MD5 - Anti androgens
1/86
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
87 Terms
what are anti androgens?
Anti-androgens are substances that block the effects of androgens, which are male sex hormones like testosterone and dihydrotestosterone (DHT). They can work in a few ways:
Receptor blockers – they attach to androgen receptors in cells, so testosterone or DHT can’t activate them.
Production inhibitors – they reduce the body’s production of androgens.
what are common anti androgens, medicines?
Common Anti-Androgen Medications
Spironolactone – blocks androgen receptors and lowers androgen production.
Bicalutamide and flutamide – mainly used for prostate cancer.
Finasteride and dutasteride – block the conversion of testosterone to DHT, often for hair loss.
finasteride specifically blocks the enzyme 5alpha reductase from turning testosterone to dht. so giving this drug means theres less dht, less shrinkage of hair follicles oin the scalp and so we get hair growth onthe scalp but maintenance of hair on the face like beard hair.
Q1: What is the prostate?
The prostate is a male gland located below the bladder that surrounds the urethra and produces fluid to support sperm.
Q2: Why can prostate problems make it hard to pee?
Because the prostate surrounds the urethra, enlargement or cancer can compress it, leading to difficulty urinating or inability to pee.
Q3: What hormone is crucial for prostate development?
Testosterone, the primary male sex hormone, is key for the development of the testicles and the prostate.
watch anatomy for proostate caner, normal vs affected
Q3: What hormone is crucial for prostate development?
Testosterone, the primary male sex hormone, is key for the development of the testicles and the prostate.
Q4: How does prostate cancer depend on testosterone?
Early prostate cancer cells need testosterone to grow, so they are called testosterone-dependent
Q5: What does androgen independence mean in prostate cancer?
It means the cancer no longer requires testosterone to grow and continues to progress even if testosterone levels are low.
Q6: What are the stages of prostate tissue changes leading to cancer?
Normal prostate epithelium
Benign prostatic hyperplasia (needs testosterone)
Low-grade prostatic intraepithelial neoplasia (PIN)
High-grade PIN
Metastatic prostate cancer
Androgen-independent cancer
Q7: Why is early detection of prostate cancer important?
Because early-stage cancer is often testosterone-dependent and may respond to hormone therapy, while later androgen-independent cancer is harder to treat.
Q1: Does prostate cancer always start needing testosterone?
Yes. Early-stage prostate cancer is testosterone-dependent, meaning it grows in response to testosterone.
Q2: What does androgen independence mean in prostate cancer?
Androgen independence means the cancer no longer needs testosterone to grow and can proliferate even when testosterone levels are low.
Q3: Why do older men often have trouble urinating?
As men age, the prostate can enlarge (benign prostatic hyperplasia), which can compress the urethra and make it harder to pee.
Q4: What is low-grade prostatic intraepithelial neoplasia (PIN)?
Low-grade PIN is a precancerous change in prostate cells. It marks the early stages that may lead to prostate cancer but usually does not change testosterone levels.
Q5: Where does prostate cancer commonly metastasize?
The most common site of metastasis is bones, especially the spine, pelvis, and ribs. Direct bladder invasion is rare.
Q6: How does prostate cancer become androgen-independent?
Through mutations or amplification of the androgen receptor gene, prostate cancer cells can grow without needing testosterone.
Q7: What is the role of testosterone in the prostate?
Testosterone is crucial for the development of the testicles and prostate and fuels the growth of both normal prostate tissue and early-stage prostate cancer.
Q8: What are the typical stages leading from normal prostate to androgen-independent cancer?
Normal prostate epithelium
Benign prostatic hyperplasia (testosterone-dependent)
Low-grade PIN → High-grade PIN (precancerous)
Metastatic prostate cancer (still testosterone-dependent initially)
Androgen-independent prostate cancer
Q1: What is watchful waiting and when is it used?
Watchful waiting is monitoring prostate cancer without active treatment, typically used for slow-growing tumors in frail or older men.
