Burns and Wounds
1/61
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
62 Terms
Thermal Burns: Epidemiology
Risk highest between 18-35 years old
75% of all injuries due to fire or scalding
43% of scalding injuries occur in children < 5 y/o
Elderly individuals have disproportionate higher death rate
Thermal Burns: Pathophysiology
Depth and severity vary by both age of victim and anatomic locations exposed
Partial thickness burns disrupt skin barrier → free water loss
Becomes significant in moderate to large burns
Result: spectrum of local and systemic homeostatic disorders contributing to burn shock
Fluid and electrolyte abnormalities seen in burn shock due to alterations in cell membrane potential
Intracellular influx of water and sodium
Extracellular migration of potassium due to dysfunction with sodium pump
Systemic vascular resistance increased due to inflammatory response of the burn
Significant metabolic acidosis may be present early in large burn injuries
Massive burns increase blood viscosity in early phases → transition to anemia from erythrocyte extravasation and destruction
Cellular damage occurs at temperatures > 45 degrees Celsius → denaturation of cellular proteins
Most important factors
Severity of the burn
Presence of inhalation injury
Associated injuries
Patient’s age and comorbid conditions
Acute organ system failure
Thermal Burns: Local Effects
Liberation of vasoactive substances
Disruption of cellular function
Formation of edema
Thermal Burns: Systemic Effects
Alters neurohormonal axis and further extends injury
Histamine release
Kinin
Serotonin
Arachidonic acid metabolites
Free oxygen radicals
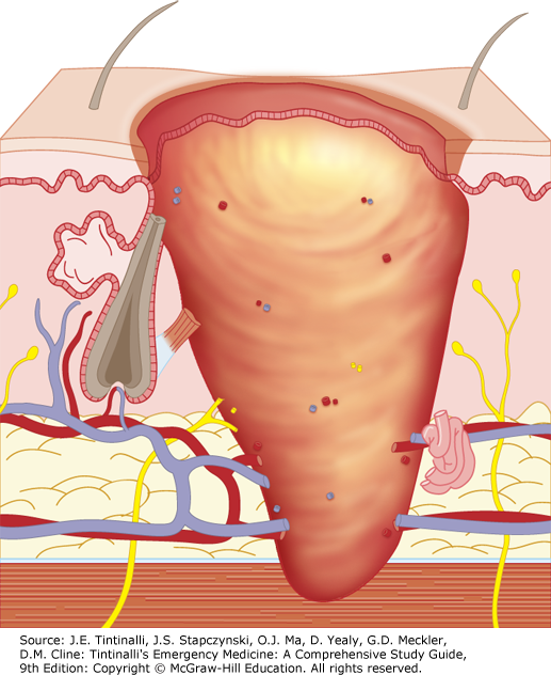
Burn Wounds and their Three Zones
Zones of coagulation
Tissue is irreversibly destroyed with thrombosis of blood vessels
No more blood flow and tissue is dead → no coming back and area is gone forever
Zone of stasis
Stagnation and microcirculation
Can become progressively more hypoxemic and ischemic if resuscitation is inadequate
Not a complete destruction
Zone of hyperemia
Increased blood flow
Minimal damage to cells and spontaneous recovery is likely
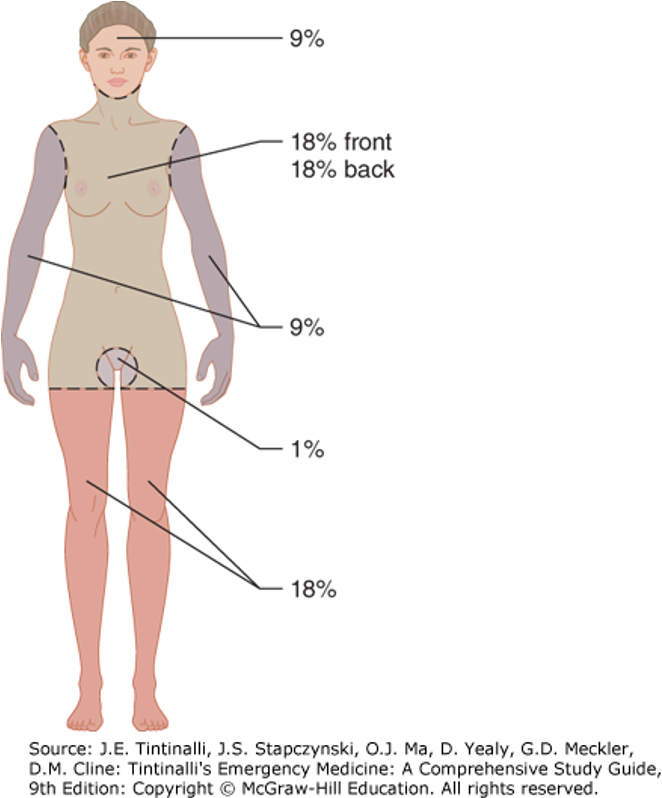
Determining Burn Size
Rule of nine’s
The area of the back of the patient’s hand is 1% of their total body surface
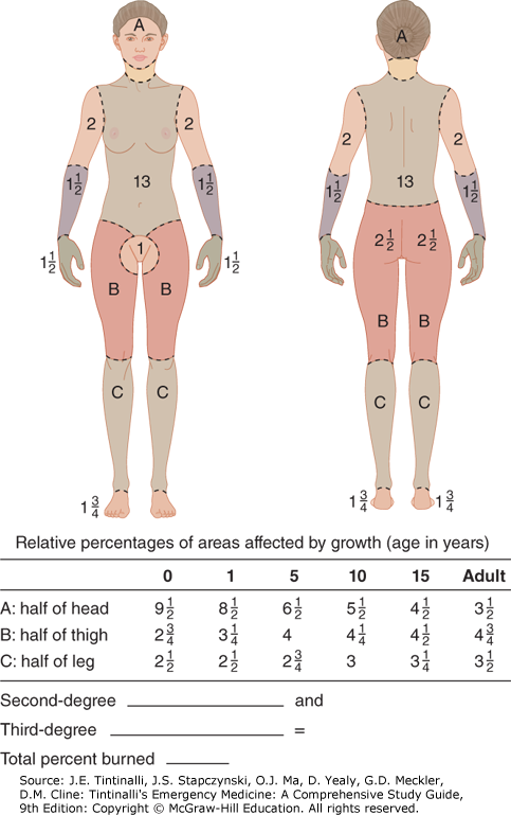
Lund Browder Burn Diagram
Allows for age adjusted determination of burn size for a given depth
Allows for anatomic differences in children
Rule of Nine’s
WILL BE GIVEN DIAGRAM
Lund Browder Burn Diagram
How to Determine Burn Depth
Historically has been described as degrees
First
Second
Third
Fourth
Classification based on surgical intervention has become accepted
Superficial partial thickness
Deep partial thickness
Full thickness
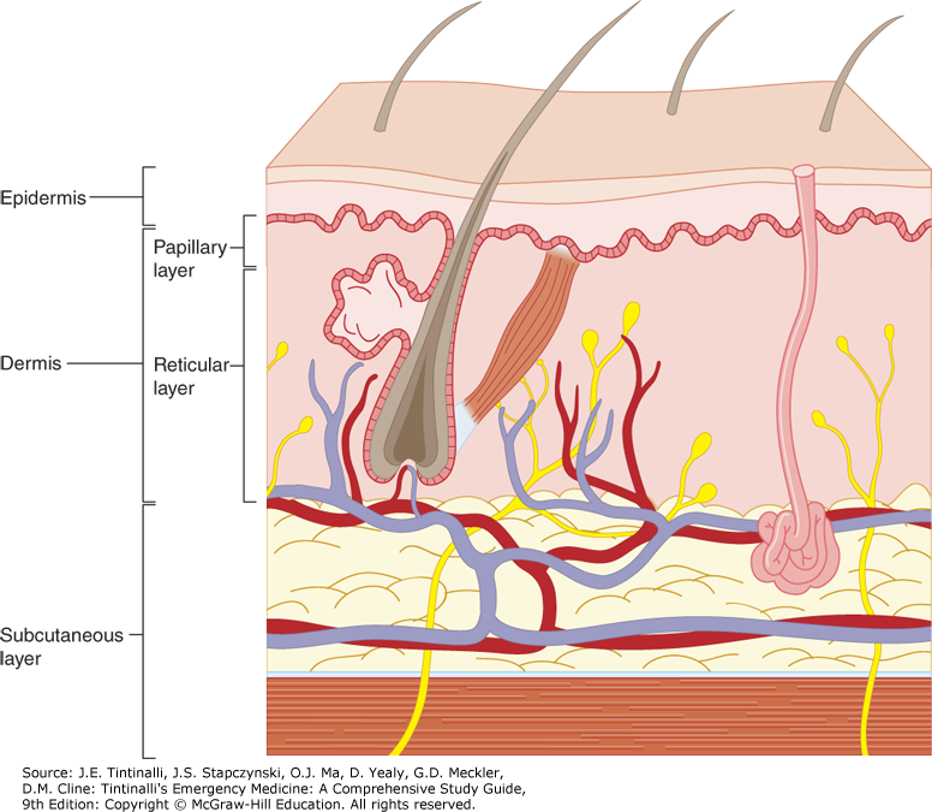
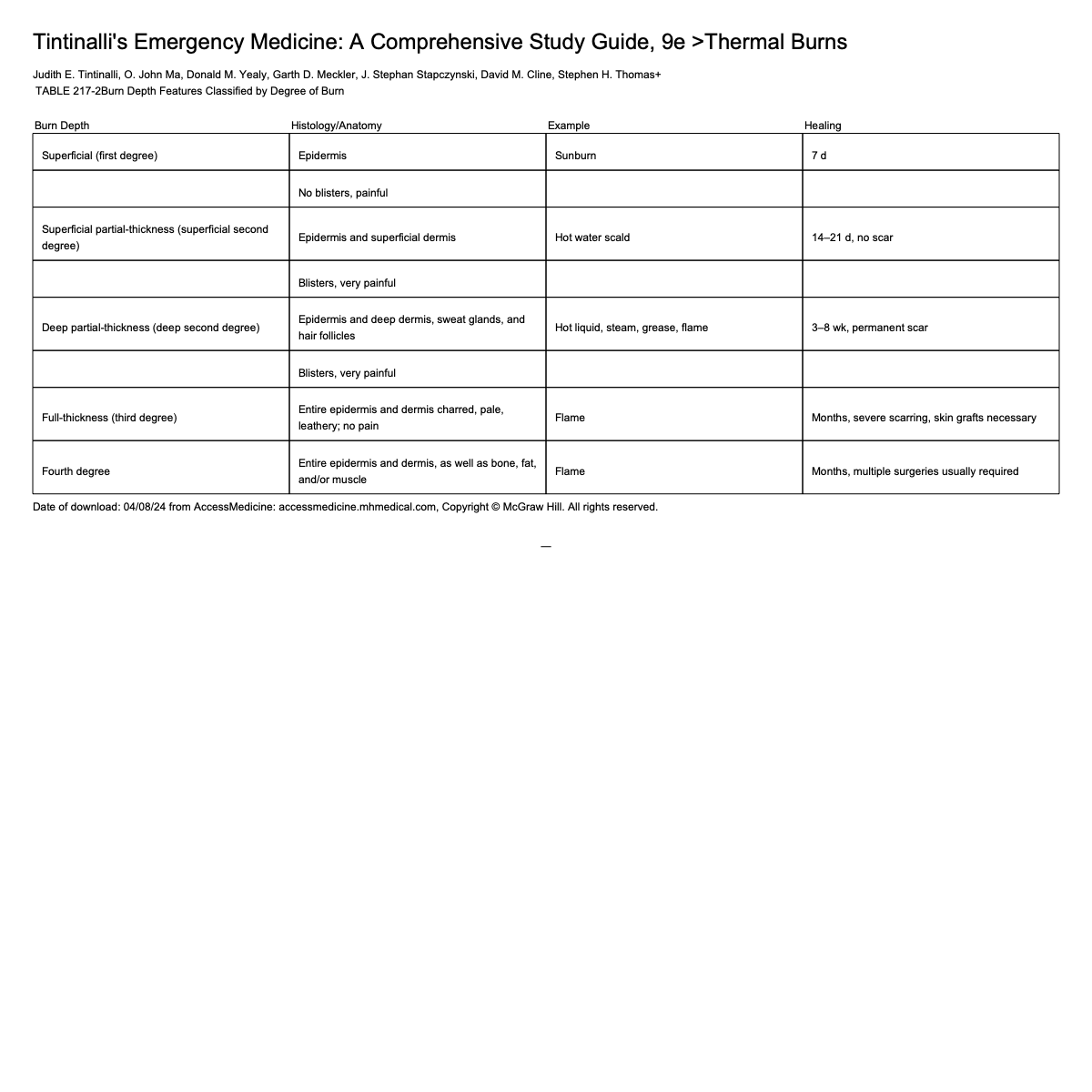
Burn Depth
Burn Classification
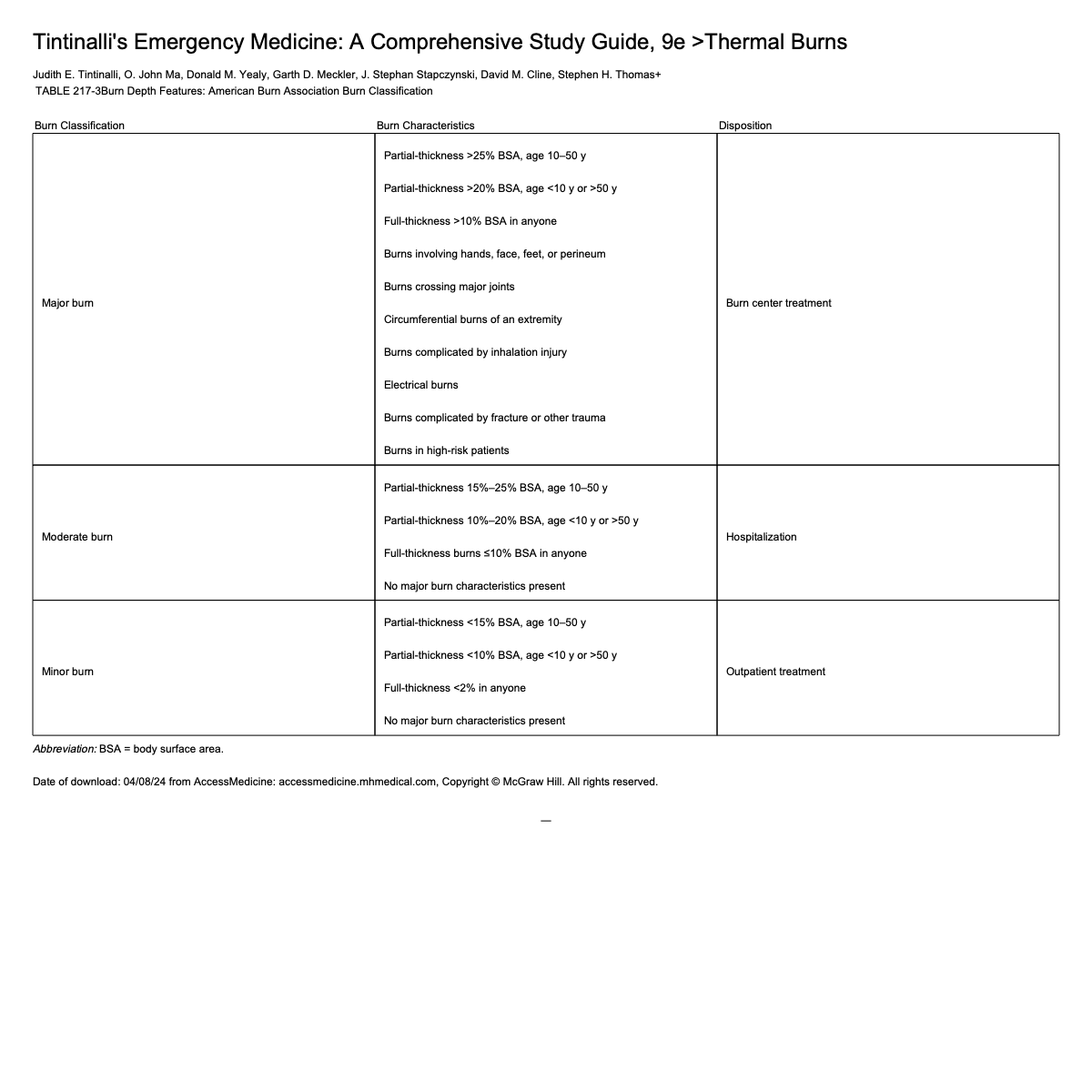
Superficial Burn
Only involves epidermal layer of the skin
Ex: sunburn
