NPTEFF-- Non/Other Systems Bootcamp
1/156
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
157 Terms
Hickman catheter
location
--insertion through cephalic or internal jugalar vein
use
--long term drug admininstration
--chemo, antibiotics
Swanz-Ganz catheter
location
--soft flexible catheter inserted through vein (usually jugular or femoral) and reaching the pulmonary artery
use
--monitors pulmonary artery pressure and heart function
Arterial line
location
--inserted into artery and attached to monitoring system
use
--measure blood pressure and ABGs
Central venous pressure catheter
location
--indwelling venous catheter with a manometer
use
--measures pressure in right atrium or SVC, right ventricle function, and circulating blood volume
cautions with lines and tubes
--chest tube, catheter, IV line, arterial line, femoral line
chest tube
--positive pressure is contraindicated, if dislodged have pt exhale and plaze gauze or gloved hand over and call nurse
catheter
--hang below level of bladder, don't empty if output is monitored, alert staff if overfilled
IV line
--arm should not be held above head for extended periods
arterial line
--if dislodged, apply firm pressure and alert nursing staff
femoral line
--avoid repetitive hip flexion more than 45 deg
CPR guidelines
1. Check environment/scene for safety
2. Activate emergency response and get AED if available
• If a child or infant and unwitnessed collapse give CPR x 2 min then activate emergency/get AED
• If a second rescuer, second person activates/gets AED, begin CPR immediately, use AED when available
3. Compression-ventilation ratio
--Adults: 30:2, 100-120 bpm, 1 breath per 6 seconds
--Children 30:2 for one rescuer, 15:2 if two rescuers, 100-120 bpm, 1 breath per 2-3
