STM Lecture 1 - Current Theories
1/94
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
95 Terms
Soft Tissue
Tissues that connect, support, or surround other structures and organs
- Tissues in body that are not bones/organs
Soft Tissue Examples
- Muscles
- Tendons
- Ligaments
- Fascia
- Nerves
- Fibrous Tissues
- Blood Vessels
- Synovial Membranes
Other Tissue
Bones + Organs
- For STM, help to identify muscles using bony landmarks
- To avoid during percussion therapy
Fascia
Continuous 3D matrix of structural support; SENSORY ORGAN
- Forms perfect profile of everything in system
- Dynamic sensory network
FASCIA FIRST !!!
Fascia Characteristics
Soft tissue component of connective tissue system
- Supports everything in body
- Deep and superficial layer
- All muscles have fascial connections
Muscle Spindles
Activate when we move; Stimulated when fascia is stretched
- Inform CNS of changes in tone and elasticity
Muscle Spindles - Location
Layers of epimysium and perimysium
Why are sensory receptors in fascia important?
Allow for smooth and safe movement
Superficial Fascia
Houses nerves, blood, and lymph
- Superficial vessels
Superficial Fascia - STM Effects
Techniques done here affect:
1. Lymph flow
2. Ability of skin to glide on superficial fascia unrestricted
Deep Fascia
Envelops all muscles in body
- 2 Types (Aponeurotic + Epimysial)
Deep Fascia - Main Function
Transmit muscular forces at a distance
- Biotensegrity
Types of Deep Fascia
1. Aponeurotic
2. Epimysial
Aponeurotic Fascia
Binds muscles together or connects muscles to bone
- Sheet-like, pearly white fibrous membrane
Epimysial Fascia
Surrounds entire muscle belly + helps separate muscles
- Fibrous connective tissue sheath