Burned skin is red, painful, and tender without blister formation
Usually heals in 7 days without scarring
Treatment → symptomatic
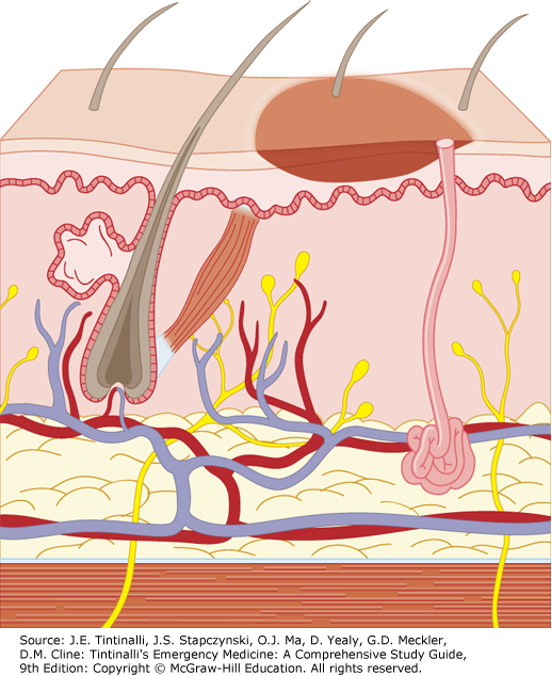
Superficial Partial Thickness Burn
Epidermis and superficial dermis (papillary layer) injured
Deeper layers of dermis, hair follicles, and sweat/sebaceous glands spared
Often caused by hot water or scalding
Skin is blistered and exposed dermis is red and moist → painful to tough
Healing occurs in 14-21 days with minimal scarring
Have full return of skin function
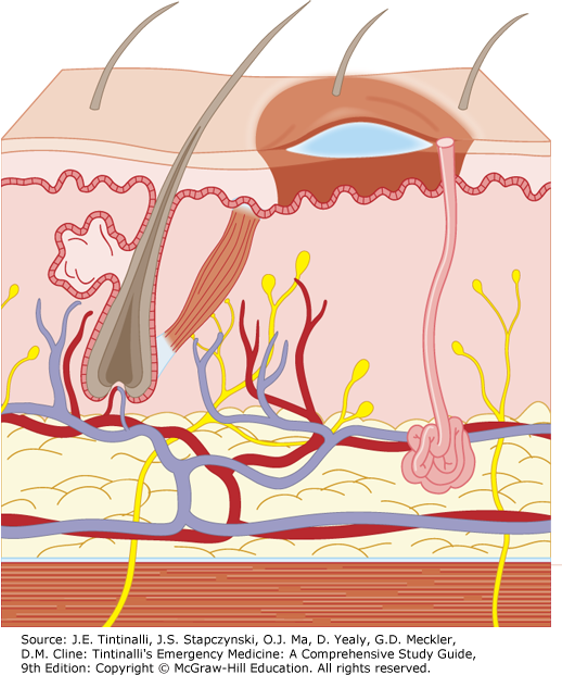
Deep Partial Thickness Burn
Extends into the deep dermis (reticular layer)
Hair follicles and sweat/sebaceous glands damaged but deeper structures usually spared
Causes: hot liquids (oil or grease), steam, flame
Skin may be blistered, exposed dermis is pale white to yellow
Burned area does not blanch and has absent capillary refill and absent pain
Difficult to distinguish from full thickness
Heals over 3 weeks to 2 months
Scarring common
Surgical debridement and skin grafting may be required to obtain maximum function
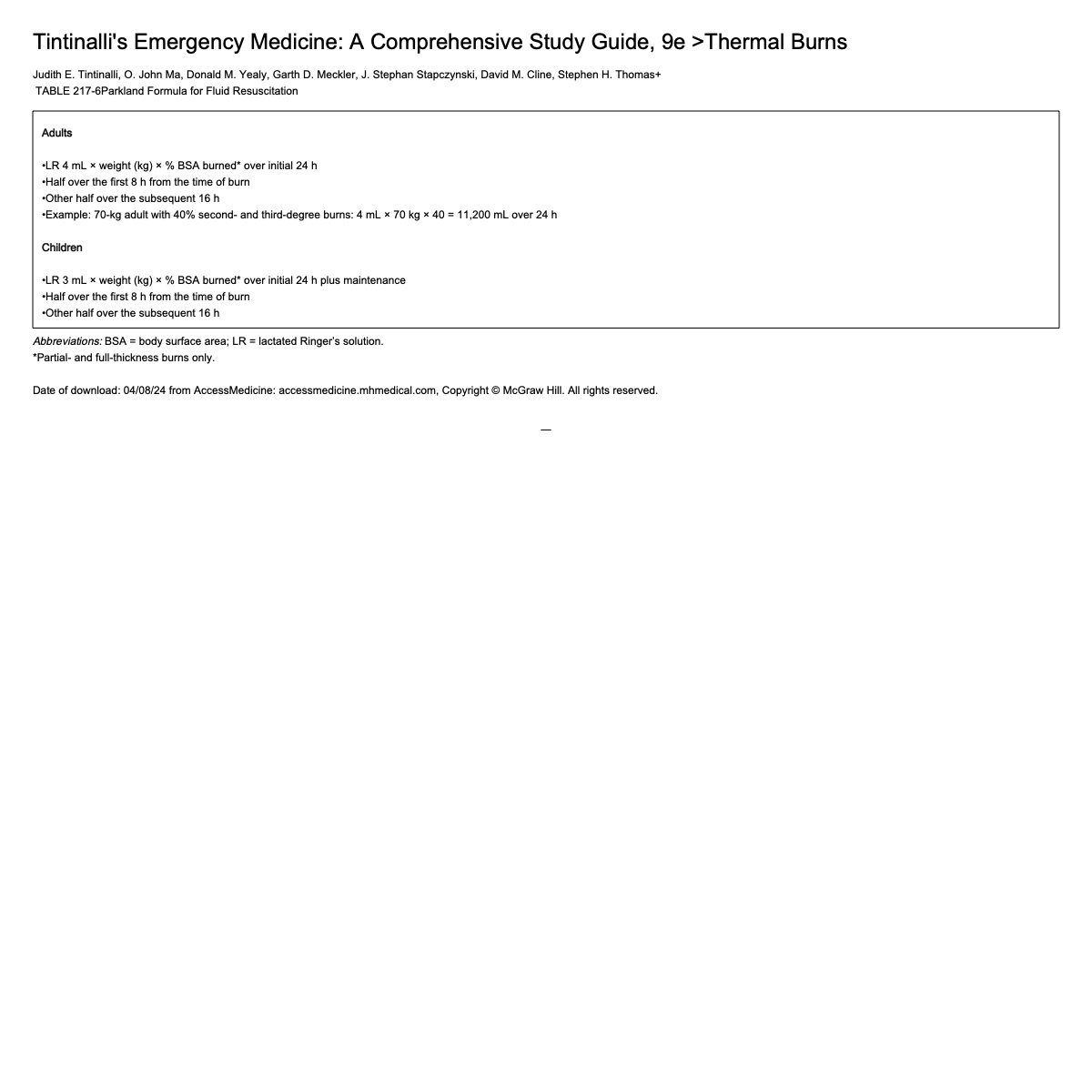
Full Thickness Burn
Involves entire thickness of skin
All epidermal and dermal structures destroyed
Typically caused by flame, hot oil, steam, contact with hot objects
Skin is charred, pale, painless, and leathery
Does not heal spontaneously
Surgical repair and skin grafting necessary
Significant scarring always present
Fourth Degree Burn
Extend through skin to subcutaneous fat, muscle, and bone
Devastating life threatening injury
Amputation or extensive reconstruction is often required
Burn Center Transfer Guidelines
Indications based on burn depth
Patient age < 10 y/o
Patient age > 50 y/o
Comorbidities (heart disease, diabetes, COPD)
Capabilities of receiving institution
Any burn involving face, hands, feet, genitalia, perineum, or major joints
Burn Treatment Pre-Hospital Care
Stop the burning process
Assess and, if needed, secure the airway → special attention to airway since rapid deterioration can occur
Initiate fluid resuscitation → IV isotonic crystalloid
Relieve pain → opiate medications
Protect the burn wound → cover with clean sheet
Transport patient to appropriate facilitiy
Burn Treatment ED Care
Obtain directed history from patient and EMS
Determine burning agent, involvement of chemicals, duration of exposure, and if injury was sustained in open or enclosed space
Assess for LOC, risk of blast injury, contact with electricity, or other trauma
Assess for need of cervical spine precautions
Quickly assess respiratory and circulation → stabilize as needed
Examine for signs of inhalation injuries → respiratory distress, facial burns, carbonaceous sputum, singed nasal hair, soot in mouth
If there is evidence of airway compromise with swelling of neck, burns inside of mouth, or wheezing → perform early ET intubation
Any airway involvement:
100% humidified oxygen (NRB, BiPAP, NC)
Early intubation
Bronchodilators
