GI
1/761
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
762 Terms
s/sx of malnutrition
body habitus wasting (adipose tissue, somatic protein, or both)
low bmi
concomitant inflammatory disorders can be present
poorly healing wounds
decreased grip strength
actual body weight <90% of ideal body weight
lab changes that show malnutrition
low albumin, prealbumin and transferrin, elevated CRP
what risk calculations are used for malnutrition and what is considered high risk
NUTRIC score >5+
NRS-2002 score >3+
enteral nutrition
delivered into the gi tract
parenteral nutrition
delivered directly into the bloodstream
enteral/gi access routes
nasogastric, nasojejunal, gastrostomy/percutaneous endoscopic gastrostomy, jejunostomy/percutaneous endoscopic jujenostomy
which enteral access routes are good for short term use
nasogastric and nasojejunal
which enteral access routes are good for long term use
gastrostomy/percutaneous endoscopic gastrostomy, jejunostomy/percutaneous endoscopic jujenostomy
when is post-pyloric placement useful
high aspiration risk, pancreatitis, gastroparesis
risk factors for feeding tube clogging
suboptimal tube care or med administration
small bore feeding tubes
frequent aspiration of gastric residuals
prevention of feeding tube clogging
flush w/ 20-30 ml warm water, q4h during continuous feeding and before + after feeds/meds
medications tips for feeding tube clogging
use liquid formulations when possible, avoid mixing meds w/ enteral nutrition, do NOT flush w/ juice or carbonated bevs
management of feeding tube clogging
use pancreatic enzymes + sodium bicarb in ~5ml water, allow to dwell ~15 mins then flush
which drugs have dosage forms that are altered by crushing and what should you do to prevent this
drugs that are delayed release, extended release or enteric coated →
change the drug to an immediate release if possible!
which drugs are inactivated by exposure to cations w/in tube feedings and what should you do to prevent this
tetracyclines, fluoroquinolones (cipro, levo) → hold tube feeding for 1h before/after admin OR admin it IV
which drugs bind to proteins contained w/in tube feedings and what should you do to prevent this
phenytoin, warfarin → hold tube feedings 1-2h before/after admin OR increase dose OR admin IV
when should parenteral nutrition be used over enteral nutrition
if pts gut cannot be used, is inadequate, cannot be tolerated
which type of nutrition maintains gut integrity
enteral nutrition
which type of nutrition has a higher infection risk? (line related)
parenteral nutrition
which type of nutrition has a higher risk of aspiration or emesis!
enteral nutrition
which type or nutrition cost more and is used in longer hospital stays
parenteral nutrition
when is parenteral nutrition indicated
if there is a c/i to enteral nutrition
conditions where EN is not safe (requires bowel rest)
inability to meet nutritional needs through the gi tract
severe metabolic or clinical instability
contraindications to EN
failed EN trial or intolerance
nonfunctional / inaccessible gi tract (paralytic ileus, mesenteric ischemia, small bowel obstruction, high-output fistula)
conditions where EN is unsafe
ischemic bowel, gi perforation, severe gi bleeding
what constitutes an inability to meet a pts nutritional needs via gi tract
inadequate oral/enteral intake for >7d
preexisting malnutrition w/ anticipated prolonged NPO status
what constitutes severe metabolic or clinical instability
severe fluid or electrolyte disturbances
severe hyperglycemia or hyperosmolar state
encephalopathy limiting safe feeding
significant multiorgan system failure
if a pts nutritional risk is low, when should you initiate PN
after 7 days
if a pts nutritional risk is high or they are clearly malnourished, when should you initiate PN
as soon as posisble!
peripheral parenteral access routes
midline catheter
antecubital peripheral line
forearm peripheral line
hand peripheral line
central parenteral access routes
central venous catheter (CVC)
port a cath
peripheral inserted central catheter (PICC)
tunneled line
which type of parenteral nutrition is given through a central line/route
total parenteral nutrition (TPN)
which type of parenteral nutrition is given through a peripheral route
peripheral parenteral nutrition (PPN)
max osmolarity for peripheral access route
900 mOsm/L
max osmolarity for central access route
1300-1800 mOsm/L
which parenteral access route has a higher risk of infection
central! specifically central line associated bloodstream infection (CLABSI)
which parenteral access route is used for short term use
peripheral!