Q2: What is active surveillance and when is it used?
Active surveillance involves careful monitoring with regular tests, often used for small tumors confined to the prostate in otherwise healthy men.
Q3: What is the role of surgery in prostate cancer?
Surgery (usually prostatectomy) removes the prostate and is frequently used for tumors confined to the prostate, but it can have major side effects such as urinary incontinence and erectile dysfunction.
Q4: When is hormone therapy used for prostate cancer?
Hormone therapy is used for hormone-dependent tumors, which rely on testosterone to grow. It reduces testosterone levels or blocks its effect.
Q5: When is chemotherapy used for prostate cancer?
Chemotherapy is used for hormone-independent tumors or cancer that has relapsed after hormone therapy.
Q6: What is high-intensity focused ultrasound (HIFU) used for?
HIFU is used to debulk prostate tumors, targeting the tumor tissue with focused heat to destroy cancer cells.
Q7: When is external beam radiotherapy used?
External beam radiotherapy is often used for small tumors confined to the prostate, delivering targeted radiation to kill cancer cells.
Q8: What is permanent seed brachytherapy?
Permanent seed brachytherapy involves implanting radioactive seeds directly into the prostate, used for tumors confined to the prostate.
Q1: How does testosterone promote prostate cancer cell proliferation?
Testosterone binds to the androgen receptor (AR), causing a conformational change. The AR-T complex moves into the nucleus and activates genes that drive cell proliferation, which can promote tumor growth.
Q2: What does “translocation” mean in this context?
Translocation means the AR-T complex moves from the cytoplasm into the nucleus to regulate gene expression.
Q3: How does hormone therapy work in prostate cancer?
Hormone therapy (androgen deprivation therapy) reduces testosterone levels or blocks AR, preventing testosterone from driving cancer cell proliferation.
Does chemotherapy block testosterone from binding to the androgen receptor?
A4: No. Chemotherapy kills rapidly dividing cells but does not block testosterone binding; that’s the role of hormone therapy.
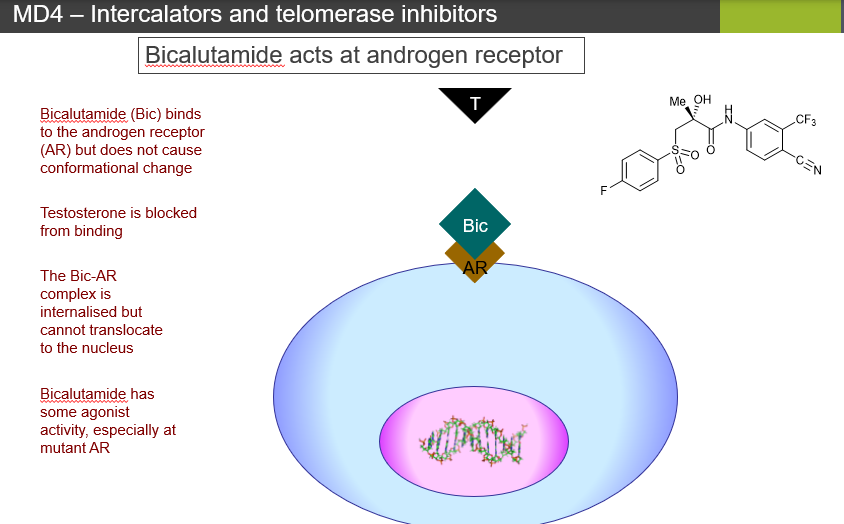
Q1: What type of drug is bicalutamide?
A1: Bicalutamide is a receptor blocker (competitive inhibitor) that blocks testosterone from binding to the androgen receptor.
Q2: How does bicalutamide affect the androgen receptor?
A2: It binds the AR without causing a conformational change, preventing the receptor from translocating to the nucleus and activating gene transcription.
