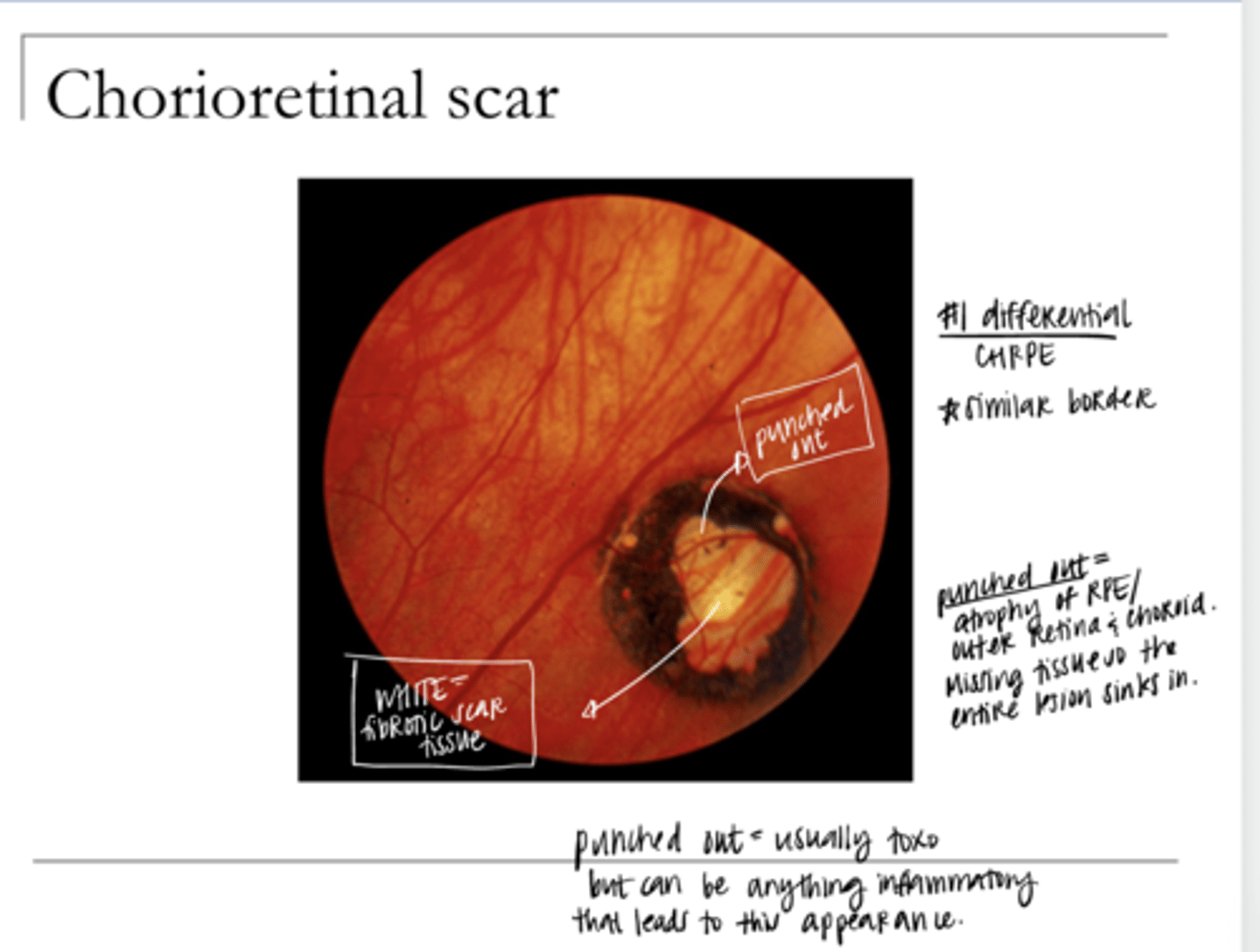
toxoplasmosis infection
What is the #1 cause of a chorioretinal scar?
