parasitology midterm 2
1/72
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
73 Terms
entamoeba lifecycle
mature cysts ingested, excystation to troph form, troph multiplies into more trophs or into cysts, cyst and troph excreted in feces
entamoeba transmission
ingestion of cysts in contaminated food or water, cysts survive days-week, 1 cyst makes 4 trophs
entamoeba trophozoite
found in diarrheal stool: single nucleus with central karyosome and peripheral chromatin, ground glass cytoplasm
E. histo: erythrophagocytosis
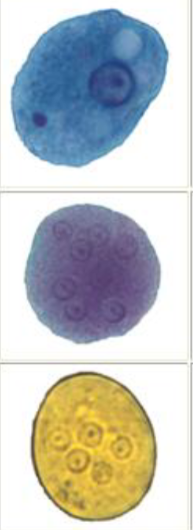
entamoeba cyst
found in formed stool: four nuclei and chromatid body, nucleic acids look like dense rod, size of monocyte
entamoeba laboratory detection
R/O with 3x stool exam, fecal EIA adjunct to microscopy, PCR, EIA for extraintestinal disease
entamoeba treatment and prevention
water treatment: iodination or boiling, chlorination doesn’t work
asymptomatic: eradicate cysts
symptomatic: eradicate trophs with metronidazole then with asymptomatic treatment
E. histolytica doesn’t respond to tetracycline
entaemoeba hartmanni
small E. histo: chromatid bodies with compact karyosome

Entamoeba coli
Large, cyst form >4 nuclei, troph form has large karyosome and vacuolated/dirty cytoplasm
entamoeba polecki
many small pointed/angular chromatid bodies

Entamoeba nana
cyst form has 4 nuclei and lacks peripheral chromatin
troph form has blot like karyosome with granular or vacuolated cytoplasm

Iodamoeba beutschlii
cyst has one large glycogen vacuole, troph is slluggish with large central karyosome

Dientamoeba fragilis
flagellate with no cyst stage, symptomatic and asymptomatic infections possible
balantidium coli
ciliated protozoa that transitions between cyst and troph form
balantidium life cycle
ingestion of contaminated food or water/fecal oral, pigs are reservoir
balantidium disease
dysentery, can be invasive and form colonic ulcers, responds to tetracycline
balantidium coli morphology
large(220-400um), ciliated with kidney bean nucleus, cysts often not seen
Giardia life cycle
1: ingestion of contaminated food or water
2: 1 cyst makes 2 trophs that replicate via longitudinal binary fission
giardia infectivity
cysts are infectious shortly after passage and can survive months in cold water, person-person is possible, if trophs are ingested then no disease/asymptomatic
humans are crucial reservoir and can be asymptomatic carriers
giardia disease
causes non invasive inflammation of jejunum
acute: watery/fatty stools
chronic: fat malabsorption syndrome, loss of vit A,D,E,K can leads to stunted growth or rickets
giardia diagnosis
weird face thing, falling leaf motility
O and P, EIA/RDT kits, PCR
do not use concentrates
giardia treatment and prevention
metronidazole, water treatment with iodination, have good hygiene
trichomonas vaginalis
flagellated protozoan specific to humans, spread through sexual contact
trichomonas vaginalis life cycle
no cyst stage, relies on sexual transmission, resides in female lower genital tract and male urethra/prostate, replicates by binary fission, troph form cannot survive in environment, spreads through sexual contact
trichomonas vaginalis symptoms
Females: more symptomatic, can lead to PID, persists
Males: more asymptomatic, rarely urethritis, epididymitis, prostatitis
neonates: congenital, rare involvement of lung
trichomonas vaginalis morphology
flagella, undulating membrane, twitching motility under wet mount
trichomonas vaginalis diagnosis
wet mount not recommended due to poor sensitivity, must be done <20min
gold standard: anerobic culture, but slow/labor intensive
preferred method is PCR
trichomonas vaginalis treatment and prevention
do whole STD/I panel, safe practices, treat under medical supervision and include all partners of infected person, can treat with metronidazole
