Systems Physiology Final Exam
1/583
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
584 Terms
Biological Signals
Ligand/receptor (hormones, growth factors, cytokines, morphogens)
Chemical Signals
Signal gradients (ions)
Physical Signals
Mechanical properties of cells and their environment. e.g stiffness of surrounding environment
Forces: fluids, loading, compression…
Mechnobiology
Cells can sense their environment
Mechanotransduction
Mechanical force influencing cellular signalling and function
Cell Environment
= cells and and extracellular matrix
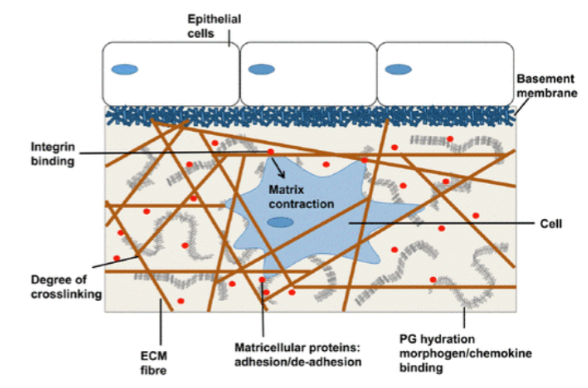
Cells + Extracellular Matrix
Cells produce extracellular matrix components. Functions of the ECM include the important mechanical and signalling roles, critical for cell, tissue and organ function.
2 Main Types of ECM
Basement Membrane and Interstitial Matrix
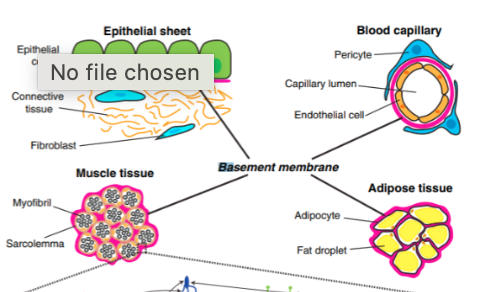
Basement Membrane
Surrounds most tissues including cell sheets (epithelial, endothelial) and cells/bundles. Specific components include type IV collagen, laminin, nidogen, perlecan. Found in adipose tissue, epithelial sheets, blood capillaries, and muscle tissue for example.
Interstitial Matrix
A 3D porous, amorphous gel surrounding connective tissue cells (fibroblasts) composed of collagen and elastin.
2 Main Types of Extracellular Matrix Components
Structural, fibrous proteins (biopolymers) and non-structural, non-fibrous proteins.
Structural, Fibrous Proteins of ECM
Collagens, elastins, and laminins
Non-Structural, Non-Fibrous Proteins of ECM
Glycoproteins/Proteoglycans
Hyalectans
Matrillins
Non-fibrillar collagens
Collagens
Largest protein component in mammals
28 Types
Monomer, cleaved by proteinases and assembled into fibrils.
Cross-linked by lysyl oxidase
4 types of Collagens
Type I - Bone, Skin, Tendon, Heart, Vessels (strength)
Type II - Cartilage
Type III - Reticulum, Heart, Blood Vessels (bit elastic)
Type IV - Basement Membrane
Elastins
Provides elasticity to tissues: major component of skin, arteries, lungs
Length can extend 2X
Tropoelastin (monomer)
Elastic fibres consist of an elastin core surrounded by microfibrils (fibrillin-1, fibulin-5)
Cross-linked by lysyl oxidise
Laminins
Important in basement membrane, mediates cell adhesion
60 possible heterotrimers

Glycoproteins/Proteoglycans
Proteins with carbohydrates/glycosaminoglycans (GAGs)
Chondroitin sulphate (CS)
Keratan sulphate (KS)
Dermatan sulphate (DS)
Heparan sulphate (HS)
Hyaluronic acid: (HA) (cartilage, synovial fluid)
Aggrecan: (CS, KS, cartilage)
Fibronectin: (basement membrane)
Perlecan: (HS, basement membrane)
Decorin: (CS, DS, interstitial matrix, associates with type I collagen)
ECM Roles
Anchorage, migration barrier, migration track, signal reservoir, low affinity co-receptor, signal presenter, functional fragments, and biomechanical force.