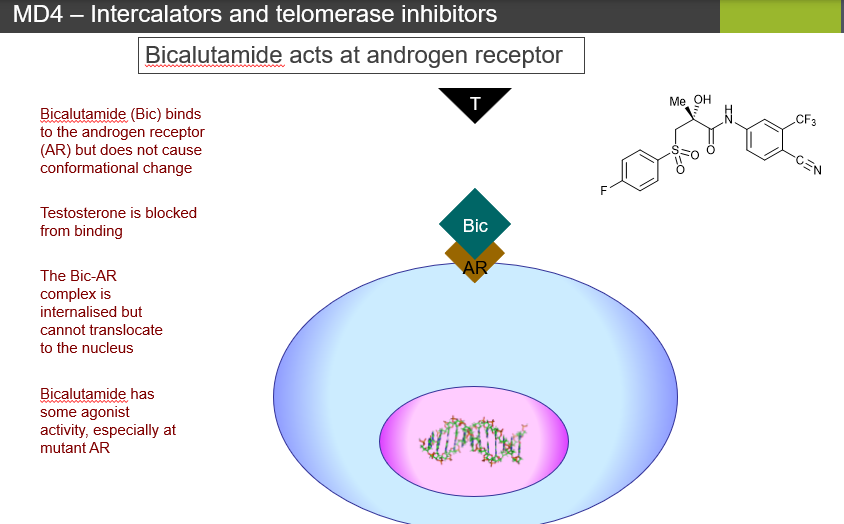
Q3: Can bicalutamide ever stimulate the androgen receptor?
A3: Yes, it has partial agonist activity, especially with mutant androgen receptors.
Q4: What happens to the AR-bicalutamide complex inside the cell?
A4: The complex is internalized in the cytoplasm but cannot enter the nucleus to signal. Over time, normal receptor recycling may degrade some AR.
Q5: How do cells respond to prolonged bicalutamide treatment?
A5: Cells may increase the number of androgen receptors (upregulation), which can allow some proliferation despite the drug.
Q6: Name newer androgen receptor blockers and their uses.
enzalutamide = widely replacing bicalutamide, rare CNS toxicity.
Apalutamide – used in nm-CRPC.
Darolutamide – nm-CRPC, short half-life.
Q7: What is the key difference between bicalutamide and testosterone signaling?
A7: Testosterone-AR complexes translocate to the nucleus and activate proliferation genes, while bicalutamide-AR complexes stay in the cytoplasm and do not signal.
Q1: How does enzalutamide work?
Enzalutamide binds to the androgen receptor, blocks testosterone from binding, and prevents the receptor from activating gene transcription.
Q2: Does enzalutamide cause a conformational change in the androgen receptor?
No. Enzalutamide does not cause a conformational change, so the receptor remains inactive.
Q3: Can the enzalutamide-AR complex enter the nucleus?
No. The complex is internalized in the cytoplasm and cannot translocate to the nucleus.
Q4: Does enzalutamide have any agonist activity?
No. Unlike bicalutamide, enzalutamide has no agonist activity, even with mutant receptors.
Q5: What is the main advantage of enzalutamide over bicalutamide?
A5: Enzalutamide completely blocks AR signaling without partial agonist activity, making it more effective in advanced or castration-resistant prostate cancer.
between bicalutamide and enzalutamide, Q1: Which drug has partial agonist activity, and which has none?
Bicalutamide can have partial agonist activity, especially with mutant AR, while enzalutamide has no agonist activity.
check against lecture slides
Q2: How do the AR complexes differ between the two drugs in terms of nuclear translocation?
Both Bic-AR and Enz-AR complexes cannot translocate to the nucleus, but enzalutamide’s blockade is more complete, without triggering compensatory proliferation.
Q3: What happens to testosterone binding in both drugs?
: Both bicalutamide and enzalutamide competitively block testosterone from binding to the AR.
Q4: How does the cell’s response differ between the two drugs?
