3 - fixational eye movements
1/74
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
75 Terms
What are fixational eye movements?
miniature or micro-eye movements that happen constantly as we fixate a target
What are the types of fixational eye movements?
1. tremor
2. drift
3. microsaccades
What is the frequency and amplitude of tremor fixational eye movements?
30-100 Hz → high frequency
5-30 seconds or arc → very small
What are tremor fixational eye movements considered?
noise
What are drift fixational eye movements considered?
mostly noise, but may be error-correcting
what is the velocity and amplitude of drift fixational eye movements?
1-8 min of arc/sec → very slow
2-5 min of arc
What is the amplitude of and how often are micro-saccadic fixational eye movements?
5 min of arc → range from 1-25', rarely 10'
occur 1-2 per second
What are microsaccadic eye movements considered?
error-correcting
Which eye movements don't follow Herrings law?
fixational eye movements → esp drift and tremor
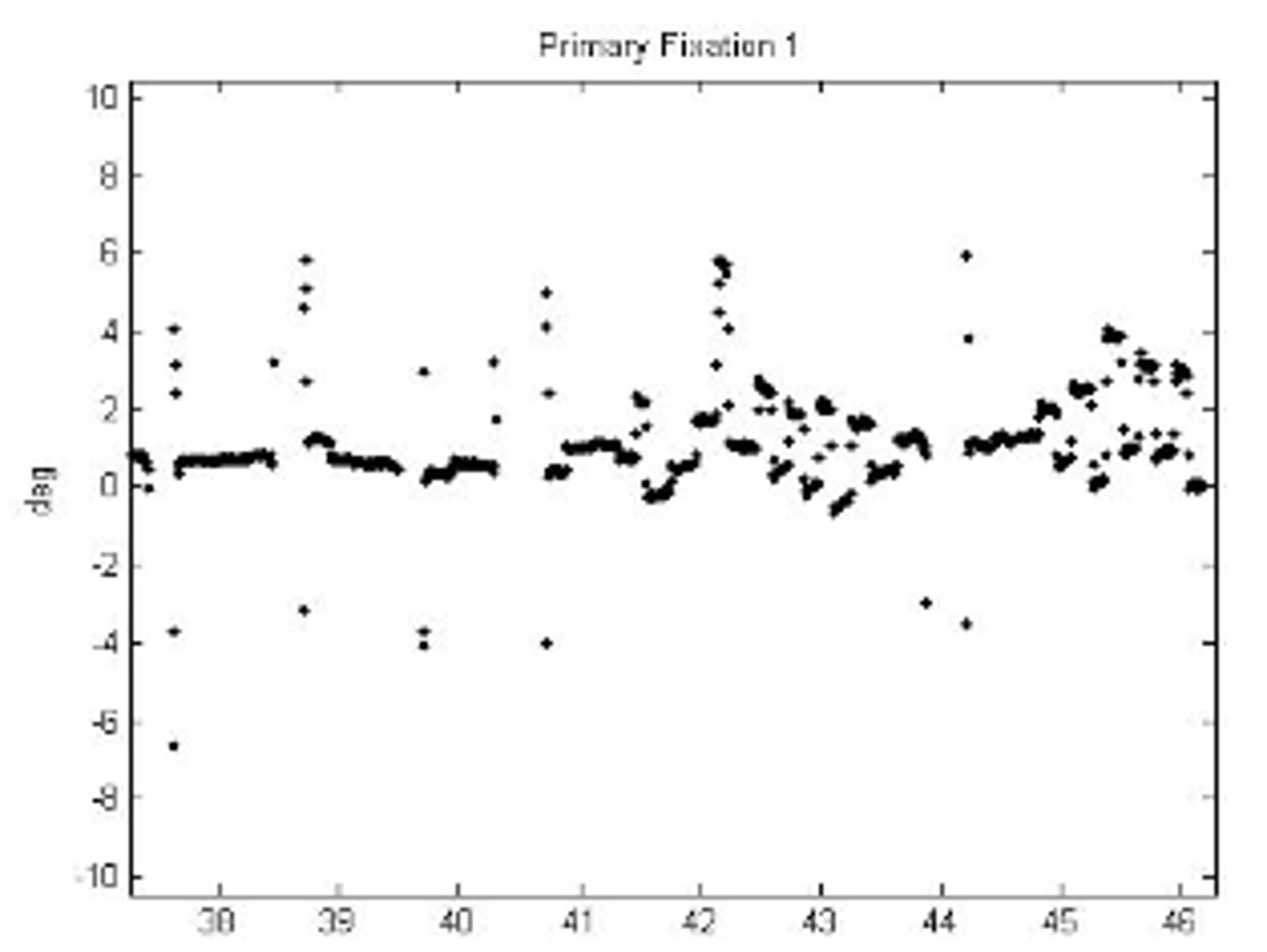
How does fixation change over time?
the longer the fixation time → the larger area of fixation
How does fixation vary?
with directional bias
i.e. fixation tends to vary along one direction of gaze
Why do we have fixational eye movements? Which fixational eye movement is most responsible for this?
stabilize the retinal image aka keeps the image on our retina with motion of the eye → mostly d/t microsaccades
What is the Troxler effect?
fading of stabilized retinal images with careful fixation
Which fixational eye movements do not prevent the Troxler effect?
tremor
drift
Which fixational eye movement does prevent the Troxler effect?