complications of peripheral lines
phlebitis, infiltration
complications of central lines
CLABSI, thrombosis, pneumothorax (placement-related)
3 ways to calculate calorie requirement
indirect calorimetry: based on o2 consumption / co2 production, most accurate but expensive
estimated energy requirement based on weight
total energy expenditure (TEE): specific to pts clinical status + body habitus, correction for stress!
calories per kg
25-35kcal/kg
maintenance: 20-25
moderate stress: 25-30
severe stress: >35
stress factor for pts confined to bed
1.2
stress factor for pts w/ sepsis
1.3
stress factor for pts w/ severe trauma
1.4
stress factor for pts w/ severe burns
2.0
ideal body weight equations
males: 50kg + 2.3kg (every in over 5 ft)
females: 45.5kg + 2.3 kg ( every in over 5 ft)
adjusted body weight equation
IBW + 0.4 (ABW-IBW)
when should ABW (actual body weight) be used
if bmi <30
or if it is less than IBW (to help maintain the current nutrition status)
when should adjBW be used
if bmi >30
protein requirement in general
1-2 g/kg
protein requirement for maintenance
0.8-1.2 g/kg
protein requirement for moderate stress
1.2-1.5 g/kg
protein requirement for severe stress
1.5-2 g/kg
protein requirement for renal insufficiency not on dialysis
0.6-0.8 g/kg
protein requirement for hemodialysis
1.2-1.3 g/kg
protein requirement for CRRT (continuous renal replacement therapy)
1.5-2.5 g/kg
protein requirement for overt encephalopathy
0.5-0.7 g/kg
fluid requirement
generally ~ 35 ml/kg
1000ml for first 10 kg, 500 ml for next 10 kg, and 20 ml/kg thereafter
maintenance: 1500ml + 20ml(pt wt in kg -20)
components of parenteral nutrition
macro: dextrose, amino acids, lipids
micro: electrolytes, vitamins, trace elements
use sterile water as vehicle!
additives (not required): insulin
calories of dextrose
3.4 kcal/g
max infusion rate of dextrose
5 mg/kg/min (25 kcal/kg/day)
max concentration of dextrose through a peripheral line (PPN)
dextrose 10%
max concentration of dextrose through a central line (TPN)
dextrose 25%
calories of amino acids
4 kcal/g
max concentration of AA through a peripheral line
2-5-5%
max concentration of AA through a central line
5-10%
calories of lipids
10 kcal/g
when are lipids contraindicated
pts w/ severe egg, soybean, and/or peanut allergy
ILE formulations
10% (1.1kcal/ml): only for premixed produces (ex: propofol)
20% (2 kcal/ml): used for direct iv lipid admin
30% (2.9-3 kcal/ml): used for compounding 3 in 1 mixture
intralipid