With bicalutamide, cells may upregulate AR or sometimes proliferate via partial agonist activity. With enzalutamide, cells cannot activate AR signaling, making it less likely for proliferation to occur despite AR upregulation.
Q1: How does testosterone bind to the androgen receptor (AR)?
A1: Testosterone binds in a special pocket in the AR called the ligand-binding domain.
This pocket has hydrophobic (water-fearing) areas that snugly fit the steroid rings of testosterone.
It also has hydrophilic (water-loving) areas where hydrogen bonds form with the –OH groups of testosterone.
Together, these interactions lock testosterone in place, allowing the AR to change shape and activate genes
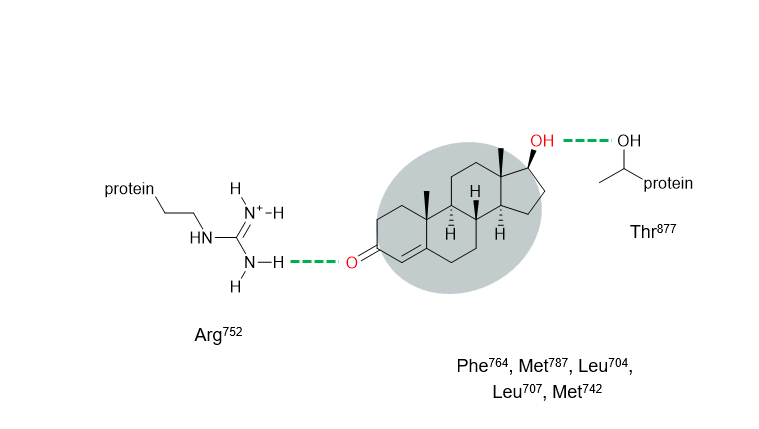
Q2: What is the role of amino acids like Arg752, Thr877, Phe764, Met742, Met787, and Leu704?
These are specific building blocks (amino acids) of the AR protein that interact with testosterone:
Arg752 and Thr877 → polar, can form hydrogen bonds with testosterone’s –OH group. Think of it like a “handshake” holding testosterone.
Phe764, Met742, Met787, Leu704 → nonpolar/hydrophobic, create a sticky pocket that fits the steroid rings snugly.
This combination of hydrophobic “grip” and hydrogen bonding “handshake” ensures the hormone stays in the right position to activate the receptor.
Q3: What does “hydrogen bonding” mean in this context?
A hydrogen bond is a weak interaction between a H atom on one molecule and an o2 (or N atom) on another.
In testosterone binding: the –OH (hydroxyl) group on testosterone can form a hydrogen bond with Arg752 or Thr877 in the AR.
These bonds are like small magnets, holding testosterone in exactly the right orientation to trigger receptor activity
Q4: What is the “hydrophilic zone” and “hydrophobic zone” in the AR pocket?
Hydrophilic zone (water-loving) → where polar interactions like hydrogen bonds happen (e.g., with Arg752, Thr877).
Hydrophobic zone (water-fearing) → where nonpolar parts of testosterone fit snugly against amino acids like Phe764, Met742, Met787, Leu704.
Together, these zones stabilize testosterone in the receptor, like a key fitting perfectly into a lock.
Q5: Why is this binding important for prostate cancer?
A5: When testosterone binds to AR:
The AR changes shape (conformational change).
The AR moves into the nucleus of the cell.
The AR turns on genes that tell the cell to grow and divide.
In prostate cancer, this is a problem because it drives uncontrolled cell growth.
Drugs like bicalutamide and enzalutamide block testosterone from binding, preventing AR from activating genes, and slowing cancer growth.
Does bicalutamide bind to the androgen receptor the same way as testosterone?
No. Bicalutamide binds slightly differently from testosterone.
why doesnt bicalutamide bind to the AR the same way as t?
Bicalutamide binds slightly differently from testosterone.
While testosterone forms hydrogen bonds with Thr877, bicalutamide mainly interacts with Asn705 instead.