microsaccades
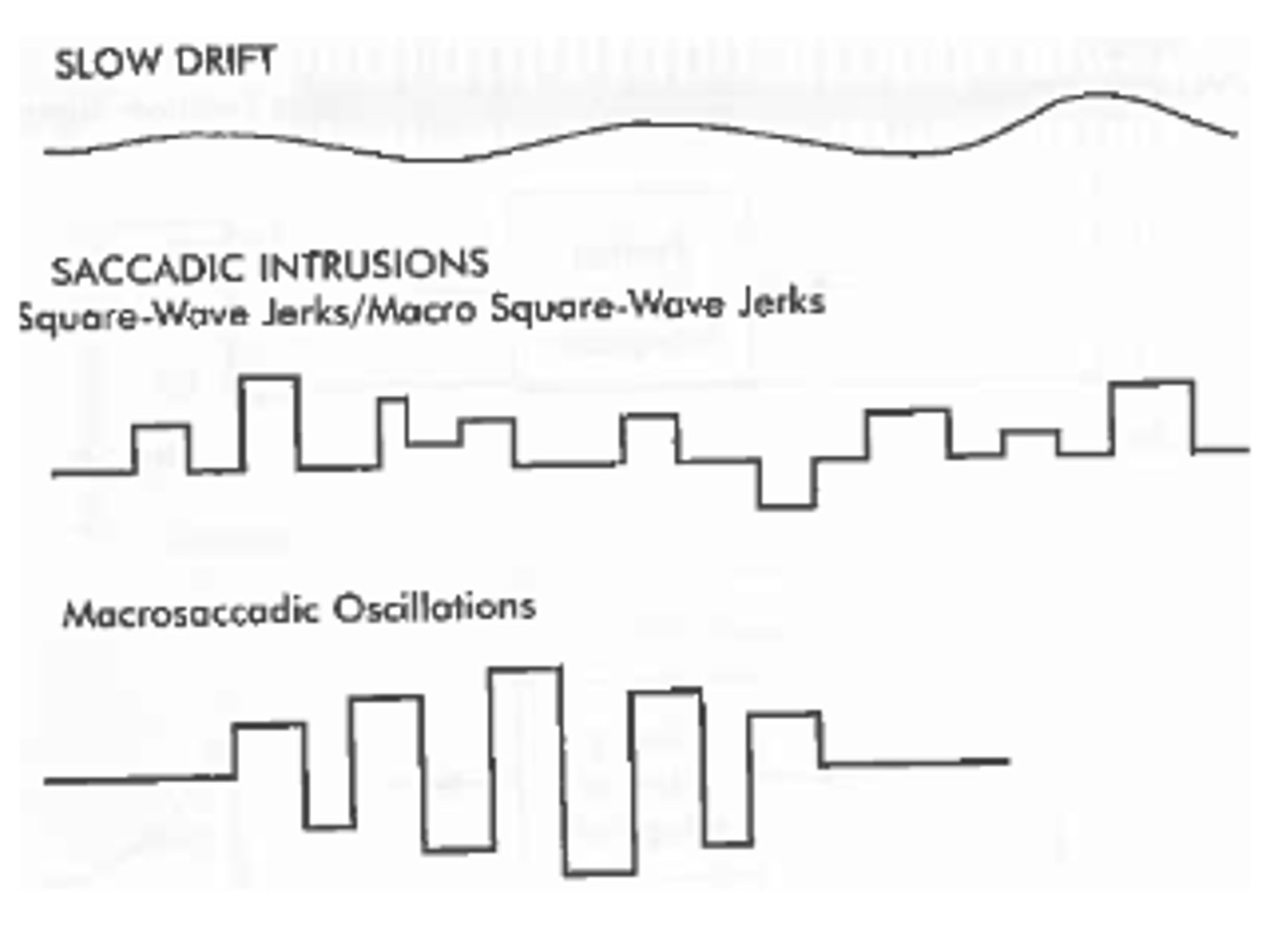
What are the 3 categories of abnormal fixation?
1. slow drift
2. saccadic intrusions
3. nystagmus
What are causes of acquired fixational abnormalities?
1. stroke
2. tumor
3. aneurysm
4. infection
5. MS → esp if lesion in brainstem, cerebellum, vestibular system
What other condition is slow drift common in?
amblyopia
Is slow drift a monocular or binocular phenomenon?
monocular
What is the amplitude of slow drift?
≤1 degree
What is the velocity of slow drift?
~2 deg/sec
faster than "normal" drift
What is slow drift corrected by?
saccades
What are the 3 types of saccadic intrusions?