- Thin and tough
Perimysium
Sheath surrounding bundles of muscle fibers
Endomysium
Sheath surrounding individual muscle fibers
Extracellular Matrix (ECM)
Fiber network of proteins + substances that provide structure to connective tissues
- Made up of / suspended by ground substance
Ground Substance
Hydrated gel-like substance that holds all other necessary cells for biological function
- Prevents adhesions
- Homeostasis of it is crucial
What does ECM supply fascia?
1. Viscosity
2. Elasticity
3. Ability to send movement
Cells in ECM
- Ground substance
- Lymphocytes
- Macrophages
- Fat Cells
- Melanocytes
- Mast Cells
- Elastic Fibers
- Collagen Fibers
- Reticular Fibers
Collagen
Provides tensile strength
Elastin
Provides recoil / elasticity
What does ground substance provide?
Glide
What stimulates ground substance?
Movement
- Maintains hydration + viscosity of tissues
- Prevents adhesions
Normal Phase of Healing
Point of injury --> Point of repair
Fibrosis
Point of repair --> Excess Repair
- TOO MUCH HEALING!
Fibrosis - Characteristics
Excessive buildup of collagen + extracellular matrix during healing
- Biological process
- When normal repair process becomes overactive/prolonged
- Limit mobility, elasticity, normal force transmission
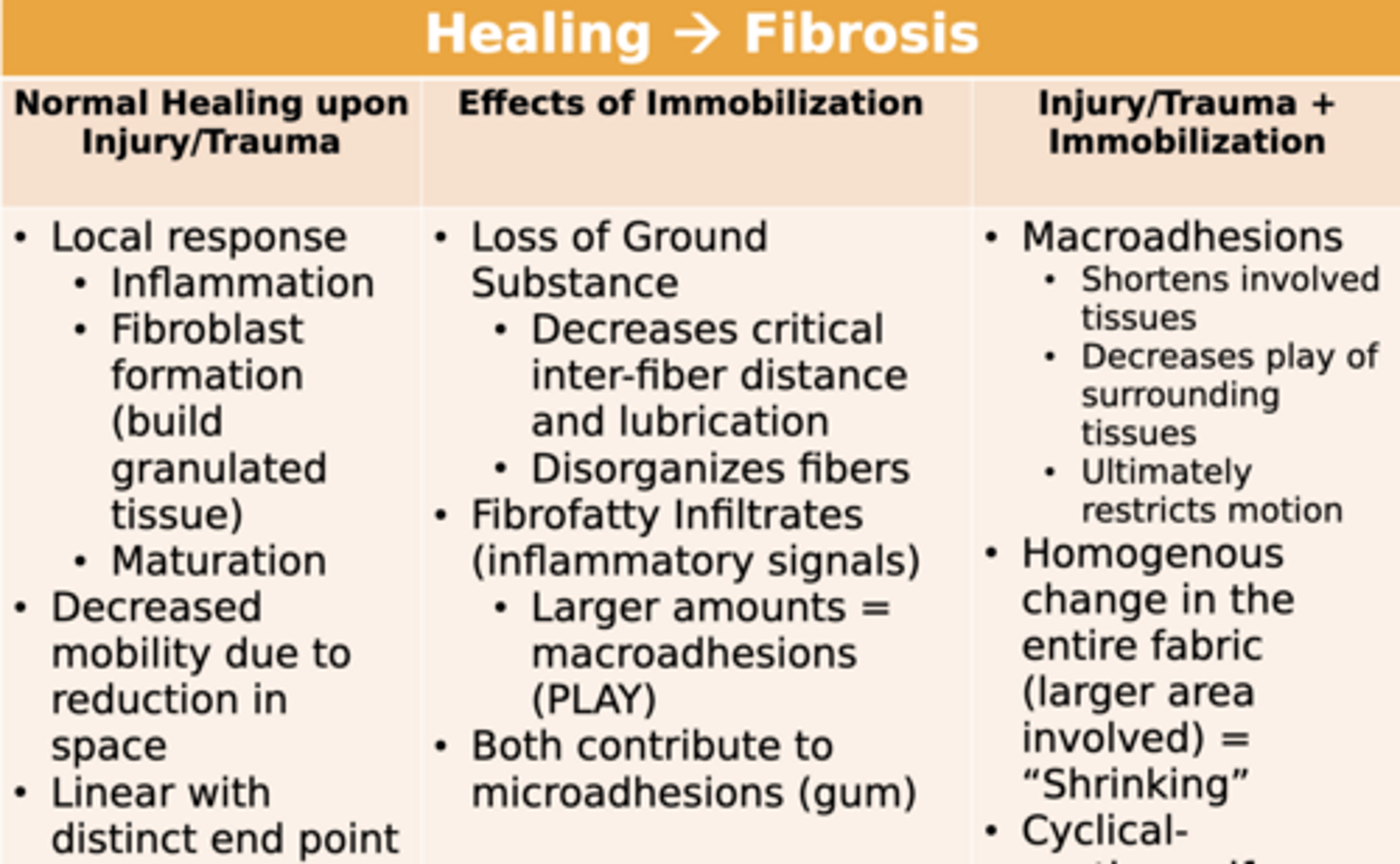
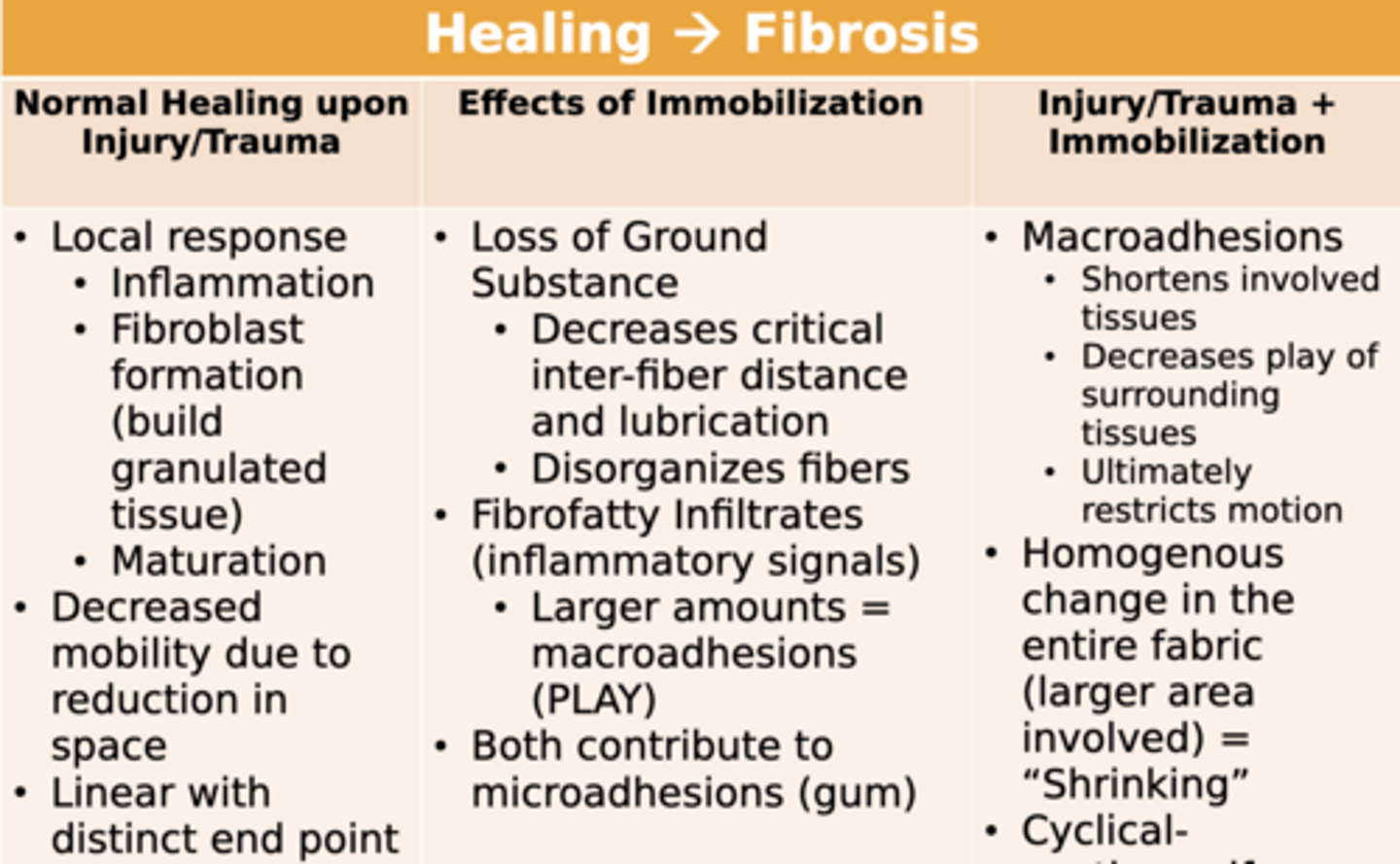
Normal Healing Upon Injury/Trauma
1. Local Response
2. Decreased Mobility due to space reduction
3. Linear with distinct end point
Local Response
- Inflammation
- Fibroblast formation
- Maturation
Inflammation
Starting point of normal healing
- Reduces space and mobility
Fibroblasts
Lay down collagen and extracellular matrix
Is healing linear?
