CM II Week 5 (Seizures/Epilepsy)
1/121
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
122 Terms
At the level of the neuron...
glutamate vs GABA
Glutamate: Excitatory NT ... excess glutamate. Seizure: too much excitation (glutamate) without enough inhibition
GABA: Inhibitory NT
Seizure
signs or symptoms caused by electrical hyper synchronization of neuronal networks in the cerebral cortex
Epilepsy
an enduring predisposition to generate epileptic seizures. Neurobiological, cognitive, psychological, and social consequences are present
Clinical definition of Epilepsy (what criteria you must meet to categorize as epilepsy)
1. At least TWO unprovoked seizures > 24 hrs apart (excludes clustered seizure pts.)
2. One unprovoked seizure and high risk of recurrence (over next 10 years)
3. Previous Diagnosis of epilepsy syndrome (ex. juvenile myoclonic seizures)
What clinical variables determine high risk of seizure recurrence in patients?
1. Prior Brain Insult (stroke, seizure, meningitis)
2. Epileptiform EEG
3. Abnormal CT/ MRI (cortical dysfunction)
4. Nocturnal seizure (wake up w/ seizure)
Epidemiology of seizure disorders
affects 8-10% of population
Epilepsy 0.5% of population
Seizures make up 1% of ED visits
What age groups are more susceptible to seizures and epilepsy
Very young (<20)
Very Old (>70)
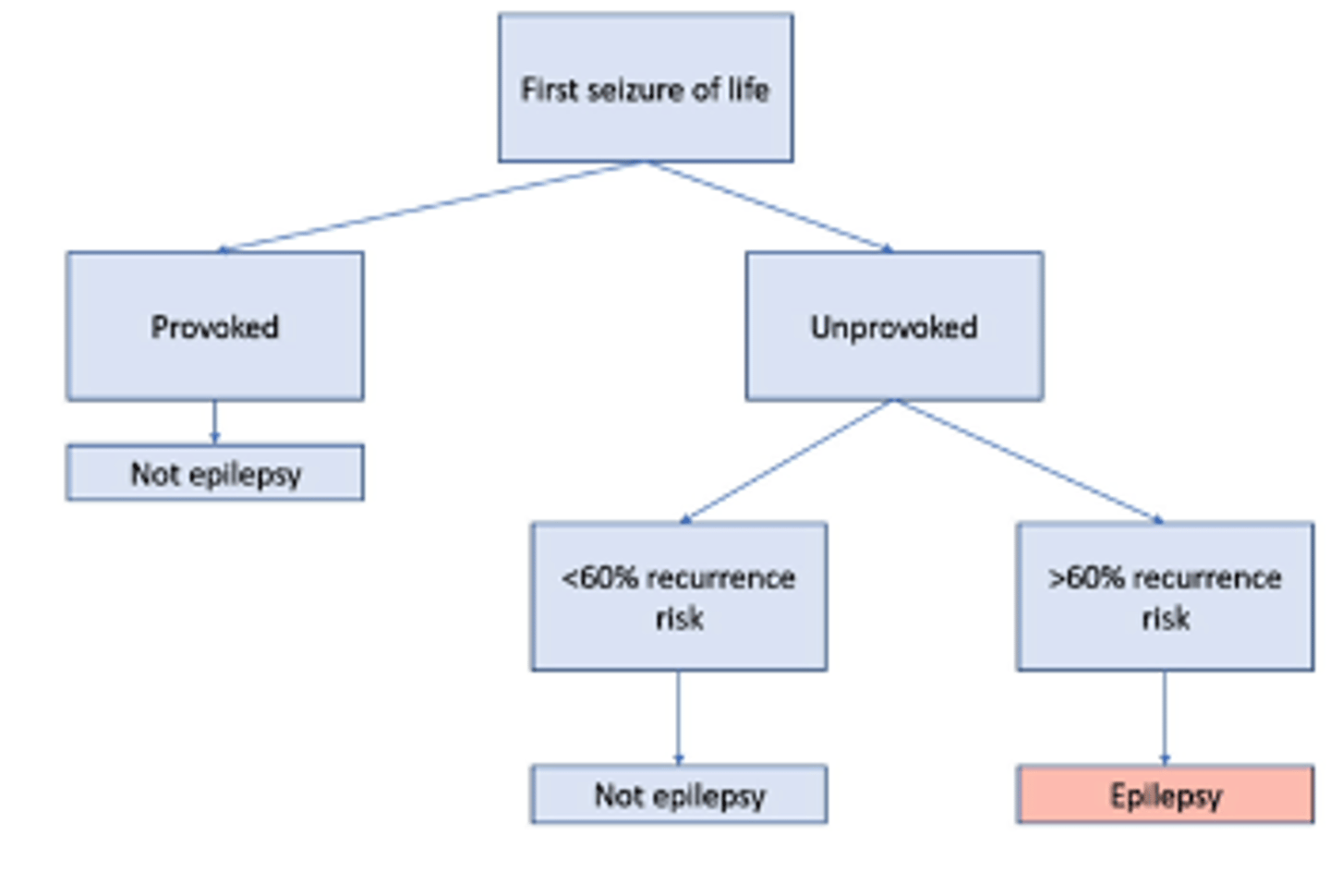
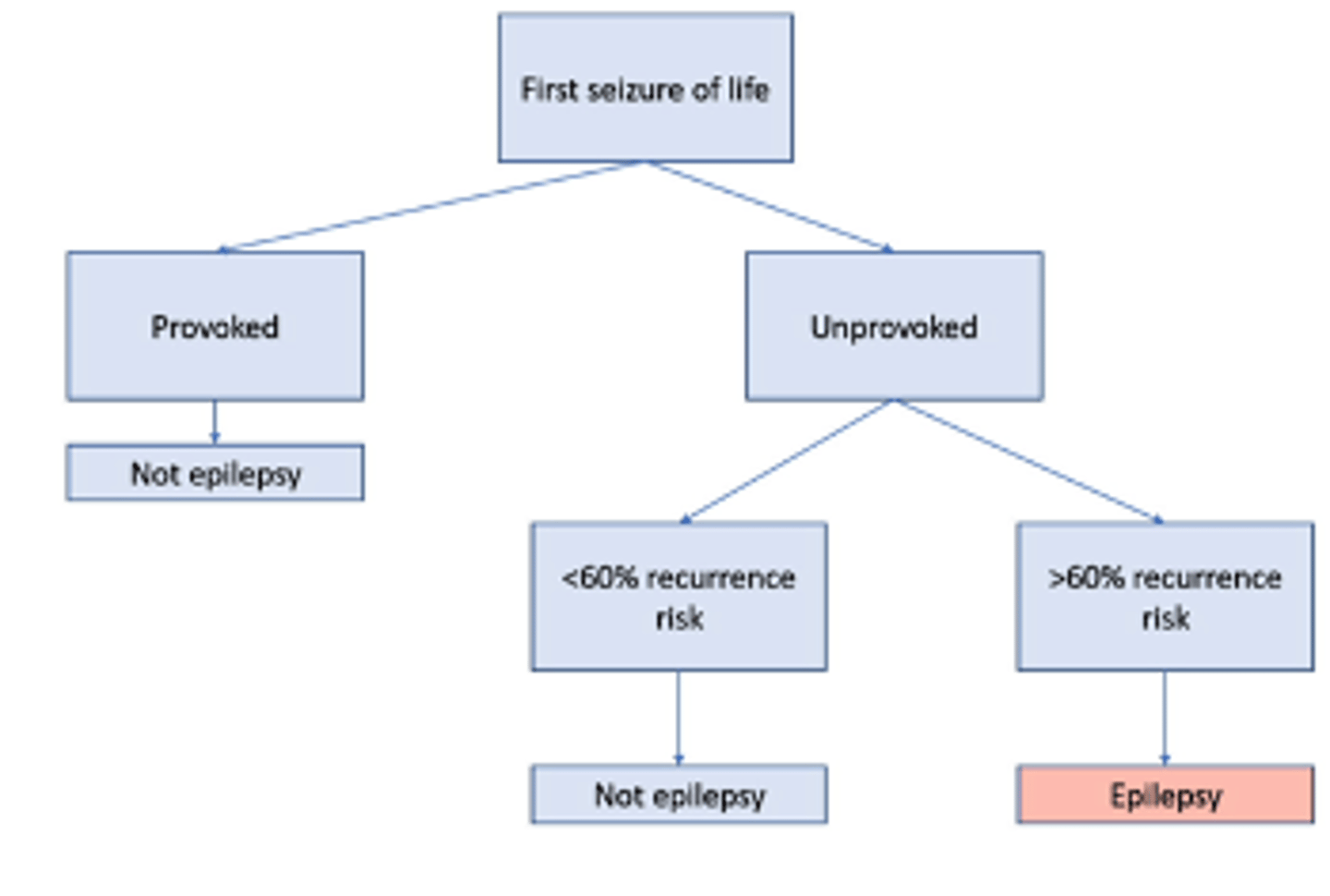
Acute symptomatic seizure
"provoked seizure" occurring with systemic insult or acute brain insult
insults include metabolic derangements, drug/alcohol withdrawal, and acute neurologic disorders such as stroke, encephalitis, or acute head injury
25-30% of first seizures are...
