CS Master Deck Final
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
24 Terms
Appendicitis HYC
Pathology: Fecalith (adult / lymphoid hyperplasia (children)
Pain:
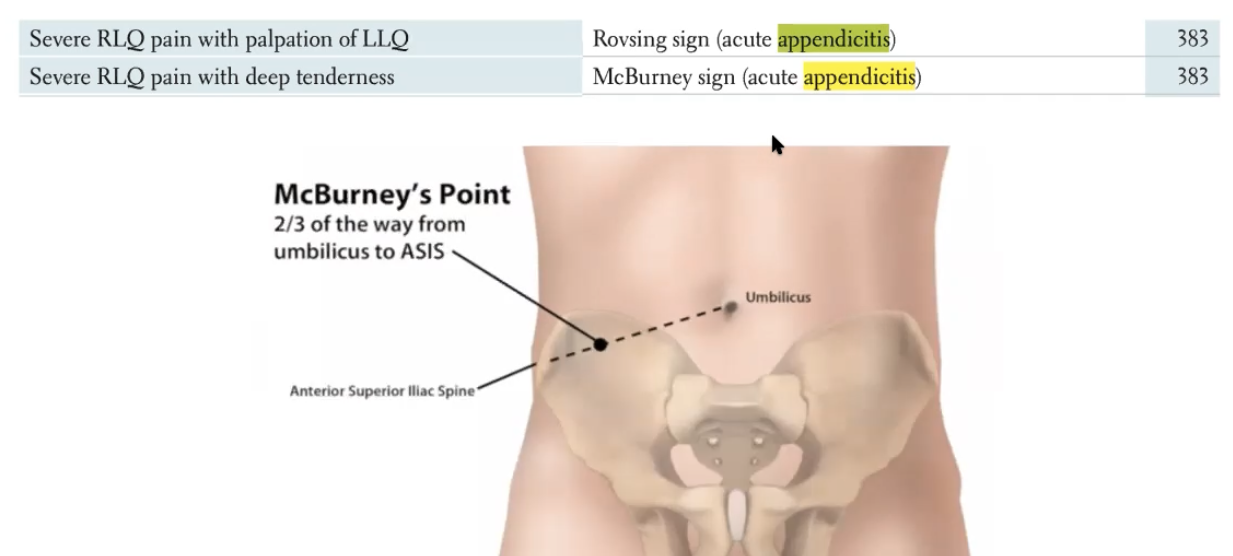
Peri-umbilical pain —→ Mcburneys point (2/3 from BB to ASIS)
Rovsing sign —> rebounding sign with palpation of the LLQ —> pain in the RLQ
Sxs: Nausea, vomiting, no appitite, + G/R/R
Tx: Clinical —-» CT abdomen/US (from children or pregnant women), Boards—→ always surgery
Chapman point (HY): Tip of the 12th rib, right side
DDx:
Think about bladder pain ie UTI or kidney stone(more central pain)
ovary/tubes/uteruses ie torsion, cysts, PID (pelvis inflammatory disorder via gonorrhea/chlamydia travel through pelvis to pariteum) ectopic pregnancy
other ie hernia, diverticulitis (usually on left, elderly)
Pseudoappendicitis - Yersinia enterocolitica (think viral gastroenteritis infection can cause RLQ pain)
Uses this to ask target questions: LMP, back pain, ovulation (mittelschmerz pain —→middle hurts, peritoneal irritation (follicular, swelling, fallopian tube contraction), urination issues, sexual history (ie STD)
Peptic Ulcer Disease HYC
Dyspepsia
DDx
Alarm Sxs
Pertinent positives and negatives
Locations of ulcer
Pathology
Types of ulcers
Sxs
Dx
Tx:
Complications
Dyspepsia
Burning pain in epigastric area (25 percent population have this at any given time)
DDx: Peptic ulcer disease, GERD, cancer, gastritis, pancreatitis, functional dyspepsia (no specific Sxs)
Alarm Sxs: Age > 50, melena (dark stool), anorexia —→ straight to EGD —> biopsy (via endoscopy)
Pertinent positives and negatives:
GERD - sour taste/burps, worst after big meal or after laying down, burning/gnawing, smoking and drinking Hx, NSAID/steroid use
Locations of ulcer: Stomach or duodenum
Gastric - worse with food
Duodenum - initially better with food but worse in 1-3 hours.