YES
- Has a distinct end point
Early movement
Helps maintain space, hydration, and alignment of collagen
- Gentle movement
Effects of Immobilization
1. Loss of Ground Substance
2. Fibrofatty Infilatrates
- Both contribute to microadhesions
Loss of Ground Substance
Decreases critical inter-fiber distance and lubrication
- Tissues dry up, have less glide
- Disorganizes fibers
Fibrofatty Infiltrates
Normal muscle fibers are replaced by fat
- Inflammatory signals
- Larger amounts = Macroadhesions (PLAY)
Immobilization Examples
- Casting
- Sling
- Bracing
- Splinting
- Protocols post-op
- Sedentary
- Fear/Avoidance of movement
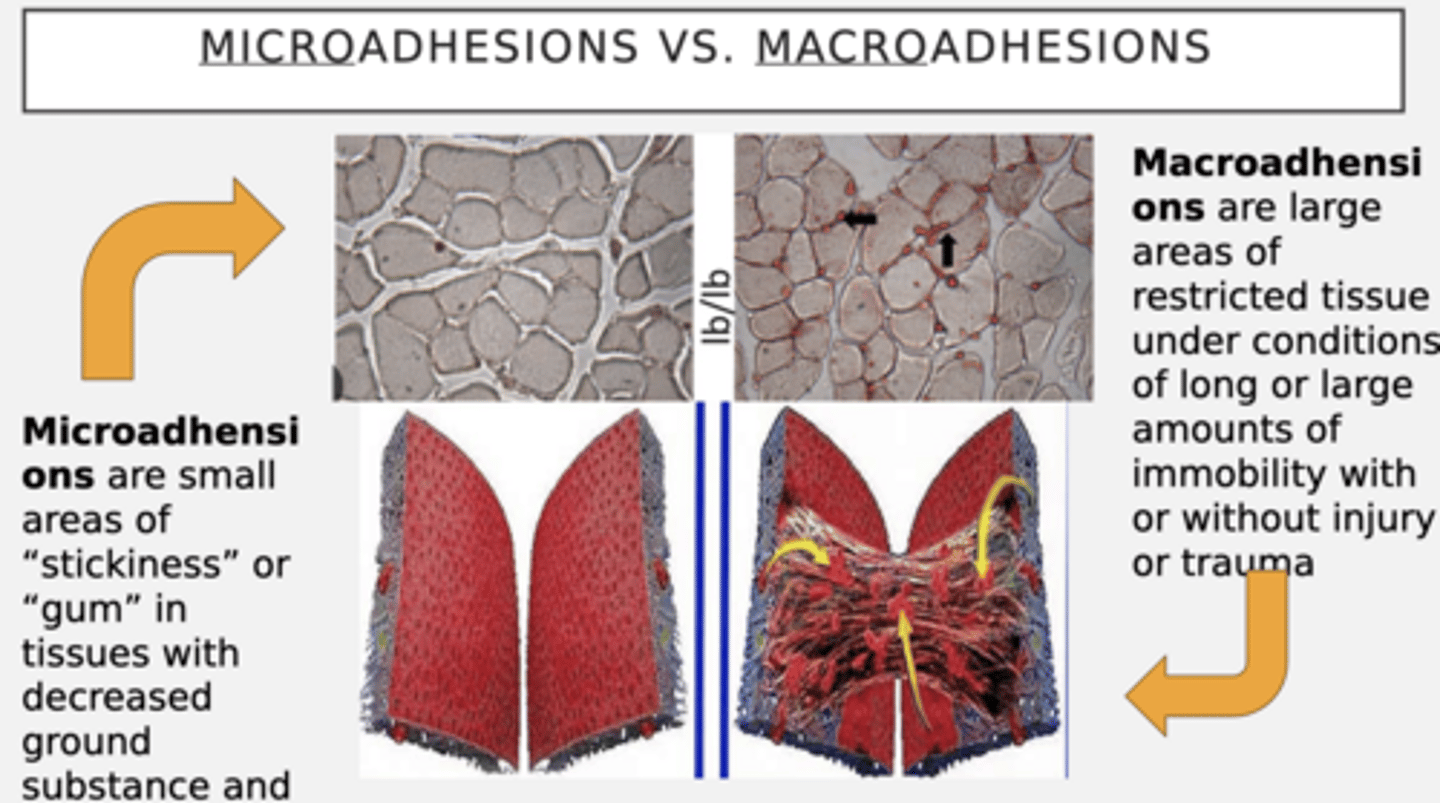
Macroadhesions
Large areas of restricted tissue under conditions of immobility
- With or without injury/trauma
Macroadhesions - Characteristics
1. Decrease play
2. Limits ROM
3. Shortens involved tissues
- Mechanical process
Microadhesions
Small areas of "stickiness" or "gum" in tissues w/ decreased ground substance + fatty fibroinfiltrates
- Smaller
What contributes to microadhesions (gum)?