Matrix Remodelling/Turnover
Extracellular matrix remodelling and turnover is common in most tissues to repair/replace = maintain homeostasis Cells produce matrix biopolymers/proteoglycans, but not all and not to the same integrity as during development. Ex. Elastin has a half-life of ~70 years
Matrix Degrading Enzymes
Matrix Metalloproteinases (MMPs)
Inhibited by
Tissue inhibitors of metalloproteinases (TIMPs)
a disintegrin and metalloproteinases (ADAMs)
ADAMs with thrombospondin motifs (ADAMTSs)
Release of Protein Fragments from Matrix Degradation
Degradation can release protein fragments with specific function = Matrikines
Cleavage of the C terminus of perlecan releases endorepellin = promotes angiogenesis (formation of new blood vessels)
Ex. for repair processes but can be bad in disease such as diabetes
What adhere cells together?
Integrins that connect to the actin cytoskeleton through focal adhesion.
Integrin Subunits
24 integrins, heterodimeric: 17 ⍺ subunits, 8 β subunits
Form combinations which are largely cell type specific
β1 can bind 12 different ⍺
β4, 5, 6 and 8 can only bind 1 ⍺
Most ⍺ only bind 1 type of β
⍺4 and ⍺v can bind multiple different β
Integrin Ligands
Can be matrix proteins
Proteins with RGD or integrin interacting domains
RGD = amino acids: arginine, glycine, aspartic acid
E.g. collagen, elastin, GAGs
Can also be growth factors, small molecules, other receptors etc.
Eg VEGF, thrombospondin, TGF-

3 Types of Cell Junctions
Gap junctions, adherens junctions, and tight junctions
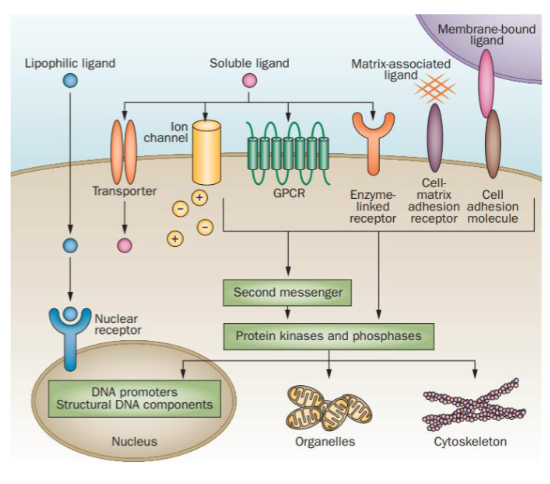
Types of Cell Receptors
GPCR, ion channels, transporters, enzyme linked receptors and nuclear receptors. All can signal to produce a cellular response and co-ordinated cell responses affect tissue level functions.
Functions of the Heart
Generate contraction force, maintain CO, HR, BP within range, and withstand fluidic forces.
2 Types of Forces in the Heart
Active = contraction of chambers
Passive = blood flow e.g., passive force of blood flowing through valves (pressure and shear)
Layers of the Heart Wall (inside → out)
Endocardium, myocardium, epicardium, pericardial cavity, parietal layer of serous pericardium, and fibrous pericardium.
Myocardium Cellular Composition
Consists of myocardial cells as well as fibroblasts, capillaries, and other types of cells.
Cells in the Heart
11 major cells types
Non-cardiomyocytes (CMs) dominate heart cellular composition
Ventricular and atria cardiomyocytes differ
Each region of the heart contains multiple different cell types
Each cell type within a region has distinct populations that differ in their gene expression and function
All these cell types and sub-types coordinate to maintain homeostasis and perform organ function
Sub-Populations of Heart Cells
Fibroblasts
Endothelial cells (line blood vessels)
Smooth muscle cells and pericytes
Myeloid cells
Lymphoid (tissue resident)
Neuronal
Adipose
Fibroblasts in the Heart
Responsible for maintenance of ECM
Distinct populations in each heart region
Smooth Muscle Cells and Pericytes of the Heart
SMCs surround larger arteries and pericytes surround capillaries.
