637 Ch15 ICU Monitoring
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
What are 5 indications of declining cardiac status?
ST changes
Onset, increase, or change of foci of PVCs
Onset of Vtach or Vfib
HB progression
Loss of pacemaker spike
What are 5 examples of noninvasive ICU monitoring equipment?
ECG
Pulse Ox for sPO2
Capnography for ETCO2 (PaCO2 at end of exhaled breath)
Blood pressure cuff oscillometric technique
RR through movement of ECG electrode waveforms
LOC outcome measures, sensors, questions etc.
What are examples of invasive ICU monitoring equipment?
Arterial line
Venous line
Pulmonary artery catheter/Swan-Ganz catheter
Temperature monitoring (brain probe, urinary catheter, esophagus probe, nasopharyngeal probe, rectal)
ICP
If the ECG alarm goes off what does this mean and what should you do?
Alarm indicates change in rate or rhythmic/poor pad placement or movement
Must identify cause of alarm before silencing it w/ CI approval
Where can SpO2 be monitored? What should the SpO2 be in the ICU? What are limitations to an accurate read?
Finger, ear, toe (finger probe best)
Above 88%
Dark nail polish, jaudnice, abnormal Hgb, anemia, intravascular dyes, dark skin pigmentation, states of low perfusion (hypothermia, vasoconstriction, low CO)
*What does capnography measure? How is the waveform measured? What is a normative value? What indicates that there is hypoventilation vs hyperventilation?
Measures end tidal CO2 (ETCO2) which is PaCO2 at end of exhaled breath
Waveform height = CO2 depleted, length = duration of exhalation
35-45 mmHg
*Hypoventilation = Long length of plateau, very high height (holding onto CO2)
*Hyperventilation = Short length of plateau, not as high height (excessive blowing off of CO2)
How is noninvasive BP measured?
Monitored by the oscillometric technique, cuff proximal to antecubital space or LE, postpones need for arterial line
How is noninvasive respiratory rate measured? What is a normal RR for an adult?
Monitored as a waveform from movement of ECG electrodes
12-18 breaths/min for adult
*What are causes of altered RR, tachypnea vs bradypnea?
Tachypnea
Exercise
Atelectasis
Fever
Hypoxemia
Anxiety/emotional distress
Pain
Asthma
PULMONARY EMBOLISM
Pneumonia
ARDS
Anaphylaxis
HF
Shock
DKA
Neuromuscular disorders
COPD
Bradypnea
Head injuries
Sedation
Drug overdose
Increased ICP
Diabetic coma
Exhaustion caused by severe airway obstruction
Sleep apnea
Obesity hypoventilation syndrome
*How does DKA and diabetic coma affect RR?
DKA - tachypnea
Diabetic coma - bradypnea
If you are suspicious of a PE, how would the patient’s RR be altered?