Loss of ground substance + fibrofatty infiltration
Microadhesions vs Macroadhesions
Same process, only difference is magnitude
Shrinking
Homogenous change in entire fabric
- Larger area involved
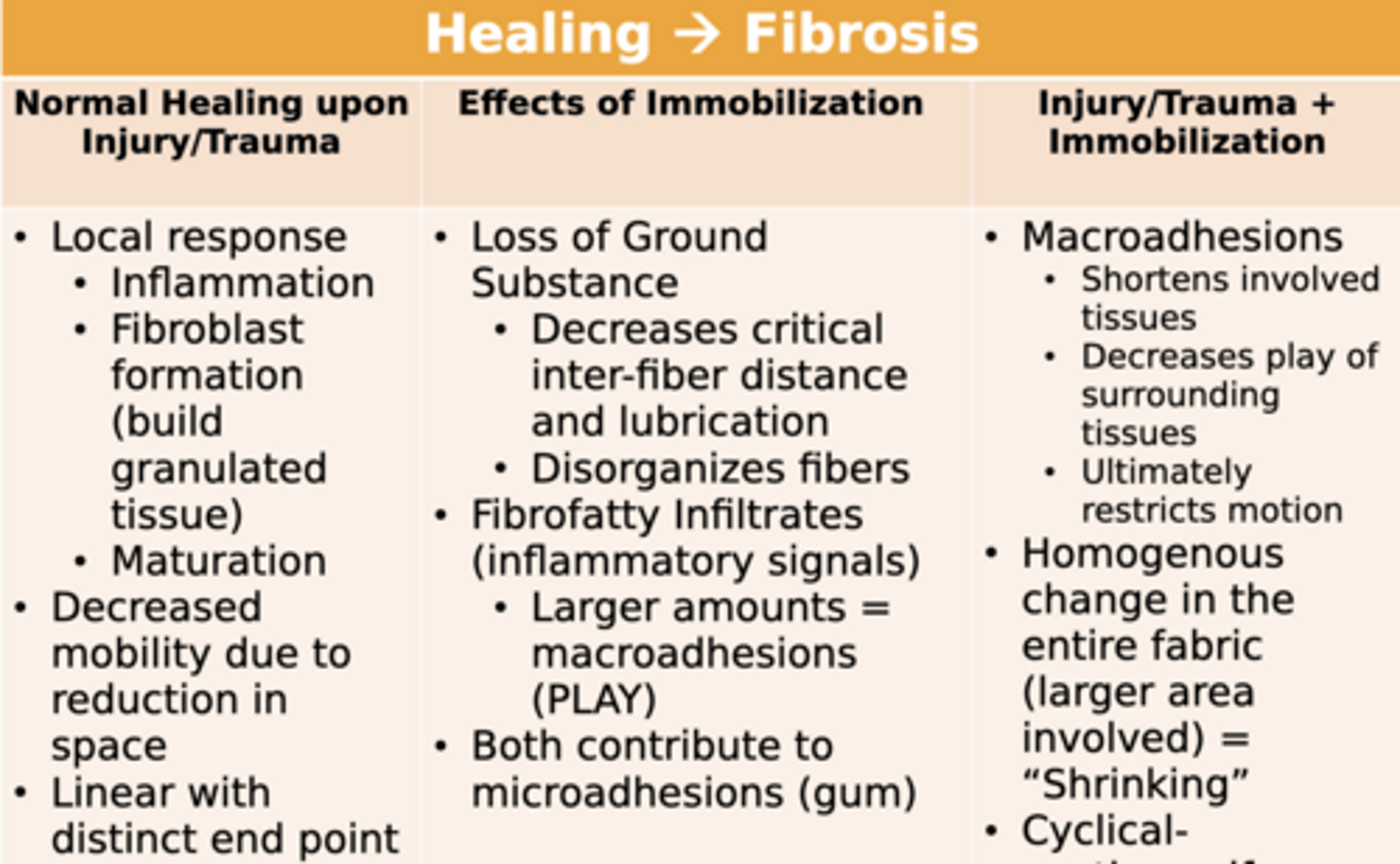
Cyclical
Continues if irritant is present
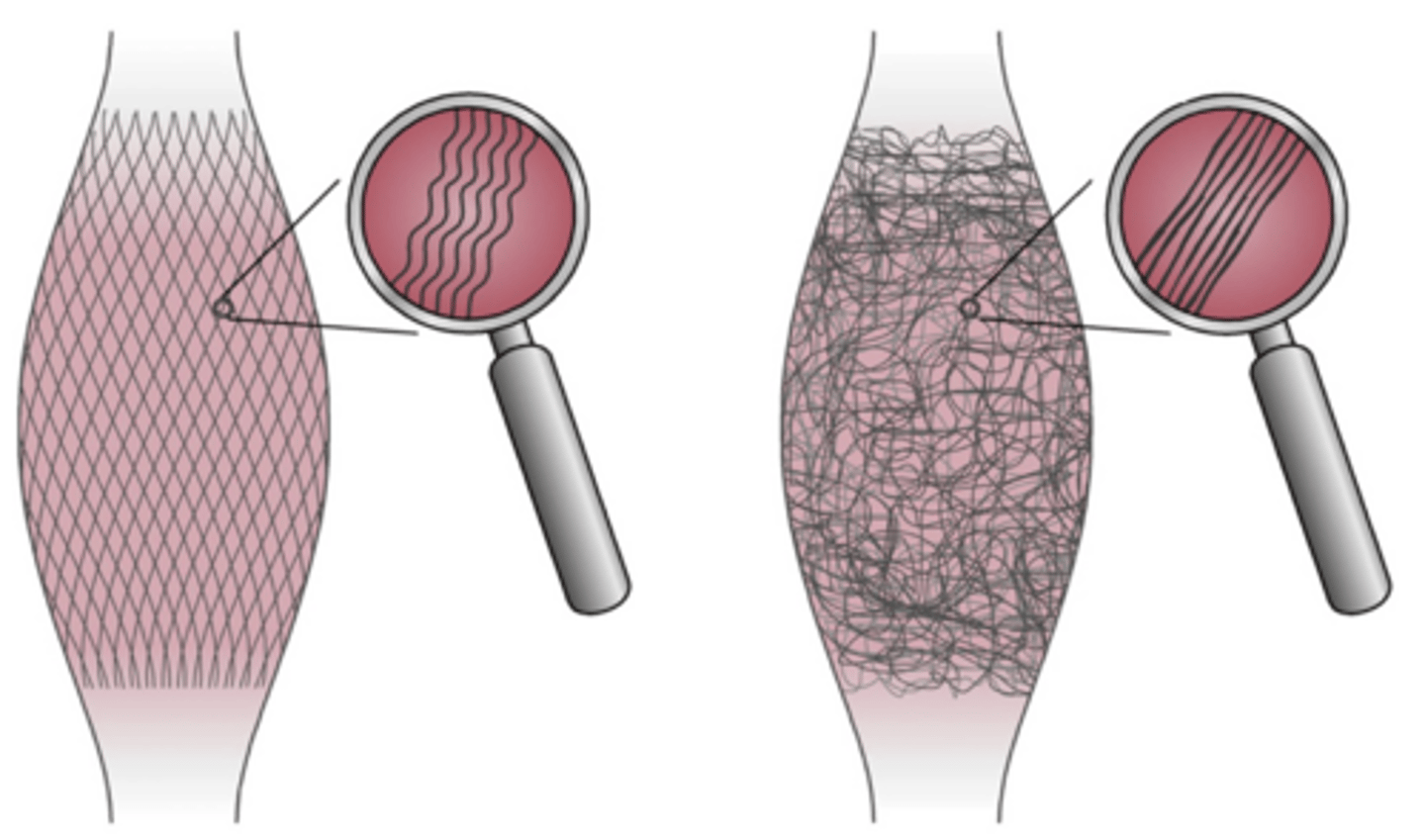
Tissue Fiber Organization - Disruptions
Disorganized = Lose elasticity + Force transmission