100% soybean!, higher omega 6 content and no omega 3 content, higher hepatotox risk
used in short term PN (<5-7d), institutional formulary limitation, cost constraints
SMOFlipid
contains soybean, medium chain TG, olive oil, fish oil
lower omega 6 content, and has omega 3 (fish oil)
lower hepatotox risk
used for long-term PN (wks - mon), in ICU pts requiring prolonged nutrition, pts at risk of liver dysfxn/cholestasis, hyperinflammatory states, critically ill
which electrolytes should be avoided
sodium bicarb, sodium lactate, calcium chloride
what does the calcium phosphate solubility curve show
the max allowable combos of calcium + phosphate that can safely remain dissolved in a 2 in 1 PN solution @ different AA concentrations
what is the standard dosing of multivitamins (ADEK + B1,2,6,12 + C + folic acid)
10 ml/bag
what is the standard dosing of trace elements (zn, cu, cr, mn, se)
1 ml/bag
insulin in TPN
use sliding scale! q6h
goal blood glucose while on TPN: 140-180 mg/dl
absorbed to plastic tubing + PVC (up to 50% loss)
add 1/2-1/3 of previous 24h ISS requirement
2-in-1 PN formulation
dextrose + AA only, lipids infused separately
max hang time: 24h
3-in-1 / total nutrient admixtures
dextrose, AA, lipids
decreases solubility of calcium + phosphate (increase risk for precipitation)
max hang time: 24h
multichamber bags
various formulations
2 in 1 or 3 in 1
convenient + cost effective`
max hang time for IV lipid emulsions (ILE)
12h
continuous TPN
infused continuously over 24h
provides stable, constant nutrient delivery
common in hospitalized pts
cyclic TPN
infused over 12-18h w/ daily “off” period
stepwise increase, steady infusion, then taper down
indicated for TPN associated cholestatic liver disease prevention, long term home TPN, improved pt qol
what additional info is important before initiating a TPN
max dextrose conc based on line status
osm limits based on line status
plans for change in line status
PMH/problem list
DM, compromised resp fxn: low dextrose conc
liver disease w/ ascites, CHF, HTN: minimize na
pancreatitis: zero/low fat conc
renal impairment: minimize k, mg, phos
fluid restriction: concentrate formula, increase fat conc
diet (full nutrition support vs supportive)
current labs
0.22 micron filters
removes pathogenic microorganisms: staph epi, e.coli, candida albicans
1.22 micron filters
used for ILE containing PN
refeeding syndrome
neg consequences of metabolic + physiological shifts of fluid, electrolytes, vitamins, + minerals d/t aggressive nutrition repletion