Lung protective ventilator settings (low tidal volumes and low airway pressures with high FiO2: concern that parenchyma damaged and at increased risk of pneumothorax)
Monitor BP, pulse, capillary refill time, mental status, and urinary output (consider urinary catheter placement, especially with perineal burns → can cause strictures and obstruct outflow) → 100-120 bpm considered normal due to catecholamine response
Perform secondary survey → head to toe assessment including eyes, estimate and record size and depth of burn injuries
Always gain pertinent PMH → important to get tetanus status (usually give vaccination regardless of status for prevention because of higher risk)
Consider NG tube for > 20% total body surface area partial thickness burns due to risk of ileus
Labs based on type and severity of burn
CBC (anemia)
BMP
ABG (inhalation/airway burn)
Carboxyhemoglobin
Serum creatinine kinase (partial and full thickness: worried about rhabdomyolysis)
Urinalysis for myoglobin (monitor end organ injuries and break down of tissues)
Imaging:
CXR (additional if indicated)
Fiberoptic bronchoscopy indicated for suspected inhalation injury (consider in intubated patient since it’s both diagnostic and therapeutic)
EKG
ED Management of Pregnant Patients
Significant morbidity to mother and fetus
Outcome of pregnancy determined by extent of injury to mother
Spontaneous termination common in large body surface area burns
Resuscitation requirements may be higher
Should have fetal monitoring and early OB consultation
Consider sending to burn center
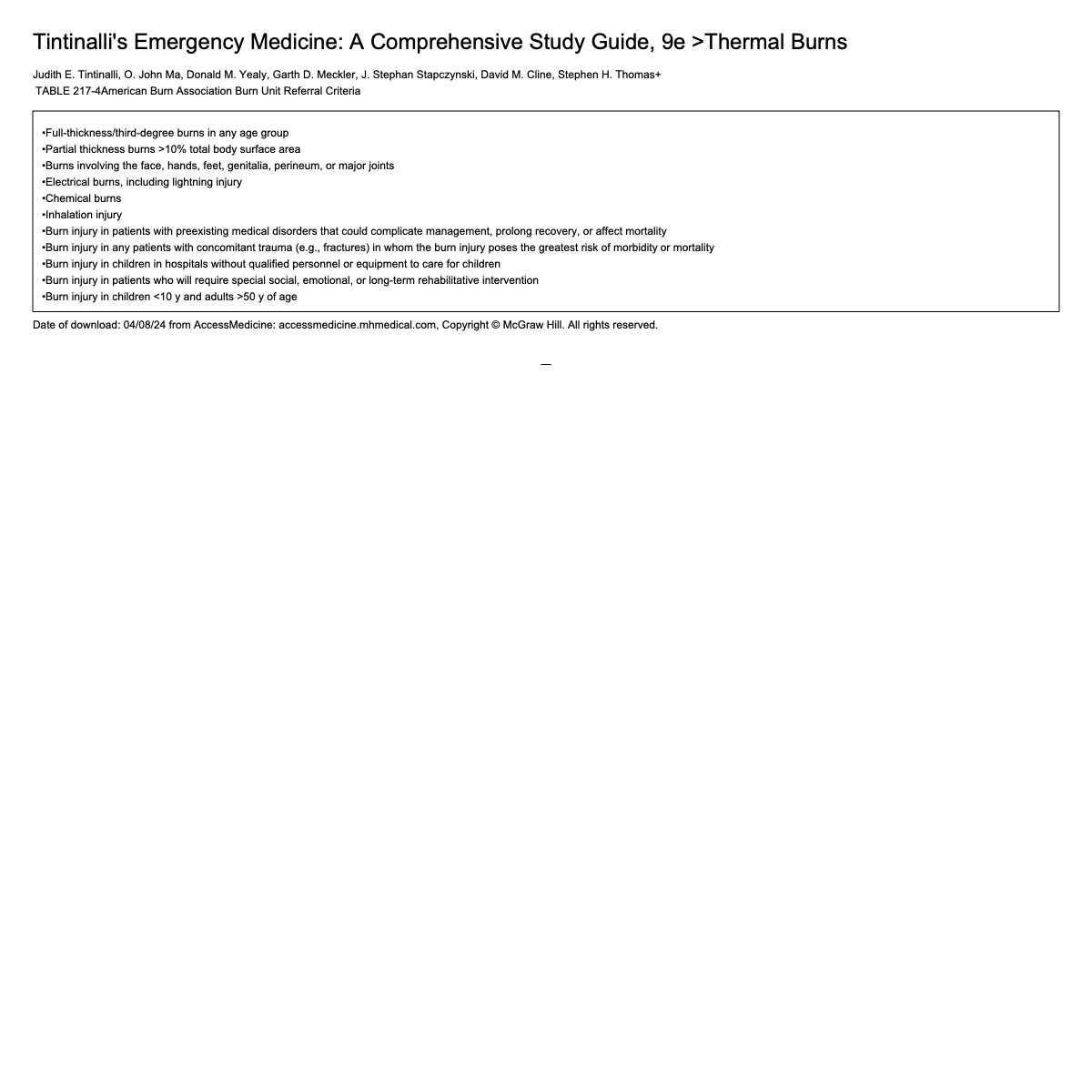
Fluid Resuscitation
WILL NEED TO CALCULATE ON EXAM
Should be guided by monitoring cardiorespiratory status and urine output → trumps any calculated formula
Patients with thermal injuries and concomitant multisystem trauma or those with inhalation injuries → more than calculated fluid needs
Electrical injuries, incineration burns, associated crush injuries, and severe burns (involvement > 48%) → may produce rhabdomyolysis and myoglobinuria → renal failure (can prevent with dilution: need more volume)
Most commonly used formula → Parkland formula
Total fluid in 24 hours = 4 x weight (kg) x burn percentage
Give first half in 8 hours
Remainder 16 hours give remaining half
Fluid of choice → isotonic crystalloid
Patients with pre-existing cardiac or pulmonary disease need close monitoring to prevent pulmonary edema
Monitor:
Vital signs
Cerebral perfusion
Skin perfusion
Pulmonary status
Urine output: should remain between 0.5 and 1.0 mL/kg/hr
Wound Care
Initially wound should be covered with clean, dry sheet
Small burns → can be covered with moist saline soaked dressing
Best while waiting for admission or transfer
Soothing effect of cooling is due to vasoconstrictor in area
Stabilizes mast cells and reduces histamine release, kinin formation, and thromboxane B2 production
Larger burns → sterile drape (saline soaked dressing to large area can cause hypothermia)
Eshcarotomy
Indicated in circumferential deep burns