- Controlled loading helps realign fibers
Fascia - Training Principles
Elastic Loading + Counter-movement
- Preloading tissue
- Dynamic stretching
- Hydration
- Consistency
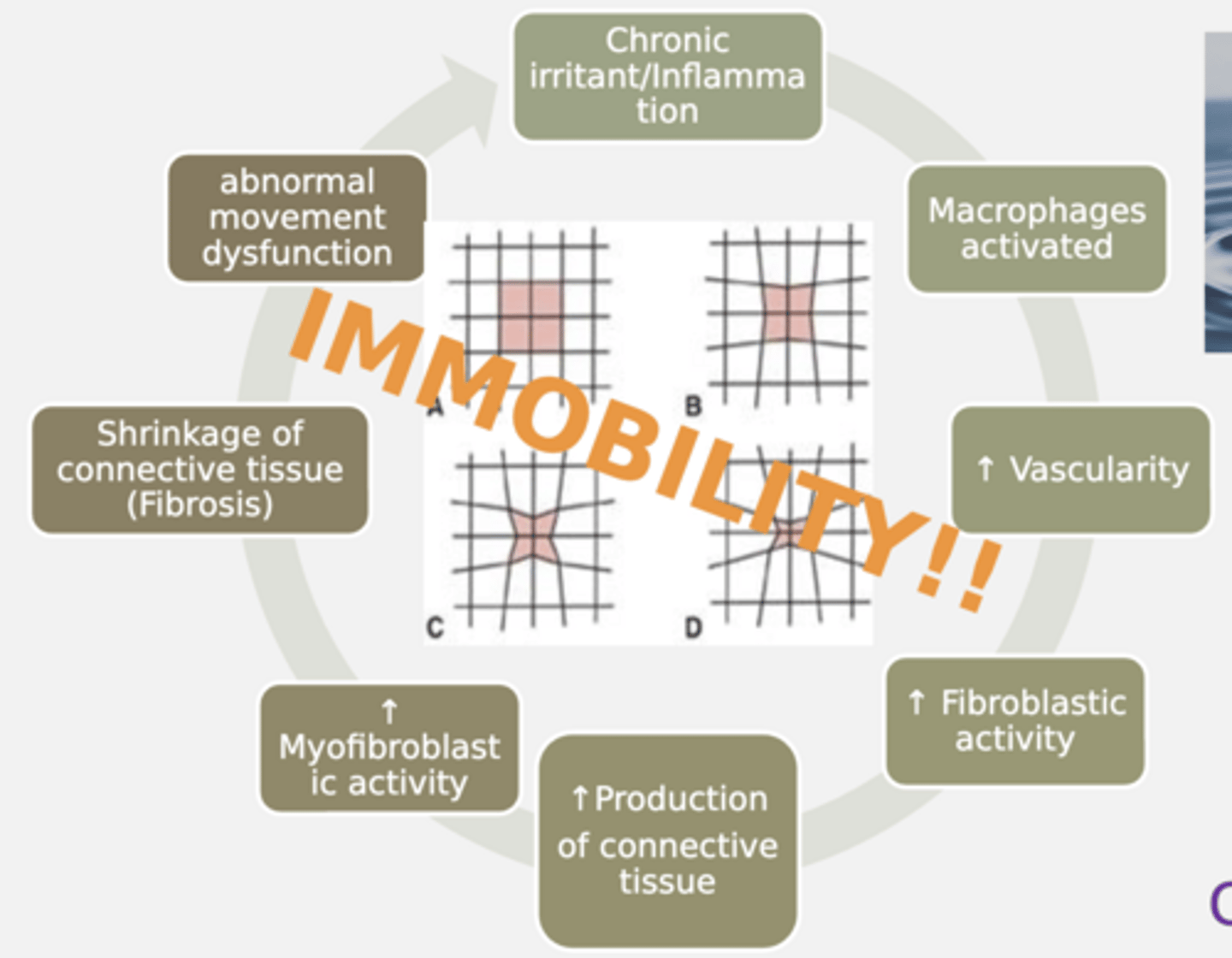
Fibrosis Cycle
CYCLE REPEATS AS LONG AS IRRITANT IS PRESENT
- Cycle occurs due to immobility
1. Trauma/Injury
2. Macrophages activated
3. Increased blood flow (vascularity)
4. Increased fibroblasts
5. Increased connective tissue production
6. Increased myofibril activity
7. Shrinking of connective tissue (FIBROSIS)
8. Abnormal movement dysfunction
Fascial Adhesions
Interfere with proper coordinated movement!
- Restrict tissue glide
- Impair sensory input
- Change CNS control of movement
How do address fascial adhesions
MOVEMENT = MOST IMPORTANT!