acute symptomatic/provoked seizures
What is the recurrence rate of provoked seizures?
Less than 20%
Unprovoked seizure
a seizure of unknown etiology as well as one that occurs in relation to a preexisting brain lesion or progressive nervous system disorder
What type of seizure is spontaneous?
Unprovoked
seizures occur spontaneously and expected to recur in the absence of treatment
Has no obvious cause so will need to obtain hx, epilepsy risk factor, imaging
List acute neurologic illnesses that may cause seizures
Stroke
Intracranial hemorrhage
Subarachnoid hemorrhage
Subdural Hemorrhage
Anoxic brain injury
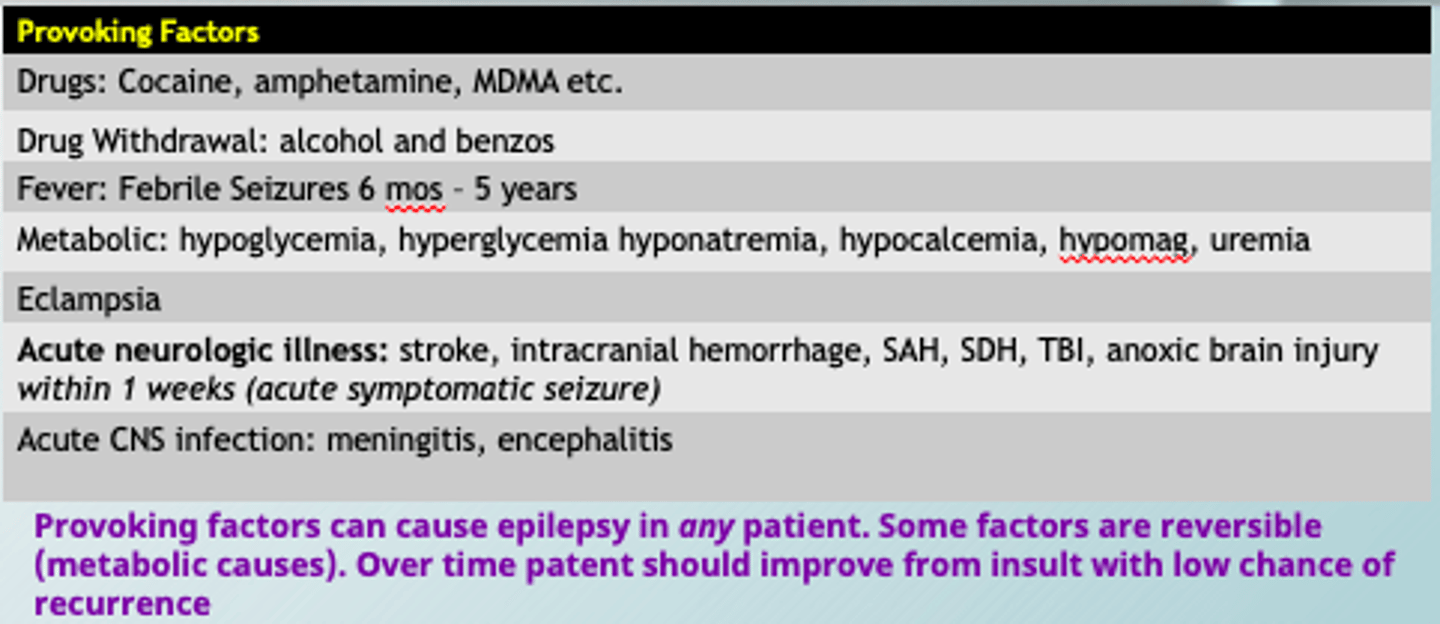
Example of reversible factor that could cause seizure
Metabolic causes: hyper/hypoglycemia, hyponatremia, hypocalcemia
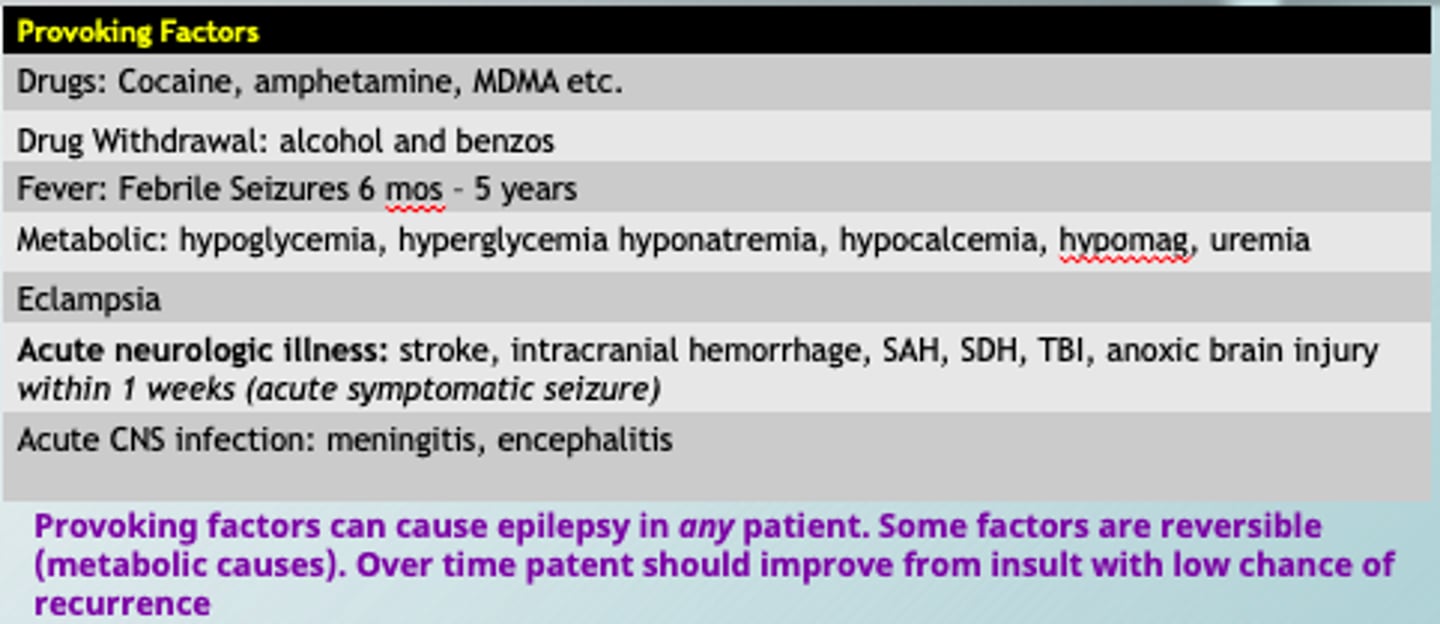
Provoking factors can cause epilepsy in?
Provoking factors can cause epilepsy in any patient. Some factors are reversible (metabolic causes). Over time patent should improve from insult with low chance of recurrence
Triggers for Seizures
Seizure Triggers causes seizures in those with epilepsy due to lowering their seizure threshold
Sleep Deprivation
Bright lights
Alcohol intoxication AND WITHDRAWAL
ASM (anti-seizure) noncompliance
provoking factors for seizures
strong enough to cause a seizure in ANYONE without epilepsy
Can provoked seizures be considered epilepsy?
NO
Can an unprovoked seizure cause future epilepsy?
YES if there is a >60% chance of recurrence
Causes of childhood epilepsy are typically...
genetic
metabolic (reversible)
congenital
structural
Adult epilepsy are more likely caused by...
acquired vascular, degenerative, or neoplastic (cancer) causes