In the limbs → can cause compromised of distal circulation, especially after initial resuscitation
Must monitor distal vascular status
If vascular compromise evident → eshcarotomy indicated
Eschar incised with scalpel at the level of the fat → done on the mid-lateral portion of the limb, avoiding the fascia
May extend to hand and fingers
Can provoke substantial soft tissue bleeding
If circumferential burns to chest and neck → may restrict ventilation
Incision made along anterior axillary line from level of second rib to level of 12th rib
The two incisions should be joined transversely so the chest wall can expand
Pain Control
Burns are exceedingly painful
Superficial burns most painful
Cause hyperalgesia → mediated by A fibers
Local cooling may soothe but do not provide pain control
Preferred treatment → IV opiates
+/- anxiolytics
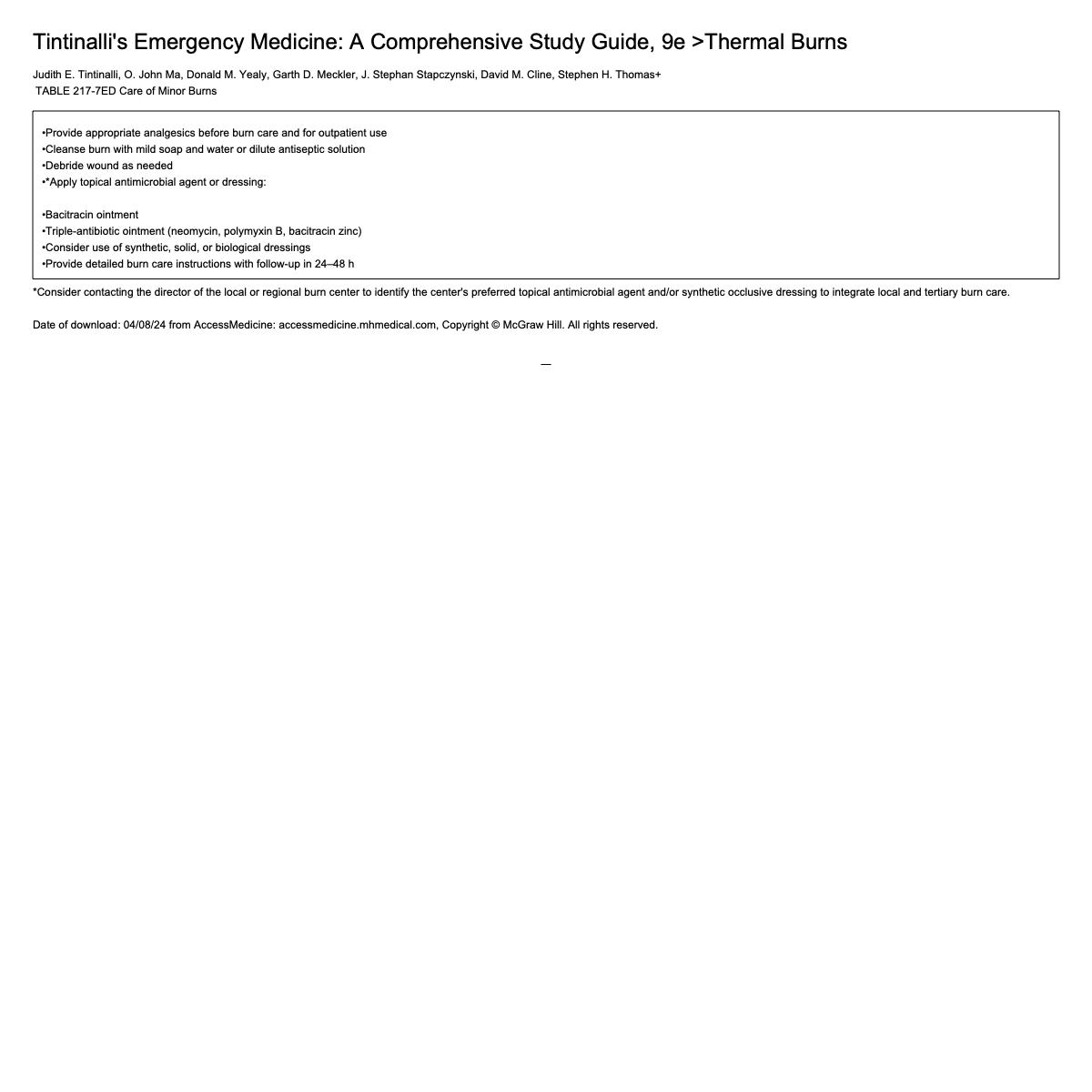
Care of Minor Burns
Minor burns typically qualify for ambulatory care
Should be:
Isolated
Not cross joints
Be circumferential
Should not meet burn center criteria
Care should be given to:
Patient extreme age
Patient with significant comorbidities
Patients with challenging social situations
Patients with inadequate pain control
Principles
Clean burns with mild soap and water
Debride ruptured blister and large intact blisters (small blisters can be left intact)
Tetanus immunization should be assessed
Topical antibiotics are important in reducing bacterial colonization and enhance rate of healing
Dressing should be changed twice daily for as long as wound continues to weep and then → daily until healing is complete
Must discharge patients with:
Appropriate wound care instructions
Adequate pain control
Coordination of outpatient follow up
Inhalation Injuries
Becoming main cause of mortality in burn patients
Associated with closed space fire/conditions that decrease mentation (overdose, alcohol intoxication, drug use, head injury)
Inhalation Injury Mechanism
Thermal injury commonly limited to upper airway
Below the level of vocal cords → occurs more in steam inhalation
Damages endothelial cells, produces mucosal edema of small airways, decreases alveolar surfactant activity
Bronchospasm
Airflow obstruction
Atelectasis
Upper airway edema can occur rapidly
Lower airway edema may not be clinically evident for 24 hours
Over time → tracheal and bronchial epithelial sloughing
About 50% of intubated burn patients → ARDS
Inhalation Injury Diagnosis
Diagnosis made from history
Physical exam
Facial burns
Singed nasal hair
Soot in mouth/nose
Hoarseness
Carbonaceous sputum
Expiratory wheezing
Labs
No single method of labs preferred
Arterial carboxyhemoglobin → can document prolonged exposure to products of incomplete combustion
Imaging
CXR: may be normal initially
Bronchoscopy: may be useful in evaluating extent of injury
Inhalation Injury Treatment
Treat suspected inhalation prior to definitive diagnosis
Humidified oxygen by face mask
Control upper airway with prompt endotracheal intubation