- With STM
Fascial Adhesions - STM Management
- Promote circulation
- Ward off microadhesions from becoming macroadhesions
- Promote normal tissue repair
- Slow scar tissue formation
- Neuromodulatuion of pain + tone
3 Models to cause soft tissue changes
All three play a role in outcome
1. Mechanical Model
2. Neurological Model
3. Myofascial Meridians
- Biotensegrity
Mechanical Model
Soft tissue work forms viscoelastic tissue
- Tissue Deformation
- Changes to hyaluronic acid --> Decrease ground substance
- Decreases in extracellular matrix space
- Fibroblast response to shearing forces (inflammation)
- Dense facial layers
- Compensations
Hyaluronic Acid
Component of ground substance
- Hydration
- Lubrication
- Viscoelasticity
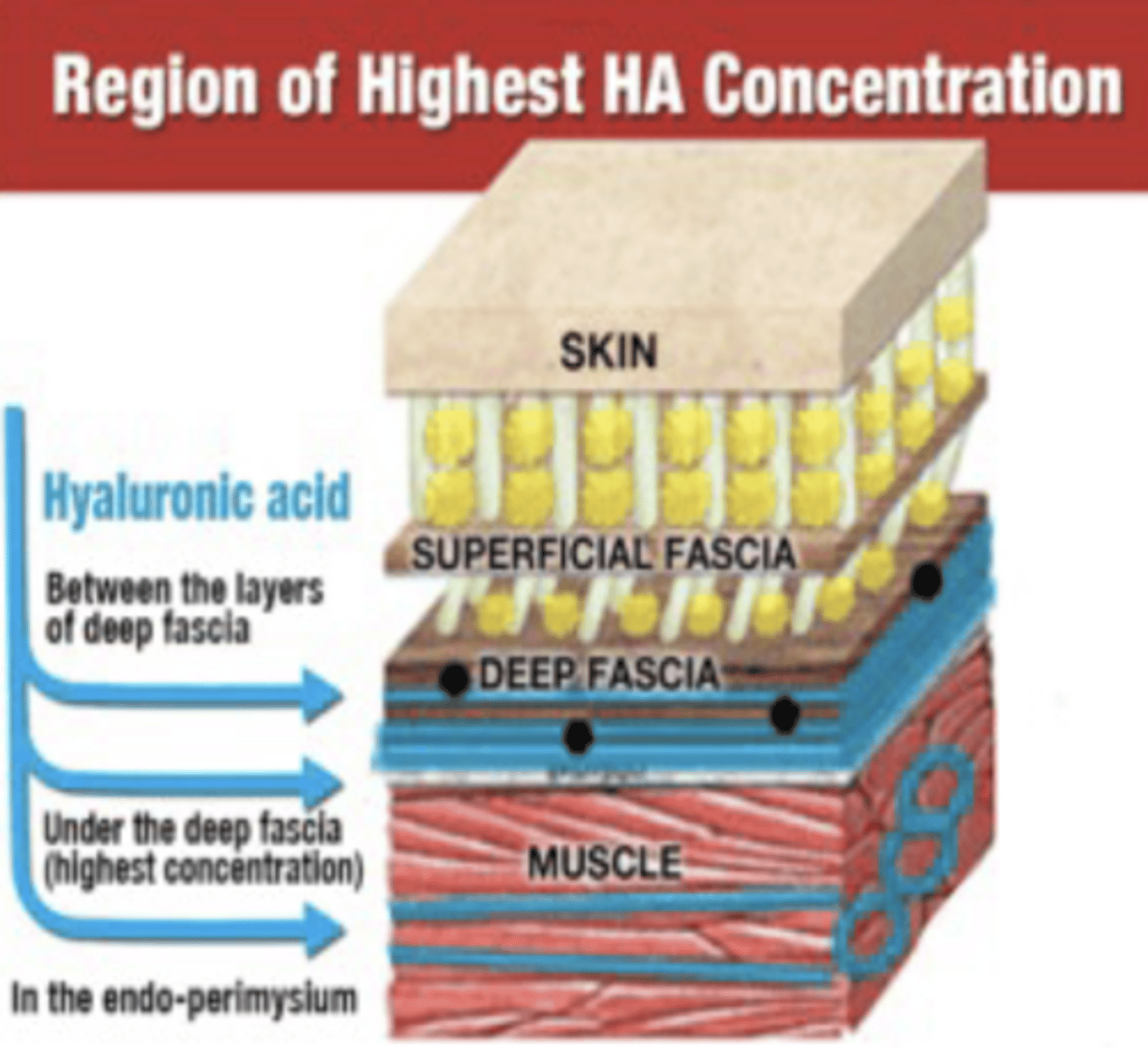
What region has the highest hyaluronic acid concentration?
Under deep fascia
Mechanical Model - Limitation
Forces from hand are too small to actually change tissues
Mechanical Model - Interventions
Influence tissue glide, treat fascia
- Cupping
- Skin rolling
Neurological Model (Dermoneuromodulation)
Changes in soft tissue are primarily due to NS
- NS MODULATION!
- Not due to mechanical reshaping
- Neurological Reset
Neurological Model - CHaracteristics
We change brain perception via skin
- Mechanical input stimulates receptors
- Brain elevates safety of sensory input
- Allows for movement once deemed safe -- More ROM
What mechanoreceptors are present within fascia network?
- GTOs
- Ruffini Endings
- Pascinian Corpuscles
What fascia has the most mechanoreceptors in the body?
Thoracolumbar Fascia
Neurological Reset
Reset occurs to downregulate muscle tone
- Overwhelming amount of info!