Pathology: H Pylori (also causes gastritis), NSAID
Types of ulcers:
Curling ulcers - burns
Cushing ulcers - increased ICP/vents (think chronic sick patients get ulcers)
Sxs:
Gnawing pain, 50 percent asymptomatic
Dx: EGD, Bx —→ breath test (most common)
Tx:
No spicy foods/nsaids/smoking/drinking, proton pump inhibitors or H2 blocker or tums
Triple therapy 2 antibiotics + proton pump inhibitor
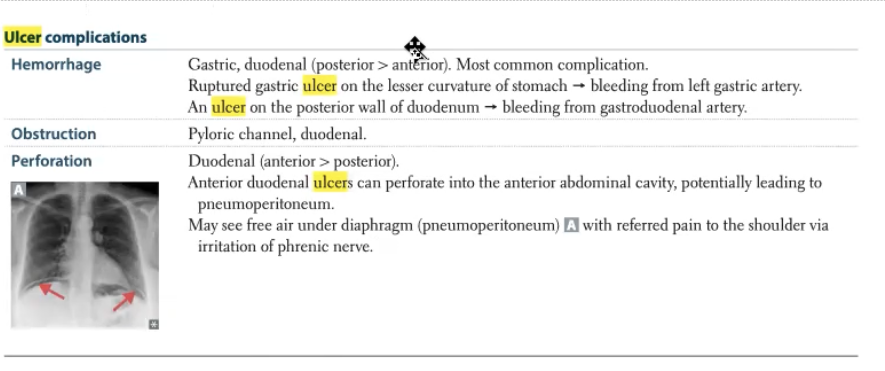
Complications:
Makes hole—> food and into intraperitoneal cavity —→ rigid acute abdomen;
bleed and hemorrhage —> anemia
***Can develop maltoma ie H Pylori is carcinogenic
Hypothyroid HYC
Thyroid cascade
T4 functions
Sxs
DDx
Test
Tx
Complications
Thyroid cascade: TRH (hypothalamus) —> TSH (ant pit) —> T4 (thyroid)
T4 inh TRH and TSH if (T4) is high, visa vera if low
TSH is used as our screening test, also used during treatment for adjustments (tells us how the body is doing)
If TSH is low then T4 is high, so low TSH is associated with hyperthyroidism, so high TSH is associated with hypothyroidism
T4 functions: Movement, metabolism, mentation
Sxs: Weight gain, constipation, bradycardia, decreased DTRs (hyporeflexia), cold, fatigue, depression
DDx: Hashimoto's thyroiditis (antibodies attacking thyroid, autoimmune)
Test: TPO antibody (for Hashimoto's)
Tx: Synthroid or levothyroxine (monitor TSH levels to know how much)
Complications: Myxedema coma
Coma
Hypothermia —→ hypotensive
Tx: Warm IV fluids, blankets, IV T 3/4
Hyperthyroid HYC
Sxs
Labs
Tests
DDx
Tx
Thyroid Storm
Sxs: Diarrhea, tachycardia —> afib, weight loss, heat intolerance, increased DTRs, anxiety
Labs: TSH will be low, T4 will be high
Tests: RAIU scan —> light up areas are actively making T4
DDx:
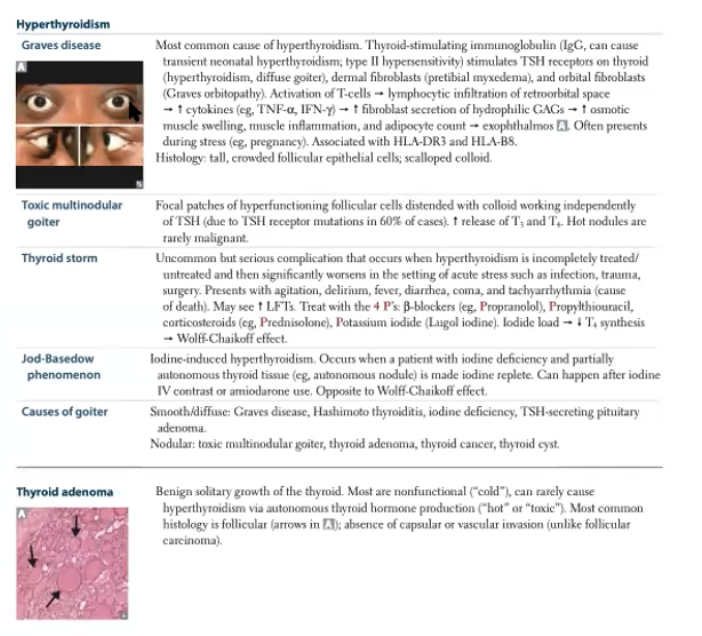
Graves disease (autoimmune, antibodies(TSI) attack and tell the thyroid to grow big); whole areas will glow with RAIU —> whole thyroid making T4
Toxic adenoma (one nodule growing) or MNG (multi nodular goiter) —> RAIU shows one or 4 light up (Tx surgery or radioablation)
thyroiditis (inflamed so spilling T4, can go back to normal or burn out which leads to hypothyroidism) —> associated with postpartum/viral, RAIU is negative (cold scan, not actively up taking iodine, T4 is high so TSH turns off thyroid)
Sxs: Exophthalmos, pre-tibial myxedema
Tx: thioamides (decreased T4, used in thyroid storm)
Thyroid Storm: severe tachycardia and/or afib (leads to hemodynamic unstably), shock, febrile (>104),