Myeloid (Immune) Cells of the Heart
Macrophages/monocytes
Monocyte-derived (from blood)
Tissue-resident
Dendritic
Collagen in the Heart
Most abundant matrix component in the heart, produced by cardiac fibroblasts. Scaffold for CMs and non-CMs (ECs and FBs), signals for proliferation, differentiation etc.
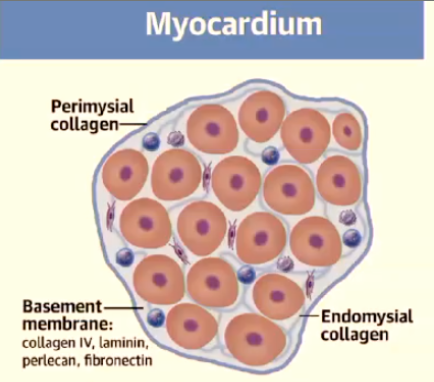
Endomysium and Perimysium
Endomysium = connective tissue around muscle fibres
Perimysium = connective tissue around bundles of muscle fibres
Purpose of Endomysium and Perimysium
Functions of these are for synchronised contraction
Passive expansion (when the ventricles are filling)
Overstretch prevention
Conduction
Collagen Type I (fibrillar)
Main collagen = confers tensile strength
Spatially organised by proteoglycans decorin, biglycan and Col XV
More found in perimysium
Contributes to overstretch prevention
Type III Collagen (fibrillar)
Thin fibres, contributes to elasticity
More in endomysium
Contributes to passive expansion
Type I and Type III Collagen Ratio and Type I Collagen Changes
Type I – Type III ratio influences mechanical properties (contraction and relaxation)
Type I Collagen increases with age
Decreases the ability for passive expansion which decreases cardiac output
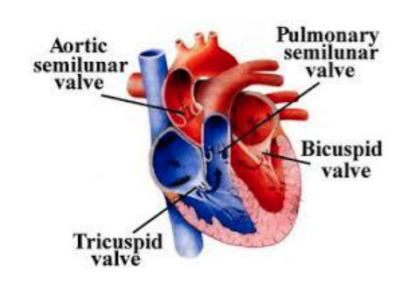
Heart Valves
Both semilunar and tricuspid valves have 3 leaflets, bicuspid/mitral valve has 2 leaflets
Include aortic semilunar valve, pulmonary semilunar valve, tricuspid valve, bicuspid valve
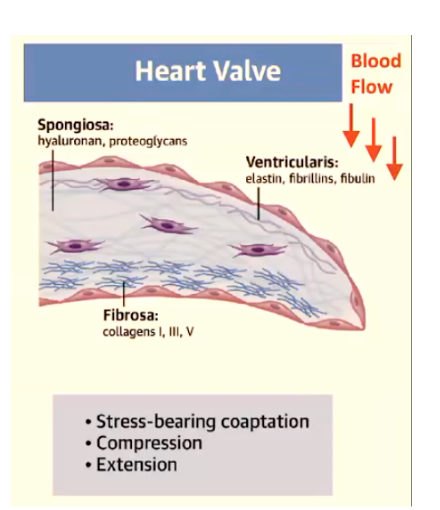
3 Layers of the Valves
Ventricularis (inflow side) (Atrialis)
Spongiosa
Fibrosa (outflow side)
Ventricularis (Atrialis)
Elastic fibres, fibrillin-1, fibrillin-2 and fibulins
Stretch and recoil
Inflow side
Spongiosa
HA (hyaluronic acid) and proteoglycans; versican, decorin and biglycan.
Cushion blood pressure forces, assist in re-alignment of collagen and elastin fibers, and resist delamination
Fibrosa
fibrillar collagens I, III and V
stiffness and ensure leaflet integrity
outflow side
Secretion of ECM
Valvular ECs and interstitial cells secrete the most matrix of all heart cells.
Fibrillin 1 Gene (FBN1) Mutations
Marfan’s syndrome = connective tissue disorder
Thickening of the AV valves and mitral and/or tricuspid valve prolapse, and aortic aneurysm.