driven mainly by insulin release after carb reintroduction (insulin increase → decrease phos, k, mg)
can occur during first 2-5 d after start of nutrition support
risk factors for refeeding syndrome
anorexia nervosa, prolonged periods of no nutrition, bmi <16
management for refeeding syndrome
initiate dextrose btwn 100-150g, titrate to nutrition goal every 1-2d
replace electrolytes according to protocols
if sudden electrolyte drop, decrease dextrose by 50%
metabolic complications
hypoglycemia: if infusion w/ >10% dextrose is stopped abruptly, must taper off + check blood sugar 1h after end of infusion
excess co2 production: d/t overfeeding w/ glucose cals, glucose oxidation produces more co2 than fat oxidation
TPN associated cholestatic liver disease: associated w/ prolonged, continuous feeding, increase in alkaline phosphatase + other liver enzymes as early as 7-10d following initiation of TPN
essential fatty acid deficiency: EFAs are substrates for other things (maintains integrity of skin + cell membranes, components of brain + retina, synthesis of prostaglandins + leukotrienes)
risk factors of TPN associated cholestatic liver disease
infxn, ongoing inflammatory process, alcoholism, obesity
management for TPN associated cholestatic liver disease
rule out other causes, decrease glucose intake (<25kcal/kg/day), cycle TPN
s/sx of EFA deficiency
dry, scaly rash
hair loss, hair depigmentation
poor wound healing
growth restriction in children
increased susceptibility to infxn
management of EFA deficiency
minimum requirement of lipid: 1g/kg/wk
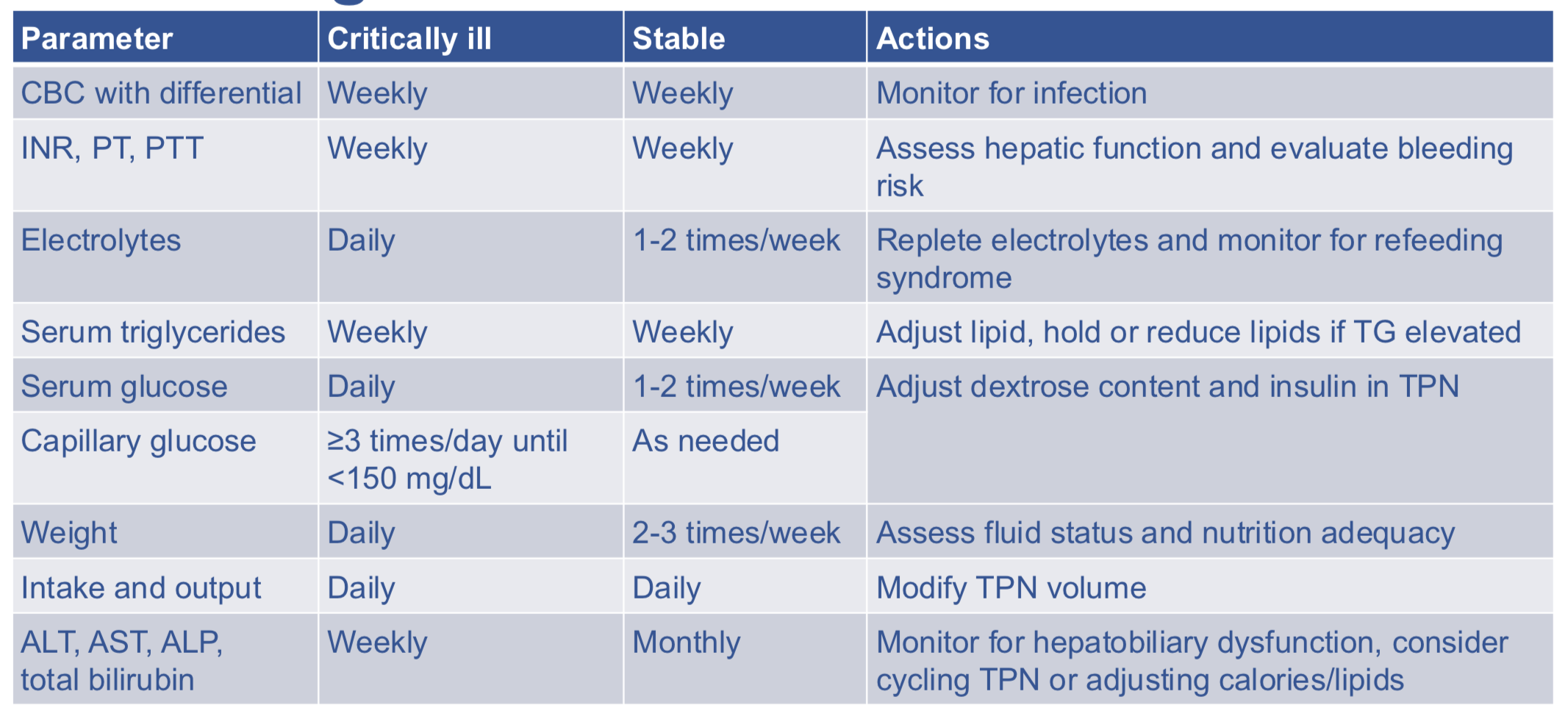
monitoring parameters
endocrine hormone
insulin → regulates blood glucose
exocrine hormone
→ amylase, lipase, trypsin, others → secreted into duodenum to facilitate organic chemical breakdown
exocrine hormone secretion pathway
pancreatic acini → pancreatic duct → common bile duct → ampulla of vater → duodenum
need all parts of pathway to fxn normally to maintain normal physiology
pathophys
inability to excrete pancreatic exocrine enzymes into the duodenum → disrupted physiology
digestive enzyme buildup may lead to pancreatic inflammation + pancreatic cell death
can cause detectable levels of pancreatic enzymes in serum
etiology
blockage in pancreatic drainage system; may or may not have clear cause
B: biliary
A: alc
D: drugs
S: scorpion sting
H: hypertriglyeridemia
I: idiopathic
T: trauma/tumor
which drugs cause hypertriglyceridemia
estrogens, hctz
which drugs cause spasm of the sphincter of oddi
opioids