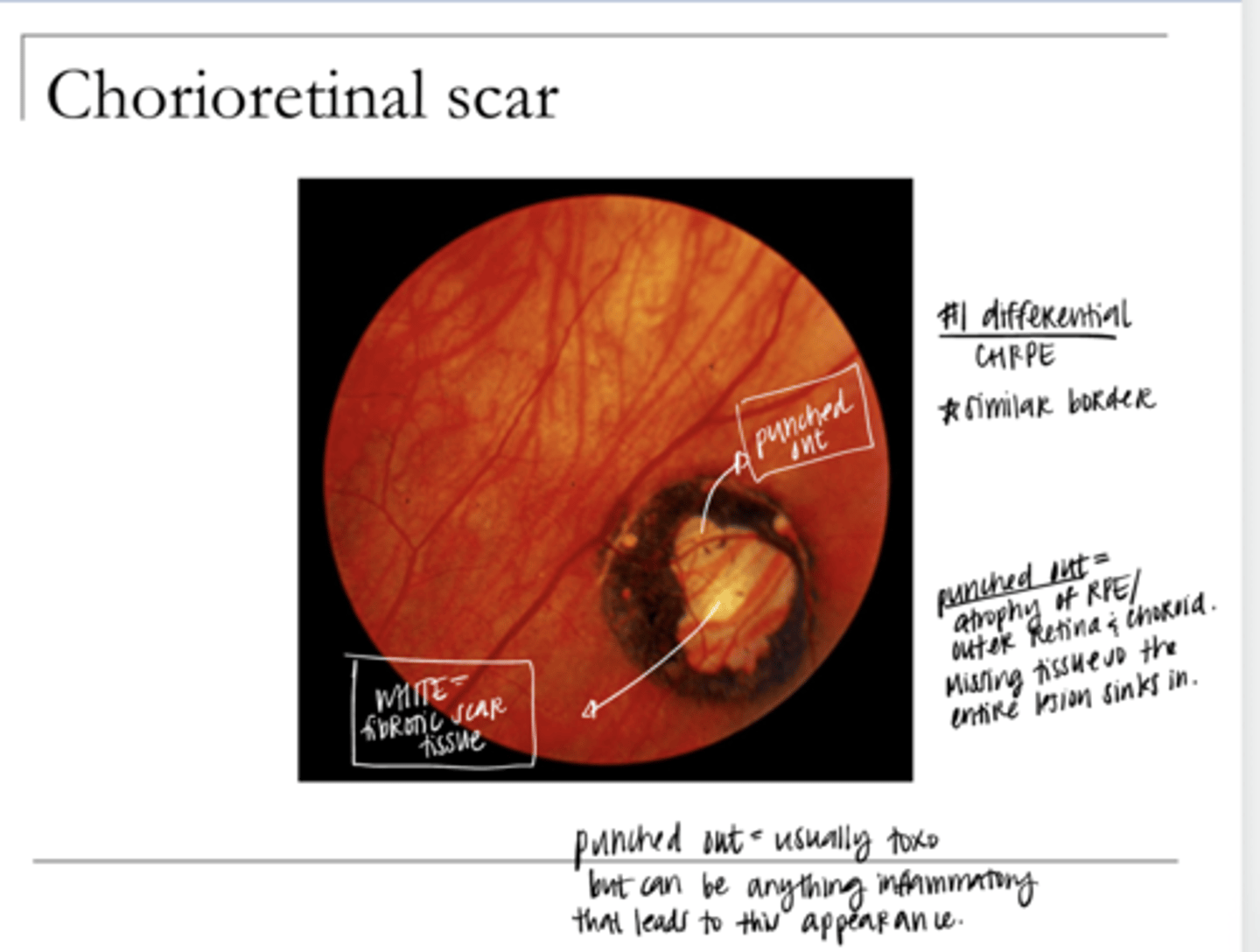
Ingested from cats, ingested from undercooked meats, or congenital
What is the etiology of a toxoplasmosis infection?
Chorioretinal Scar Pic
Chorioretinal Scar Pic
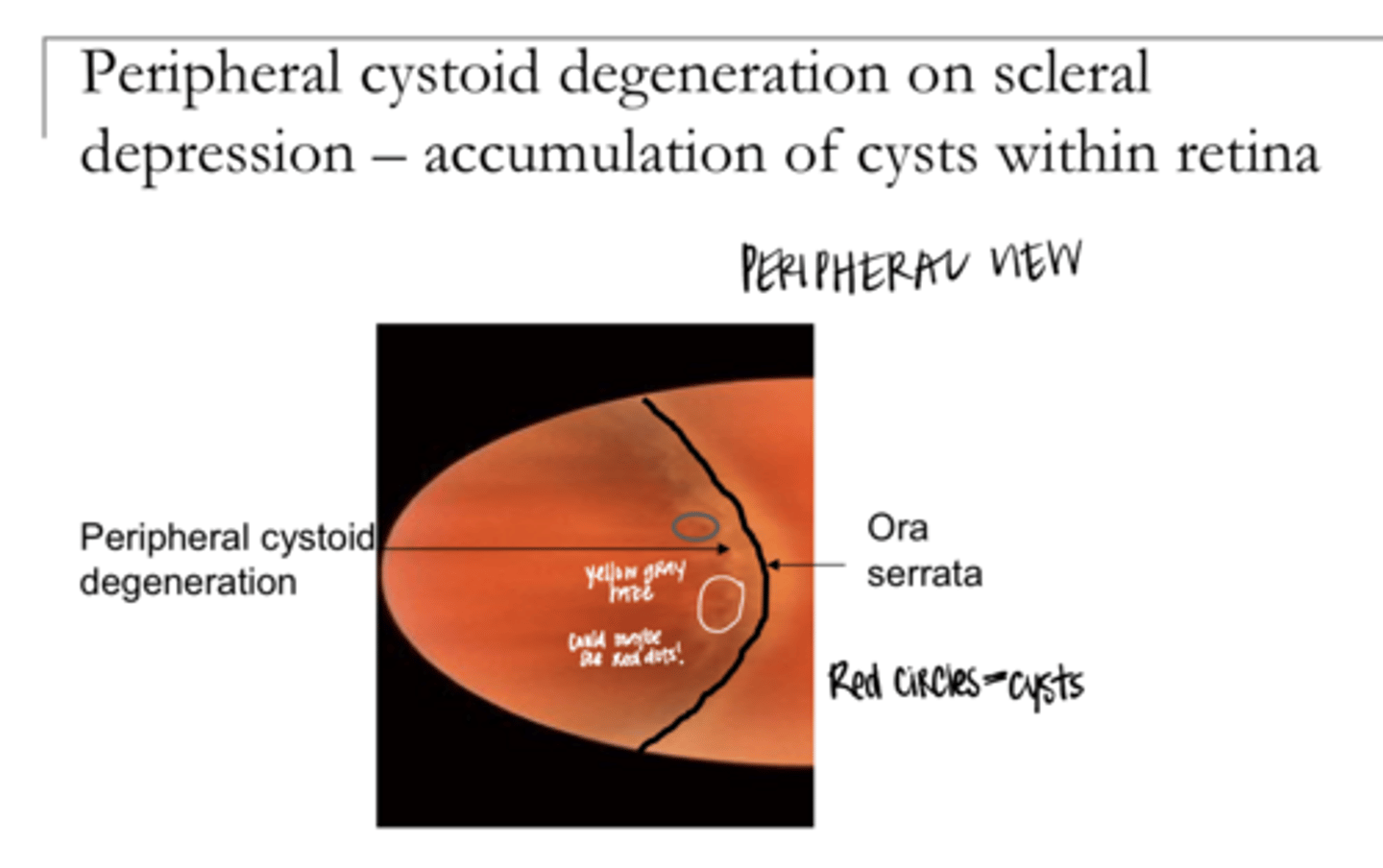
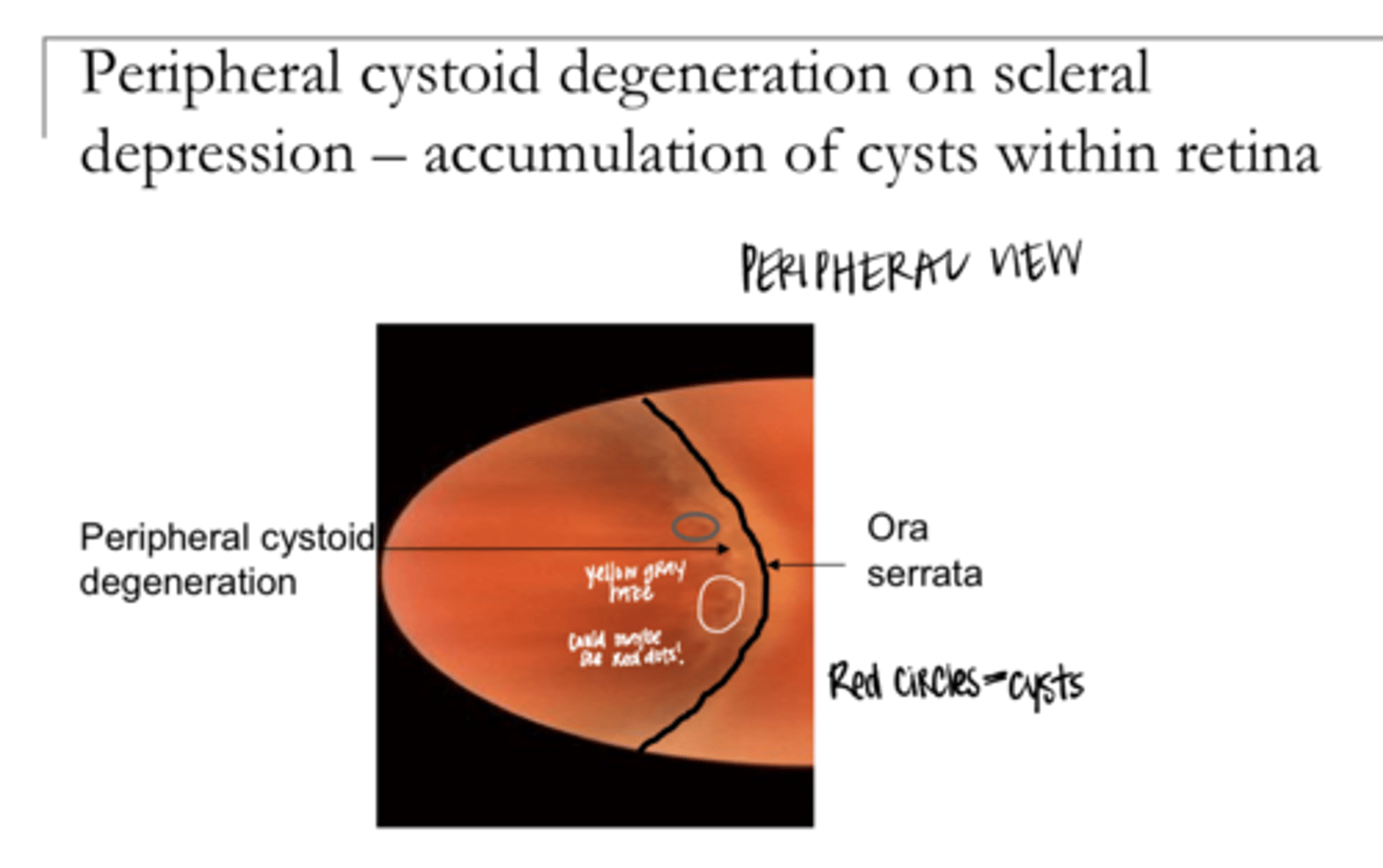
Cystoid Retinal Degeneration Pic