Triggered seizures are
seizures in those with diagnosed epilepsy that have a lower seizure threshold
Structural Causes of Epilepsy Include
Vascular: Vascular malformation, stroke
Neoplastic: primary and mets
Trauma
Infectious - meningitis, encephalitis
Autoimmune encephalitis
Degenerative - Alzheimer's
Mesial Temporal Sclerosis
Congenital: Focal Cortical Dysplasia and tuberous sclerosis
Genetic causes of epilepsy
known or presumed genetic defect
multiple gene abnormalities w/ seizure susceptibility
Ex: childhood absence epilepsy, juvenile myoclonic epilepsy
Metabolic causes of Epilepsy
glucose transporter deficiency
creatine deficiency
mitochondrial cytopathies
Immune causes of Epilepsy
CNS inflammation
Rasmussen and NMDA encephalitis
Infectious causes of epilepsy
HIV
TB
Malaria
Unknown causes of epilepsy
~30-50% of patients have an unknown cause of epilepsy
Causes of Acute Symptomatic Seizures and Epilepsy in older adults
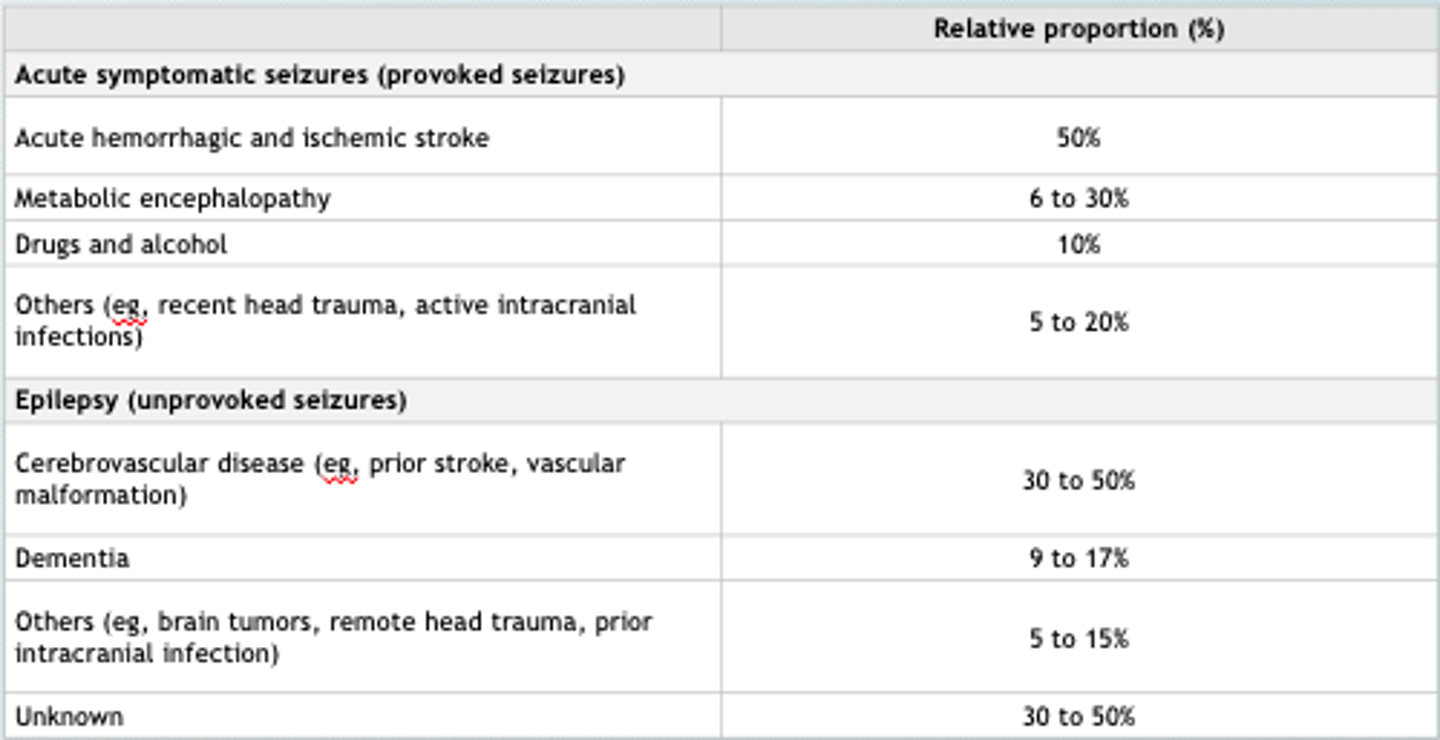
Most common cause of provoked seizures in older adults
Acute hemorrhagic and ischemic stroke
Most common cause of unprovoked seizures/ epilepsy in adults
Cerebrovascular disease (prior stroke, vascular malformation)
Test to evaulate a patient with possible encephalopathy
EEG
Scalp EEGs
can miss focal epilepsies
Buzz Words for Epileptiform waves
Spike and Sharp waves w/ lateralized epileptiform discharges
Reasons to admit someone to an epilepsy monitoring unit
1. Based on your diff diagnosis
2. Seizure classification
3. Medication Titration & Surgical Evaluation
true or false: in epilepsy monitoring unit, pts are stimulated with potential seizure triggers to attempt to provoke another seizure
TRUE!