1. square-wave jerk
2. macro square-wave jerk
3. macrosaccadic oscillation
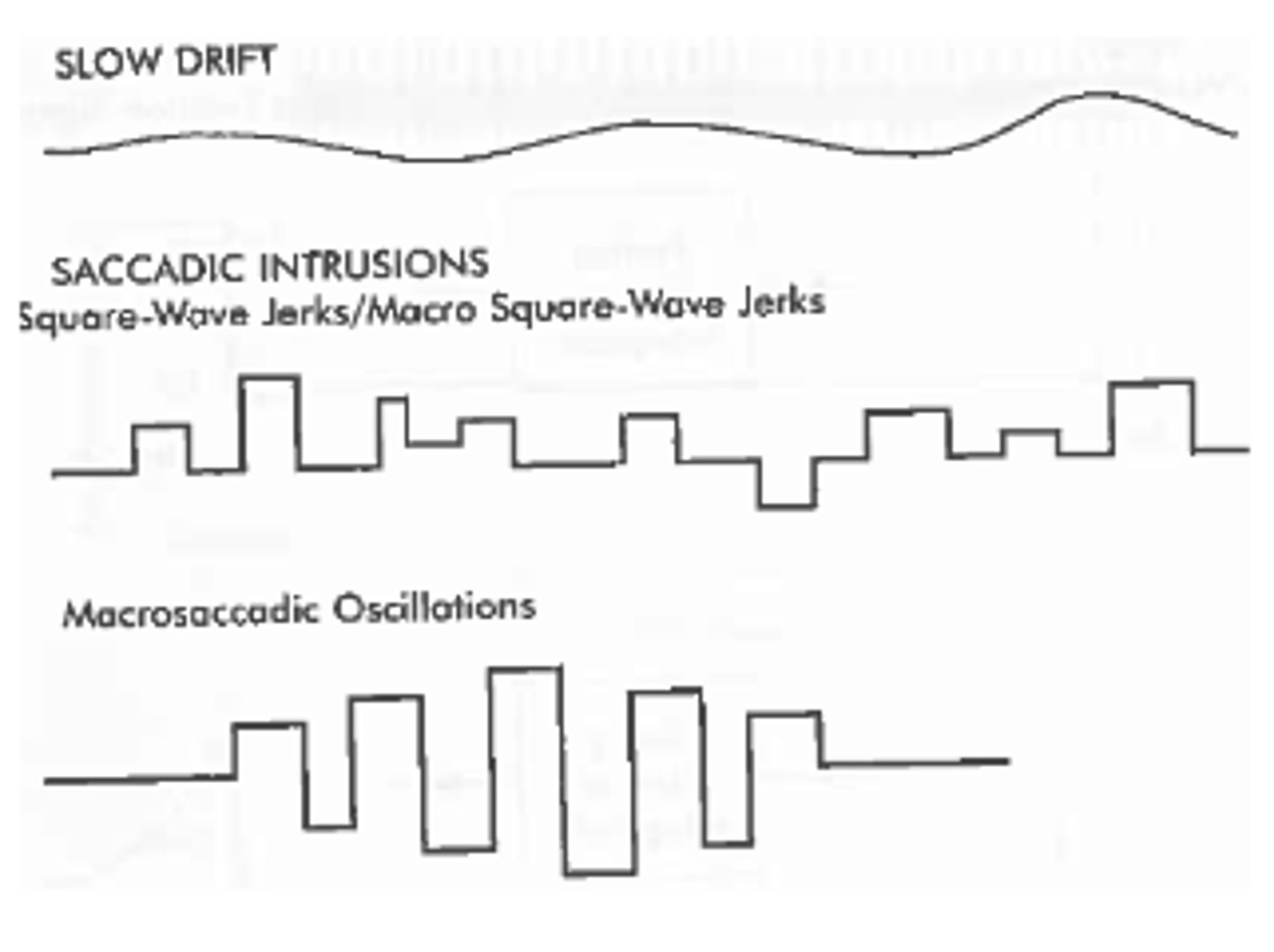
What are square-wave jerks/macro square wave jerks?
saccade away from fixation followed by a corrective saccade
What is the amplitude of square-wave jerk?
<5 degrees
typically 0.5 - 5
What are the etiologies of square-wave jerks?
1. cerebellar disease
2. MS
nothing → occurs in 50% of normals
Which saccadic intrusion does not occur in normals?
macro square-wave jerk
etiology
1. typically MS
2. cerebellar disease
What is the amplitude of a macro square-wave jerk?
>5 degrees
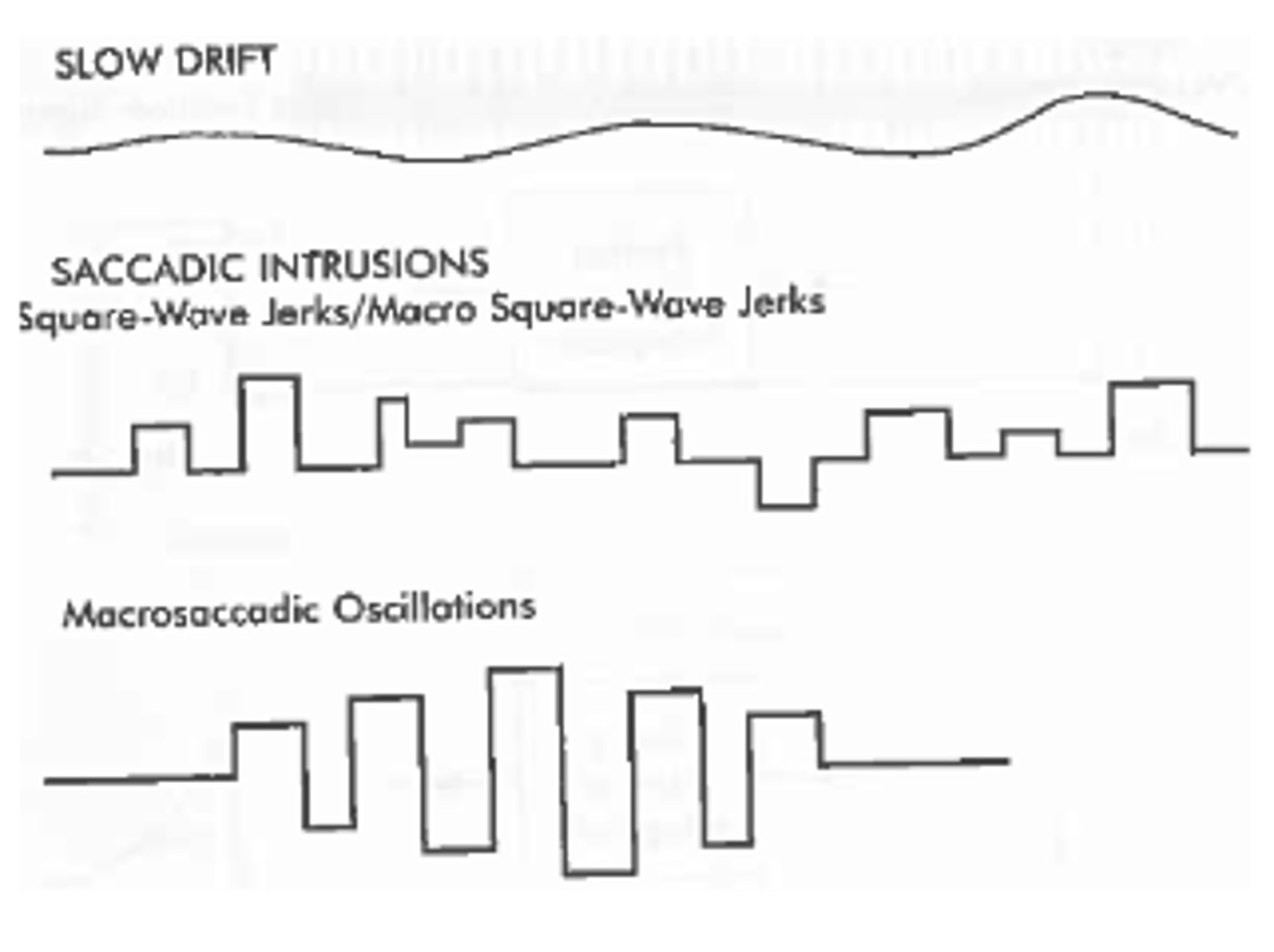
What is a macrosaccadic oscillation?