seconds
4. Compression depth and hand placement
--Adults: 2 inches, 2 hands on lower sternum
--Child/infant: 1/3 AP chest diameter
(2 inch in child, 1.5 inch in infant), 1 hand in small child, 2 fingers in infant center of chest
5. Limit chest compression interruptions to <10 seconds
contact precautions
lice, scabies, impetigo, uncontrolled diarrhea, HepA, HepB, dermatitis, rota virus, MRSA, VISSA, VRE, clostridium
hand washing, gloves, and gown
private room without negative air flow
minimize transport, pt washes hands if they leave room
droplet precautions
mumps (rubella), streptococcus a, mengingitism pneumonia, influenza, pertussis
hand washing, gloves, and mask w/in 3ft of pt
--contact precautions only when skin lesions present
private room without negative air flow
minimize patient transport, pt wears mask if leaving room
airborne precautions
(MTV) measles, tuberculosis, varicella, SARS, herpes zoster, chickenpox, small pox
hand washing with gloves, gown, and N95 mask
private room with negative air flow, keep door closed
minimize patient transport, pt wears mask if leaving room
types of data
parametric (measurable quantity)
--interval: equal intervals, no true zero
IE: MCAT score, credit score, IQ score
--ratio: equal intervals, but has a true zero (zero is an actual zero value)
IE: ROM values, weight, height, time value
nonparametric data (NO measure, quality)
--nominal: different categories, no zero, no order/rank, no intervals
IE: sex, ethnicity, blood type, eye color
--ordinal: categories which are ordered/ranked but interval is not measurable or equal
IE: MMT grades, low vs middle vs high income status, level of agreement, political status
meaning of reliability
reliability