Try to induce seizures in epilepsy monitoring unit by:
•Sleep deprivation
•Photic stimuli
•Alcohol intoxication/withdrawal
•ASM noncompliance
Natural History of Seizure Disorders
•Up to 70% of individuals with epilepsy can achieve seizure freedom
•Others will have drug resistant epilepsy that will be difficult to manage
•In children, epilepsy syndromes such as absence seizures often resolve by adolescence
•Other epilepsy syndromes typically genetic or developmental have worse outcomes and associated with frequent seizures and encephalopathy
What are the stages of a seizure?
1. Prodromal/ Trigger
2. Aura
3. Ictus
4. Post Ictus
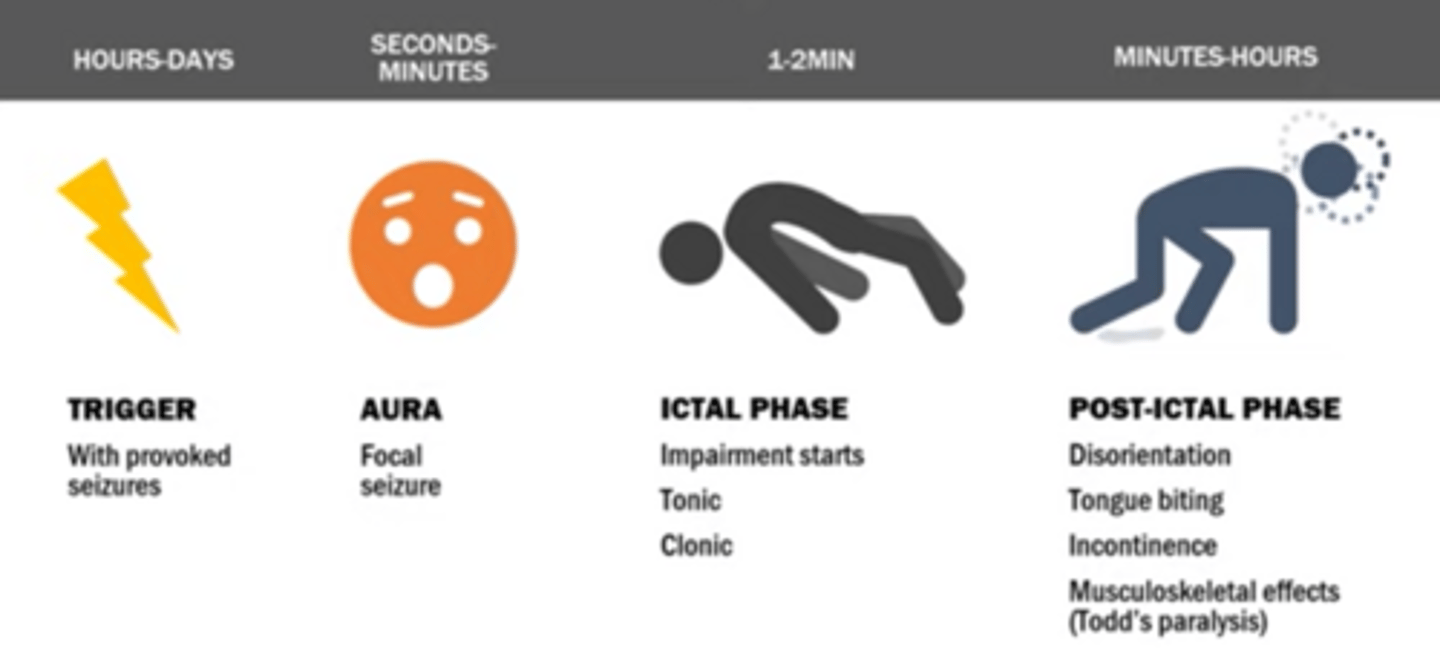
Prodromal/Trigger stage of seizure
only with provoked seizures:
•Sleep deprivation
•Photic stimuli
•Alcohol intoxication/withdrawal
•ASM noncompliance
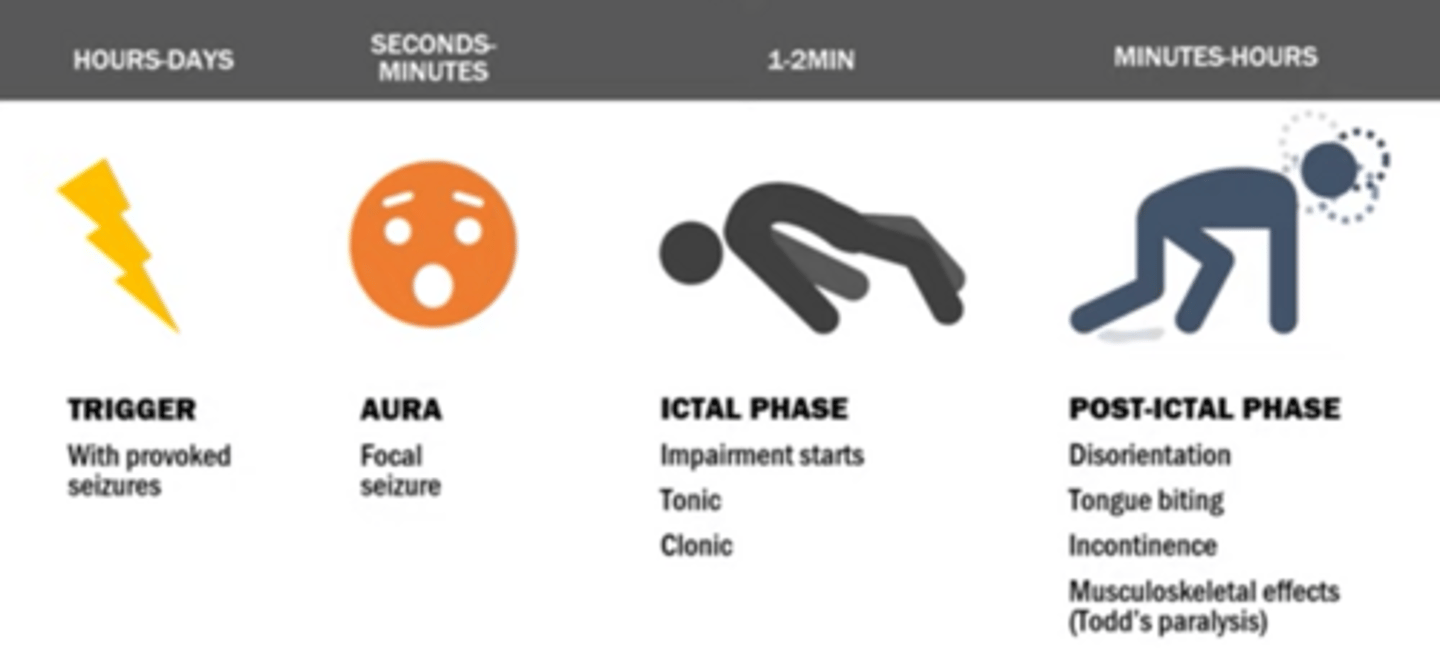
Aura of a seizure
Period of altered sensation before the onset of a seizure
- Often aware of strange smells, auditory, motor activity, or sights prior to seizure
- Aura - déjà vu and detachment from reality
- Auras are focal seizures that affect enough of the brain to cause symptoms, but not enough to interfere with consciousness (sense of doom)
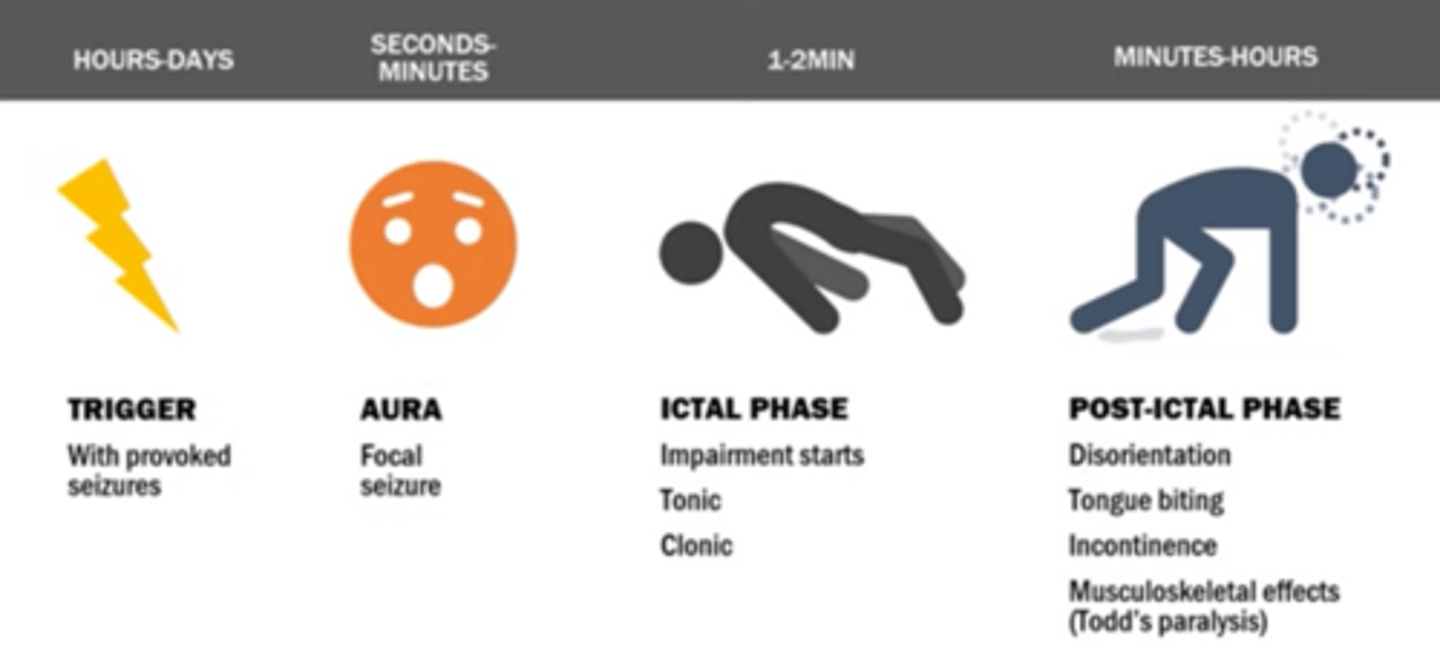