sequence of increasing and decreasing amplitudes to either side of the fixation points
corrective saccades over correct
What is nystagmus?
rhythmic oscillations of the eye
What are the two categories of nystagmus?
pendular or jerk
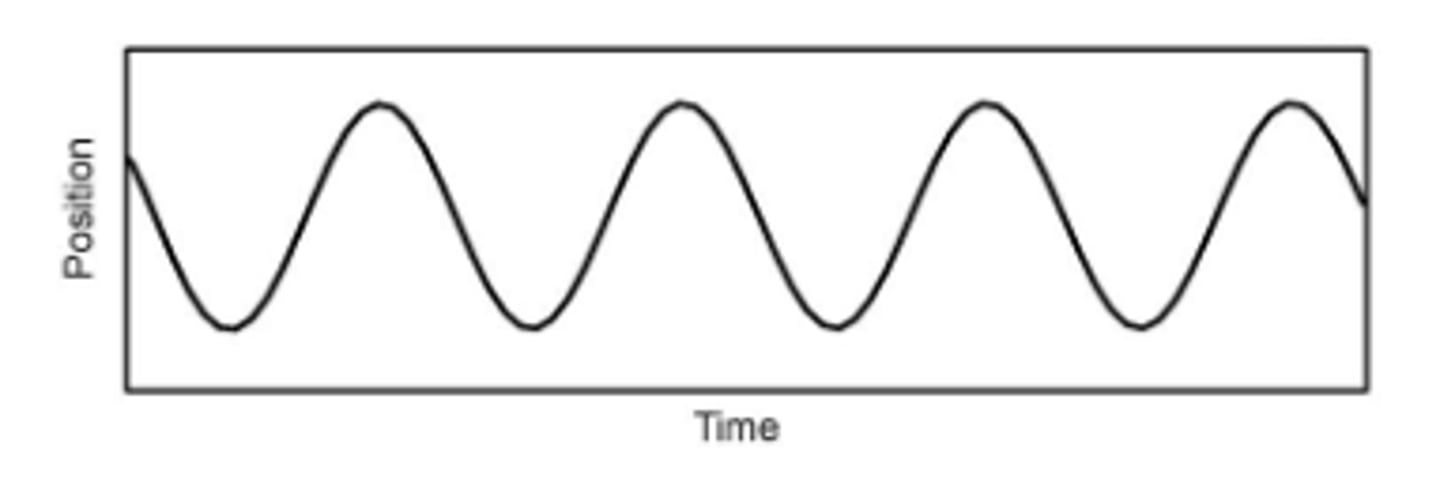
What is pendular nystagmus?
nystagmus that follows a sinusoidal motion
What is jerk nystagmus?