Full thickness burns of face or peri-oral region
Circumferential neck burns
Acute respiratory distress
Progressive hoarseness or air hunger
Respiratory depression or altered mental status
Supraglottic edema and inflammation on bronchoscopy
Fluids: careful fluid resuscitation guided by hemodynamically monitoring to prevent pulmonary edema and ARDS
Chemical Burns Epidemiology
Most exposures occur occupationally
Morbidity and mortality are high
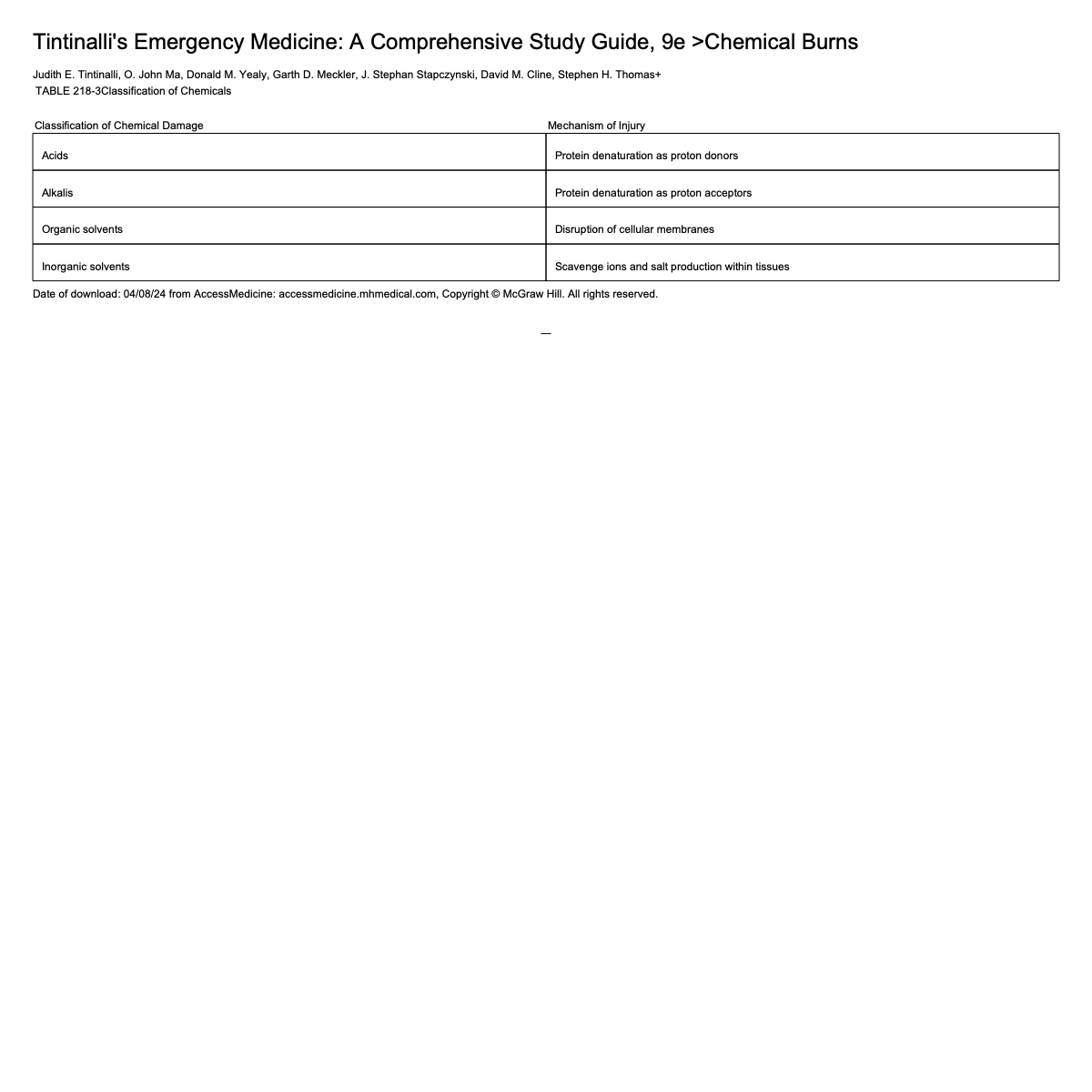
Chemical Burns Pathophysiology
Outer stratum corneum layer of skin functions as barrier → some chemicals can penetrate and produce burns, dermatitis, allergic reactions, thermal injuries, and systemic toxicity
Most chemical burns caused by acids or alkalis
Acids tend to cause coagulation necrosis with protein precipitation → tough/leathery eschar → limits deeper penetration of agent
Alkalis produce liquefaction necrosis and saponification of lipids → poor barrier to chemical penetration allowing deeper burns and persistent tissue injury
Multiple factors influence tissue damage and percutaneous absorption of chemicals
Duration of contact
Concentration of agent
Quantity of agent
Mechanism of action
Extent penetration
Death early after severe chemical burns is related to hypotension, acute renal failure, and hypovolemic shock (can be from systemic toxicity if agent is absorbed)
If there is systemic absorption → acidosis, hypotension, hyperkalemia, dysrhythmia, shock
Chemical Burn Treatment
Initial goal → remove patient from exposure and prevent further exposure
Aggressive large volume irrigation with water
Should be started immediately at scene of accident → chemicals will continue damaging tissue until removed or deactivated and can decrease exothermic reactions
Amount of time to initial dilution or removal of chemical is directly related to eventual depth and degree of injury
Severe alkali burns require several hours of irrigation → pH indicator should be used to check for continued presence of agent in wound and should continue irrigation until pH is normal
Dry chemicals should be brushed away before irrigation
Some chemicals can react with water (sodium metals) → should be covered with mineral oil or excised before irrigation
Once irrigation is complete:
Debride any remaining particles and devitalized tissue
Apply topical antimicrobial agent
Tetanus immunization as needed
Remaining treatment similar to thermal burns
Acid Burns
Perform complete exam of patients with significant acid burns
Can also have respiratory and mucous membrane irritation and skin absorption can result in systemic illness
Most strong acids (other than hydrofluoric acid) produce coagulation necrosis → denaturation of proteins in superficial tissues
Most strong corrosives have pH < 2
Most important chemical burn feature that can be altered by healthcare providers → contact time with skin
Alkali Burns
Penetrate skin deeper and longer than acids → presents greater danger of toxicity from systemic absorption