--refers to if the test can be accurately repeated or reproduced
types of reliability
intra rater
--accuracy of repeated measurements taken by the same tester
inter rater
--accuracy of repeated measurements taken by different testers
test retest
--same test repeated on same individual at different time
meaning of validity
how well an instrument measures what it is intended to measure
IE: goniometer has strong validity for measuring ROM but weak validity for measuring balance
pretest-posttest research design
1. study sample that has random assignment into
--experimental group OR control group
2. pre test measure/observation taken
3. application of independent variable
--experimental intervention OR no intervention/placebo
4. post test measure/observation taken
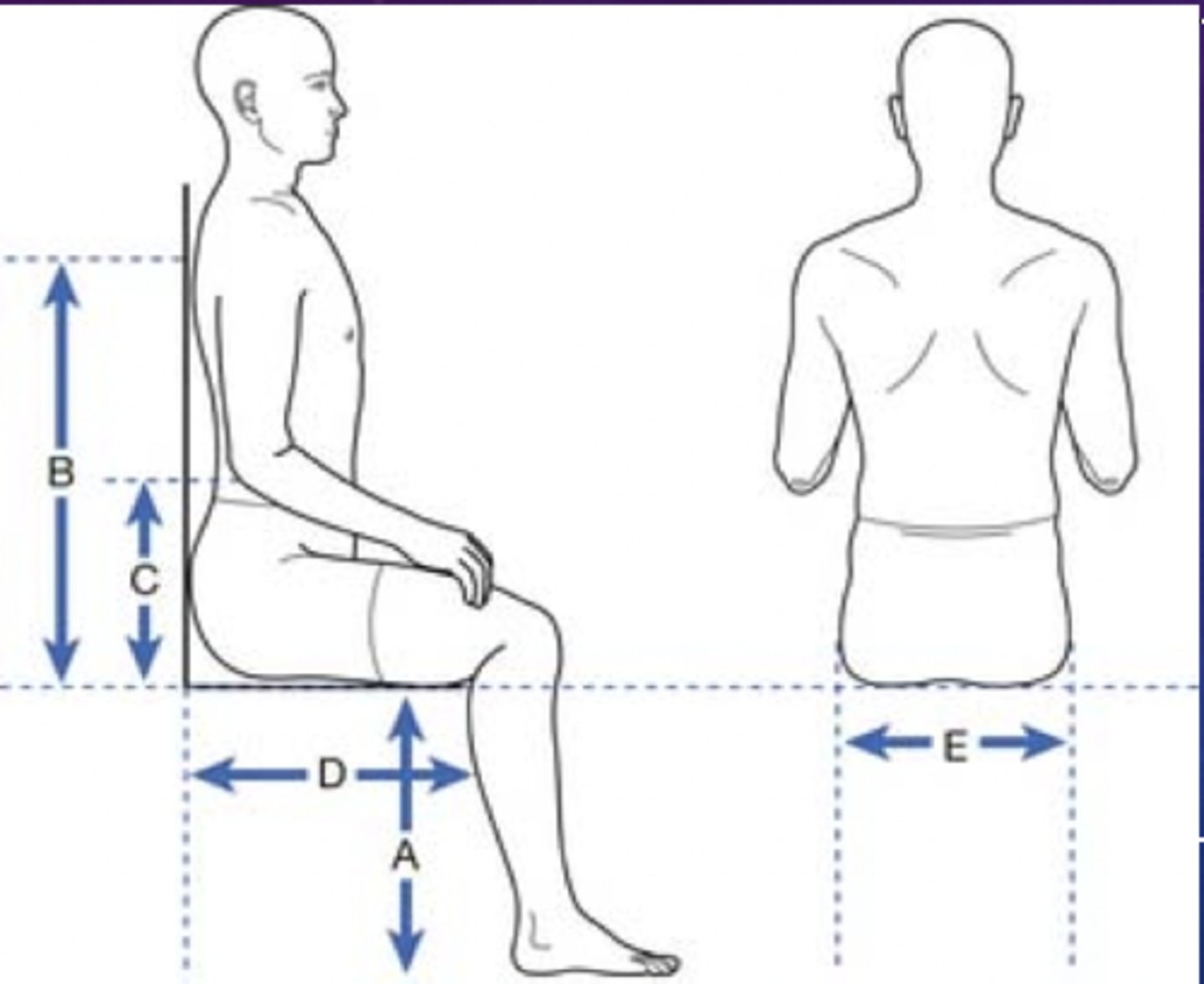
wheelchair measurements: seat height
how to measure
-- heel to popliteal fold (plus 2 inches)
average measure
-- 19.5-20.5 inches
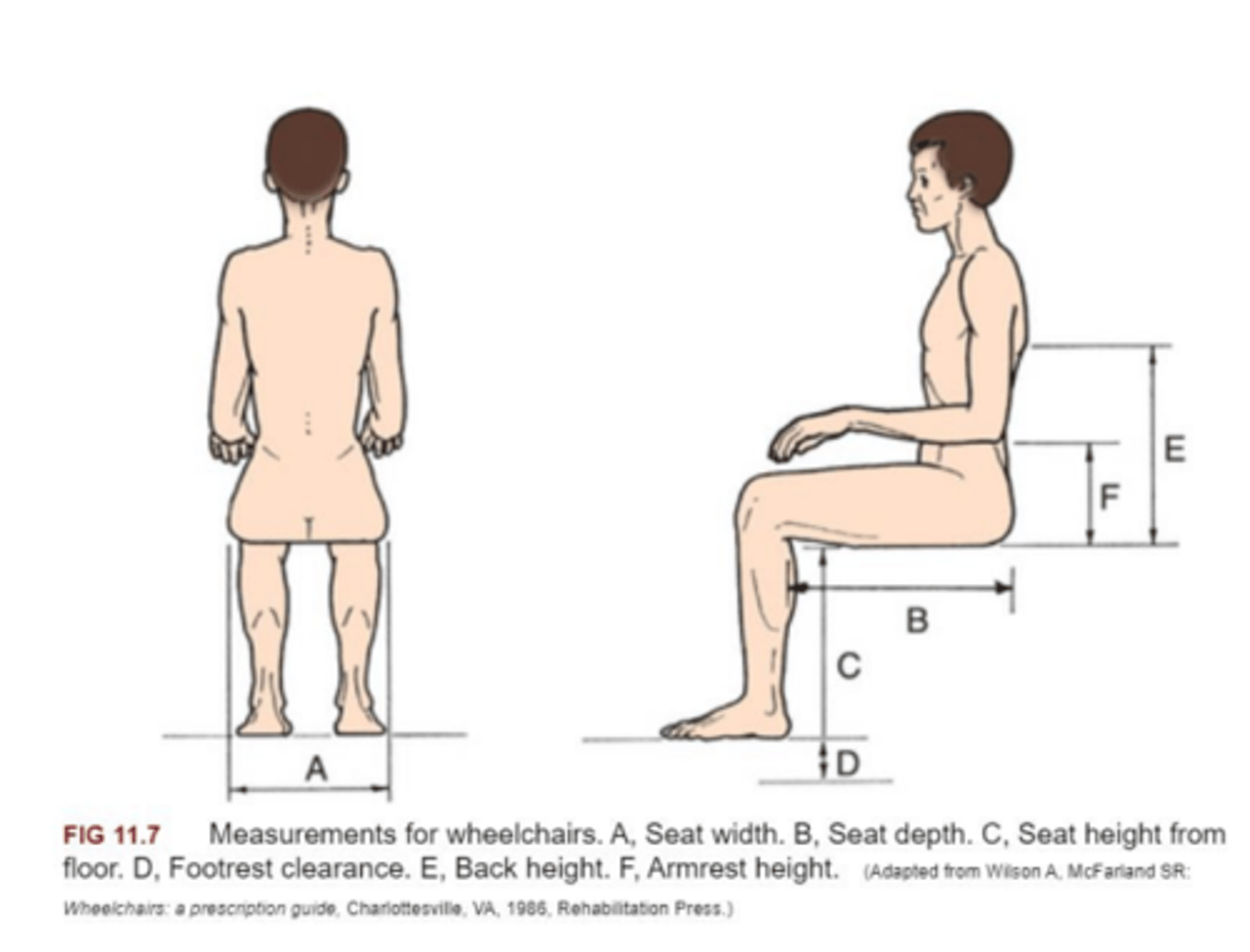
wheelchair measurements: seat depth
how to measure
-- posterior buttock along lateral thigh to popliteal fold (minus 2 inches) (along lateral length of femur)
average measure
-- 16 inches
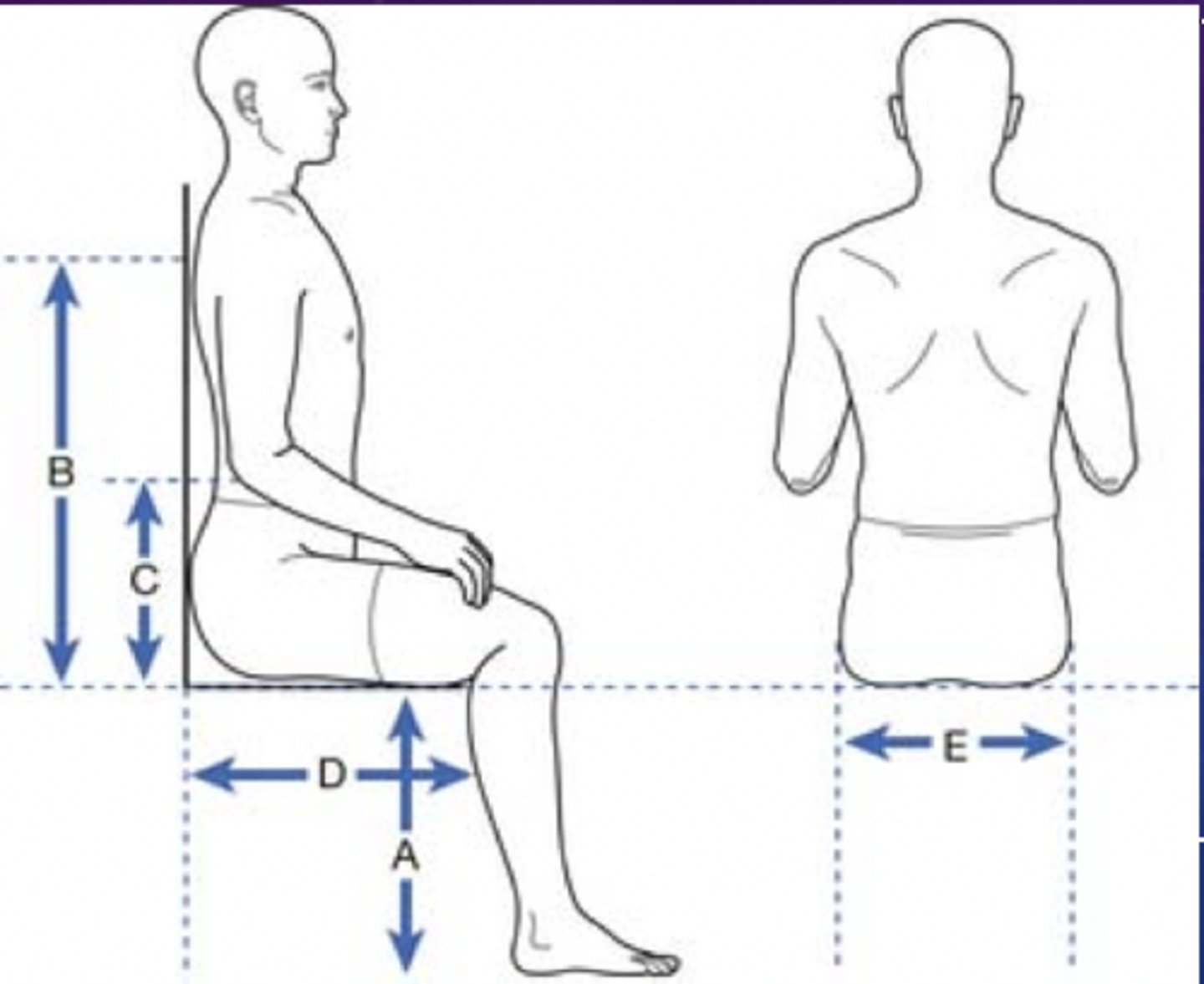
wheelchair measurements: seat width
how to measure
-- widest aspect of buttocks/thighs (plus 1.5-2.0 inches)
average measure
-- 18 inches
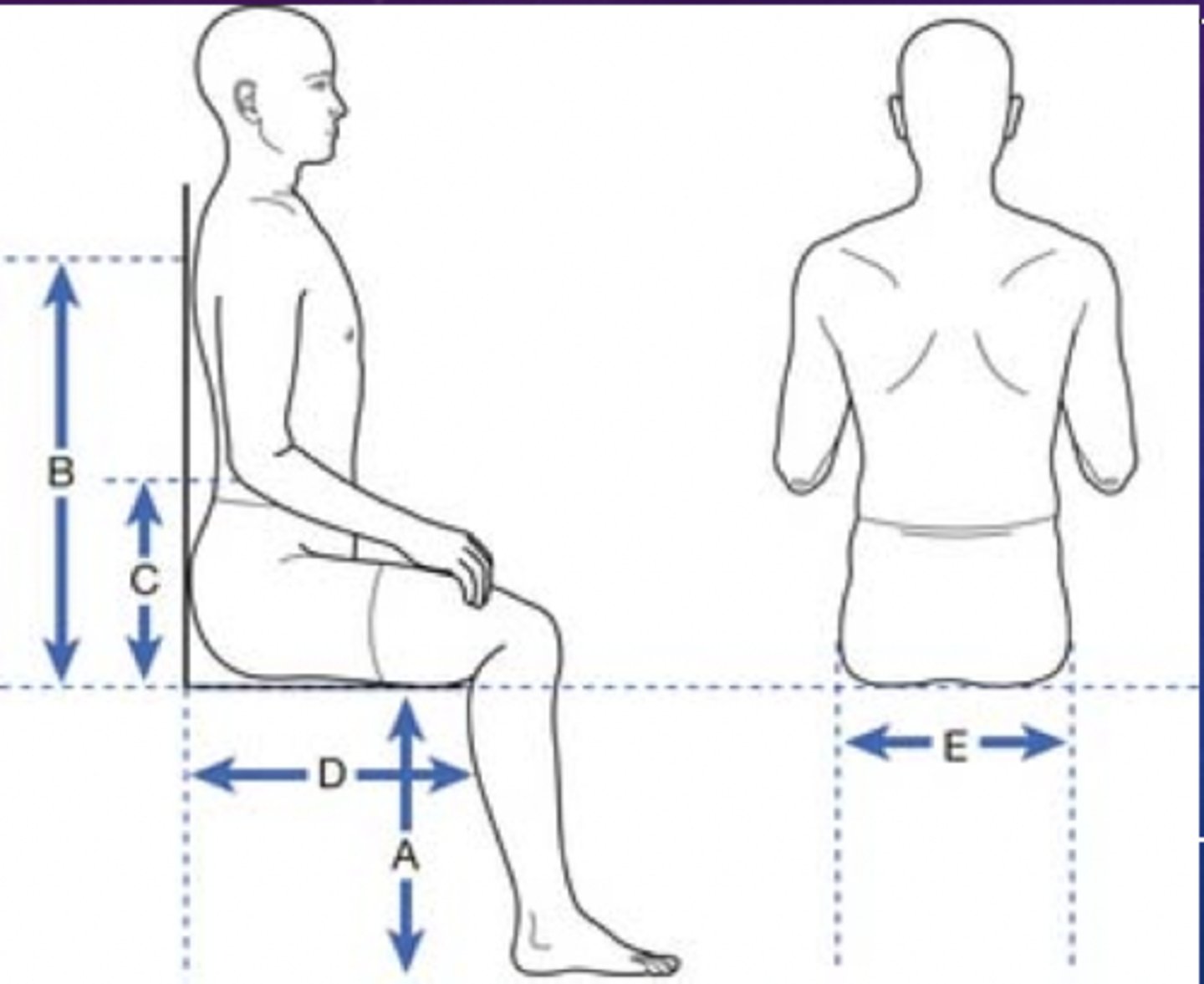
wheelchair measurements: back height
how to measure
-- chair seat to axilla (minus 4 inches) (consider any seat cushions and add thickness to final value)
average measure
-- 16 inches
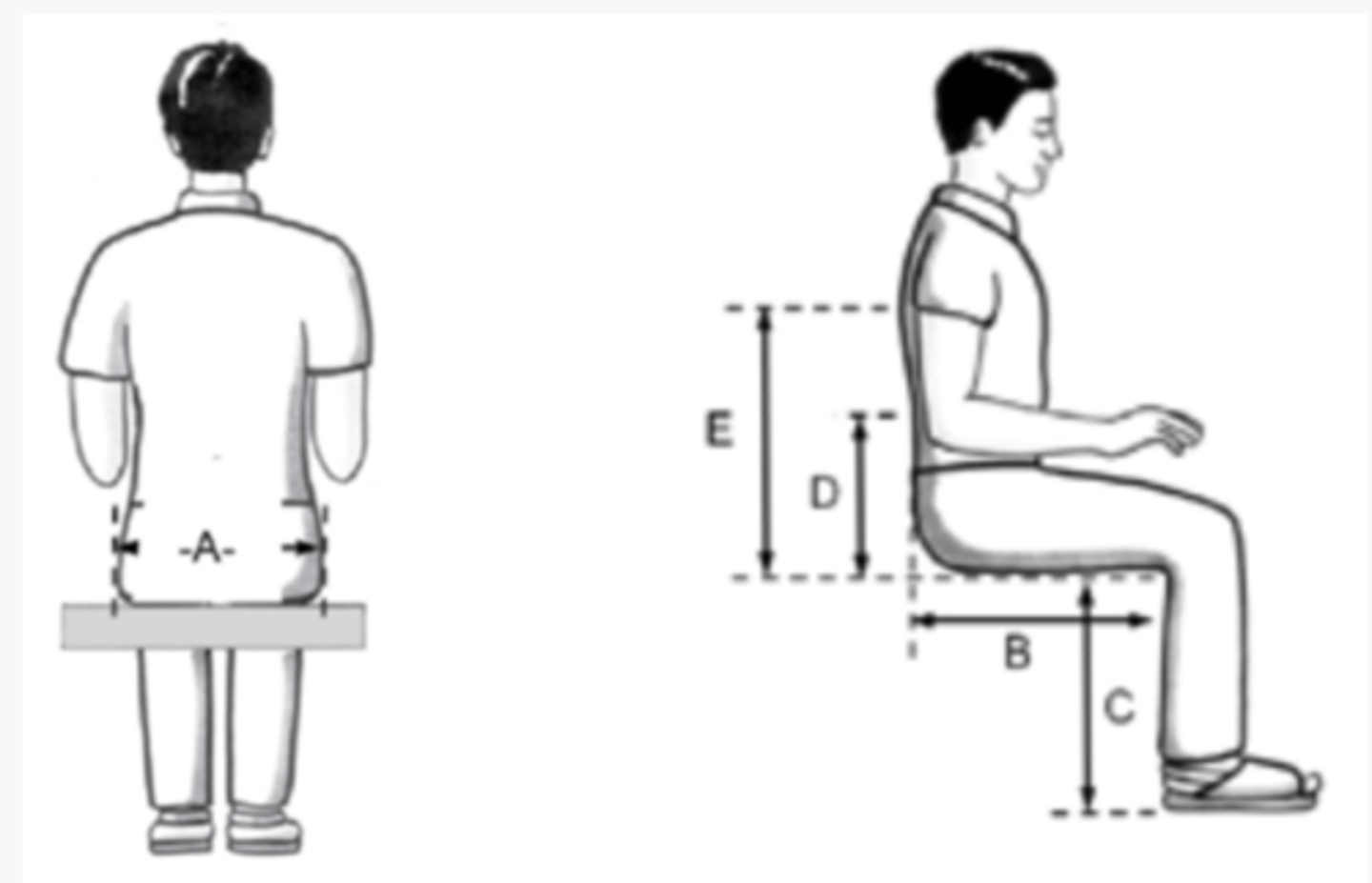
wheelchair measurements: armrest height
how to measure
-- seat of chair to olecranon (plus 1 inch) (consider cushion thickness)