Tx cold fluids, beta blocks, thioamides
Ectopic Pregnancy HYC
Definition
Risk factors
Clinical presentation
DDx:
Diagnosis
Management
Follow up
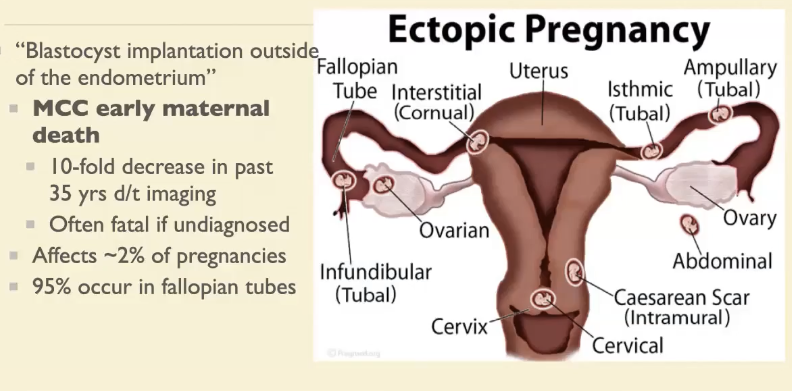
Definition: Blastocyst implantation outside of the endometrium
MCC early maternal death (10 fold decrease in last 35 yers d/t imaging)
~2% of pregnancies, 95% in fallopian tube
Risk factors
Previous ectopic pregnancy (top risk factor), previous tubal surgery, Hx of infertility, endometriosis, PID (Hx of STD ie chalmydia), smoking (decrease motility), age
Clinical presentation
Early preg. Sxs less common due to lower hormone levels
Suspect in reproductive age w vaginal bleeding and/or pain
No confirmed intrauterine preg, amenorrhea > 4 weeks
Hx of conception with IVF
Hemodynamically unstable w acute abdomen, no obvious source
DDx:
Normal pregnancy (implantation bleeding)
Abortion (threatened, inevitable, complete)
Cervical, vaginal, uterine (laceration, infection ,polyps, subchorionic hematoma)
Gestational trophoblastic disease (associated with high bHCG)
Other ie UTI, nephrolithiasis, appendicitis, ovarian pathology/mass, round ligament pain
Diagnosis
Transvaginal ultrasound more sensitive than transabdominal
No intrauterine preg and ring of fire
Extrauterine gestational sac, adnexal mass
intraperitoneal bleeding (free fluid, coagulates)
Gold standard —→ Dx with laparoscopy
Rare —> heterotopic pregnancy (both intrauterine and one ectopic)
US and HcG levels used for diagnosis
Transvaginal 1500-2000 HcG should be seen with IUP
Transabdominal above 5000 HcG should be seen on IUP
bHcG should double q48hours (if pt is stable and preg is unknown location) —> then can repeat ultrasound (ie 1500 on Monday should be 3000 on Wednesday)
Management
Methotrexate
Inhibits folate synthesis (stop prenatal vitamins), multiple dosaging regimens, Follow LFTs, bHCG until zero, reverse w leucovorin
Indications: Asymptomatic compliant pt (needs to follow up for HCG labs), bHCG < 5000, unruptured sac, no fetal cardiac activity, size < 4cm
Surgical
Indications: non compliant ( no f/u), hemodynamically unstable, desires surgery
Laparoscopy vs laparotomy
Depends on hemodynamic factors, possible to preserve fertility w salpingostomy
Follow up
More likely to have another one now, resolution of preg needs to be confirmed w neg preg test (before becoming preg again), counsel on future preg and offer BC if no desire to become preg in future