Wound may initially appear superficial → becomes full thickness burn in 2-3 days
Combines with protein and lipids in tissue → forms soluble protein complexes/soaps → permits passage of hydroxyl ions deep into tissues
Often have production of soft, gelatinous, friable, brownish eschar
Strong alkalies have pH > 12
Electrical Burns Epidemiology
Types
High voltage: > 1,000 V
Low voltage: < 1,000 V
Electrical Burns Pathophysiology
Conductors: materials that allow electrical flow easily
Insulators: materials that do not allow electrical flow
Tissue/Organ properties
Tissue with high fluid and electrolyte content → conduct better than tissue with less
Bone: highest resistance
Nerves and vascular: low resistance
Dry skin: high resistance
Wet-sweaty skin: less resistance
For current to flow through person → complete circuit needs to be created
Current flows through person from one contact area to the other in parallel paths
Electrical Burns Physiologic Effects
Physiologic effects of electric shock related to: amount, duration, and type of current (AC vs DC)
AC: standard household electricity
DC: electricity in batteries and lightning
Both AC and DC can throw patient away from source → blunt injury
AC can be more dangerous than DC
Alternating currents can cause Vfib
AC can produce more muscle tetany → cannot let go of electrical source
Mechanism of Electrical Injury
Risk of serious and fatal electricity injury increases with voltage → associated with severe MSK, visceral, and nervous system injury
Especially > 600 V
High voltage defined as > 1,000 V
Mechanisms
Direct tissue damage from electrical energy
Tissue damage from thermal injury
Mechanical injury from trauma due to fall or muscle contractions
Burns more common with high voltage
Clinical Features of Electrical Burns
Immediate cardiac dysrhythmias
Respiratory arrest
Seizures
Cutaneous burns often seen at electrical contact areas
Entry and exit wounds in DC
Contact wounds in AC
Commonly painless, gray-yellow, and depressed
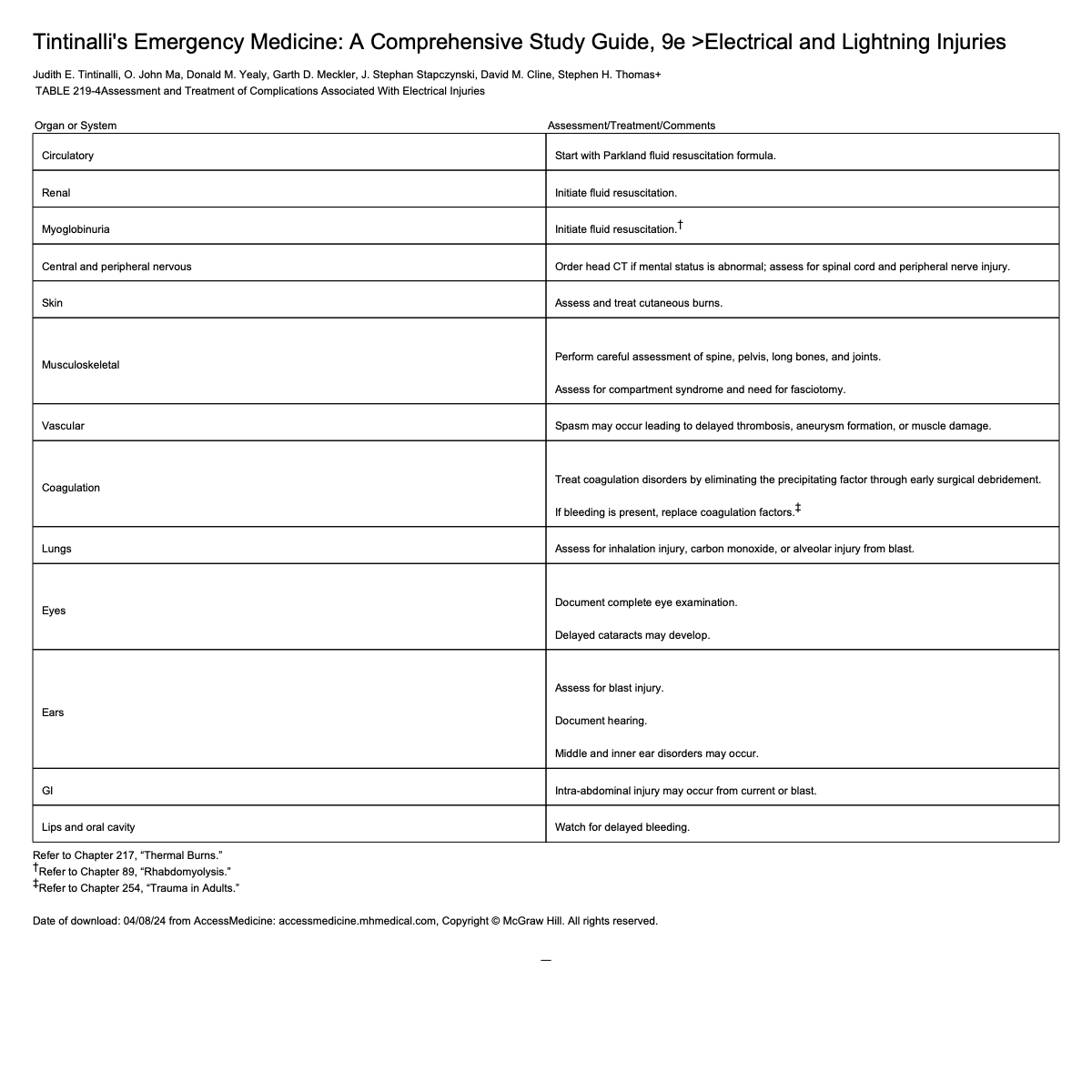
Electrical Burns Treatment
Same as thermal burns
Monitor for cardiac dysrhythmias
Fluid resuscitation guided by Parkland formula
Extensive deep tissue damage may be present even if cutaneous injury is limited → fluid requirements often greater than predicted
Wounds: Principles of Initial Evaluation
Begin with overall patient assessment
Remove rings or other jewelry to prevent constricting bands in settings of edema
Control external bleeding with direct pressure
Replace skin flaps to avoid exacerbating vascular compromise
Amputated fingers/extremities should be kept moist and sterile → place in waterproof bag and on ice to preserve for possible reattachment
Provide some form of anesthesia
Wounds: Risk Assessment
Obtain pertinent patient history
Predictive factors for infection → mechanism of injury, depth, location, configuration, contamination
Determine status tetanus immunization
Keloid Scar
More common in Black and Asian patients