Cystoid Retinal Degeneration Pic
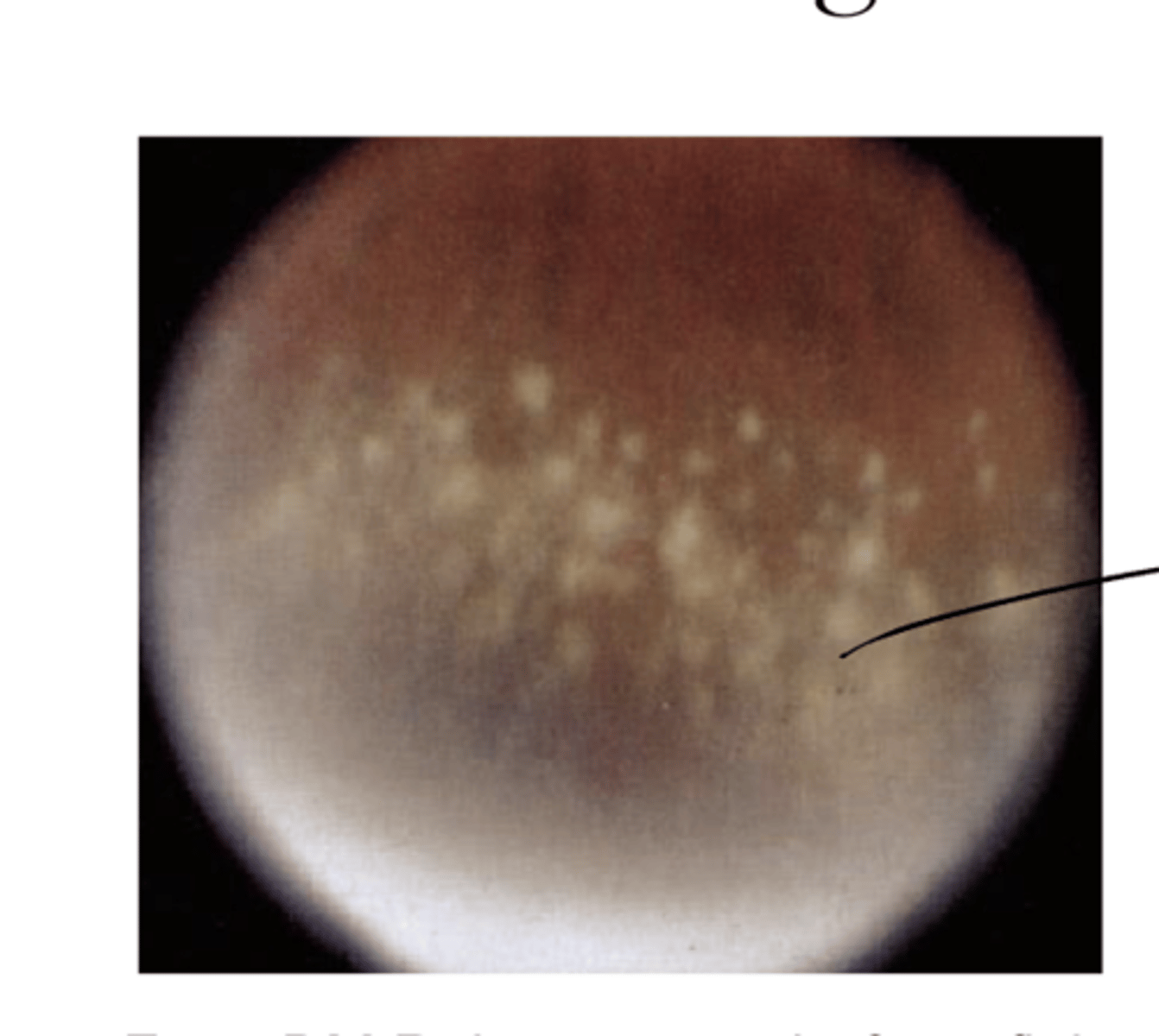
Snowflake Degeneration Pic
Snowflake Degeneration Pic
Snailtrack Degeneration Pic
Snailtrack Degeneration Pic
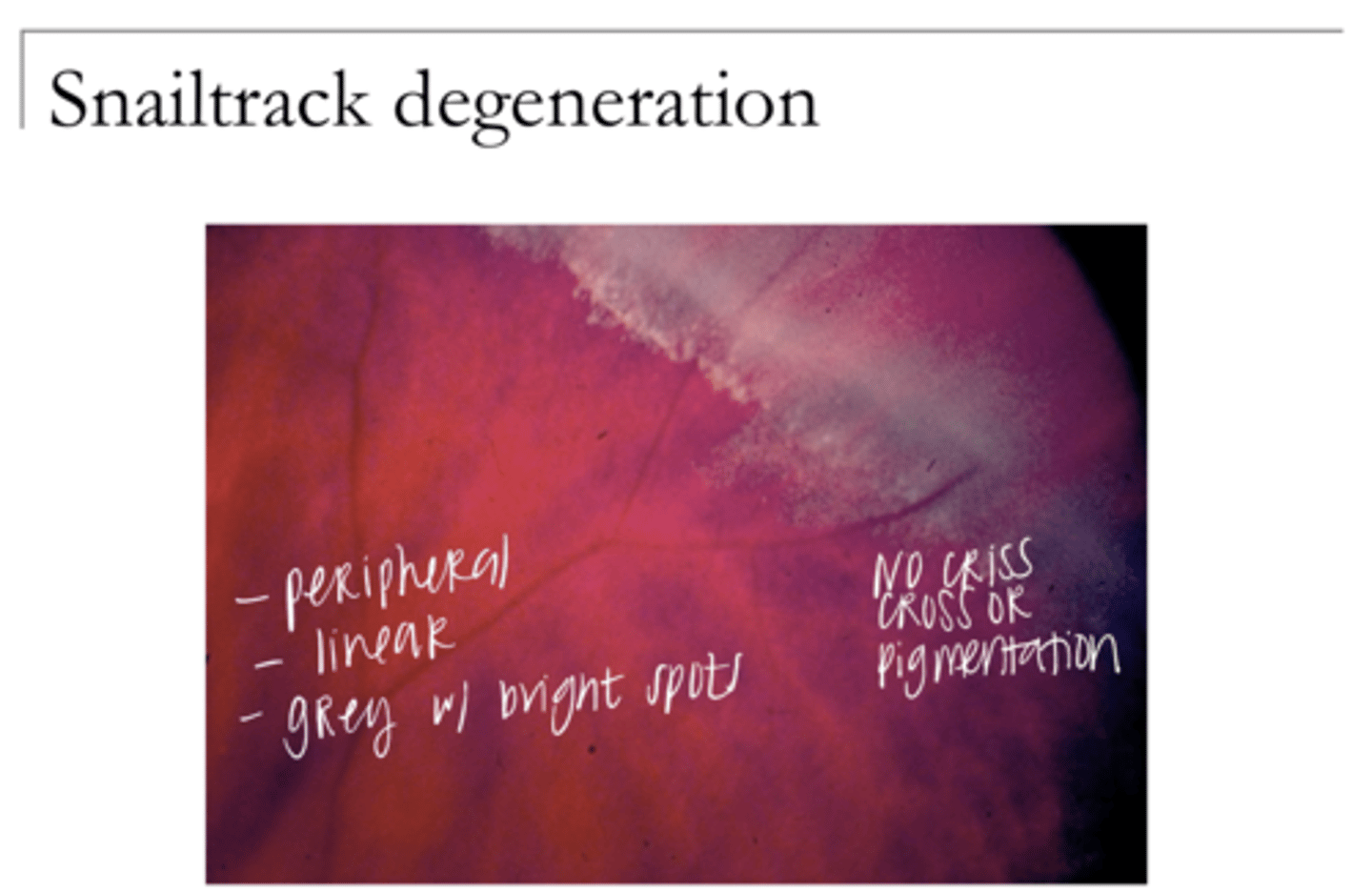
they all lead to shiny spots peripherally
Why are cystoid/snowflake/snailtrack all differentials?