Tachypnea
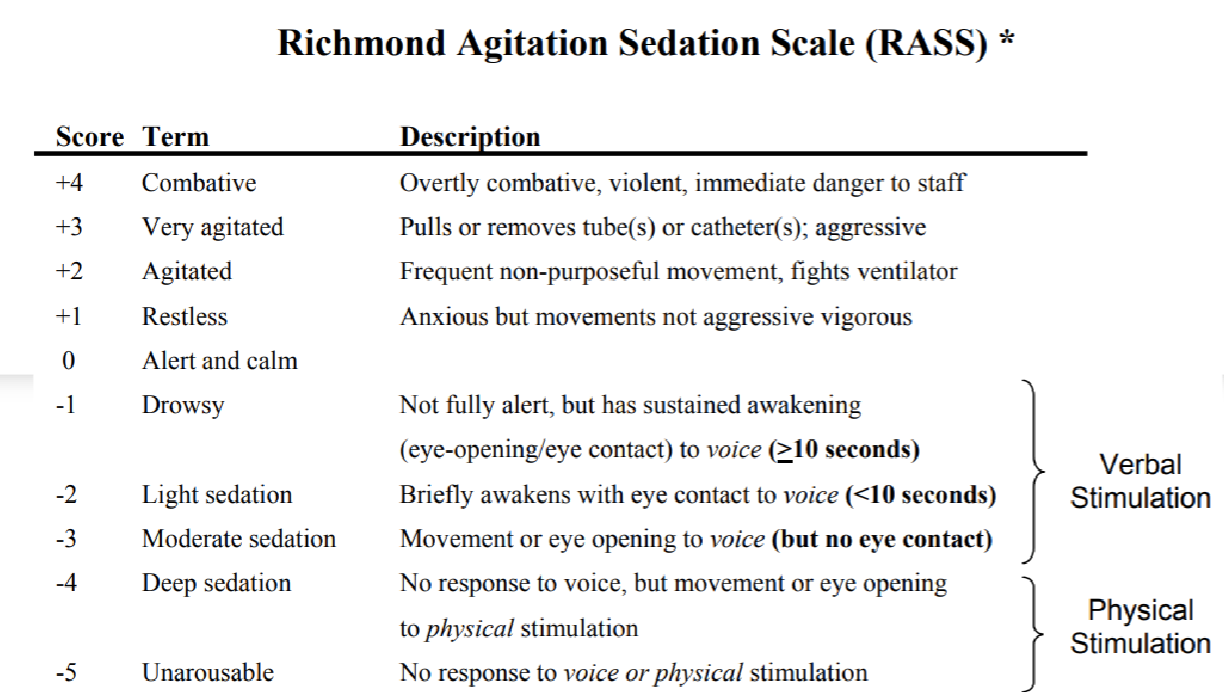
*What are 3 ways to measure LOC?
Richmond Agitation Sedation Scale (RASS)
Confusion assessment method in the ICU scale
Bispectral index (BSI) - sedation levels in ICU
*Describe the scoring on the RAAS scale.
*What does an arterial line do? Who typically gets one? Where is it inserted and how often do you monitor it? What do you do if it gets dislodged? What activities do you want to avoid? Ideal positioning of transducer?
Intraarterial BP monitoring
Hemodynamically unstable, risk for instability, low SV, excessive peripheral vasconstriction
Radial, femoral, brachial, axillary, ulnar, or dorsalis pedis; monitor before, during, and after for bleeding
Dislodged → apply pressure, notify nursing ASAP
Avoid w/b on UE w/ arterial line
*Lower transducer = higher BP, higher transduer = lower BP; ideal @ RA
If the arterial line gets dislodged, what do you do?
Apply pressure
Immediately notify nursing staff
What are 6 indications for an arterial line?
Continuous BP measurement
Frequent analysis of ABGs
Frequent sampling of blood for critical lab values
Drug admin
Use of an intraaortic balloon pump (IABP)
Hemodynamic monitoring for cardiac parameters and fluid status
Why would you want an arterial line for a pt w/ COPD?
If fluctuating pH, want to monitor ABGs
What are signs for carpal tunnel after insertion of arterial line?
Persistent pain and paresthesia
Where is a venous line inserted? What does it measure and what happens when it is increased/reduced? What else can it be used for? Where is a PICC line inserted?
Central (jugular/subclavian to superior vena cava) or peripheral
Measures central venous pressure (CVP) or right atrial pressure (RAP) for fluid status & cardiac fx
Increased CVP - hypervolemia/fluid overload, tricuspid insufficiency, ventricular failure
Reduced CVP - hypovolemia/low blood volume, dehydration
Also for meds, fluids, blood sampling, temporary pacemaker, port = central venous catheter
PICC peripheral access - cephalic, basilic, brachial to superior vena cava
What happens with increased vs reduced CVP?
Increased CVP - hypervolemia/fluid overload, tricuspid insufficiency, ventricular failure
Reduced CVP - hypovolemia/low blood volume, dehydration
What is a pulmonary artery catheter/Swan-Ganz catheter? What is it used for? Where does the transducer need to be? What does a high/low SvO2 mean?