average measure
-- 9 inches
wheelchair axel positioning
normal axel positioning (axel of back wheels)
--in line with shoulder or slightly posterior
for bariatric patients (obese pts)
--move rear wheel axel anterior
for bilateral transfemoral amputee patients
--move rear wheel axel behind pts shoulders
--amputations cause more COM to move posterior in chair so need to compensate with further posterior axel
wherever weight is moving-- thats the direction axel moves
wheelchair propulsion: propulsion phase
apply a smooth, continuous push on the push rims, extending arms forward
--this motion propels the wheelchair
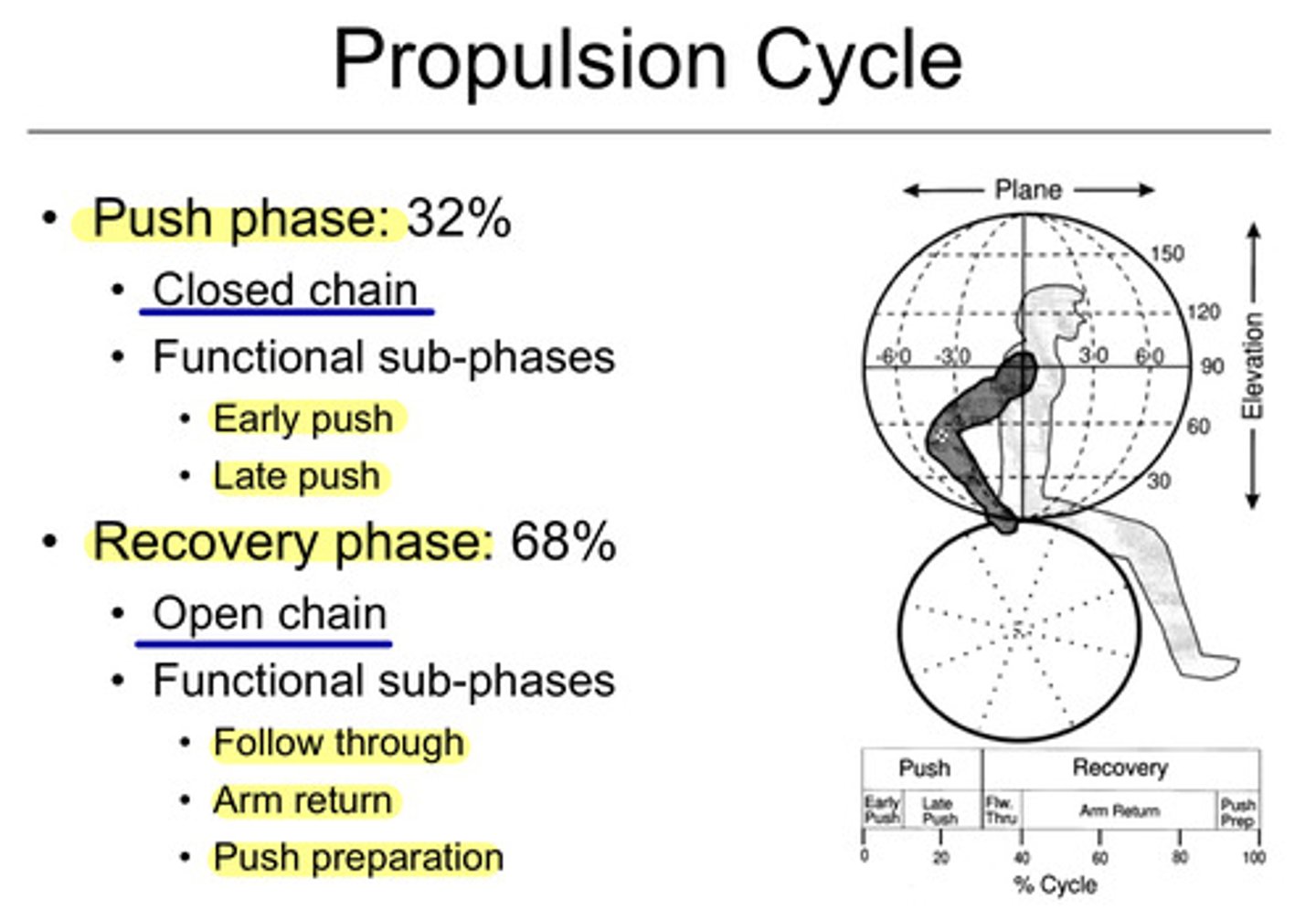
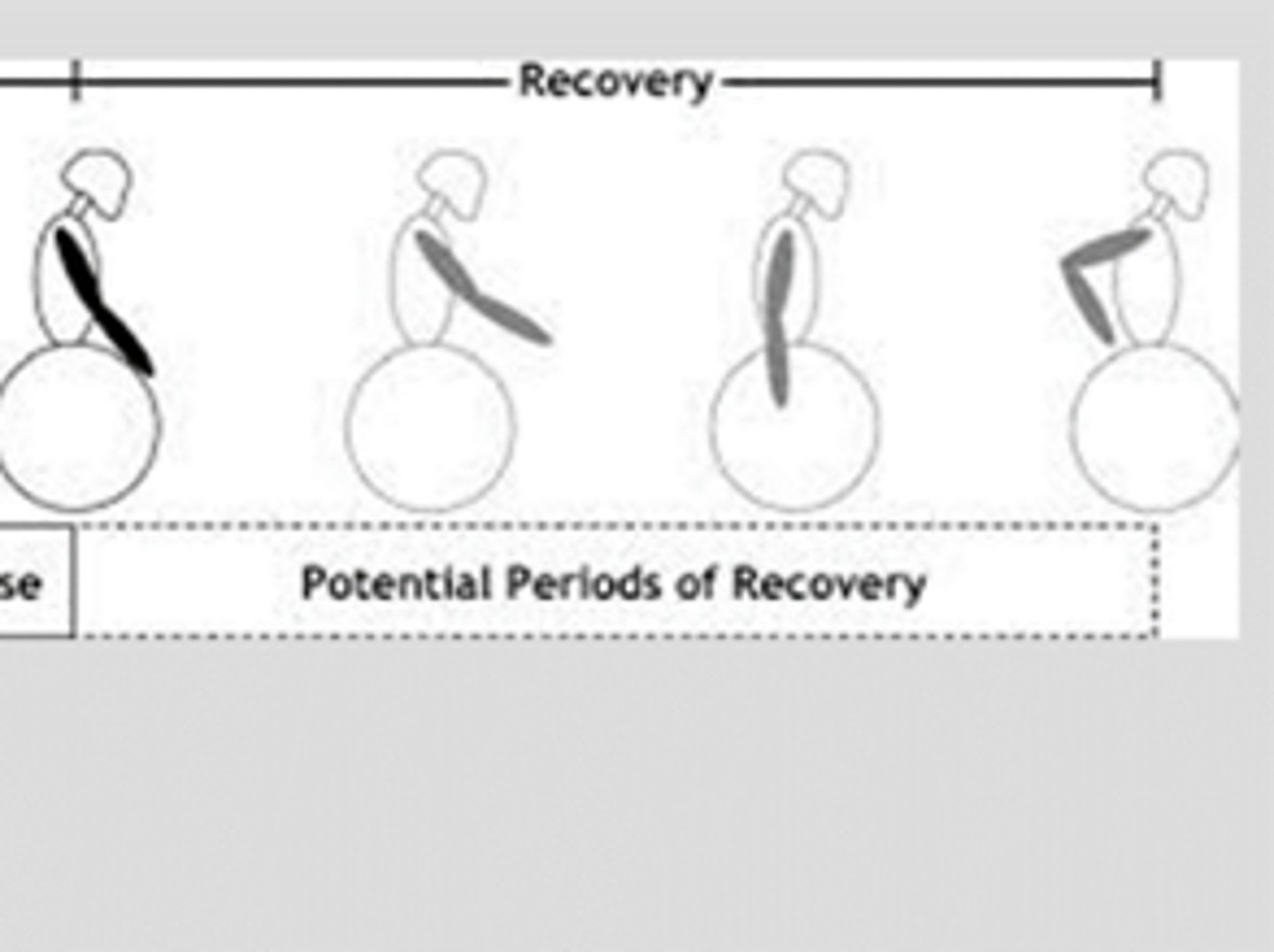
wheelchair propulsion: recovery phase
after the push, release the push rims and bring hands back to starting position
--ready for the next push
wheelchair propulsion: turns
pull one wheel backward and other wheel forward
turn right
--push L wheel forward and R wheel backward
turn left
--push R wheel forward and L wheel backward
wheelchair propulsion: wheelie
patient places hands back on hand rims, then push rims forward abruptly and forcefully
wheelchair propulsion: ascending curb
Ascending curb:
-- Lift the front casters onto the curb by performing a small wheelie
-- Push forward on the push rims to lift the
rear wheels onto the curb
wheelchair propulsion: descending curb
Descending curb:
-- Perform a wheelie and descend with rear
wheels off the curb followed by castor
wheels
OR
-- Descend backwards: Allow the rear wheels
to slowly roll off the curb, followed by the
castor wheels
assistive devices: standard crutches (axillary crutches)
Standard Crutches (Axillary Crutches)
-- Axilla space of approx. 2 inches