Ictal phase
full seizure - impairment, tonic, clonic
Stereotypical
Rhythmic
Brief
(Depends on brain region)
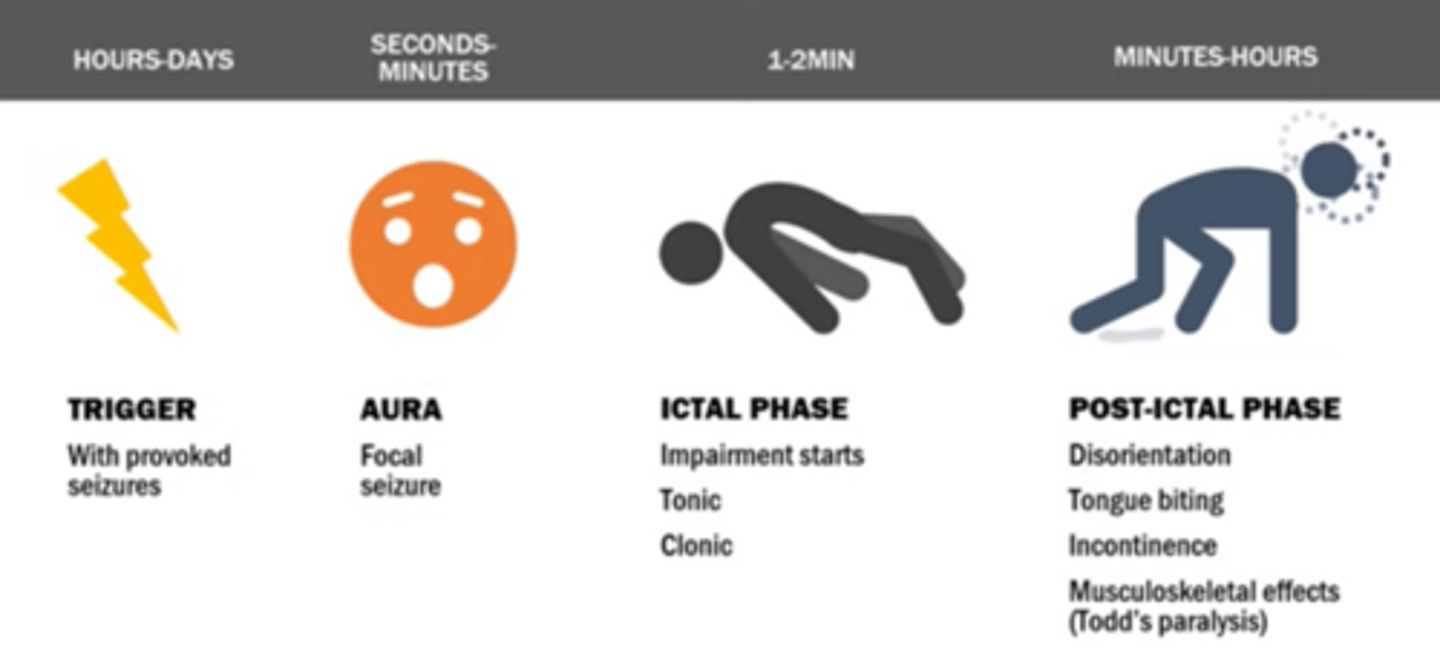
Post-ictal phase
The final phase of a generalized seizure, during which the patient becomes extremely fatigued and disoriented
fractures, incontinence, tongue biting, often characterized by somnolence, confusion, and headache
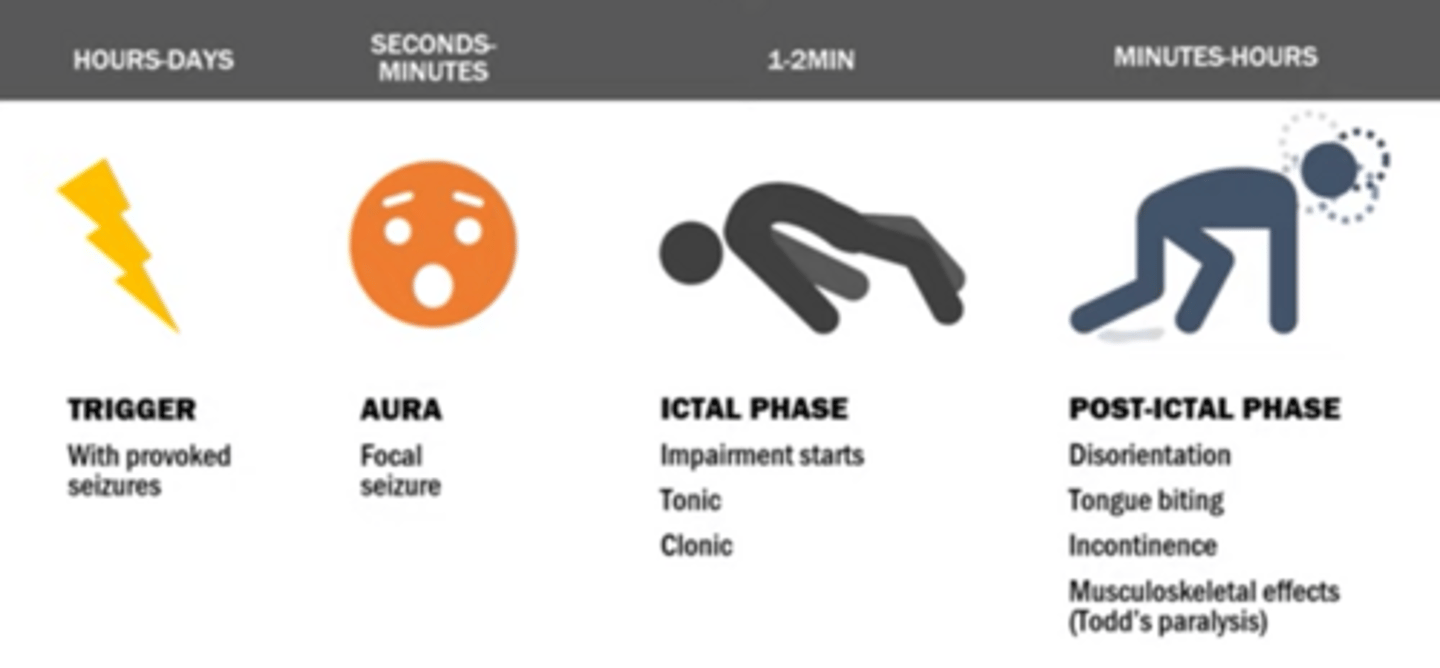
Todd's paralysis/ paresis
focal weakness in a portion of the body following a seizure, typically left or right side
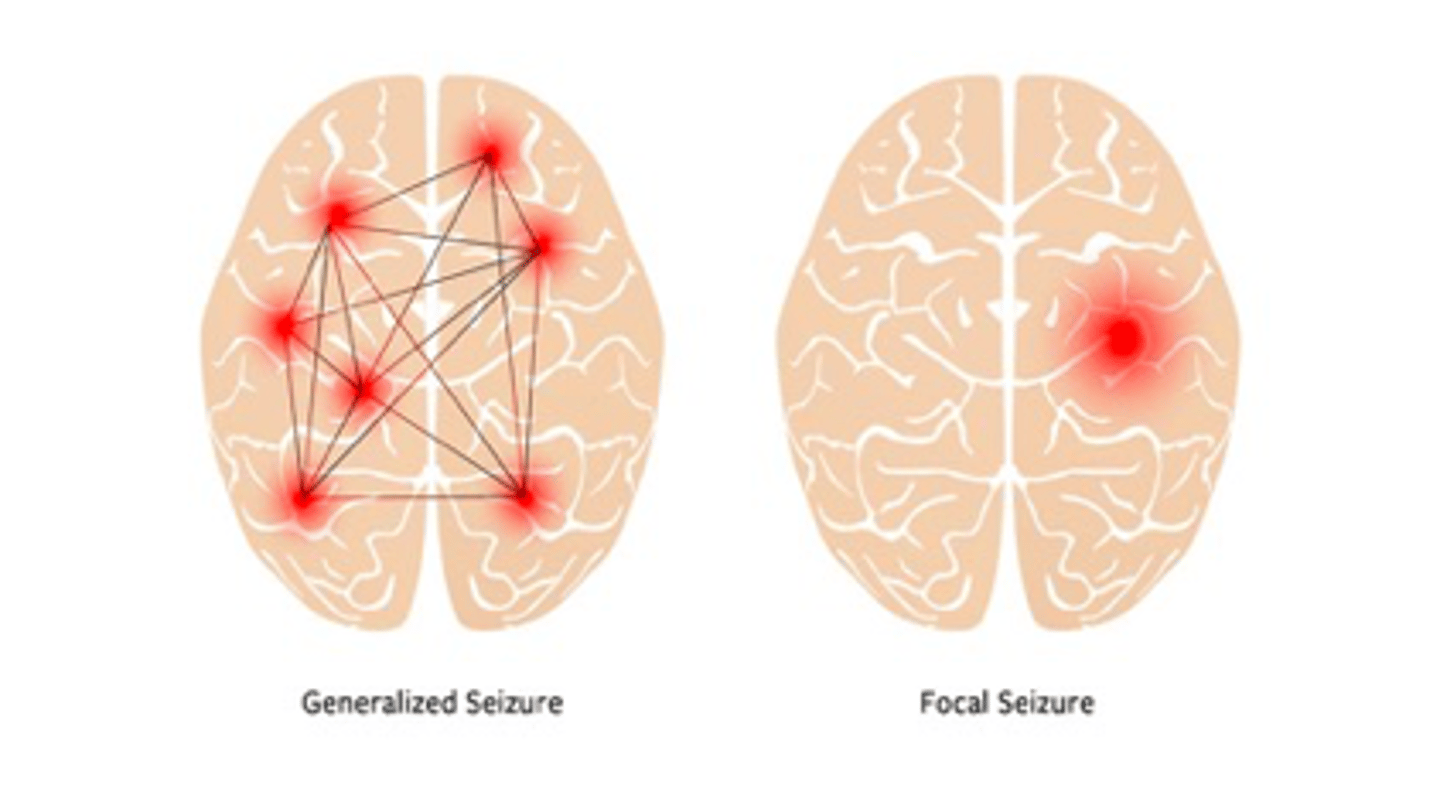
How are seizures classfied?