- NS can be reset with diaphragmatic breathing
Neurological Reset - Steps
1. Muscle stimulated (stretch/tension)
2. Mechanoreceptors activate
3. Info to CNS via sensory neurons
4. New instructions carried by motor neurons --> mm fibers
5. Muscles relax and lengthen
Diaphragmatic Breathing
Can reset nervous system
Mechanical Model - Overall Summary
TISSUE DEFORMATION
Neurological Model - Overall Summary
NERVOUS SYSTEM MODULATION
Tensegrity
Tensional integrity; Describes how structure is stabilized
- Continuous tension + Discontinuous compression
- Takes shearing, bending moments, levers into account
- Self-organized, hierarchal, load distributing
- Low energy consuming
How do bone and fascia contribute to Tensegrity?
Pulling one apart impacts entire structure
- Forces distribute EVERYWHERE
- BONE = Anchor
- FASCIA = Fabric between bone
Pec Minor - Tensegrity Example
By working on pec minor, you are impacting system to help shoulder ROM
- Coracoid Process and Ribs = Anchors
- Pec Minor = Cable between ribs and coracoid process
Biotensegrity
Body's integrity is maintained by balance of continuous tension and discontinuous compression
- Body is a connected network
- Tensegrity applied to anatomy
- Change in tension ANYWHERE within system is instantly signaled everywhere else in body
Biotensegrity - Components
Continuous tension = fascia + muscles
Continuous compression = bones and joints
Biotensegrity - Fascia + Muscles
Fascia distributes force --> Muscles dynamically adjust
- Continuous tension
Biotensegrity - Spine
Acts as central tensegrity tower integrated with entire system
Total Body Modeling
1. Viscoelastic bony segments
- Limbs
2. Viscoelastic connectors
- Cartilage
- Joint capusles
- Ligaments
3. Viscoelastic active motor system
- Muscle
- Tendons
- Connective tissue
4. Visceral Organs
Kinetic Chain
Functional, sequential movement of joints and muscles
- If joint doesn't move, muscle won't move it
Myofascial Meridians (Anatomy Trains)
Mapped fascial lines; Tension in one area influences another
- Like highways
- Longitudinal connections between muscle + fascia
- Muscles do not act in isolation
- Continuous fascial sheaths
- Global force transmission
Anatomical Slings / Myofascial Chains / Myofascial Slings
Cross-body force transmission system; Movement engines
- Can manipulate one area to influence another
- i.e. Posterior oblique sling, lateral sling, anterior oblique sling
Myofascial Meridians vs. Anatomical Slings
Myofascial meridians = Map entire body's connectivity
Anatomical slings = Part of Myofascial meridian system
- Specifically identified units within map
ICHARTS
I = Intake Forms
- PT order
C = Chief Complaint
- Why are they here
H = History
- Goals, medical hx, lifestyle
A = Asymmetries
- Rule out areas that are not problem, start hypothesizing
R = ROM
- Active/Passive
T = Tissues
- Play/Tone
S = Special tests
- Neurodynamics/Ortho
- Do at end to avoid provocating patient (annoying)
Strumming
Used to assess tone
Perpendicular Deformation
Used to assess play
Clinical Practice Guidelines (CPG)
Evidence-based recommendations that drive clinical decisions
- A-F; What works for whom and which situation?
- Reduce variability in care
CPG - A thru C
CAN PRIORITIZE
CPG - A
Strong Evident (Should Do)
- Hip OA
- Lateral ankle sptain
- Heel pain / Plantar Fascitis
CPG - B
Moderately Evident (May Do)
- Acute LBP (<3 months)
- Chronic neck pain
- PFPS (taping)
CPG - C
Weak Evidence (Can Do)
- Carpal tunnel syndrome
- Sub-acute neck pain to T/S + C/S
CPG - D thru F
Should NOT be part of treatment
CPG - D
Conflicting Evidence
CPG - E
Theoretical
CPG - F
Opinion (SHOULD NOT PRIORITIZE)
- STM not mentioned in multiple CPGs
Does it mean a technique does not work if it is not in a CPG?
NO -- Further evidence is just needed
Evidence Based Practice
1. Best Evidence
2. Clinical Expertise
3. Patient Values
STM - Indications
- Loss of ROM
- Scar tissue and adhesions
- Play/Tone disruptions
- Poor quality of movement
STM Contraindications
- Open Wound / Broken Skin
- Hematoma
- Fracture
- Active infection (CAN SPREAD)
- Cancer
- Acute circulatory disorders (Embolism risk)
- Skin conditions
- Advanced diabetes
- Anti-coagulant medications
- Systemic infection (cellulitis)
- Obstructive Edema (Can worsen swelling)
- Acute RA (CAN CAUSE FLARE UP)
STM Precautions
Keep STM to minimum, focus more on integration of movement
- Psychosocial factors (Anxiety, pain, fear avoidane)
- Pregnant
- Hypersensitivity
- Hyper/Hypotension
- Acute/Inflammatory stage of healing