Seizure HYC
Medical Jurisprudence
Definition of death
Upper brain death
Organ donation
Definition of death
Historical criteria: when an individual’s cardiac and pulmonary function cease
Modern criteria, as defined in the Uniform Determination of Death Act (1981):
“An individual who has sustained either irreversible cessation of circulatory and respiratory functions or irreversible cessation of all functions of the entire brain
Including the brainstem, is dead. A determination of death must be made in accordance with accepted medical standards.”
Whole Brain Death: functioning of the entire brain ceases, including the brain stem
Upper brain death
Persistent Vegetative State (PVS): When an individual has irreversibly lost all cognitive function. Not considered to meet the standard criterions of death in any states
Organ Procurement for Transplantation: Allowing neurological criteria to determine death increases the availability of viable donor organs
Organ donation
Uniform Anatomical Gift Act
Regulates posthumous organ donation
Competent adults may gift their organs in advance of death (or by a proxy decision-maker at time of death death) for education and research, as well as for transplantation
National Organ Transplant Act
Established the Organ Procurement and Transplantation Network (OPTN) in the attempt to better allocate organ donations to recipients. Banned the sale of organs (exceptions apply, i.e., blood, sperm, oocytes)
Organ Procurement
Post-Mortem: authorization must be given to gift organs
Living Persons: may donate renewable tissues or those in abundant supply, or gift non-essential organ
Organ Allocation
OPTN: oversees organ procurement and allocation for organ transplantation in U.S.
United Network of Organ Sharing (UNOS): nonprofit organization tasked with managing OPTN
Transplant centers
Each individual transplant center applies its own criteria in determining waitlist eligibility
Factors considered for eligibility can include expected quality of life after transplant, likelihood of successful surgery, length of time the transplant is expected to benefit the recipient (+geographic zone)
Medical Jurisprudence
Capacity v. Competence
Decision making authority: Living Wills vs Durable Power of Attorney for Healthcare
Capacity
a person’s ability to freely make and communicate their health care decisions.