This small difference changes how the AR behaves, preventing the normal conformational change that testosterone causes
Q2: What is the role of the fluorophenyl group in bicalutamide?
The fluorophenyl group is a chemical part of bicalutamide that fits into a hydrophobic side pocket of the AR.
This helps anchor bicalutamide in the receptor.
By occupying this pocket, it blocks testosterone from binding properly.
Q3: Why does this different binding prevent AR activation?
Because bicalutamide:
binds without causing the usual shape change in the AR.
Forms an AR complex that stays in the cytoplasm and cannot move to the nucleus.
Prevents gene activation that would normally drive cell growth.
This is why bicalutamide blocks testosterone-driven proliferation in prostate cancer cells.
Q4: How is bicalutamide’s binding advantage different from testosterone?
Testosterone’s binding activates AR, driving growth, while bicalutamide’s slightly different binding:
Does not activate AR (mostly antagonist).
Blocks testosterone from binding.
Can occupy additional hydrophobic pockets that testosterone does not, making the blockade stronger.
How does bicalutamide bind differently to the androgen receptor compared to testosterone?
Testosterone forms hydrogen bonds with Thr877 and fits snugly in the main ligand-binding pocket to activate AR. Bicalutamide instead binds to Asn705 and occupies a hydrophobic side pocket, preventing AR from changing shape and staying inactive.
Q2: What is a hydrophobic side pocket in the androgen receptor?
It’s a small nonpolar cavity next to the main binding pocket. Nonpolar groups, like bicalutamide’s fluorophenyl group, can fit there. This stabilizes the drug in the receptor and blocks testosterone from binding.
Q3: Why is the fluorophenyl group important for bicalutamide’s function?
the fluorophenyl group fits into the hydrophobic side pocket, acting like an extra anchor. This keeps bicalutamide bound tightly, prevents the receptor from activating, and blocks prostate cancer cell growth.
Q4: How does bicalutamide’s binding stop gene activation and cancer growth?
A4: By binding slightly differently than testosterone and occupying the side pocket:
AR cannot undergo the normal conformational change.
AR stays in the cytoplasm and cannot enter the nucleus.
Genes that drive cell proliferation are not turned on, slowing cancer growth
Q1: How effective is enzalutamide in metastatic castration-resistant prostate cancer (mCRPC)?
A1: Enzalutamide can extend median survival by 4–5 months, but resistance is common.
Q2: What is the difference between primary and acquired resistance?
Primary resistance: cancer is not sensitive to enzalutamide from the start.
Acquired resistance: cancer initially responds but recurs or progresses after treatment.
Q3: How can AR gene amplification cause enzalutamide resistance?
amplification, cancer produces more androgen receptors, so the drug cannot block all of them. Some ARs still signal for cell growth.
Q4: How can AR mutations cause resistance?
Certain mutations can convert enzalutamide from an antagonist to an agonist, meaning the drug promotes growth instead of blocking it. This usually happens with one specific drug, not all AR blockers.
Q5: What are AR splice variants, and why are they important?
Splice variants are truncated forms of AR that may lack the drug-binding site, allowing AR signaling to continue despite enzalutamide. They often appear after castration or AR-targeted therapy.
Q6: How do metabolic changes lead to resistance?
Cancer cells can make more androgens or upregulate steroid synthesis, which can overwhelm enzalutamide and allow AR signaling to continue.
Q7: What is lineage plasticity in prostate cancer resistance?
Lineage plasticity occurs when cancer cells reprogram themselves epigenetically, becoming AR-independent. They no longer rely on testosterone signaling, so AR blockers like enzalutamide stop working.
How much can enzalutamide extend survival in castration-resistant metastatic prostate cancer, and why is resistance important?
Enzalutamide can extend median survival by 4–5 months, but resistance is common, which means cancer often recurs or progresses despite treatment.
What is the difference between primary and acquired resistance to enzalutamide?