Result in production of excess collagen beyond wound barriers
Should be apart of part of history → any experience may predict poor scar formation
Hypertrophic Scar
Caused by tissue tension during wound healing
Scars stay within the original wound boundaries
Tends to undergo partial spontaneous regression within 1-2 years
Wound Closure Timing
No clearly defined relationship of time to closure of clinical infection
Time from injury to presentation is only one element to be considered before deciding on primary vs delayed wound closure
Should also consider: mechanism, location, degree of contamination, host risk factors, and cosmetic concern
Ex: do not like to close bite wounds immediately because have higher risk of infection and therefore abscess formation
Wound Colonization
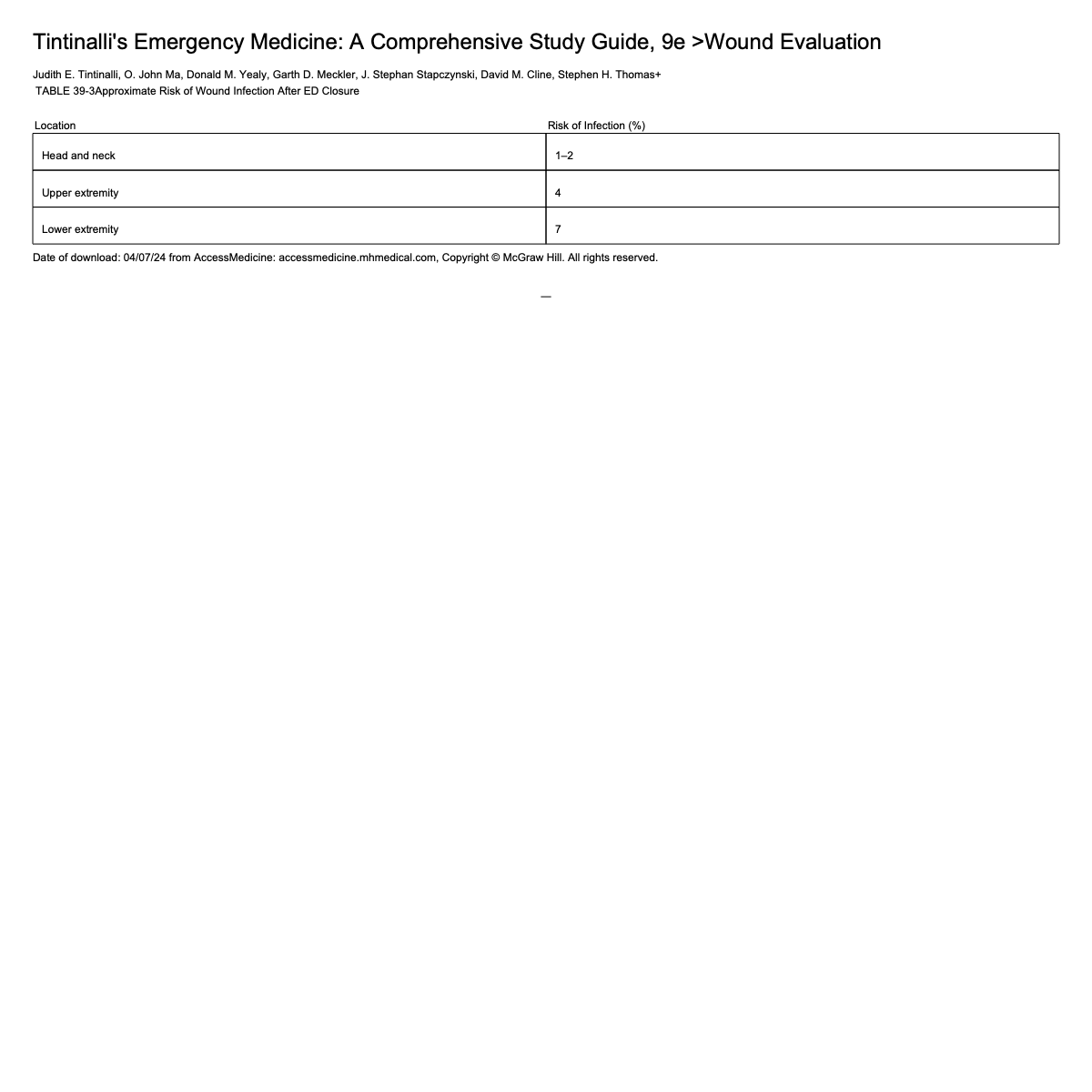
Anatomic location of injury helps to predict clinical outcome both in terms of infection and cosmetic result
Risk of infection is determined by both baseline bacterial colonization and vascular blood supply
Density of bacterial population is low on upper arms, legs, torso
Moist areas have higher bacterial populations, including anaerobes
Wounds on highly vascular areas → less likely to be infected
Role of Imaging in Wounds
Most lacerations do not require imaging
Wounds with concern for foreign bodies can be imaged
Most foreign bodies are much denser → can be seen on X-ray
CT and MRI → useful for identifying and locating object with similar density to tissue
U/S may be helpful but limited in small fragments
Wound Preparation
Wound preparation → aimed at reducing risk of infection, improving cosmetic outcomes, and minimizing pain/discomfort
Try to reposition joint to position assumed during injury to better reconstruct mechanism
Full sterile technique not required
Most lacerations can be repaired with clean non-sterile gloves
Disinfect skin with Chlorhexidine
Wound anesthesia
Most wounds require some form to allow for examination, irrigation, debridement, and repair
Specific choice and route determined by: size, location, patient condition
Most common local → lidocaine
Can consider anxiolysis
General anesthesia for severe wounds/sensitive areas
Wound Irrigation
High pressure irrigation in heavily contaminated
Should irrigate with at least 50-100 cc of fluid: tap water as effective as normal saline
Wound Debridement
Devitalized, nonviable tissue increases risk of infection and poor cosmesis
Remove any non-viable tissue and imbedded foreign bodies → reduces bacterial burden in traumatic wounds
Can be done using scalpel or fine scissors
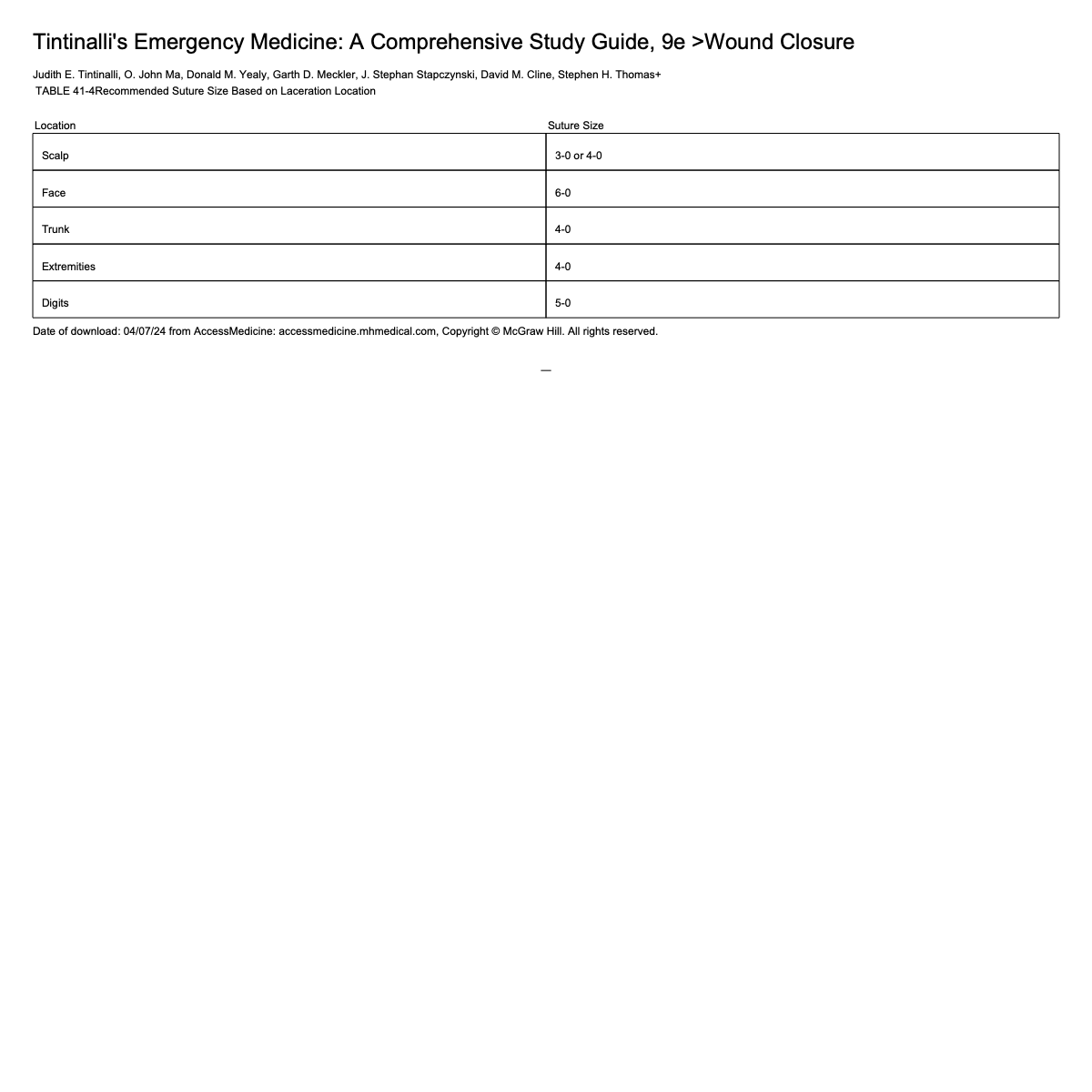
Wound Closure
Can be closed by:
Sutures
Staples → better for head wounds
Adhesive tapes
Tissue adhesives
Hair apposition
Sutures
In the ED: the choice between adsorbable and non-adsorbable material for percutaneous sutures is clinically irrelevant
Larger diameter material produces more damage to tissue and leaves larger holes → should use thinner material when possible