taenia saginata/solium lifecycle
Humans: ingestion of raw or undercooked infected meat/muscle tissue with cysticerci, scolex attaches to intestine, adult worm releases eggs/gravid proglottids in feces
intermediate host: cattle and pigs infected by ingesting contaminated vegetation, oncospheres hatch and penetrate intestinal wall, oncospheres circulate and develop into cysticerci in muscle tissue
cysticercosis
T. solium eggs ingested by human hosts, oncospheres hatch and penetrate intestinal wall and circulate to muscle tissue, cysticerci can develop in any organ(brain, eyes, subcutaeneous tissue)
taenia vector
T. saginata: cow
T. solium: pig
taenia disease
eggs can calcify in tissue and rupture later
T. solium: propensity to make cysticerci in brain
T. saginata: no cysticerci in humans
cysticercosis: larvae form cysts in humans
taenia morphology
4 suckers
T. solium: rostellar hooks, proglottid is thinner and more branched
T. saginata: no rostellum, proglottid thicker and less branched
taenia diagnosis
take extreme care in processing specimen, ingestion can cause cystercerosis
O and P: eggs are indistinguishable, usually don’t see proglottid, hooks indicate cestode, differentiate species by striations in eggs
taenia prevention and treatment
post mortem inspection of swine carcass by USDA, stop coprophagia, cook food
treat humans with praziquantel
Echinococcus granulosus/multilocularis definitive hosts
Dogs/canidae, multi(foxes, dogs, cats)
Echinococcus granulosus/multilocularis Intermediate host
Granulosus: sheep, goats, swine, wild herbivores
multilocularis: rodents
Humans are dead end host
diphyllobrothriid(fish tapeworms) lifecycle
unembryonated eggs passed in feces of definitive host, eggs embyronated in water, intermediate host facilitates larvae maturation, infected crustacean ingested by second intermediate host, predator fish eats smaller fish, definitive host ingests plerocercoids in infected fish
fish tapeworm hosts
definitive host: fish eating mammal
intermediate host 1 is crustacean
intermediate host 2 is freshwater fish
fish tapeworm disease
tapeworm absorbs huge quantities of vitb12 which leads to anemia
fish tapeworm morphology
really long(>30ft), width>length of proglottid compared to taenia, “mind the knob”
fish tapeworm prevention
proper cooking/freezing of fish
eneterobius vermincularis(pinworm) lifecycle
embryonated eggs ingested, adult worm lays eggs in gut, mature female worm migrates out of anus and lays eggs at night
eneterobius vermincularis(pinworm) morphology
nematodes: males are curlier and females are longer with tapered ends
enterobius diagnosis
sample collected with clear tape or paddle
enterobius prevention
wash linens, treat family, trim fingernails
enterobius disease
eggs are immediately infectious and easily cause autoinfection/reinfection, causes peri-anal itching
trichuris trichiura(whipworm) lifecycle
embryonated eggs ingested, larvae hatch in small intestine, adults reside in cecum and lay eggs that pass in feces, eggs 15-20 days in soil before development
whipworm(trichuris) disease in normal host
cecum colonized, mostly asymptomatic, coinfections common, can cause malabsorption or inflammation
whipworm(trichuris) disease in compromised kids
severe chronic diarrhea, tenesmus, abd pain, rectal prolapse, allergic manifestations(eosinophilia)
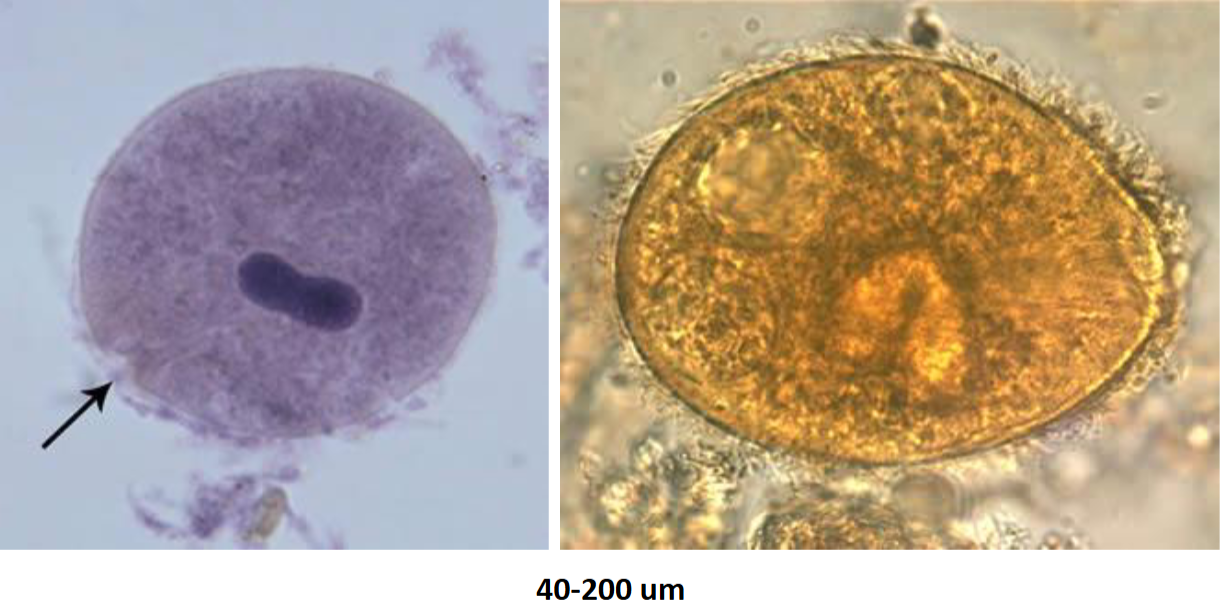
whipworm(trichurius) egg morphology
unembryonated: thick wall with hyaline polar plugs
lookalike: capillaria has striated shell and less prominent polar plugs
ascaris lumbricoides lifecycle
mature eggs release larvae, larvae penetrate GI mucosa, extra GI migration to liver then lungs, cross epiglottis and re enter GI tract, egg laying adults months after exposure
ascaris lumbicoides transmission