slow phase away from fixation with a fast phase back to fixation
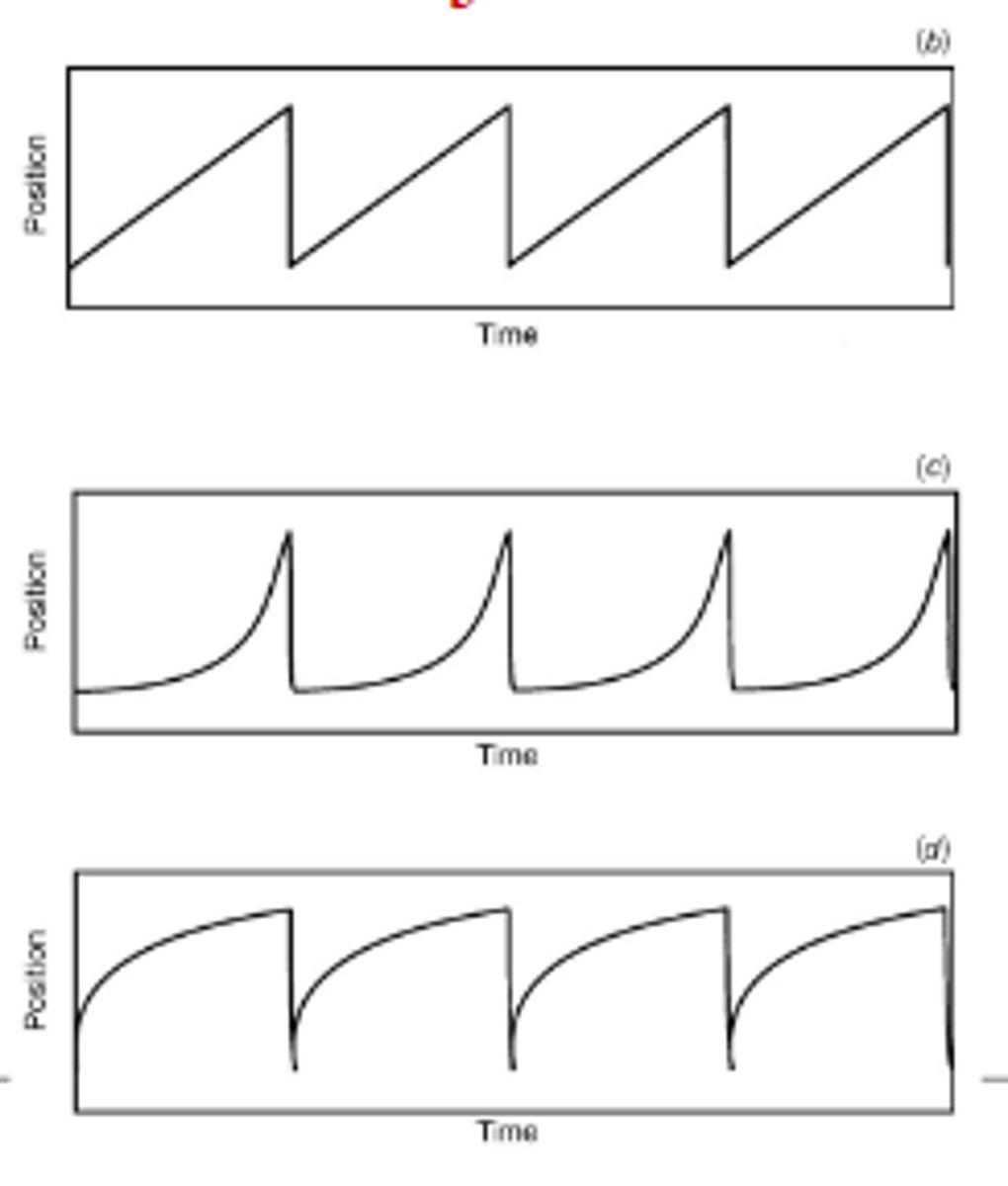
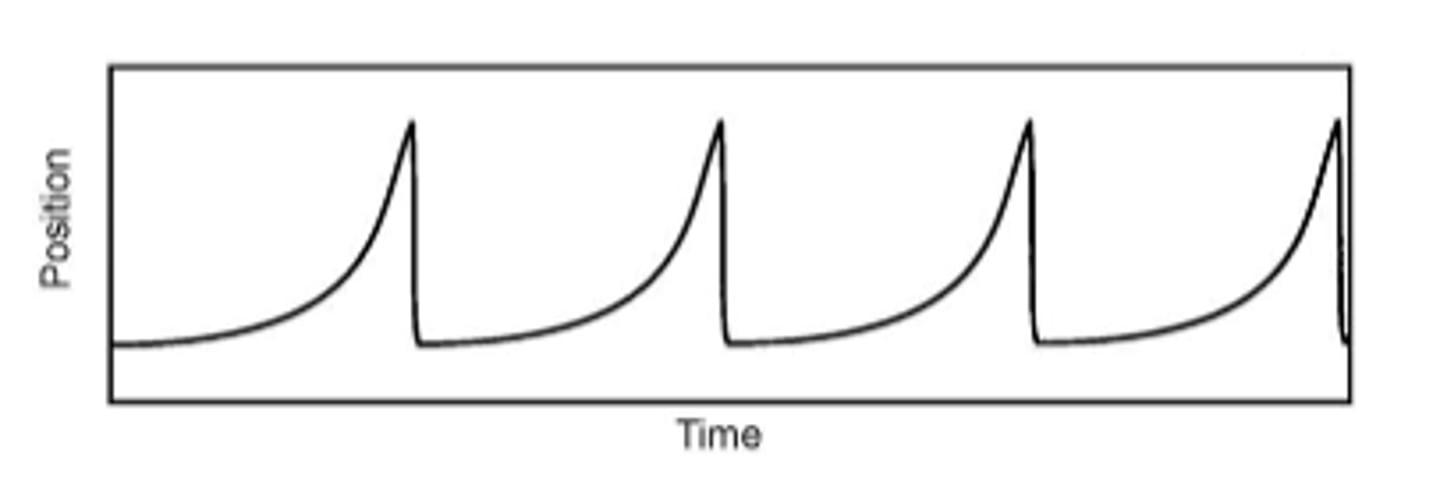
What are the waveform types of jerk nystagmus?
1. constant velocity slow phase/saw-tooth
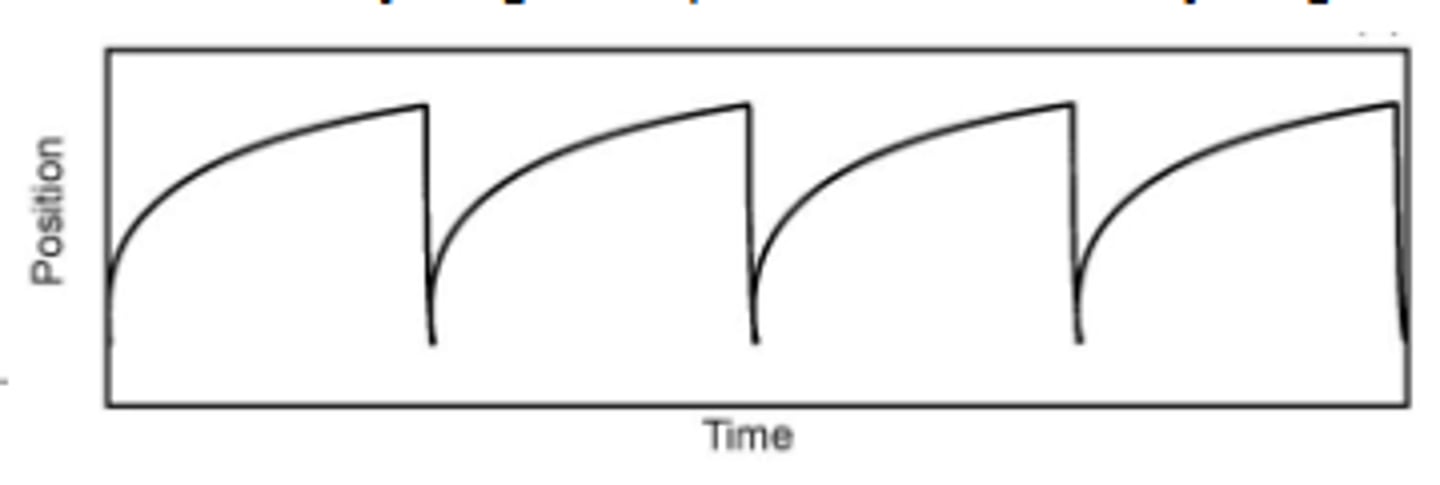
2. accelerating slow phase
3. decelerating slow phase
wavefront names are based off of slow phase
How do you name a jerk nystagmus?