Cystoid Degeneration Pic
Cystoid Degeneration Pic
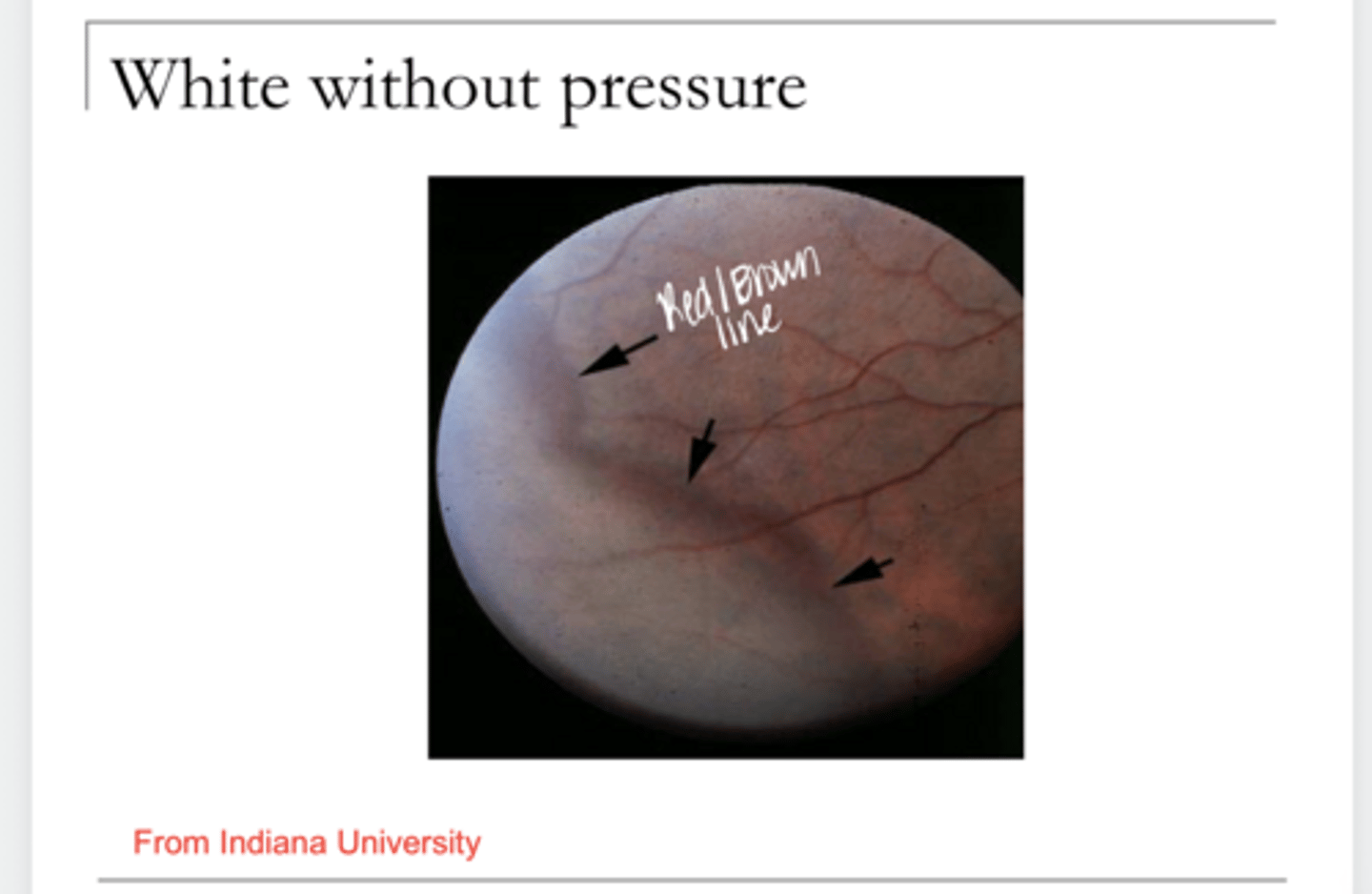
White Without Pressure Pic
White Without Pressure Pic
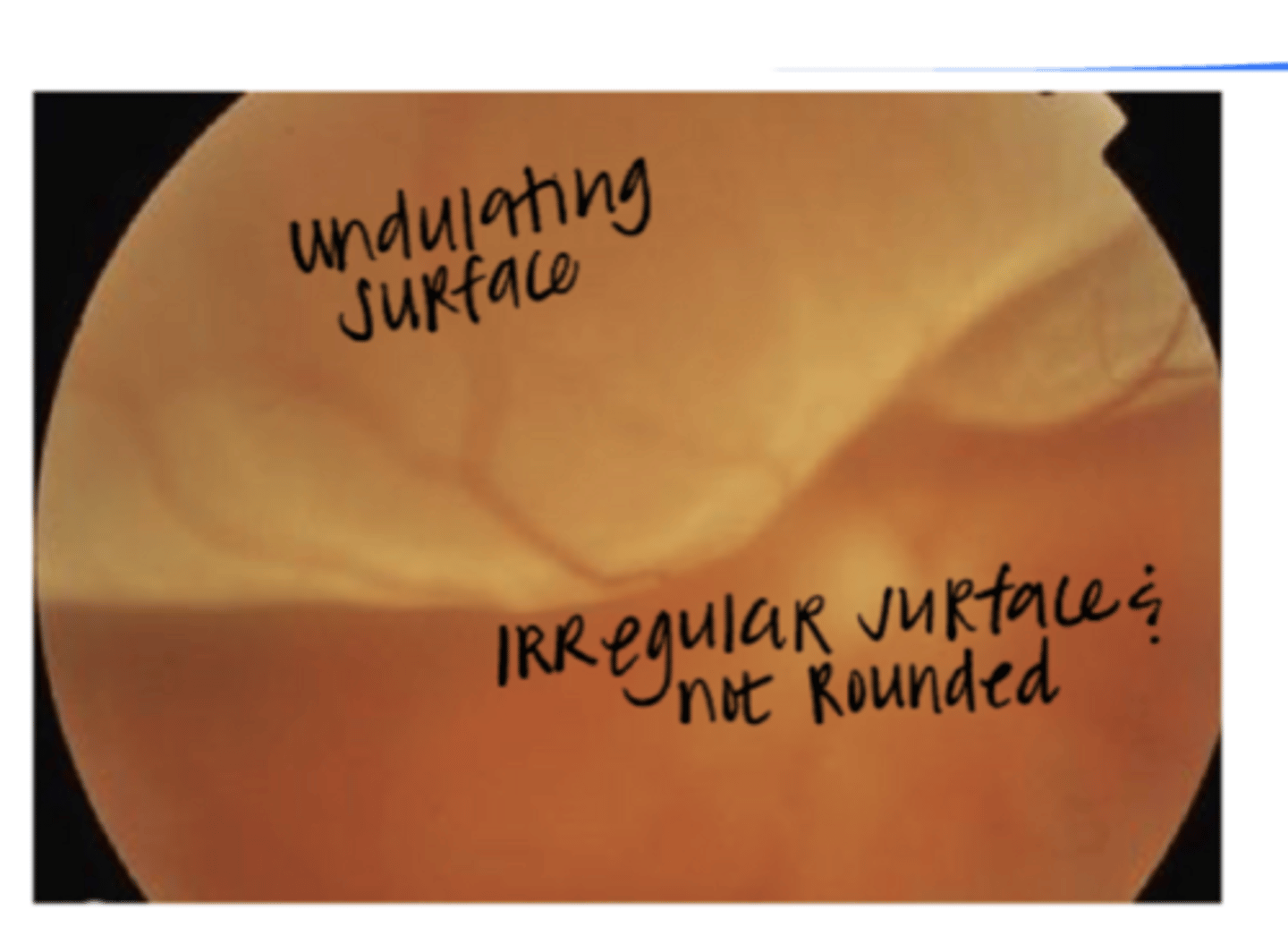
Retinal Detachment Pic
Retinal Detachment Pic
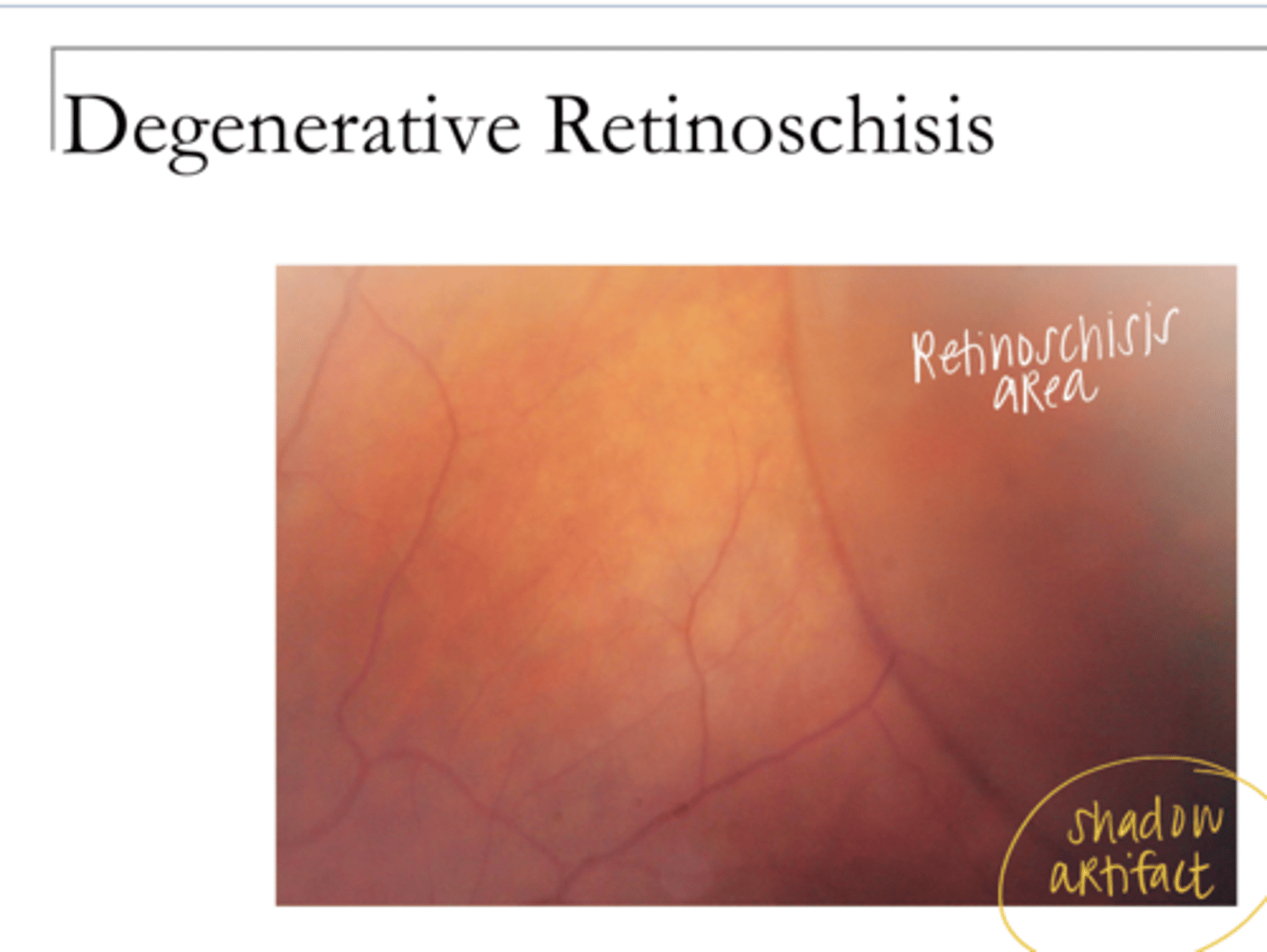
Retinoschisis Pic
Retinoschisis Pic
all lead to blurry areas
Why are Peripheral Cystoid/WWOP/RD/Retinoschisis differentials for eachother?
Refer if outer layer hole, if there is a high water mark present, retinal detachment present, or if there is progression towards the posterior pole
What is the management plan for a retinoschisis?
-Refer if new symptoms
-Refer if there is a retinal tear within the lattice or on the border
-Refer id there is a retinal hole at the border of the degeneration
What is the management of lattice/snailtrack degeneration?
abnormal
Arterial pulsation is (normal/abnormal)
normal
Venous pulsation is (normal/abnormal)
because the venous perfusion pressure is similar to the intraocular pressure
Why does venous pulsation occur?
arteriosclerosis with occlusion of vein by an artery at AV crossing; or by a thombus
What is the etiology of BRVO?
-need systemic vascular workup
-BP check
What is the management plan for a patient with a BRVO?