-- Crutch is approx. 2 inches lateral and 4-6 inches anterior to the patient’s toe of the shoe
-- Elbow flexion approx. 20-25 degrees when grasping handpiece
assistive devices: forearm crutches (lofstrand crutches)
Forearm Crutches (Lofstrand Crutches)
-- Top of forearm cuff is just distal to elbow, approx. 1.0-1.5 inches below olecranon process
-- Crutch is approx. 2 inches lateral and 4-6 inches anterior to the patient’s toe of the shoe
-- Elbow flexion approx. 20-25 degrees
assistive devices: cane
Cane
-- Always goes on the opposite side
-- Cane is approx. 2 inches lateral and 4-6 inches anterior to the patient’s toe of the shoe
-- Elbow flexion approx. 20-25 degrees
-- Ascending = Good foot goes up first, followed by bad foot and cane
-- Descending = Bad foot and cane first, followed by good foot
therapist positioning: level ground ambulation
Stand behind and slightly toward the patient’s affected lower extremity
Therapist’s hand should be nearest to the patient to grasp under the back of the gait belt with forearm supinated
Therapist should move forward in step/in sync with the patient; PT’s forward foot moves with the assistive device
therapist positioning: stair navigation
Ascending positioning
-- Therapist should be positioned posterolateral (to the patient’s weak side)
-- Grasp the gait belt with one hand; be prepared to use your other hand to control the trunk
-- Advance your feet up one step after the patient has advanced one step, but maintain your feet in an anteroposterior position
Descending positioning
-- Therapist should be positioned anterolateral (to the patient’s weak side)
-- Grasp the gait belt with one hand
-- Do not allow the patient to develop momentum when descending the stairs.
