Unit 2: Mastication and Ventilation
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
what structures form the TMJ?
mandibular condyle and mandibular fossa of the temporal bone with a disc that separates two cavities- the inferior between the inferior aspect of the disc and mandibular condyle, and the superior between teh disc and the segment of bone formed by mandibular fossa and articular eminence
what is the mandibular condyle lined with to absorb forces?
a thin layer of fibrocartilage with a more superior reparative process
is the articular surface or the non articular suface of the mandibular fossa more load bearing?
the articular surface
what are the characteristics of the articular and non articular surface of the mandibular fossa?
the articular surface (also known as the articular eminence) is a thick bone lined with fibrocartilage, and the non articular surface is a thin layer of bone and fibrocartilage that occupies much of the superior dome and posterior walls of the fossa
what are the characteristics of the fibrous capsule of the TMJ?
surrounds the TMJ and disc, the internal surfaces are lined with a synovial membrane. the medial and lateral capsule is relatively firm and provide stability during lateral movements, and the anterior and posterior capsule is relatively lax, allowing the condyle and disc to translate forward when mouth is opened
what is the characteristics of the articular disc of the TMJ?
is made of dense fibrocartilage that lacks blood supply and sensory innervation except at the periphery, is divided into 3 regions- posterior, intermediate, and anterior
how is the posterior region of the articular disc contoured and how thick is it?
convex superiorly and concave inferiorly, 2-3 mm
how is the intermediate articular disc contoured and how thick is it?
concave inferiorly and flat superiorly, 1 mm
how is the anterior region of the articular disc contoured and how thick is it?
flat inferiorly and concave superiorly, 2-3 mm
what is the function of the articular disc of the TMJ?
maximizes joint congruency to reduce contact pressure, adds joint stability and helps guide mandibular condyle during movement, slides with the translating condyle and is governed by the intraarticular pressure, muscle forces, and collateral ligament
which ligament stabilizes the lateral side of the TMJ capsule?
the lateral temporomandibular ligament, which is the primary reinforcing ligament.
what can tears of the lateral TM ligament cause?
medial migration of the disc by the superior head of the lateral pterygoid muscle
what are the role of the accessory ligaments (the stylomandibular and sphenomandibular ligaments)?
help to suspend the mandible from the cranium and likely only have a limited dynamic role in mastication
how much motion is available in protrusion/retrusion of the TMJ?
1.25 cm
how much motion is available in lateral excursion of the TMJ?
11 mm
how much motion is available in depression/elevation of the TMJ?
40-50 mm
what is the arthrokinematics of protrusion/retraction of the TMJ joint?
mandibular condyle and disc translate anterior and posteriorly respectively in protrusion and retrusion, with the disc and condyle following the downward slope of the articular eminence, with the mandible sliding slightly downward with protrusion and upward with retrusion
what is the arthrokinematics of lateral excursion of the TMJ?
the condyle and disc perform side to side translation within the fossa that is paired with slight multiplanar rotations typically (lateral excursion is paired with horizontal plane rotation to allow slightly wider arc of motion)
what is the arthrokinematics of depression (opening the mouth) of the TMJ?
in the early phase, see rotation of the mandible relative to the cranium in which the condyle rolls posterior (or is this anterior?) within the concave inferior surface of the disc- stretches the oblique portion of lateral ligament and helps to initial the late phase, which consists of translational movement of the condyle and disc in a forward and inferior direction (to max joint congruency)
what structure within the TMJ prevents excessive/past full opening of the mouth?
tension in the superior retrodiscal lamina, tension also help to initiate the early phase of closing the mouth
what are the arthrokinematics of elevation (closing the mouth) of the TMJ?
first phase includes translational movement, the later phase includes rotation of the condyle within the concavity of disc and is terminated when the upper and lower teeth are in contact
how much of the ROM does the early phase of depression of the TMJ account for?
35-50%
how much of the ROM does the late phase of depression of the TMJ account for?