Primary resistance: the cancer does not respond to the drug from the start.
Acquired resistance: the cancer initially responds but later progresses or recurs.
Q3: How does AR gene amplification lead to enzalutamide resistance?
Cancer cells produce more androgen receptors (ARs). With more receptors than the drug can block, some ARs remain active, allowing continued signaling and cancer growth.
Q4: How can AR mutations cause enzalutamide resistance?
Some mutations change the AR so that enzalutamide acts like an agonist instead of an antagonist.
This means the drug starts promoting growth rather than blocking it.
These mutations are usually specific to one drug, so other AR blockers may still work.
Q5: What are AR splice variants, and why do they matter for resistance?
Splice variants are truncated forms of the AR that often lack the part of the receptor that enzalutamide binds.
They appear more often after castration or treatment with enzalutamide/abiraterone.
Their exact role in resistance is still not fully clear, but they can allow AR signaling to continue.
Q6: How do metabolic changes in cancer cells contribute to resistance?
Cancer cells can increase androgen production or upregulate steroid synthesis, producing more testosterone or related hormones than enzalutamide can block.
This can overwhelm the drug, allowing AR signaling to continue.
What is lineage plasticity, and how does it make prostate cancer resistant to enzalutamide?
: Lineage plasticity occurs when cancer cells reprogram themselves through epigenetic changes, becoming AR-independent.
These cells no longer need testosterone signaling, so AR-targeted drugs like enzalutamide stop working entirely.
What is CYP17A1 and what is its role in testosterone production?
CYP17A1 is an enzyme that converts progesterone into 17α-hydroxyprogesterone, a key step in testosterone synthesis. Its heme iron active site and arginine residues help stabilize the steroid and perform oxidation reactions.
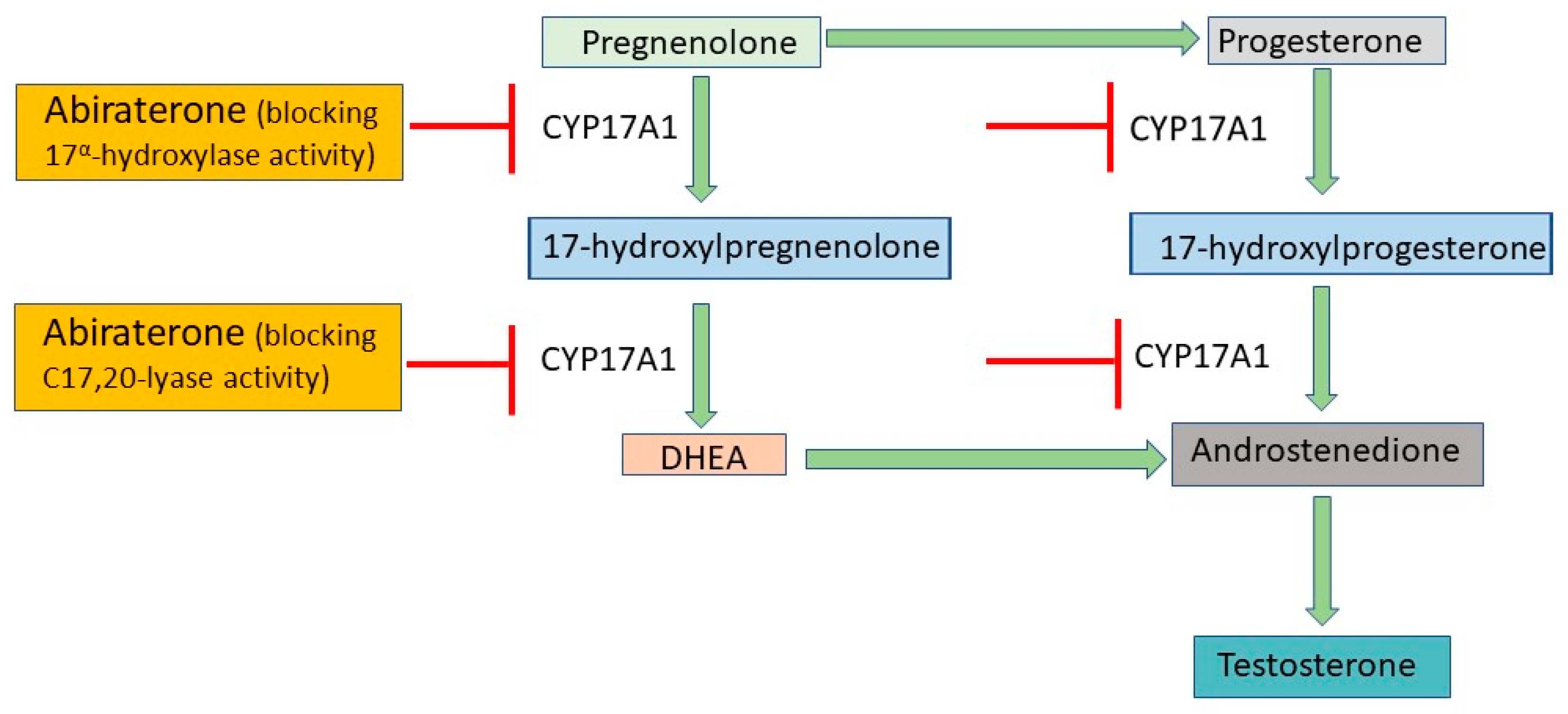
Q2: Why is CYP17A1 a target in prostate cancer therapy?
Prostate cancer often depends on testosterone for growth, so blocking CYP17A1 reduces testosterone, starving hormone-dependent cancer cells.