Hypertension
___ is the most common association with BRVO
partial blockage with fewer hemes and cotton wool spots
What is non-ischemic BRVO?
nearly complete or complete blockage with more hemes and cotton wool spots
What is an ischemic BRVO?
true
True or False:
New venous occlusions usually have significant hemorrhage
-vascular sheathing
-tortuosity
-retinal collaterals
-hard exudates
What are the retinal signs post-BRVO?
-macular edema
-retinal neovasc
What are the major ocular concerns post-BRVO?
Anti-VEGF intravitreal injections may help with macular edema in BRVO; established anti-VEGF meds as the first line treatment for macular edema secondary to BRVO
What was the findings of the BRAVO, HORIZON, RETAIN Studies?
thrombus typically
What is the etiology of a CRVO?
-systemic vascular work up
-BP check
What is the management plan for patients with CRVO?
Hypertension
______ is the most common systemic association with CRVO
partial blockage with fewer hemes and cotton wool spots
What is non-ischemic CRVO?
nearly complete or complete blockage with more hemes and cotton wool spots
What is ischemic CRVO?
-vascular sheathing
-tortuosity
-retinal/optic nerve collaterals
-hard exudates
What are the retinal signs post-CRVO?
-macular edema
-Retinal neovasc
-iris neovasc
-neovascular glaucoma
What are the major concerns post-CRVO?
-grid laser WAS NOT helpful for macular edema
-Wait until NVI develops to perform PRP in non-ischemic CRVO
-Eyes with extensive hemes are often ischemic
What were the findings in the central vein occlusion study (CVOS)?
Anti-VEGF intravitreal injections may help with macular edema in CRVO; established anti-VEGF meds as the first line treatment for macular edema in CRVO
What were the findings of the CRUISE, HORIZON, RETAIN studies regarding CRVO?
-branch
-central
What are the forms of arterial occlusions?
embolus
What is the etiology of arterial occlusions?
retina appears white (giant cotton wool spots)
What is the appearance of the retina with an arterial occlusion?
painless loss of vision
What is the common symptom of arterial occlusion?
Yes
Is an arterial occlusion an ocular emergency?
hypertension
What is the #1 cause of venous occlusion and macroaneurysm?
mild to early moderate
Hypertensive retinopathy is usually ____ to _____
No
Do venous occlusions usually happen with mild to early moderate hypertensive retinopathy?
-generalized narrowing of the arteries
-AV crossing changes
-widening of the arterial light reflex (sheathing)
-tortuosity
What are the common retinal changes with mild hypertensive retinopathy?
-everything in the mild category can occur
- vascular leakage
- vascular occlusion
-microaneurysms (like diabetes)
What are the common retinal changes with moderate hypertensive retinopathy?
-may show everything in mild & moderate categories
-optic nerve head edema
What are the common retinal changes with malignant hypertensive retinopathy?
By controlling blood pressure w/ diet and exercise and/or medications
How is hypertensive retinopathy controlled?
No -- the mild changes will probably remain but will progress more slowly
Will all hypertensive retinal changes resolve with diet and exercise change to control BP?
Yes
Will moderate/malignant retinal changes d/t hypertension resolve with diet and exercise change to control BP?
Hypertension
What is the most common systemic association with vascular occlusion (BRVO/CRVO) and macroanuerysm?
No
Is arteriosclerotic retinopathy associated with any systemic disease?
age
Arteriosclerotic retinopathy is ____ related
mild changes of hypertensive retinopathy
What does arteriosclerotic retinopathy resemble?
vascular leakage or vascular occlusion
What does arteriosclerotic retinopathy NOT include?
exogenous insulin
Type 1 diabetics must get _____
endogenous insulin is made, but it does not work properly
Describe Type 2 diabetes
Type 2
Metabolic syndrome describes most (Type 1/Type 2) diabetics
Obesity with genetic insulin resistance will lead to hypertension, Type 2 diabetes, Lipid abnormalities (lower HDL, higher triglycerides), increased uric acid
Metabolic syndrome description
All of the above disorders (hypertension, Type 2 diabetes, Lipid abnormalities (lower HDL, higher triglycerides), increased uric acid) WILL occur together
What is the FOGT Conception that deals with Metabolic syndrome?
IF these disorders (hypertension, Type 2 diabetes, Lipid abnormalities (lower HDL, higher triglycerides), increased uric acid) occur together, then a patient is at risk for vascular disorders such as hypertension and diabetes
What is the NIH Conception that deals with Metabolic syndrome?
polyuria, polyphagia, polydipsia
Classic triad of symptoms in diabetes?
Yes -- transient (days) or more long-lasting changes in refractive error are possible
Can refractive error change d/t diabetes?
duration and control
What are the major determinants of diabetic retinopathy progression?
does not contain
Nonproliferative diabetic retinopathy (NPDR) (contains/does not contain) neovascularization
Proliferative = neovasc present (NVE, NVD, NVI)
What is the difference of PROLIFERATIVE diabetic retinopathy from NPDR?
microaneurysms
Usually ____ are the first retinal changes in NPDR
Yes -- hemes and hard exudate are common
Is vascular leakage commonly seen with NPDR?
1) Retinal thickening within 1/3 DD of the fovea
2) Hard exudate within 1/2DD of the fovea (with associated retinal thickening)
3) Retinal thickening at least 1DD within 1DD of the fovea
What are the 3 definitions of Clinically Significant Macular Edema from the ETDRS Study?