OB/PEDS Final Exam
1/58
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
59 Terms
Infant Age
Birth - 1 year
Toddler Age
1-3 years
Preschool Age
3-6 years
School Age
6-12 years
Adolescence Age
12-18 years
Infant VS
HR 100-160
RR 30-60
BP 50-75/30-45
Toddler VS
HR 70-110
RR 20-30
BP 90-105/55-70
Preschooler VS
HR 65-110
RR 20-25
BP 95-110/60-75
School Age VS
HR 60-95
RR 14-22
BP 100-120/60-75
Adolescent VS
HR 55-85
RR 12-18
BP 110-125/65-85
Sensorimotor
Birth - 2 years
causality & object permanence
Preoperational
2-7 years
take what you say literally
Concrete Operational
7-11 years
Cannot think hypothetically; must use visual demonstration
Have them explain things back to you
Formal Operational
11 years to adulthood
Start to understand disease processes and outcomes
Things can be explained with words/without visual demonstration
Trust v. Mistrust
Infant
Autonomy v. Shame & Doubt
Toddler
Initiative v. Guilt
Preschool
Industry v. Inferiority
School Age
Identity v. Role Confusion
Adolescent
GTPALM
G - # of Pregnancies including current
T - # of Pregnancies that have gone to term (20 weeks)
P - # of Preterm births
A - # of Abortions
L - # of Living children
M - # of Multiple pregnancies
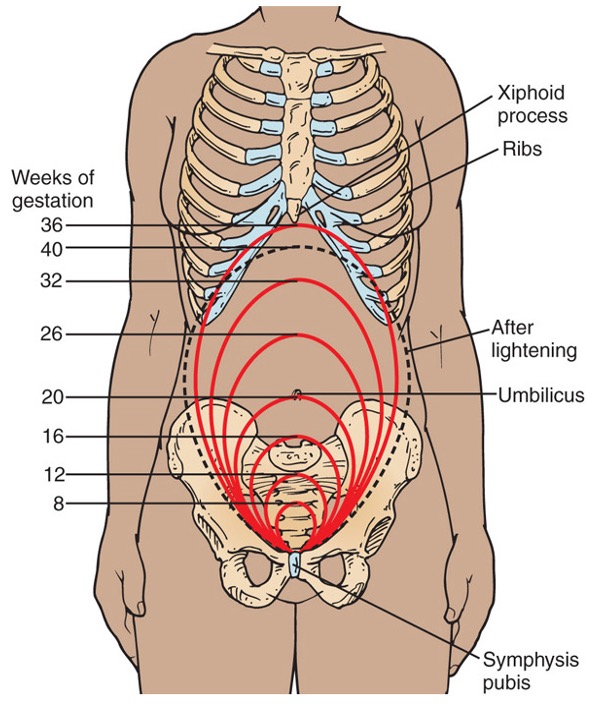
Normal Fundal Height for Gestational Age
Presumptive Signs of Pregnancy
Subjective (felt by woman)
P - Period absent
R - Really tired
E - Enlarged breasts
S - Sore breasts
U - Frequent urination
M - Fetal movement felt by mom
E - Emesis & nausea
Probable Signs of Pregnancy
Objective (Observed by HCP)
P - Positive pregnancy test or Pigment changes
R - Leukorrheal thick discharge
O - Outline of fetus palpable
B - Ballottement (return of the fetus when tapped)
A - A softening of the cervix (Goodell’s sign)
B - Blueish color of the cervix (Chadwick’s sign)
L - Lower uterine segment softens (Hegar’s sign)
E - Enlarged uterus/abdomen
Positive Signs of Pregnancy
F - Fetal movement felt by HCP
E - Electronic detection of Fetal Heart Tones
T - The delivery of the fetus
U - Ultrasound
S - Movement seen by HCP
Naegele’s Rule
First day of LMP - 3 months + 7 days
Preterm Labor Risk Factors
Hx of preterm labor
African American
IVF
Intimate partner violence
Late or no prenatal care
Strenuous job
Lack of support
Alcohol or drugs
Infection
Preterm Labor Management
Antenatal steroids for fetal lung development
Tocolytics - reduce contractions
Magnesium Sulfate
Preterm Premature Rupture of Membranes (PRROM) Management
Between 34-36 weeks:
Labor induction
Abx therapy
Before 33 weeks:
Bed rest
Corticosteroids - Betamethasone
Abx therapy
Amnioinfusion
No cervical checks if mom is not in active labor
Gestational Hypertension Manifestations and Labs
no multisystem disturbances consistent with preeclampsia
BP is > or equal to 140 systolic AND 90 diastolic at two separate appointments
No proteinuria
Preeclampsia Manifestations
> or equal to 160 systolic and/or 110 diastolic at two separate appointments
Edema of the face, upper extremities and lungs with increased pitting edema in lower extremities
Proteinuria, oliguria (<30ml/hr)
Kidney and liver damage
Weight gain of >2lbs/week
Eclampsia Manifestations
Cerebral edema in brain causing
Headache
Visual disturbances
Seizure, hyperreflexia
Coma
HELLP Syndrome Manifestations
Malaise
N/V, RUQ tenderness
Bruising, petechia, edema
Headache, visual disturbances
Preeclampsia, Eclampsia & HELLP Syndrome Labs
Thrombocytopenia (<100000)
Decreased RBC
Creatinine >1.1
Increased AST & ALT
CBC, BMP, LFT, Urinalysis
Gestational Diabetes - Glucose Tolerance Testing
1 hour glucose tolerance test
if it is 140 or higher schedule 3 hours glucose tolerance test
3 hour glucose tolerance test
must have two of the 4 glucose levels in the chart for a diagnosis