Q3: How does abiraterone work?
Abiraterone selectively binds to CYP17A1, especially the heme iron, blocking testosterone synthesis.
Q4: What is abiraterone acetate?
Abiraterone acetate is a prodrug that is converted in the body to active abiraterone, which then inhibits CYP17A1.
Q5: How is ketoconazole different from abiraterone?
Ketoconazole is a non-specific CYP inhibitor, weaker and originally an antifungal. Abiraterone is selective for CYP17A1, making it a stronger anti-androgen therapy.
Q1: What does it mean when a prostate cancer is androgen-dependent?
Androgen-dependent prostate cancer requires testosterone to grow. These cancers rely on androgen receptor (AR) signaling to drive cell proliferation.
Q2: What is androgen-independent prostate cancer?
Androgen-independent prostate cancer no longer requires testosterone to grow. These cancers often develop after long-term therapy and are harder to treat with hormone-blocking drugs.
How can androgen-dependent prostate cancers be treated at the receptor level?
They can be treated by blocking the androgen receptor (AR) with drugs such as:
Flutamide
Nilutamide
Bicalutamide
Enzalutamide
Apalutamide
Darolutamide
These drugs bind to AR through hydrogen bonds, hydrophobic interactions, and by occupying the side pocket, preventing testosterone from activating the receptor.
How can androgen-dependent prostate cancers be treated at the hormone production level?
They can be treated by inhibiting testosterone synthesis in the testes and adrenal glands via CYP17A1 inhibitors, such as:
Ketoconazole
Abiraterone
Abiraterone acetate (prodrug of abiraterone)
Q5: How do CYP17A1 inhibitors work?
they block testosterone production by binding to CYP17A1, using:
Ligation to the heme iron (Fe) in the enzyme
Hydrogen bonds and hydrophobic interactions
Complementary shape of the drug to the active site
Q6: What is the difference between abiraterone and abiraterone acetate?
abiraterone acetate is a prodrug, meaning it is converted in the body to active abiraterone, which then inhibits CYP17A1 and reduces testosterone production.
optional resource that TIM mentioned to look at and is useful. (may be useful for exma). SAVED AS MD5- ANTI ANDROGENS PAPER