Get backflow because the valves don’t close properly
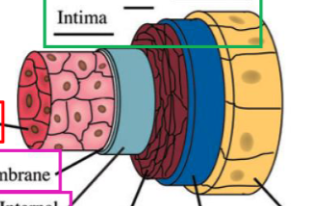
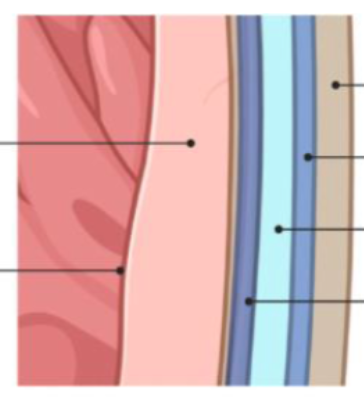
Layers of Vasculature (outside → inside)
Adventitia - connective tissue and external elastic lamellae
Media - smooth muscle cells and internal elastic laminae
Intima - endothelium and basement membrane
Arteries vs Veins
Same layers, but veins have a thinner media layer
Arteries pressure reservoirs
Veins volume reservoirs
Arterial Wall
Single cell layer of endothelium
SMCs in layers separated by concentric elastic laminae
Stiffness and strength mediated by collagen and elastin (50-70%)
Elastin is essential for vessel architecture and function
Forces Against Arteries
Arterial stiffness (force to deform vessel during systole)
Wall strength (max force applied before vessel failure/rupture)
Main Fibrillar Collagens in Elastic Arteries
Type I, III, and V. III in media (want in the middle to stretch), I in adventitia (prevent overstretch), collagen IV (basement membrane) and VI.
How are the mechanical properties of fibrillar proteins measured?
By stretching the tissue (applying tensile force) which can be plotted on a stess-strain curve.
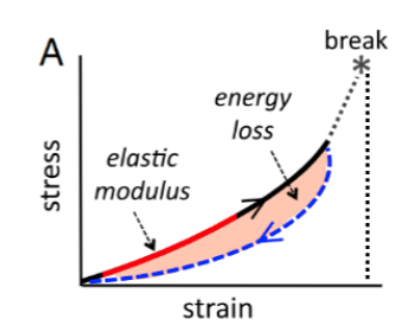
Stress-Strain Curve
Extension (strain) is measured with applied force (stress). Young’s Modulus (gradient – linear region, aka elastic modulus) as a measure of ‘stretchiness’ of a tissue.
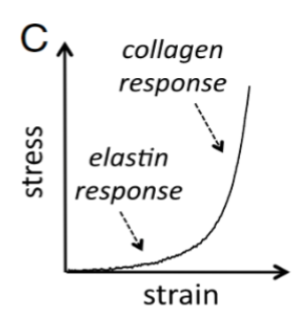
Collagen and Elastin Plotted on a Stress-Strain Curve
5 Steps of the Cardiac Cycle
The hearts cardiac cycle can be broken down into five steps that can then be grouped into: systole (state of contraction) and diastole (state of relaxation - ⅔ time spent in diastole)
Late Diastole
Both sets of chambers are relaxed and ventricles fill passively (note this stage starts with already about 65mL of blood in the left ventricle - it is never empty).
Atrial Systole
Atrial contraction forces a small amount of additional blood into ventricles
Isovolumic Ventricular Contraction
First phase of ventricular contraction which pushes AV valves closed but does not create enough pressure to open the semilunar valves.
Ventricular Ejection
As ventricular pressure rises (to about 80 mm Hg) and exceeds pressure in the arteries, the semilunar valves open and blood is ejected (get to end systolic volume (ESV).
Isovolumic Ventricular Relaxation
As ventricles relax, pressure in ventricles falls. Blood flows back into the cusps of semilunar valves and snaps them closed.
Sino Atrial (SA) Node
“Pacemaker” myocytes with unstable membrane potential capable of spontaneous depolarization. Action potential conduction velocity ~1 m/s. Never reaches a flat line on graph = unstable.
Atrioventricular (AV) Node
Electrically connects atria to the ventricles. AV node slows the action potential conduction velocity to 0.05 m/s to allow time for atria to contract.