based on direction of the fast phase
What are the causes of constant velocity slow phase/saw-tooth nystagmus?
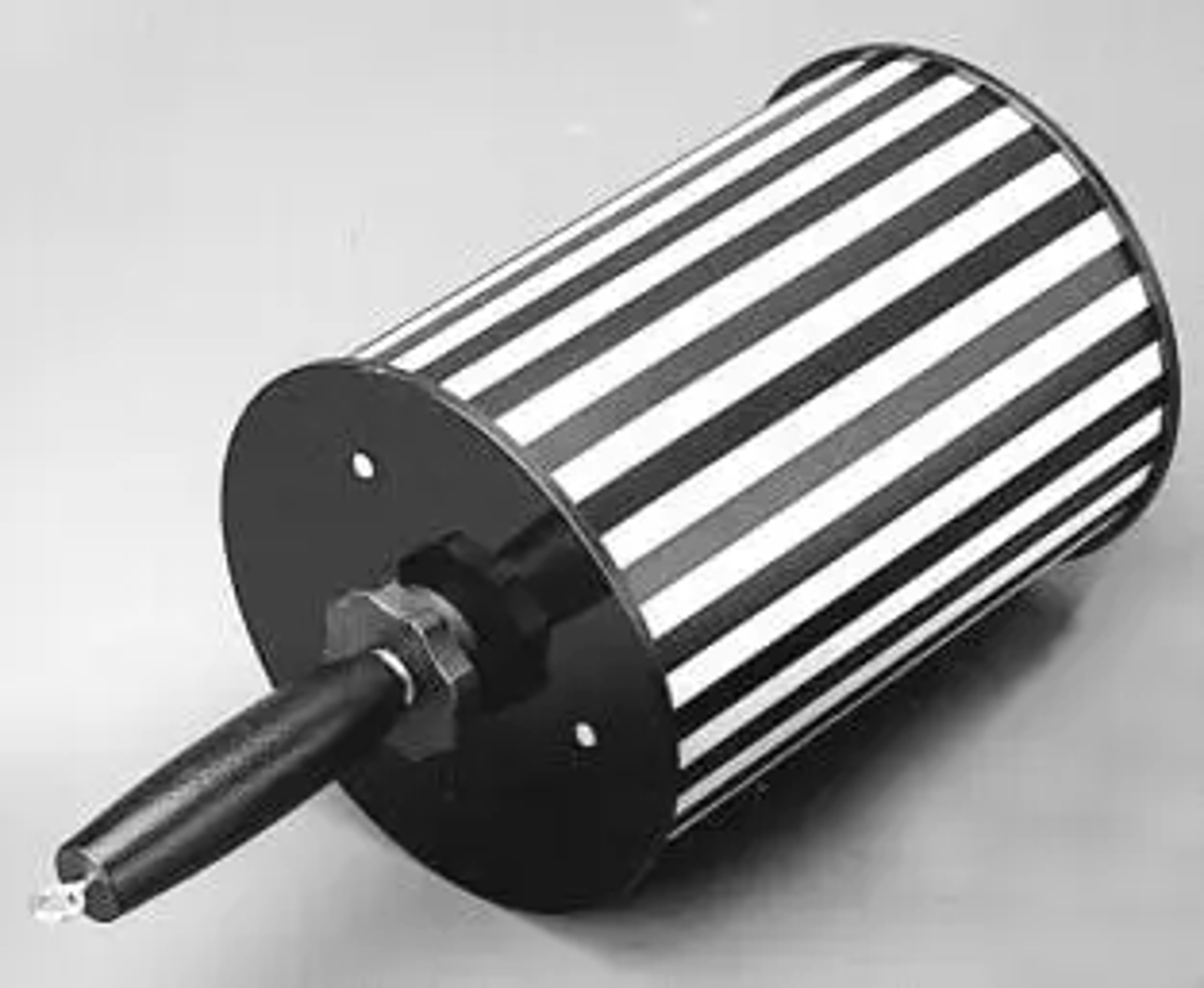
1. physiologic → after spinning or caloric (blowing in ear) testing
2. acquired
3. Optokinetic Nystagmus (image)
What is the cause of accelerating slow phase nystagmus?
congenital
What are the types of decelerating slow phase nystagmus?
1. gaze-evoked nystagmus
2. latent nystagmus
What is gaze evoked-nystagmus?
when looking in extreme gaze angles → the eye will drift toward primary gaze then saccade back to fixation
What are the causes of gaze-evoked nystagmus?