Inserted into central v & pulmonary a; ballon at tip of catheter inflated for pulmonary capillary wedge pressure or left sided filling pressures
Used for:
LVF
Mitral/aortic valve dysfunction
Pulm edema
pHTN
Hypovolemic states
Transducer @ RA, midaxilla
High SvO2 = bad perfusion, low SvO2 = high O2 consumption, low CO
Why do you want to measure temperature invasively? For what type of patients? Examples? Gold standard?
Multiorgan dysfunction → met & sys issues
Comatose pts
Brain temp w brain probe urinary catheters, esophagus probe, nasopharangeal probe, rectal
Gold standard - Swan-Ganz Catheter, not for routine use
Is a pulmonary a. catheter/Swan-Ganz Catheter good for routine use?
No, but is the gold standard for temp monitoring
*Why would you want to measure intracranial pressure invasively? What is a normal ICP range for adults and children under 6 y/o? What is the target cerebral perfusion pressure (CPP)? What kind of ICP & CPP will you see after a brain injury? What helps reduce ICP?
Intracranial hypertension from neurologic insults i.e. TBI, hypoxic brain damage, aneurysm, hemorrhage, cerebral tumor, meningitis, brain surgery
*ICP <10 mmHg adults, 0-5 mmHg children under 6 y/o
CPP 50-70 mmhg
Brain injury → High ICP causes low CPP
Hyperventilation reduces ICP
What kind of activities increase ICP? How can we reduce ICP?
Isometric exercise
Valsalva maneuver
Extreme hip flexion
Lateral neck flexion
Coughing
Prone
Head position below 15 degrees horizontal
Occlusion of the tube
Pain
Manually influence ventilation b/c hyperventilation reduces ICP
What is the ideal position for venous drainage for patients w/ high ICP?
HOB >30deg
What does non-invasive positive pressure ventilation (NPPV) do? Two examples/gold standard?
Provides vent support for those w/ acute/chronic vent failure and NM disease
1. CPAP - gold standard for OSA, pressure THROUGHOUT, less intense
2. BiPAP - two levels of pressure, high during inspiration, low during exhalation, more intense, can be used if pt cannot handle CPAP
What is a nasal cannulae (NC) used for? Complications? What kind of flow is a high flow nasal cannulae (HFNC)? How does it differ?
NC - Low and medium dose O2 flow 1-6L/min
Dryness if >4L/min → humidifier
HFNC - high dose O2 flow >6L/min, ALWAYS used w/ heat & humidification
Reduce CO2 in upper airways and work of breathing
What are reasons for using high flow O2?
Hypoxemic respiratory failure
Postextubation
Preoxygenation before intubation
Attempt to avoid intubation
Acute pulmonary edema
Transport of the critically ill
Pts who have DNR/DNI orders
What are the 5 masks for O2 delivery? Describe them.
Simple mask
pts who mouth breathe/have nasal restriction; 5-10L/min
Aerosol mask
for aerosolized meds (i.e. bronchospasm), + nebuillizer, 10-12L/min
Reservoir mask
attached to reservoir bag, some/no rebreathing of gases, tightly sealed & uncomfy
Partial - first 1/3 exhaled into bag, 2/3 vented out
Non-rebreather - no rebreathing of exhaled air
Venturi mask
Mixed O2 w/ room air with a side port/holes
Tracheostomy
Collar placed over open stoma, pt weaning from vent
What are four purposes of artificial airways? Indications? Cardinal signs of dangerous airway obstruction?
Bypass upper airway obstruction
Assist/control respirations over prolonged period of time
Facilitate care of chronic RTIs
Prevent aspiration of oral & gastric secretions
Indications
Restlessness
Tachycardia
Confusion
Motor dysfunction
Decreased O2sat
Obstruction if: stridor & full chest wall retractions
Cyanosis: late and ominous sign
What is a passy muir valve?
speaking valve/button for tracheostomy
If a pt with a trach is gasping what do you do? If the trach is shifting up and down what do you do?
Call a code
Call nursing