3-Hour Glucose Tolerance Test | |
Test time | Pregnant glucose level |
Fasting | ≥ 95 mg/dL |
1 hour | ≥ 180 mg/dL |
2 hours | ≥155 mg/dL |
3 hours | ≥ 140 mg/dL |
Hyperemesis Gravidarum S/S
Persistent vomiting leading to dehydration and electrolyte imbalances
Poor skin turgor, dry mucus membranes
Weak, dizzy, lightheaded
Low BP, high HR, decreased urine output, concentrated urine
Hyperemesis Gravidarum Treatment
Ginger or peppermint
Reduce odors
IV hydration
monitor lab values
NPO
Meds: Antihistamine H1 receptor blockers, ondansetron, and B6 or B12
Iron-deficiency Anemia S/S
Pallor, fatigue, weakness, and malaise
Reduced exercise tolerance and dyspnea
Anorexia, pica
Edema
Hemoglobin below 10-11
Hematocrit below 33%
Menstruation
Episodic uterine bleeding in response to cyclical normal changes that brings ovum to maturity and renews uterine tissue bed.
3-7 days, 5 on average
Starts from 9-16 years old, average of 12
Average of a 28 day cycle with ovulations typically occurring 14 days before next menses
Involves hypothalamus (LHRH/GnRH), Anterior pituitary glad (FSH & LH), Ovaries (progesterone & estrogen), and the uterus
Conception
Usually occurs in the outer third fallopian tube and must occur quickly
Ovum viable for 24-48 hours
Spermatozoon viable for 48-72 hours
Causative Factors of Male Infertility
Hormone deficiencies
Gonadotoxins
Impaired sperm transport
Risk Factors of Male Infertility
Excessive alcohol use
Marijuana or cocaine use
Advanced age
STI
SmokerA
Causative Factors of Female Infertility
Anovulation
PID, endometriosis, or uterine fibroids
Cervical mucus factor
Vaginal problems
Acidic pH kills sperm
Risk Factors of Female Infertility
Diabetic
Excessive alcohol use
Obesity
Advanced age
STI
Oxytocin Challenge Test / Contraction Stress Test
A small amount of oxytocin is administered to trigger contractions to see how FHR responds to contractions
Mom is hooked to EFM and TOCO
Baseline FHR is taken before beginning procedure
Mom should have 3 contractions that last 40-60 seconds within a 10 minutes period
If baby has decels during half the contractions it can indicate baby is not well-oxygenated
Monitor mom for 30 minutes post-procedure
Non-stress Test
Mom is put in semi-fowlers and hooked up to EFM and TOCO and Mom presses clicker when she feels fetal movement and it is marked on the EFM
Done after 28 weeks
Measures the FHR in response to fetal movement
2 Accels occur with fetal movement within a 20 minute period indicated baby is well oxygenated
Less than 2 accels in a 40 minute period is a non reassuring result
If result is non reassuring try to stimulate/wake baby by eating or using VAS
Amniocentesis
A needle is inserted into the amniotic sac to draw up and evaluate amniotic fluid color and test for genetic disorders
Performed between 15 and 20 weeks
Ultrasound to find where to place needle
Mom hooked up to EFM and TOCO and observed until 30 minutes post-procedure
Can be used to treat polyhydraminos
Chorionic Villus Sampling
Cell sample from placental villi that can be used to detect chromosome abnormalities, genetic disorders, and be used for DNA testing
Performed week 10-12
Rh negative moms should receive rhogam after procedure
Kick Count Education
Recommended to record daily kick counts starting at 28 weeks
Baby should kick at least 4 times per hour or 10 times in 2 hours
If baby kicks less than 3 times in one hour or less than 4 times in two hours see HCP
WBC for Pedi
5000-13000
RBC for Pedi
3.2-5.2
Hemoglobin for Pedi
11-12.5
Hematocrit for Pedi
35-45%
Bilirubin for Newborns
1-12
Creatinine for Pedi
0.4-1.2
Phenylalanine
3-9
Chloride Sweat Test
20
>60 = Cystic Fibrosis
Iron Level
7-14
Lead Level
<9
Thyroid Levels