for BOTH: PTs feet should be on two separate stairs to maximize stability if pt falls
assistive device stability (MOST to LEAST stable)
terms to use
--axillary crutches
--single point cane
--parallel bars
--quad cane
--forearm crutches
--walker
--hemi walker
1. Parallel bars
2. Walker
3. Hemi walker
4. Axillary crutches
5. Forearm crutches
6. Quad cane
7. Single point cane
lifts and transfers: 3 person lift
Used to transfer a patient from a stretcher to a bed or treatment plinth
lifts and transfers: 2 person lift
Used to transfer patients of different heights or surfaces or transferring to the floor.
lifts and transfers: dependent squat pivot transfer
Used to transfer a patient who cannot stand independently but can bear some weight through the trunk and lower extremities.
lifts and transfers: hydraulic lift
Used for dependent transfers when the patient is obese, there is only one therapist available to assist with the transfer or patient is totally dependent
ramps and slopes: standard measures
32 inches for doorway
36 inches for hallway (no turning required)
1:12 ratio for stair/ramp (7in is one stair)
--1 inch of stair for 12inch ramp
wooden floors
Metabolic syndrome (definition and criteria for dx)
consists of signs and symptoms that are risk factors and are strongly linked to type 2 diabetes, cardiovascular disease, and stroke.
A diagnosis is made if 3 or more are present:
Waist circumference
-- > 40 inches in men or > 35 inches in women
Fasting Plasma Glucose
-- > 100 mg/dL
Blood Pressure Systolic
--130 mmHg (or higher) and/or diastolic BP = 85 mmHg (or higher) (stage 1 HTN)
High Density Lipoprotein (HDL)
-- < 40 mg/dL in men or < 50 mg/dL in women
--HDLs are good so they should be high in healthy adults
Triglycerides
--150 mg/dL or higher
WEIGHHT
--weight expanded
--impaired glucose
--hypertension
--HDLs
--triglycerides
Hypothalamus-- regulation
responsible for regulation of ANS
sends signals to anterior and posterior pituitary glands
Anterior pituitary gland-- regulation
ACTH
--to adrenal cortex
--which releases cortisol and aldosterone
TSH
--to thyroid gland
--which releases T3 and T4
FSH, LH
--to ovaries and testes
--which releases estrogen, progesterone, testosterone
GH
--to bones and tissues
--promotes growth and metabolism
Prolactin
--milk production in breasts
what does cortisol stimulate?
regulates stress, glucose, regulates BP, anti-inflammatory
what does aldosterone stimulate?
retains sodium and water
excretes potassium (kicks out K)
Posterior pituitary gland-- regulation
ADH aka Vasopressin
--regulates water and mineral balance, water retention
Oxytocin
--stimulates uterine contractions during birth, skin to skin contact
Thyroid gland-- regulation
produces hormones that act to control the rate at which cells burn the fuel from food
Parathyroid gland-- regulation
regulate calcium and phosphate metabolism
Adrenal gland-- regulation
produces corticosteroids that will regulate water and sodium balance, the body's response to stress, the immune system, and metabolism
Addison's disease
Adrenal insufficiency
--decreased cortisol and aldosterone
--decreased BP, dehydration
--hyperkalemia
--decreased glucose
--weight loss, anorexia, GI issues
--general weakness
--intolerance to cold and stress
--anxiety and depression
bronze pigmented skin
aDDisons
DD-- double decreased
little Ms. Addisons
Cushing's disease
Overactive adrenal gland
--elavated cortisol and aldosterone
--increased BP and water retention
--hypokalemia
--increased glucose
--weight gain, round moon face
--proximal muscle weakness and atrophy
--intolerance to heat
--osteoporosis
red, ruddy appearance
Cushings is cushy and chubby
Cushing's disease vs Cushing's syndrome
Cushing's disease
--pituitary issue with more ACTH secretion
--stimulates adrenal gland and more cortisol released
Cushing's syndrome
--adrenal gland tumor
--secretes more cortisol leading to drug toxicity
symptoms common for both
Hyperthyroidism (Grave's disease)
increased T3 and T4, low TSH
--increased HR
--low BP
--high BMR (metabolism)
--heat intolerance
--restlessness, insomnia
--hyperreflexia
--diarrhea
--increased perspiration
--weight loss and increased appetite
--silky skin, moist palms
increased glucose absorption into body (less in blood)
graves like death valley (hot in arizona)
Hypothyroidism (Hashimoto's disease)
decreased T3 and T4, high TSH
--decreased HR
--high BP
--low BMR (metabolism)
--cold intolerance
--sleepy
--proximal muscle weakness
--delayed reflex response
--constipation
--decreased perspiration
--weight gain and decreased appetite
--dry skin and hair, brittle nails
decreased glucose absorption into body (more in blood)
Hyperparathyroidism
high calcium in blood and low phosphate
--can demineralize bone; low density
--glove and stocking sensory loss
osteopenia, peptic ulcers, kidney stones, renal insufficiency, fatigue, depression, confusion
hypercalcemia causes short QT interval
Hypoparathyroidism
low calcium and high phosphorus
--muscle cramps
--fingers and mouth sensory loss
convulsions, cardiac arrhythmias, muscle twitching, muscle cramps/spasms, tetany, fatigue, weakness
hypocalcemia causes prolonged QT interval
Type 1 Diabetes Mellitus (DM)
Pancreas produces no insulin → insulin dependent DM
Diagnosed mostly at childhood, but can be any age
Symptoms:
--Polyphagia, weight loss, ketoacidosis, polyuria, polydipsia, blurred vision and dehydration
ketoacidosis is a medical emergency (body excessively uses fat instead of glucose for energy; acetone fruity breath)
Type 2 Diabetes Mellitus (DM)
Body's resistance to insulin → insulin resistant DM
Occurs secondary to other dysfunctions
Symptoms:
--Similar to Type 1 with rare occurrence of ketoacidosis
fasting blood glucose level
> 126 mg/dL
random blood glucose level
measured at any time
> 200 mg/dL
hemoglobin A1C (HbA1c) level
avg glucose level over span of 3mo
> 6%
normal is 4-6%
immediate insulin needed over 10%
Hypoglycemia
glucose < 70 mg/dL
--pallor, sweating
--shakiness
--poor concentration
--tachycardia
--dizziness, faint
--excessive hunger
Hyperglycemia
glucose > 300 mg/dL
--weakness
--dry mouth
--frequent urination
--dull senses, confusion
--diminished reflexes
--excessive thirst
exercise and diabetes (do's and dont's)