Bundle of His and Purkinje Fibres
Conduct the electrical potential through the entire ventricle. Action potential conduction velocity 3-5 m/s.
if and iba Ion Channels in Cardiomyocytes
Supply inward depolarizing current (Na+) during initial part of pacemaker potential.
iNa-Cab Ion Channels in Cardiomyocytes
Important contribution to later part of pacemaker depolarization by providing inward flow of Na+.
iCa Ion Channels in Cardiomyocytes
Contribute to last third of pacemaker potential and generates slow-rising action potential by inward movement of Ca2+.
iKv Ion Channels in Cardiomyocytes
Delayed rectifier, voltage-operated channel that supplies decaying current during pacemaker potential and also supplies repolarization current via outward movement of K+.
Myocardial Autorhythmic Cells
Also known as pacemaker cells and the heart beats rhythmically from action potentials they generate. Speed of depolarisation sets the heart beat and can be altered. Resting membrane potential of a myocyte is -80 to -90 mV.
2 Main Types of Heart Cells
Myocardial Contractile Cells (approx. 99%): They are responsible for contracting and relaxing to pump blood throughout the body.
Myocardial Autorhythmic Cells (approx. 1%): They initiate and propagate electrical signals, setting the heart's rhythm and coordinating contractions
How to measure the activity of ion channels?
Using electrophysiology - patch clamp. Can do single channel or whole cell recordings.
Organisation of Sarcomeres
Myocyte is packed with contractile bundles called myofibrils (1 μm wide). Myofibril is composed of contractile units called sarcomeres.
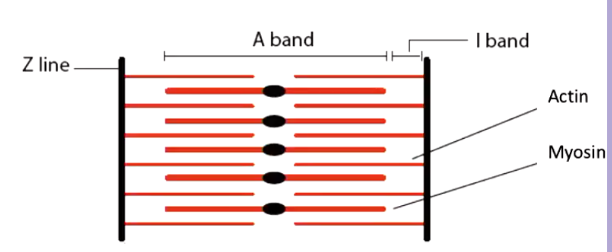
Sarcomeres
Are 1.8-2.0 μm in length and consist of two filamentous proteins between two thin partitions (Z Lines). Thick myosin bands occupy the centre of the sarcomere arranged in parallel (A band). Thin actin bands are rooted in the Z line (I band) and then cross over the myosin filaments into the A band. On the sarcolemma, at each Z line are transverse tubules (T-tubules).
Contraction of Sarcomeres
Contraction occurs when actin slides into spaces between myosin. I band shortens but A band does not. Crossbridge cycling mediates constriction and occurs in three stages.
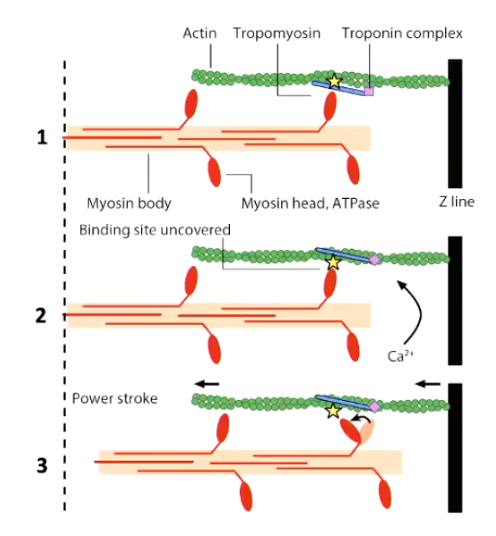
Crossbridge Cycling
Rest: Actin-binding sites (yellow star) are blocked
Binding site exposed: Ca2+ displaces troponin-tropomyosin complex
Flexion: the myosin head flexes towards the centre of the sarcomere pulling the Z line with it
Contractile Force and Energy Source
Contractile force is determined by the number of cross-bridges formed
ATP provides the energy for the flexion
Mitochondria occupy 30-35% of the cell volume of myocytes to provide the ATP
Pre-Load
The stretch of myocardium or end-diastolic volume of the ventricles.
Frank-Starling and Length-Tension Relation
Increasing preload increases the contractile force upon stimulation. i.e. The more stretched the sarcomere in cardiac muscle, the more sensitive it is to Ca2+ and the more force it produces.