50-65%
what is the resting and closed packed position of the TMJ?
resting is the mouth slightly open, with the lips together and the teeth not in contact. the closed pack position is with the teeth tightly clenched
what are the muscles of mastication?
masseter, temporalis, medial and lateral pterygoid
what is the function of the masseter?
bilaterally elevated the mandible to brings teeth into contact during mastication and slightly protrudes the mandible, unilaterally produces slight lateral excursion of mandible and is enhanced when the mandible is in a position of contralateral excursion
what is the function of the temporalis?
bilaterally elevates the mandible to produce a biting force, with the oblique posterior fibers elevate and retrude the mandible, unilaterally causes slight ipsilateral excursion of the mandible which is enhanced when muscle is activated from a position of contralateral excursion
what is function of the medial pterygoid
bilaterally elevates and to a limited extent protrudes the mandible, unilaterally produces a very effective contralateral excursion of the mandible, due to oblique line of force
what is the function of the lateral pterygoid?
bilaterally strong protrusion of mandible, unilaterally contralateral excursion of the mandible and rotates the ipsilateral condyle anterior-medially
what is the function of the inferior head of the lateral pterygoid?
is the primary depressor of the mandible and rotates ipsilateral condyle opening the mouth, especially during resisted opening of the mouth
what is function of the superior head of the lateral pterygoid?
helps to control tension within the disc and its position during resistance closure of the jaw, important during resisted, unilateral closure of the jaw (like biting down on a hard piece of candy)
which muscles form a functional sling around the angle of the mandible, assisting in transfer of biting force?
medial pterygoid and masseter muscle
what are the secondary muscles of mastication?
the suprahyoid muscles can assist with depression of the mandible and opening of the mouth, while the infrahyoid muscles stabilize the hyoid bone, are also involved in speech, tongue movement, swallowing, and in control of boluses of food before swallowing
how can an overly depressed scapulothoracic joint theoretically predispose the articular disc of the TMJ to derangement?
by stretching the omohyoid muscle, transferring tension to the hyoid bone and mandible, leading to altered alignment and disc derangement
does resistive mouth closing (as during chewing) or full opening generate larger joint loading or disc compression?
resistive mouth closing
is the superior head of the lateral pterygoid active during mouth opening?
even though it attaches directly to the disc, it is relatively inactive during mouth opening
what are the step in the muscular control of opening the mouth?
the inferior head of the lateral pterygoid contributes to mandibular protrusion, the mandibular condyle rotates due to suprahyoid influences, and gravity assists
during full opening, translating mandibular condyle contacts articular eminence
the disc and the condyle slide forward as a unit during the late phase, the disc is stretched and pulled anteriorly by the translating condyle and the increased intraarticular pressure created by activation of inferior head of the lateral pterygoid
describe the muscular control of closing the mouth
the contraction of the masseter, medial pterygoid, and temporalis muscle creates a favorable moment arm, the mandible translates in a posterior-superior direction and reseats the condyle within fossa at the end of closing phase. the forward tension of the disc and neck of the mandible by eccentric activation of the superior head of lateral pterygoid in which the tension helps to position the disc between the condyle and articular eminence, and balances the retrusion force by the posterior fibers of temporalis
what is the primary difference in the functional demands placed on the dome of the mandibular fossa and the articular eminence of the temporal bone during chewing?
the dome of the mandibular fossa experiences small demands, wherease the articular eminence experiences large demands, which are reduced by the coordinated action of the articular disc
what is ventilation?
the mechanical process (occurring 12-20 times per minute) by which air is inhaled and exhaled through lungs and airways
what is the difference between quiet ventilation and forced ventilation?
quiet occur during sedentary activities with low metabolic demands, and forced occurs during strenuous activities requiring rapid and voluminous exchange of air, such as exercising
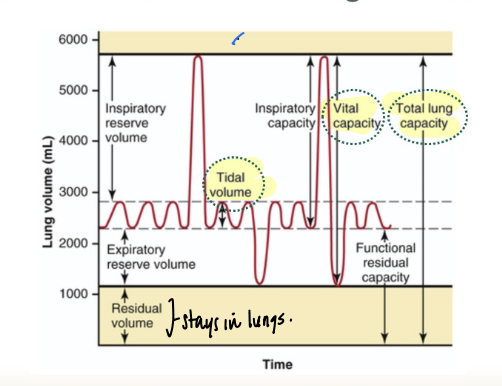
what are the important lung volumes?