--avoid extreme temps
--do not exercise at peak of insulin (2-4 hrs)
(bc exercise increases insulin in general so there will be excessive insulin causing low blood sugar and hypoglycemia)
--provide initial carb snack
-exercise in morning
exercise and diabetes (FITT principle)
-- 3-7 days per week
-- 11-13 RPE (can go up to 17)
-- at least 150 min/week
-- moderate intensity
blood glucose levels for exercise
100 - 250 = safest
70 - 99 = carb snack
< 70 or > 300 = contraindication
> 250 = assess for ketoacidosis
(if ketones then NO, if no ketones then proceed with caution)
stress incontinence (definition and treatment)
Involuntary leakage of urine during cough, sneezing, or exertion. Can be seen postpartum, pelvic floor muscle weakness.
treatment
--strengthen pelvic floor muscles
urge incontinence (definition and treatment)
Involuntary contraction of the detrusor muscle with a strong desire to void (urgency). Can be seen with infections, Parkinson's disease, UMN lesions.
treatment
--treat infections; voiding schedule
overflow incontinence (definition and treatment)
Incontinence caused by an acontractile or underactive detrusor muscle. Bladder is
overdistended, can not empty completely, and urine dribbles or leaks out. Can be seen with benign prostatic hyperplasia, DM.
treatment
--behavior mods like double voiding, meds, catheter
functional incontinence (definition and treatment)
Incontinence due to mobility, dexterity, or cognitive deficits. Can be seen with dementia, lower extremity weakness.
treatment
--clear clutter, improve accessibility to bathroom, prompt voiding
Benign prostatic hyperplasia
hypertrophy of the prostate glands causing narrowing of the urethra resulting in an increase in urinary retention and dilation of urinary bladder
pregnancy-- MSK changes
weight gain 25-35lbs
postural changes
--forward head, kyphosis, increased lordosis, anterior pelvic tilt
--postural stress continues postpartum d/t lifting and carrying baby
treatment
--postural education, stretching tight muscles, strengthening weak muscles
--pelvic stabilizations, pelvic tilts
pregnancy-- CVP changes
BP is LOW in 1st and 2nd trimester
--increases in 3rd trimester
supine lying can cause compression of IVC and decreases CO
--STOP after 1st trimester (or else will cause supine hypotensive syndrome
resting HR increases 10-20 bpm
--work of breathing increases
left side lying is considered the best
--decreases compression to IVC ansd maximizes CO
--also decreases GERD as internal organs are relaxes
--improves maternal and fetal circulation
HR does not proportionally increase with exercises
pregnancy-- metabolic rate, heat production, and fasting blood glucose levels
metabolic rate and heat production
--increases
normal fasting blood glucose levels
--decrease
preeclampsia
Pregnancy-induced acute hypertension after the 20th week of pregnancy
Presentation
--increase in protein in urine, hyperreflexia, edema, headache, sudden weight gain seen
Diagnosis confirmed
--a blood pressure reading more than 140/90 mmHg
--second abnormal blood pressure reading four hours after the first confirms the diagnosis
It is an emergency!
gestational diabetes
a form of diabetes mellitus that occurs during some pregnancies ONLY
--lowered production of insulin and blood glucose increase
--after birth, levels become normal
eclampsia
NOT during pregnancy
seen after birth
--more severe than preclampsia
characterized by seizures
ectopic pregnancy
when fertilized egg is not implanted in the uterus
--it is anywhere else in uterine cavity; usually in fallopian tubes
--not safe, needs to be terminated
--bterm-72leeding occurs
pregnancy-- contraindicated to exercise
heart disease with unstable hemodynamics
RLD
incompetent cervix
--early dilation of cervix before full term
vaginal bleeding
placenta previa
--after 26 weeks
--placenta located where it may detach before delivery
preclampsia or pregnancy-induced HTN
rupture of membranes
--loss of amniotic fluid before labor
premature labor
--labor beginning before 37th week of pregnancy
uncontrolled maternal T1 DM
severe anemia
pregnancy-- treatment for diastasis recti
> 2 cm
--abdominal bracinjg and head lift
--progress >>> bracing, head lift, and posterior pelvic tilt
> 4 cm abdominal bracing and breathing exercises
gastroesophageal reflux disease (GERD)
backflow of contents of the stomach into the esophagus, often resulting from abnormal function of the lower esophageal sphincter, causing burning pain in the esophagus
s/s
--heart burn after eating/lying down
--dysphagia
--hoarseness of voice
--atypical pain of head and neck
complications
--aspiration pneumonia, asthma
--esophagitis
GERD treatment
Maintain upright positions
Eat meals at least 3-4 hours before sleep
AVOID supine: tends to straighten the esophagus
Sleep on the LEFT side preventing nocturnal reflex
Exercise must be completed 2-3 hours after eating or before meals
AVOID spicy, chocolate, and fatty food
Drugs
--Antacids
--H2 receptor blockers
--Proton pump inhibitors
pain referral locations
--mid back, scapula
--shoulder
--pelvic, low back, sacrum
mid back; scapula
--esophagus, gallbladder, stomach, pancreas, kidney
shoulder
left shoulder
--heart, diaphragm, spleen, tail of pancreas
right shoulder
--gallbladder, liver, head of pancreas
pelvic; low back; sacrum
--colon, appendix, pelvic viscera, prostate
Pancoast tumor (and referral location)
upper lung tumor
--pain referred om C8-T2 nerve distribution
--mimics TOS
--pain on top of shoulder, ipsiL shoulder
typical pain patterns-- quadrants
Right Upper Quadrant (RUQ)
--head of pancreas
--gallbladder pathology
--liver pathology (hepatic)
--peptic ulcer
**good luck harry potter (gall, liver, head, peptic)
Right Lower Quadrant (RLQ)
--appendix
--crohn's disease
**air conditioning (appendix, crohn's)
Left Lower Quadrant (LLQ)
--diverticulitis
--ulcerative colitis
--IBS
**DUI (diverticulitis, UC, IBS)
Left Upper Quadrant (LUQ)
--tail of pancreas
--spleen pathology
**don't be stupid, kid (diaphragm, body/tail pancreas, spleen, L kidney)
Good luck Harry Potter,
Don't be stupid kid
and get a DUI
Go home and use air conditioning
RUQ, LUQ, LLQ, RLQ
**looks like "C" if looking at own chest
what is a hernia and its referred pain?