Patient must: understand information provided about their health care decision, clearly communicate their choice, appreciate and evaluate the facts relating to the decision, display reasoned decision-making
Competence
a legal determination of whether an individual is able to freely make conscious decisions
Decision making authority
Hierarchy: competent patient, advanced healthcare directive, next of kin, ethics committee
Advanced healthcare directive
Living Wills: a legal document describing how an individual wishes medical decisions to be made when they are no longer able to make such decisions for themself
Durable Power of Attorney for Healthcare: a legal document appointing a proxy decision-maker for healthcare decisions for an individual in the event they cannot make their own healthcare decisions
Next of kin
State statutes establish the hierarchy of decision-making authority for next of kin ie Spouse, adult children, parents, adult siblings. Can also include other relatives or close friends dependent on state (if a better option is not available for the patient)
Ethics committee
If a patient does not leave an advance healthcare directive and a surrogate decision-maker cannot be established, then an ethics committee will likely make the healthcare decisions for the patient

Medical Jurisprudence
Discussion making for minors
End of life decision making
Withdraw treatment
Physician aided suicide
Medical Futility
Discussion making for minors
U.S. Supreme Court acknowledged a right for parents to make their own decisions regarding how they raise their children, but the right is subject to reasonable limits
The state may intervene in a parent’s decisions when the health and safety of the child is at risk
End of life decision making
Patient’s Individual Interests ie Personal autonomy/Right to informed consent, Right to privacy
State’s Interests: Ie Preservation of life, Integrity of the medical profession, Suicide prevention, Protection of innocent third-party welfare
Refusals: For competent adults, courts favor preserving a patient’s autonomy over the state’s interests. Courts are disinclined to give the government the authority to choose whose lives should be preserved
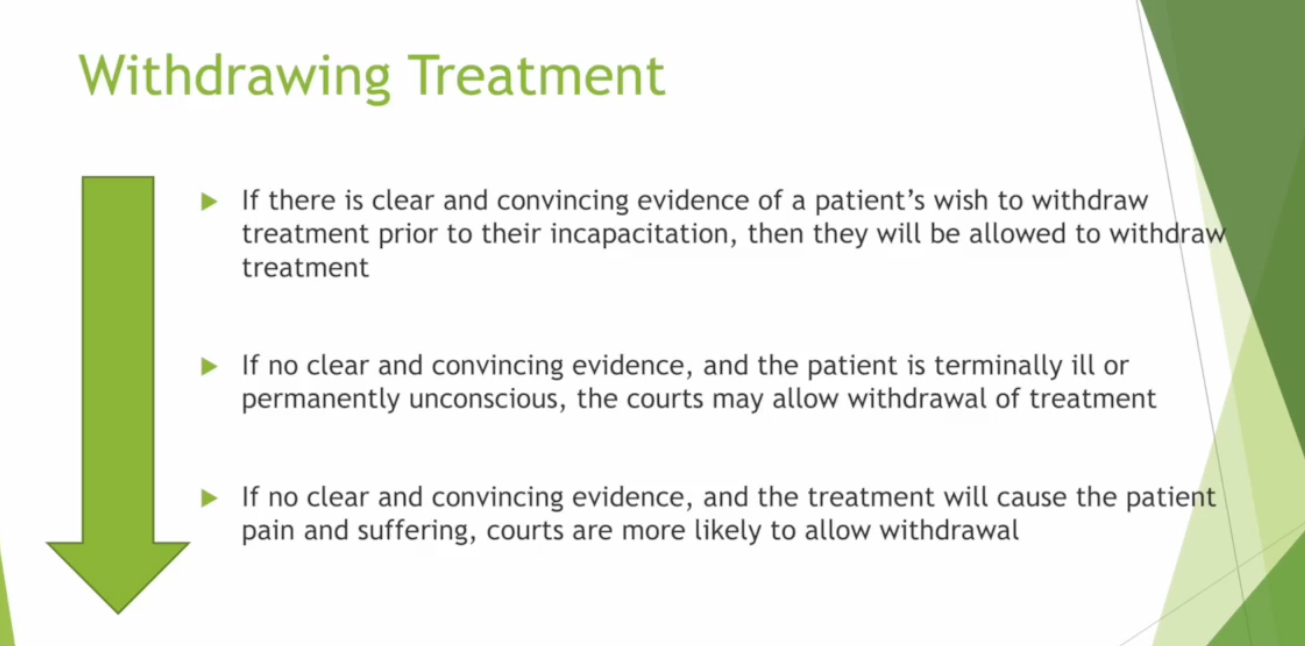
Withdraw treatment
See picture
Withholding vs withdraw
Once deemed more acceptable than withdrawing treatment. Courts also no longer use the extent of a treatment’s invasiveness as a factor in whether the patient may refuse; even minor invasiveness is still deemed to be some form of bodily invasion that a patient may refuse
Physician aided suicide
Competent patient has a right to refuse medical treatment even if doing so may result in death; however, the Supreme Court has decided that there is no right to assistance in dying. 11 states (plus District of Columbia) allow for physician aid in dying, through statute (less than 6 months to live, has to show interest for > 15 days)
Medical Futility
A physician’s determination that a treatment will not provide a benefit to the patient
Two measures used to determine treatment futility:
Qualitative Measure: evaluate whether the treatment would result in sufficient benefit to justify use