common in soil eaters(pica) and kids, love openings, eggs take 18 days to be infectious
ascaris disease
asymptomatic, may crawl out if high fever
worm may migrate to lungs for high O2 and cause pneumonia
may ascend to liver causing jaundice, inflammation
can cause pancreatic block or acute GI blockage
ascaris treatment
deworming with mebendazole/albendazole: binds to beta tubulin and prevents microtubule polymerization, adult worm dies
treatment for 1-3 days
ascaris egg morphology
unfertilized egg: mammalated
fertilized egg: mammalated with curled worm inside
decrotication: loss of outer layer
hookworms
new world: necator americanus
old world: anclyostoma duodenale
hookworm lifecycle
flariform larva penetrates skin, moves from subcutaenous venules to lymphatics and into circulation, enter lungs and cross epiglottis, reaches GI tract, adults 5-9 weeks post exposure
hookworm transmission
resides in small intestines and penetrates bare feet
questing: flariform larvae on blades of grass
hookworm disease
acquired iron deficiency anemia, severity directly correlated to number of parasites, can impair physical/intellectual developement
hookworm morphology
rhabitiform larvae not normally found in stool, must RO strongyloides
old world: sharp teeth
new world: cutting plates
hookworm treatment and prevention
avoid going barefoot, sanitary sewers, educational/deworming campaigns
treat with albendazole
strongyloides lifecycle
flariform larvae penetrate skin and enter circulatory system, transported to lungs and penetrate alveolar spaces, carried to throat and swallowed into small intestine where they become adults, female worm parthogenesis in intestine and can autoinfect, rhabitiform larvae in intestine excreted in stool
stronglyoides signal searching
humans are principle reservoir
non specific signals: CO2, NaCl
specific signals: urocanic acid 5x on foot vs other body parts
strongyloides hyperinfection disease
risk for immunosuppression or HTLV(not HIV): occurs when accelerated autoinfection tremendously increases worm burden
massive tissue invasion leads to malnutrition, hypoproteinemia, polymicrobial infections, septicemia, high mortality
strongyloides disease in normal host
asymptomatic autoinfection up to 40yrs
acute migratory phase induces respiratory symptoms, eosinophilic pulmonary infiltrates(loffler’s)
chronic: digestive issues with minimal inflammation or abd pain
strongyloides morphology
short and sexy, short buccal canal with prominent genital primordium
strongyloides diagnosis
3 O and P for rhabditiform larvae: seldom see eggs
stool concentration important, stool culture for larvae tracks/gliding
strongyloides treatment and prevention
careful with steroid reaction, don’t go barefoot, proper hygiene/sanitation
ivermectin, nasal thiabendazole for hyperinfection
trichinella spiralis(and others) lifecycle
two lifecycles: domestic and sylvatic, humans are dead end hosts
ingestion of uncooked meat, larvae released in small intestine and mature into adults, reside in small intestine >1mo, larvae deposited in mucosa, encysted larvae in striated muscle tissue
trichinella spiralis diagnosis
mainly clinical diagnosis: muscle biopsy, serology, peripheral blood eosinophilia up to 90%
can see curled organism in muscle tissue
trichinella spiralis treatment and prevention
prevent cyst formation(in small intestine >1mo): heat 76.6C for 4min or freeze-29C for 10days, do not microwave, do not freeze T.nativa
USDA prohibits feeding raw meat scraps to hogs
anisakis(sushi parasite) lifecycle
marine mammals excrete unembryonated eggs, eggs embryonated in water, larvae hatch from eggs(free-swimming), larvae ingested by crustacean and mature into L3 larvae, infected crustacean eaten by fish and squid, infected fish or squid ingested by marine/human mammals
anisakis diagnosis
gastroscopic examination