--hiatal, femoral, inguinal, umbilical
hernia is a condition where part of an organ is displaced and protrudes through the wall of the cavity containing it
Hiatal hernia causes shoulder pain
--similar symptoms to which
condition? GERD
Femoral hernia causes
--lateral pelvic wall pain and groin pain
Inguinal hernia causes
--groin pain
Umbilical hernia causes
--pain around umbilical ring in the mid to lower
abdomen
what are the contraindications after hernia repair
AVOID for the first 6 weeks
--stretching anterior structures
--increasing intraabdominal pressure
what is cholecystitis?
Blockage or impaction of gallstones in the cystic duct resulting in inflammation of the gallbladder
pain in RUQ radiating to R should and R scapula
--nausea, vomiting, low grade fever
--pain increases with eating fatty food
SPECIAL TEST
-Murphy's sign
what is Murphy's sign?
palpating near R subcostal margin as patient takes deep breath
if pain and tenderness increases during inspiration, the test is POSITIVE
what are peptic ulcers?
--definition, pain referral, characteristics, and types
open lesions in digestive system that cause pain
pain is burning, cramping in epigastric area
--can refer to R shoulder
characteristics
--coffee ground vomit (both)
--dark tarry stools (common of duodenal ulcers)
2 types
--gastric ulcers (stomach)
--duodenal ulcers
Gastric (stomach) ulcers vs Duodenal ulcers?
Gastric ulcers (stomach)
--lesions in stomach caused by chronic use of NSAIDS, stress, anxiety, or H pylori bacteria
--pain increases with presence of food d/t acid secretion, pain after eating
-pain relieved with antacids or medically treating infection
Duodenal ulcers
--lesions in duodenum causes mainly by H pylori infection
--pain increases with absence of food, midnight pain
--pain relieved by medically treating the infection
Inflammatory Bowel Disease (IBD)
Chronic inflammation of the gastrointestinal tract
more severe than IBS
2 types
--Ulcerative colitis (LLQ)
--Crohn's disease (RLQ)
Ulcerative colitis vs Crohn's disease?
Ulcerative colitis (L for Left, LLQ)
--only in large intestine and rectum
--continuous lesions
--s/s rectal pain, bleeding, bloody diarrhea with mucus/pus, fecal urgency, weight loss, LBP
Crohn's disease (R for Right, RLQ)
--occurs anywhere in GI tract
--skip lesions (not continuous in tract)
--s/s abdominal pain, weight loss, joint arthritis, pain relieved by passing gas
Inflammatory Bowel Syndrome (IBS)
spastic, nervous and irritable colon
causes
--emotional stress, anxiety, high fat, lactose foods
symptoms
--pain relieved by defecation
--sharp pains in morning or after eating
--nausea, vomiting, bloating, foul breath, diarrhea
--symptoms disappear while sleeping
--ribbon like stool
LLQ pain
treatment
--stress reduction
--dietary changes
--exercise
what is appendicitis?
inflammation of the appendix
--progression can lead to swollen infected appendix
symptoms
--pain in RLQ
--pain comes in waves then becomes steady
--anorexia, nausea, vomiting, elevated temperature, leukocytosis, fever
SPECIAL TESTS
--McBurney's point is tender to palpate
--Rovsing sign for pain migration
--Blumberg's sign for rebound tenderness
what is McBurney's point?
tender area at RLQ when palpating RLQ (appendicitis)
what is Rovsing's sign?
RLQ pain upon palpation of LLQ (appendicitis)
what is Blumberg's sign?
increased pain and rebound at RLQ over McBurney's point (appendicitis)
other tests for appendicitis?
--hop sign, psoas sign, obturator sign, Markle sign, pinch-an-inch test
hop sign
--hop on R leg causes RLQ pain
psoas sign
--hip in extension causes RLQ pain
obturator sign
--hip in IR causes RLQ pain
Markle sign
--heel drop or lowering heel from a heel raise causes RLQ pain
pinch-an-inch test
--pinch skin at RLQ; RLQ pain is (+) for appendicitis
--pinch skin at LLQ, LLQ pain is (+) for diverticulitis
seizures-- recognition and best immediate response
recognition
--sudden unresponsiveness or LOC
--muscle jerking or twitching
--muscle stiffening or loss of muscle tone
--incontinence
response
--remove any nearby objects that are sharp or can cause injury
--turn person to sidelying
--note amount of seizure time (if more than 5 min call EMS)
--dont hold person down or place objects in mouth
concussions-- recognition and best immediate response
recognition
--HA
--nausea
--balance issues
--fatigue
--blurred vision
--sensitivity to light or noise
--numbness / tingling
--cognitive, emotional deficits
response
--stop activity immediately if playing sports
--monitor symptoms
--consult healthcare professional promptly
when to seek EMS
--LOC
--repeated vomiting
--severe HA
--seizures
--unequal pupil size
--prolonged confusion
--weakness or numbness
dehydration-- recognition and best immediate response
recognition
--mild: thirst and dry mouth/lips
--mod: very dry mouth, cracked lips, HA, sunken eyes, postural hypotension
severe: rapid and weak pulse, confusion, lethargy, rapid breathing, seizures, inability to cry or urinate
response
--monitor s/s and prevent worsening
--drinking water
--if nauseous, drink small sips
--severe cases may need IV fluids
heat exhaustion vs heat stoke
heat exhaustion
--lots of sweating
--can have nausea, HA, rapid breathing, slightly elevated temp
--can be unconscious
--pupils normal
heat stroke
--no sweating
--can have nausea, HA
--very elevated temp (106 to 110 deg F)
--unconscious and convulsions
--pupils contract then dilate