tidal volume (which is the volume of air moved in and out of the lungs during the ventilation cycle- approx 0.5L), the vital capacity (which is the total volume of air that can be forcibly exhaled after a maximum inhalation), and residual volume (the volume of air remaining in the lungs after a maximal exhalation)
how does inspiration occur?
the intrathoracic volume is increased by contraction of muscles that attach to the ribs and sternum- the thorax expands, pressure within the interpleural space is reduced which creates suction that expands the lungs, the expansion of the lungs reduces the alveolar pressure below atmospheric pressure, ultimately drawing air into the lungs
how does expiration occur?
reduction of the intrathoracic volume increase alveolar pressure, driving air out of the lungs, when quietly is a passive process that does not depend on active muscle activation but relaxation of inspiratory muscles and elastic recoil of the lungs, thorax, and connective tissues of the stretch inspiratory muscles
what does forced expiration require?
active forced produced by the expiratory muscles such as the abdominals
what structures seal the inferior and superior poles of the thoracic cavities?
the diaphragm seals the thoracic cavity inferiorly, and the upper ribs, clavicles, cervical fascia, and cervical muscles seal it superiorly
which joints are involved in respiration?
manubriosternal joint (before ossification in late life), sternocostal joints, interchondral joints, costovertebral joints (costocoproreal and costotransverse), thoracic intervertebral joints (interbody joints and apophyseal joints)
what vertical changes do you see in the thorax with inspiration and expiration?
with inspiration, see increase in vertical diameter of the thorax with the contraction and lowering of the diaphragm, with quiet expiration, see the dome recoiling back to the resting postion (vertical diameter shrinks back)
what antero-posterior and medial-lateral changes do you see with inspiration?
primarily due to the costovertebral joints, in inspiration see the elevation of the ribs so that they lie parallel with the associated transverse processes (like a bucket handle), and with forced inspiration also see slight extension of the thoracic spine
what antero-posterior and medial-lateral changes do you see with expiration?
with expiration see the pump handle lower back down (returning to original position), with forced expiration, see some motion of the ribs with slight flexion of the thoracic spine
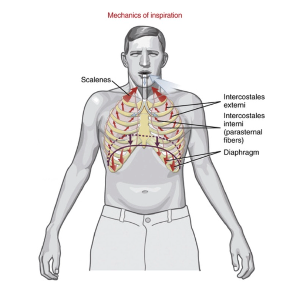
what are the muscles of quiet inspiration?
the diaphragm, scalenes, intercostales
which is the primary muscle of inspiration (most important)?
the diaphragm since it performs 60-80% of the ventilatory process
what is the primary and secondary role of the diaphragm?
primary is to lower and flatter to increase the vertical diameter of the thorax and facilitate inspiration, secondary is to aid in stabilization of the trunk since its lowering is resisted by the abdomen and stabilizes the dome as well
how many cm of movement occurs in the diaphragm with quiet inspiration vs forced inspiration?
drops down 1.5 cm vs 6-10 cm
to what level does the diaphragm drop down to with maximum inspiration?
right side descends to about T11, left to T12 (the right side is inhibited by the liver)
what is the role of the scalenes in inspiration?
if the cervical spine is well stabilized, bilateral contraction increases the intrathoracic volume by elevating the upper ribs and sternum (active during every inspiration cycle
what is the role of the intercostales in inspiration?
external intercostals directly drive inspiration, wherease the internals will help to stabilize the intercostal space to prevent inward collapse of the thoracic wall, as well as driving forced expiration
what are the additional muscles of forced inspiration?
serratus posterior superior and inferior, levator costarum (elevates the ribs), sternocleidomastoid, latissimus dorsi, iliocostalis thoracic and cervis (extends the back), pectoralis minor, pectoralis major, and quadratum lumborum (stabilizes the lower ribs during early forces inspiration)
what are the muscles of forced expiration?
the abdominal muscles (rectus abdominus, transversus abdominis, external and internal obliques), transversus thoracis, intercostales interni (interosseus fibers), passive recoil of the diaphragm
how much volume of air is released in quiet expiration normally?
500 mL