Effect of Adrenaline on Contraction
Increases calcium in intracellular calcium and increase in the calcium stores as well. This increases heart rate, contraction force, and speed of contraction.
Effect of Endothelin-1 on Contraction
IP3 is produced which binds to IP3 receptors on the SR, stimulating calcium release. DAG activates PKC which increases the opening probability of L-type calcium channels.
Effect of Caffeine on Contraction
At high doses, caffeine can activate Ca2+ release from SR via ryanodine receptors
At lower concentrations, caffeine can inhibit phosphodiesterase’s (PDE’s) and thus increase free cAMP
Caffeine can also inhibit IP3 and adenosine receptors at mM concentrations
Effect of Ouabain on Contraction
Inhibits the Na+/K+ pump, this keeps Na+ inside the cell. Na+ gradient regulates Ca2+ exchangers and voltage regulated Ca2+ channels
Features of Vascular Smooth Muscle
Actin and myosin structures are very different to cardiac myocytes
Troponin not present, instead constriction dependent on phosphorylation
SR Ca2+ store accounts for 1-4% of cell
SR have inositol 1,4,5 triphosphate receptors and ryanodine receptors
Myogenic Tone
Maintenance of a continuous, baseline level of tension of arteries by SMCs. Resistance arteries sense pressure and respond with constriction. Vascular smooth muscles depolarize and voltage gated Ca2+ channels open. Artery contracts against pressure reducing radius and blood flow with increased wall tension.
Smooth Muscle Membrane Potential and Ion Channels
Membrane potential -60 mV
K+ channels and Na+/K+ exchanger generate the negative potential
Stimulation of the K+ channels mainly contributes to vasodilation
Depolarization opens membrane bound L-Type calcium channels increasing constriction
Constriction can occur independent of depolarization
Calmodulin Role in Smooth Muscle Contraction
Increased calcium leads to calcium binding to calmodulin
Calmodulin activates myosin light chain kinase
Phosphorylated myosin light chain kinase leads to constriction
As an additional pathway myosin light chain is sensitized to calcium stimulation via inhibition of myosin light chain phosphatase
Transcytosis
Transport within the cell
Endothelium
The inner cellular lining of all blood vessels and the lymphatic system and is one cell layer thick. Flat 1-2 μm thick, 10-20 μm in diameter, ‘cobblestone’ appearance.
Tight Intercellular Junctions in Endothelium
Tight intercellular junctions to maintain integrity of the vessel wall. Toxic substances (e.g. nicotine) open up these junctions and allow large molecules to pass through the wall, this can lead to disease.
Pinocytosis/Macropinocytosis
Concentrations of small vesicles adjacent to cell membranes
Transport of solutes and fluid into/across the cell from the blood
Facilitates bulk exchange (gases, metabolites, nutrients and proteins)
Caveolae
A special type of endocytotic/transcytotic vesicle
Contain caveolin, a transmembrane protein associated with receptors, enzymes and ion channels
Caveolin-mediated endocytosis of specific factors (ex. LDL)
Weibel-Palade Bodies
Elongated storage granules specific to endothelial cells
Main cargo = von Willebrand Factor (vWF) monomers
Also contain interleukin (IL)-8, endothelin 1, endothelin-converting enzyme, tissue plasminogen activator (tPA), angiopoietin
EC Arrangement
ECs respond to changes in the blood (biochemical and physical)
ECs are shear sensitive (they need to respond to changes in flow)
More aligned in the direction of flow in arteries compared to veins
SMCs and ECs
SMCs are arranged circumferentially in layers
SMCs need to provide pulsatile force
ECs act as a semipermeable barrier between blood and SMCs
Forces Experienced by Endothelial Cells
Contact-derived stresses: topography (thickness, fibres and pores), curvature, stiffness
Flow-derived stresses: shear stress, pressure, tensile strain
Major Roles of Ecs
Metabolism, barrier integrity, vascular tone, mechanotransduction, injury repair, hemostasis, and angiogenesis.
Vascular Tone
The degree of constriction or contraction of vascular smooth muscle within blood vessel walls relative to their maximum diameter. ECs control vascular tone by responding to various hormones, neurotransmitters and vasoactive factors.