1. drug/alcohol
2. acquired - if at less extreme gaze angles
What is latent nystagmus?
decelerating slow phase jerk nystagmus that shows up when monocular
What is usually the cause of latent nystagmus?
congenital
What is latent nystagmus often associated with?
strabismus (50% of patients)
What is the direction of the fast phase in latent nystagmus?
fast phase in same direction as viewing eye
ex: OD viewing → right fast phase
What other ocular condition is highly correlated with congenital nystagmus?
strabismus
When does congenital nystagmus usually appear?
within first few months of life
What is the null position?
direction of gaze where intensity of congenital nystagmus is minimized/least and VA is optimal
what does intensity equal?
= amplitude x frequency
What is periodic alternating nystagmus (PAN)?
congenital nystagmus where null position shifts around over several minutes or longer
What are the characteristics of congenital nystagmus?
1. has a null position → turn head opposite to null position
2. decreases with convergence
3. foveation periods
4. tend to not have oscillopsia - world will not appear to be spinning
5. typically only horizontal
What is a foveation period?
period of time in congenital nystagmus where gaze is close to putting target on fovea → patient have good visual performance at that area
What are the main differences in signs between congenital and acquired nystagmus?
1. null point (congenital)
2. decreased on convergence (congenital)
3. direction (acquired is any, congenital is horizontal only)
4. oscillopsia (acquired)
5. foveation periods (congenital)
6. abnormal head posture (congenital)
What is the treatment for congenital nystagmus?
1. yolked prism to move images to null point
2. BO prism to increase convergence demand
3. surgery to move eyes to null point → 2 or 4 muscle procedure
what is tenotomy surgery/combined procedure?
cut off all horizontal recti and attach in same position or do tenotomy but change position of muscles like in 2 muscle procedure
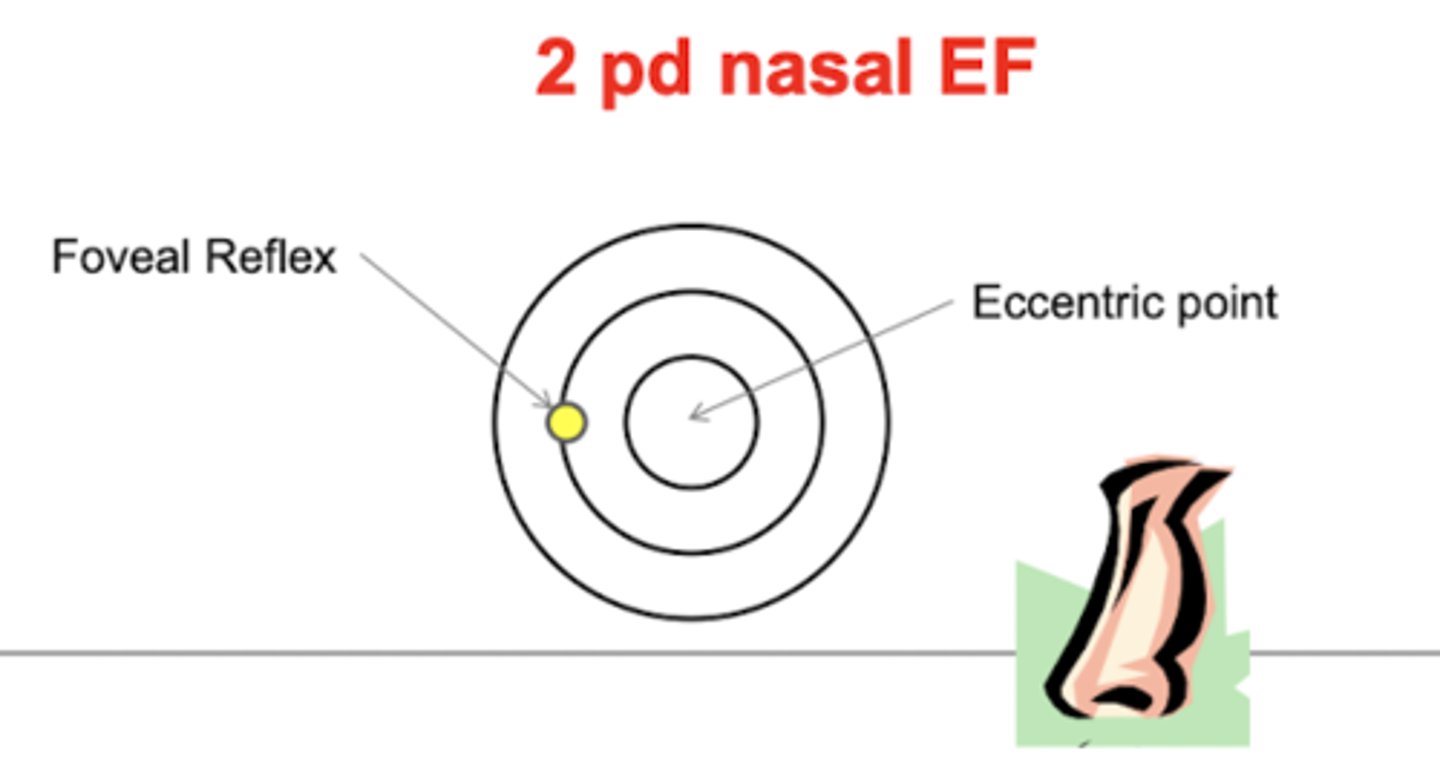
What is visuoscopy?
using direct ophthalmoscope to look at the macula → should see foveal reflex directly in center of the target when centrally fixating
what does visuoscopy determine?
if fixation is steady or unsteady
what can visuoscopy detect?