Quantitative Measure: evaluate the likelihood the treatment will have the desired effect
Reproductive law
Traditional vs gestational surrogacy arrangements
Contraceptions
Abortions
The United States Supreme Court recognizes:
Right to Privacy (in the bedroom) + Right to Procreate + right to pursue assisted reproduction (Artificial Insemination by Donor, IVF (divorce = potential to become child or custody agreement as seen in court), Surrogacy Arrangements( remember implication with sperm donors, ie will not have parental access unless that is that intent, baby to married woman = husband is the father)
Traditional vs gestational surrogacy arrangements
Traditional: Father sperm + surrogate egg —→ baby (surrogate has to give up right but it is not enforceable / illegal)
Gestational surrogacy —→ surrogate does not provide egg (iffy areas ie birthing mom vs owner of egg)
Contraceptions
The United States Supreme Court recognizes a constitutional right to privacy coupled with a right to choose not to procreate ie right to use of birth control
Defining Cases; Griswold v. Connecticut (1965) (sexual acts vs procreation) and Eisenstadt v. Baird (1972) (right to privacy extends beyond the bed, free from unwanted governmental intrusion to bear a child)
Abortions
The United States Supreme Court does not recognize a constitutional right to abortion
Defining Cases:
Roe v. Wade (1973) (liberty right to pregnancy, if restrictions are put on adoption to interested of state and to serve state interest)
Trimester framework: 1st state couldn’t impose, 2nd state could if imposed to maternal health, 3rd state could regulate abortions due to risk of life of mother or baby
Planned Parenthood of Southeastern Pennsylvania v. Casey (1992) (government could put limitations of abortion as long as it didn’t increase burden to get a abortion)
Dobbs v. Jackson Women’s Health Organization (2022) (up to state to keep regulations)
- Look into nevada leg ************
Occupational Safety and Health Act (OSHA)
Purpose/What does it do?
Clause
Reports
Purpose:
ensure safe and healthy working environments
What does it do?
Sets industry health and safety standards
Enforces established standards
Provides education, training, outreach, and compliance assistance
Clause
Employer must ensure that the workplace is “free from recognized hazards that are causing or are likely to cause death or serious physical harm” to employees
Employer must undertake a hazard assessment of the workplace and put into place procedures to mitigate the risk of an occupational incident
Healthcare Facility Standards:
Bloodborne Pathogens
Hazard Communication
Personal Protective Equipment
Reports
Most violations are precipitated by an employee complaint filed with OSHA
Whistleblower safeguards protect employees from employer retaliation
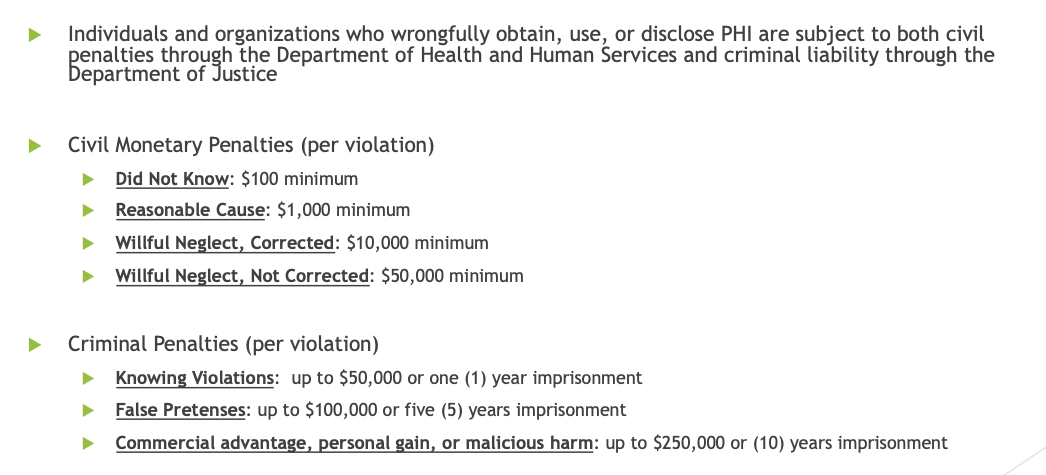
Health Insurance Portability and Accountability Act (HIPAA)
Main Purpose:
To protect patient and health insurance member’s information privacy and prevent disclosure of their protected health information without their consent or knowledge
What does it do?