Lower number → higher diameter → bigger hole
Sutures: Non-adsorbable
Retain tensile strength for at least 60 days
Most often used to close outermost layer of skin or repair tendons
Avoid deep vascularized tissue → have to go back in to remove, which can cause more damage
Origin and structure
Monofilament: preferred for non-adsorbable
Polybutester: can elongate which can be useful if wound edema is anticipated
Nylon and polypropylene: cannot expand and may lacerate wound edges if tissues swell
Sutures: Adsorbable
Lose their tensile strength in < 60 days
Better for deep structures and high tension wounds
Have many different types (do not need to know the different types)
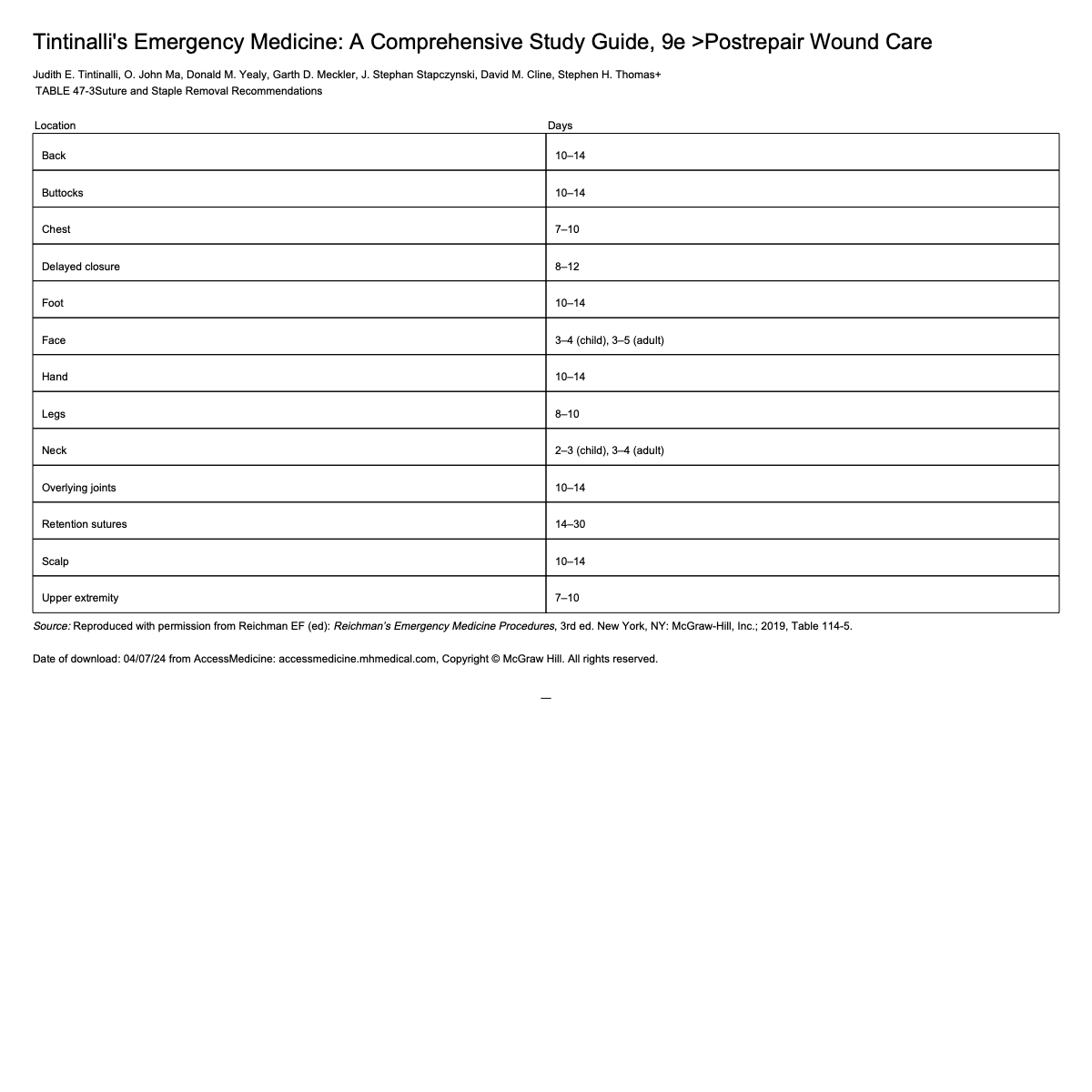
Timing of How Long Sutures Stay In
Should know that there are recommendations but do not need to know specific recommendations
Wound Dressing
Sutured or stapled lacerations can be covered with protective non-adherent dressing for 24-48 hours
Maintain moist environment to increase rate of re-epitheliazation (occluded wounds heal faster than those exposed to air)
Topical antibiotic creams can be used to maintain moist environments → should not be used if tissue adhesives used because it can prematurely break adhesive
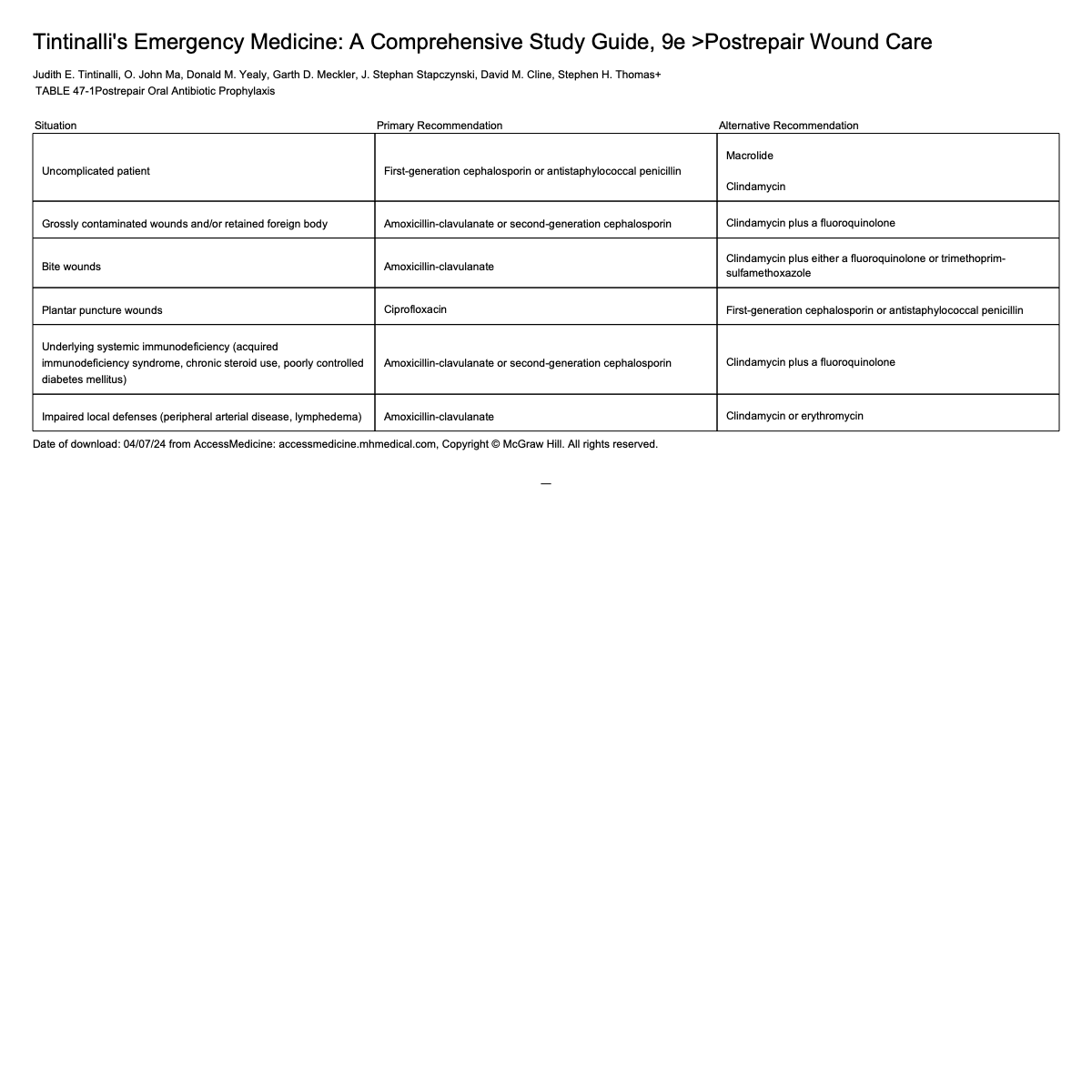
Prophylactic Antibiotics
Not recommended except for select circumstances
Human bites
Cat bites
Deep dog bites
Bite wounds to hand
Open fractures
Wounds that expose joints/tendons
Compulsive wound cleaning is far more important to reduce post repair infection
Bite wounds → Augmentin
Uncomplicated → cefalexin
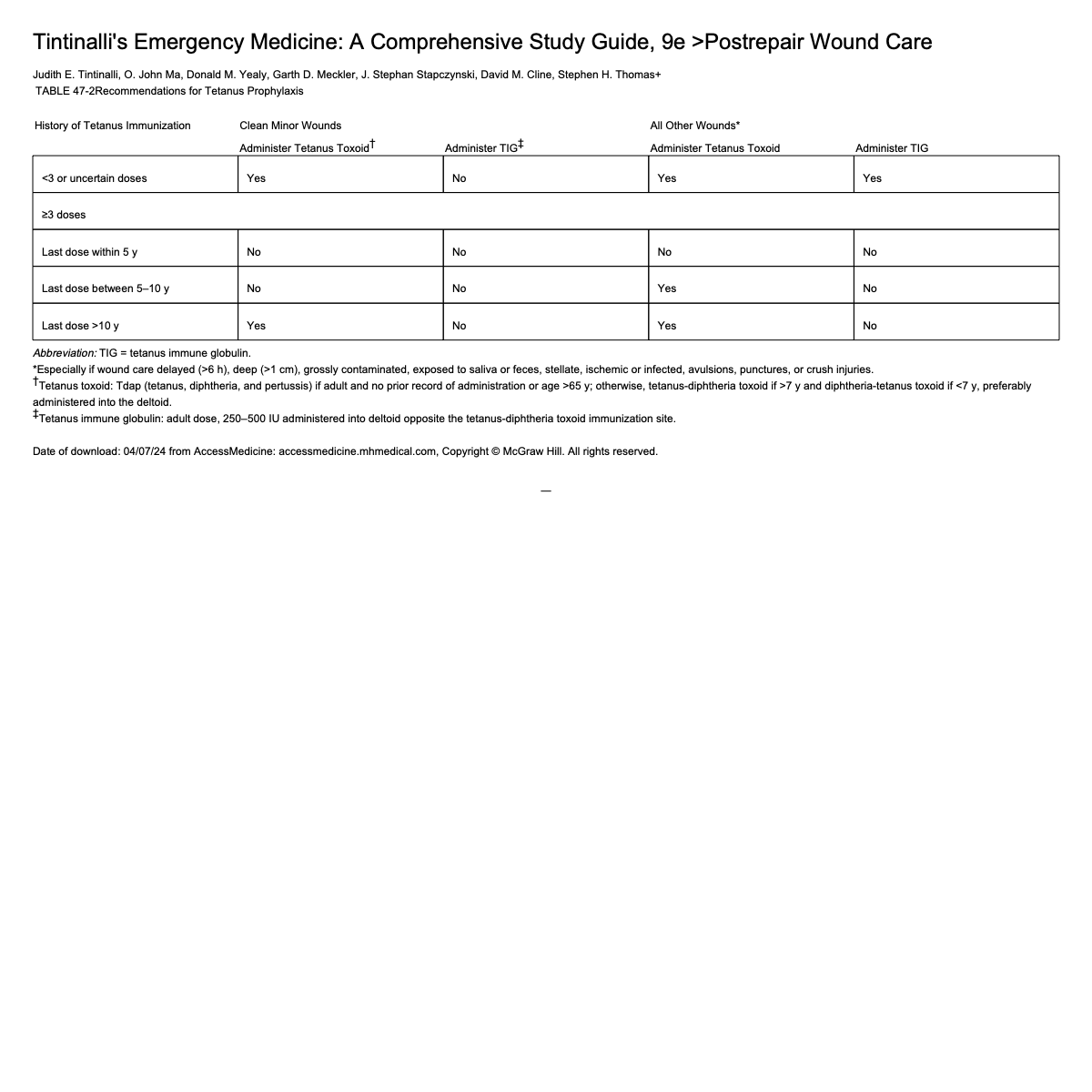
Tetanus Recommendations
Mammalian Bites
Most bites in ED from domestic dog or cat
Complications
Mechanical injury from bite itself
Local bacterial infection
Systemic infection or illness
In most animal bite wounds, there is isolated soft tissue injury → wound management and prevention of infection are key issues
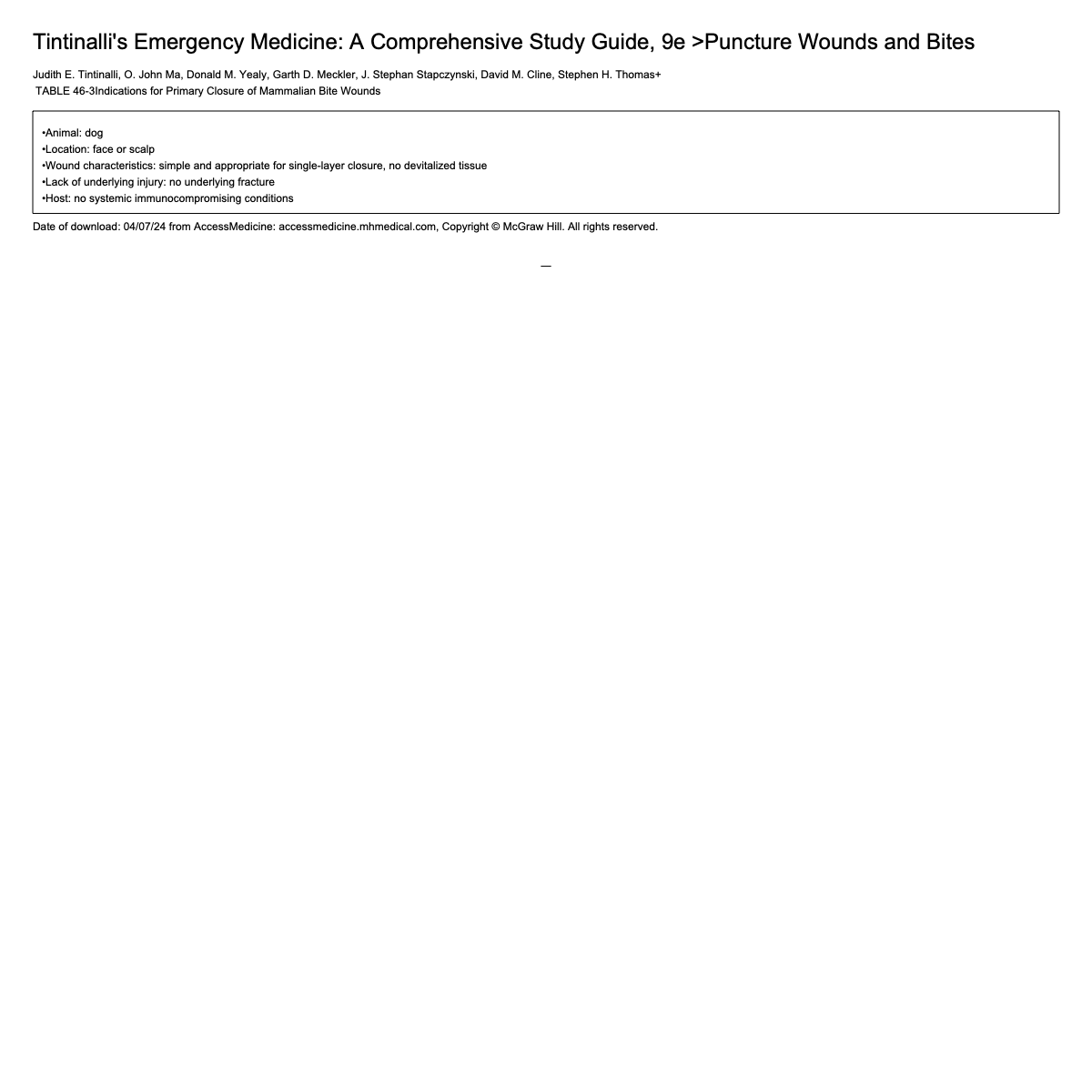
Some bites can undergo primary repair → increased risk of post repair wound infection
Should give prophylaxis with Augmentin
Non-closure or delayed primary closure is applicable for management of contaminated bite injuries, especially areas other than face
Wounds with Highest Risk of Infection
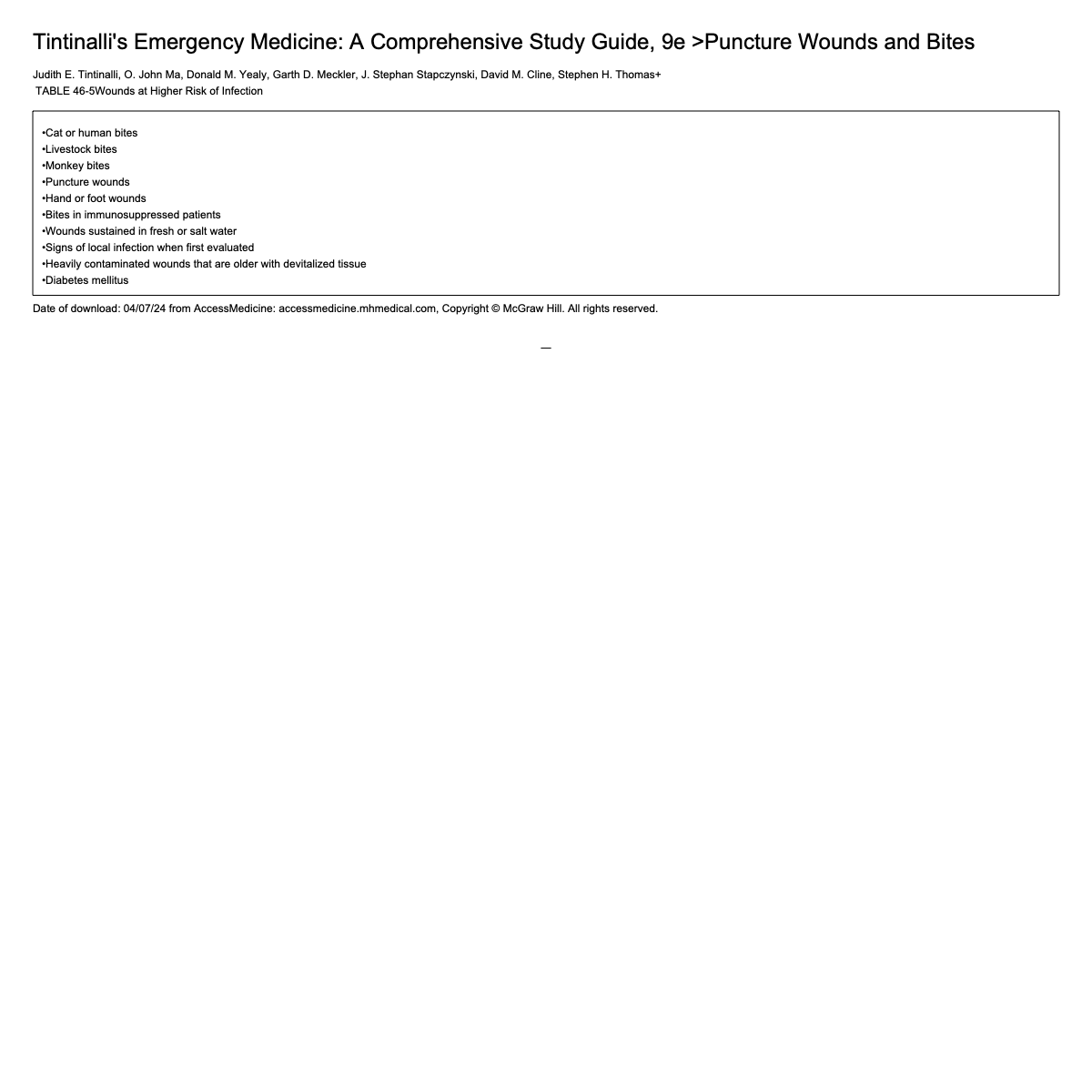
Cat and Dog Bites
Most dog bite wounds are relatively superficial → may not need antibiotics
Up to 50% of cat bites will become infected if not treated due to sharper teeth and deeper wounds
Should use prophylactic antibiotics on higher risk uninfected wounds
All cat bites
Immunocompromised patients
Dog bite puncture wounds
Hand wounds
Wounds undergoing surgical repair
Human Bites
More serious than domestic animals
HSV can cause herpetic whitlow after human bite with infected saliva
Usually polymicrobial → most commonly staph and strep
Adequate initial agent → cephalexin or can also use Augmentin
Prophylaxis should be considered after all but trivial human bites