1. abnormal fixational eye movements → slow drift, saccadic intrusions, nystagmus
2. normal fixational eye movements are harder to detect
what can you observe with visuoscopy?
if fixation is central or eccentric → if eccentric determine the direction and magnitude of eccentric fixation
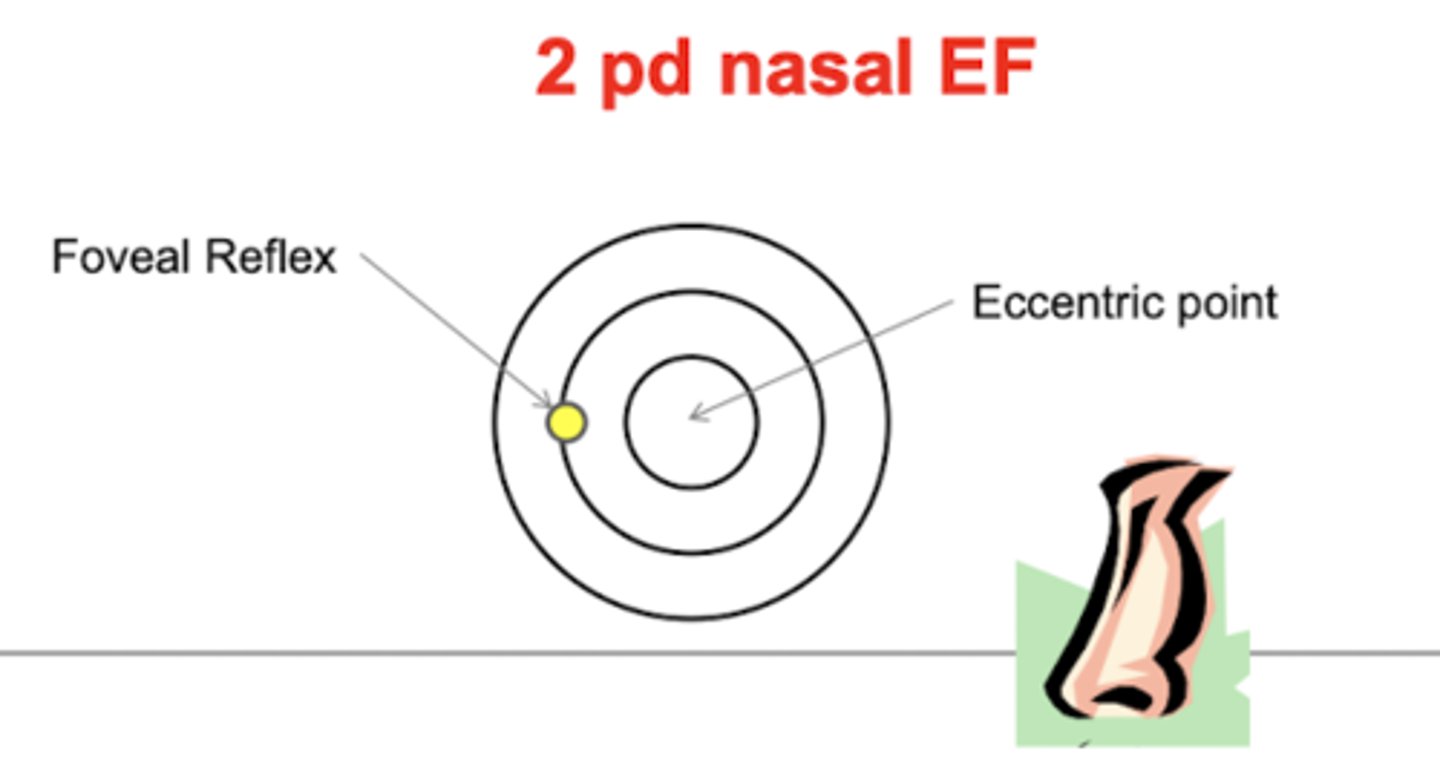
How do we find the direction of the eccentric fixation?
the location of the eccentric point (center of target) relative to the fovea
What is the eccentric point?
point on retina where object is imaged
How do you know the magnitude of eccentric fixation in visuoscopy?
measure eccentric fixation from fovea (example: eccentric fixation is 2 pd nasal to fovea)
projected target from a distance of 1 m → separation of 1cm = 1 pd
What ocular condition is eccentric fixation seen in?
strabismic amblyopes
Is eccentric fixation a monocular or binocular phenomenon?
monocular
what tests does eccentric fixation affect?
any testing done while having the patient fixate monocularly
How does eccentric fixation differ from eccentric viewing?
1. in eccentric fixation, patients believe they are looking straight at the target vs. in eccentric viewing, patients are intentionally looking off the the side to get around scotoma.
2. clinically we try to eliminate eccentric fixation, but try to teach eccentric viewing.
How can you approximate VA with eccentric fixation?
MAR = EF + 1
What VA means your patient does not have eccentric fixation?
If they are 20/20
how to assess fixation with a penlight?
pt monocularly looks at a penlight held by the dr → dr notes position of the 1st Purkinje image relative to the center of the entrance pupil
what is the clinical angle kappa?
average result with central fixation is a corneal reflex that is +0.25-0.5 mm nasal to the center of the entrance pupil
what is the sign convention for clinical angle kappa?
+ = reflex nasal to center of entrance pupil
- = reflex temporal to center of entrance pupil
what happens when pt moves from central fixation to looking temporally to light?
entrance pupil and corneal reflex move temporally but entrance pupil will more further temporally → corneal reflex is displaced further nasal relative to center of entrance pupil
what is a shift of 1 mm equivalent to?
12 deg ~ 22 pd
what is the Hirschberg test?
objective test for strabismus → same concept as angle Kappa only now test binocularly
what should the Hirschberg test always be compared to?
angle Kappa → assume normal angle Kappa is +0.5 mm
if the reflex is 0.5 mm nasal to the center of the entrance pupil in both eyes?
indicated pt is fixating accurately with both eyes → fusion or ortho-tropia (gives no indication if there is a phoria or not)