Privacy Rule: covered entities cannot disclose a patient’s Protected Health Information (PHI) without the patient’s prior written authorization
Covered entities may disclose PHI under two situations (1) to comply with a court order, warrant, subpoena, or administrative request, OR (2) for treatment, payment or other healthcare operations (TPO)
Security Rule: covered entities must implement administrative, physical, and technical measures to protect electronic PHI
Emergency Medical Treatment and Active Labor Act (EMTALA)
False Claims Act
Anti-Kickback Statute
Emergency Medical Treatment and Active Labor Act (EMTALA)
Purpose:
To regulate the duty to treat in emergency or life-endangering situations
What does it do?
Places a ‘duty to treat’ on hospitals (and physicians)
Procedural steps that must be followed:
An individual who arrives at a hospital’s emergency facility must be screened, if the hospital staff determines that an emergency medical condition exists, the individual must be rendered life-saving care until they are stabilized
False Claims Act
Main Purpose:
To protect the government from being defrauded
What does it do?
Imposes civil and criminal liability upon individuals or entities who knowingly deceive or make misrepresentations to the government
Applied to health care, the FCA creates liability for knowingly submitting false or fraudulent claims to government-funded medical programs
Violators may be fined up to three (3) times the government’s loss, plus a penalty between $5,500 - $11,000 per false claim filed
Anti-Kickback Statute
Main Purpose:
To protect patients from having their treatment decisions be influenced by a providers’ potential financial gain and self-interest
What does it do?
Illegal to offer “remuneration” to generate or reward patient referrals or increased business involving any good or service paid by government-funded programs
Remuneration is anything of value and can include meals, hotel stays, cash, excessive compensation, etc.
Liability on both sides, Intent is a key element to liability under the statute; illegal to pay remuneration when the payments are intended to reward or induce an increase in health care business
Results in Fines, Jail sentences, and Exclusion from participation in the Federal health care programs

Physician Self-Referral Law (Stark Law)
Exclusion Statute
Civil Monetary Penalties Law
Physician Self-Referral Law (Stark Law)
Purpose?
To prevent health care fraud and a provider’s referral decisions being motivated by self-interest and self-gain
What does it do?
Physicians cannot make referrals to to entities with which the physician or physician’s immediate family member has a financial relationship
Applies to referrals for designated health services paid by Medicare
Exclusion Statute
If an individual or entity has been convicted of certain criminal offenses, they are required to be excluded from participating in all federal health care programs
Convictions leading to exclusion:
Medicare or Medicaid fraud, as well as any other offenses related to the delivery of items or services under Medicare or Medicaid
patient abuse or neglect
felony convictions for other health-care-related fraud, theft, or other financial misconduct
felony convictions for unlawful manufacture, distribution, prescription, or dispensing of controlled substances
Civil Monetary Penalties Law
The Office of Inspector General may seek civil monetary penalties, assessments, or Federal program exclusion from individuals or entities for engaging in prohibited conduct
Prohibited conduct that invokes Civil Monetary Penalties Law includes violations of EMTALA, False Claims Act, Anti-Kickback Statute, and Physician Self-Referral Law
***Tips
Establish and/or comply with compliance programs to ensure you do not submit false or fraudulent claims or violate referral laws
Use your critical thinking skills to evaluate offers and agreements made with individuals and entities within the health care industry
Practice proper patient evaluation and charting to lower risk of making mistakes