Focal or generalized
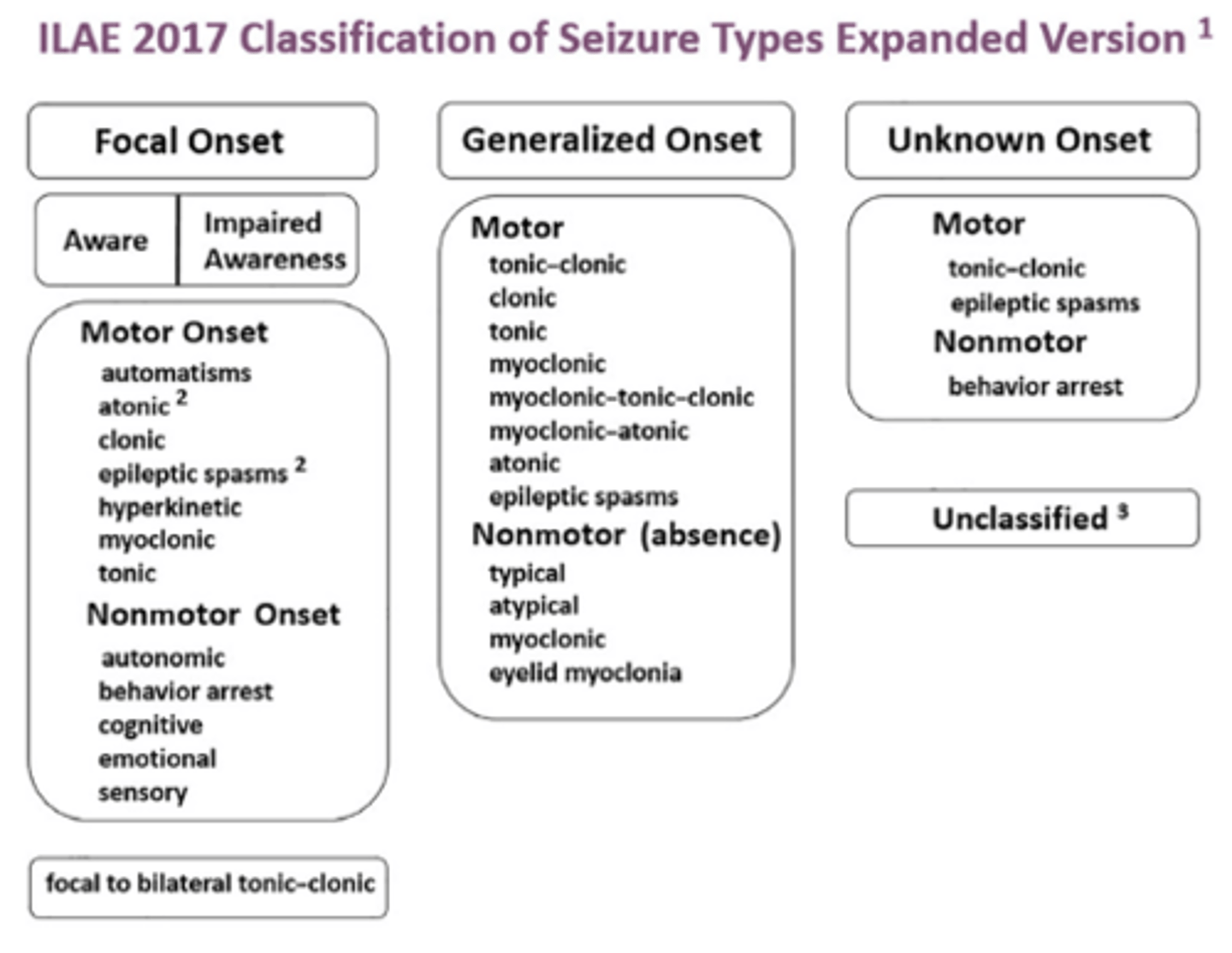
Generalized seizures involve
both hemispheres of the brain
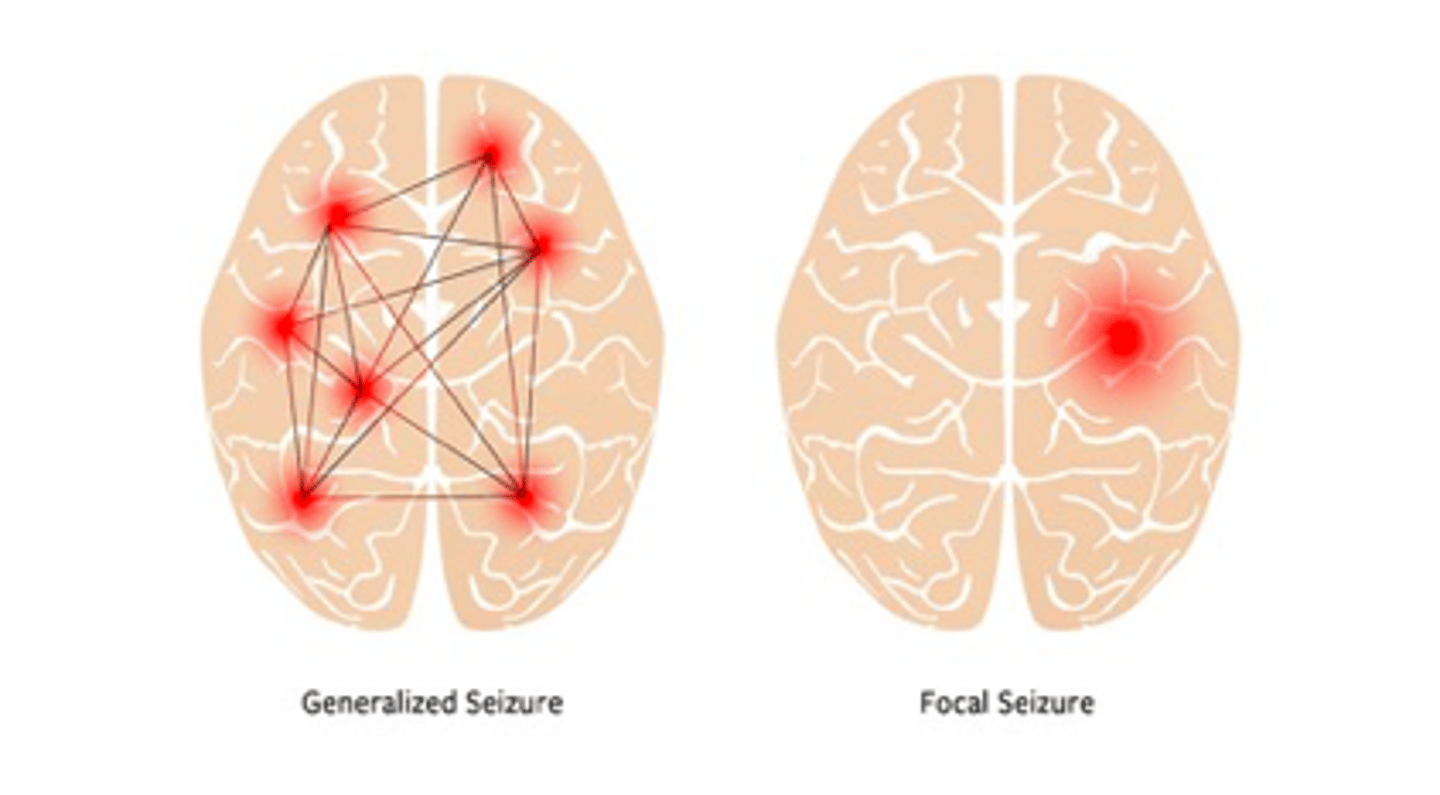
focal seizures involve
one part of the brain
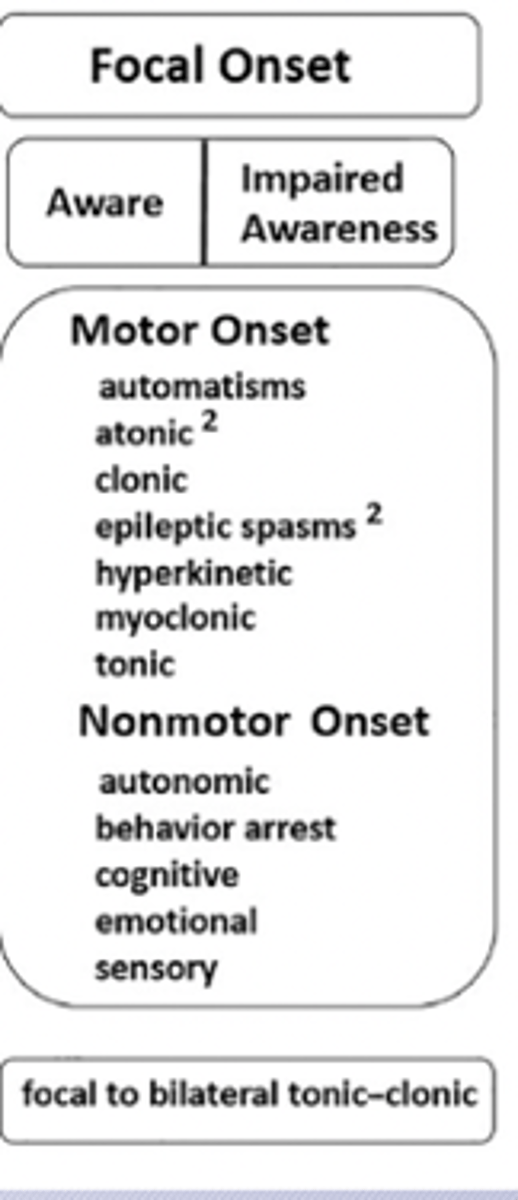
Focal Seizure with Retained Awareness
Simple partial seizure; patient is aware of and able to recall event and able to answer questions about it
characteristics of Focal with Retained Awareness Seizure (simple partial)
•Auras are focal aware sensory seizures
•Paraesthesias, tingling, gustatory, olfactory, visual and auditory sensations
•Behavioral arrest, speech arrest, déjà vu, fear/feeling of doom
•Epigastric pain, sweating, tachycardia
•Can have automatisms and unilateral motor features
List examples of sensory signs of Aura
Sensory Effects: Paresthesia, tingling, olfactory, gustatory, visual & auditory sensations
List examples of autonomic signs of Auras
Epigastric Pain
Sweating
Tachycardia
Focal Impaired Awareness Seizure (FIAS)
Focal Impaired Awareness (complex partial): impaired responsiveness with environment, confusion, unable to recall events
characteristics of Focal Impaired Awareness Seizure (FIAS)
•Appears awake but not responding normally to instructions or questions
•Automatisms: repetitive behaviors such as facial grimacing, gesturing, chewing, lip smacking, or repeating words
•Seizures typically last less than three minutes
•Can be postictal: characterized by somnolence, confusion, and headache for up to several hours
Focal Motor Seizure
The clinical manifestations of seizures vary based on?
The clinical manifestations of seizures vary based on the location of the seizure in the brain and the amount of cortex that is involved
Focal Motor Seizure - motor sx
•can have unilateral tonic, clonic, myoclonic events
•Jacksonian March
Jacksonian March Seizure
progressive neuroanatomic spread
focal seizures may propagate diffusely to cause?
Focal seizures may propagate diffusely to cause bilateral tonic-clonic seizures (previously referred to as secondarily generalized seizures)
Temporal Lobe Epilepsy
most common form of focal epilepsy
almost 2/3 of cases of intractable epilepsy managed surgically
etiology of temporal lobe epilepsy
Mesial temporal sclerosis is common etiology
Temporal Lobe Epilepsy associated with what sx
Associated with aura including anxiety, déjà vu, olfactory, gustatory/auditory, hypokinetic, staring, aphasia, amnesia
Temporal Lobe Epilepsy
Can have seizure freedom after?
can have seizure freedom after temporal lobectomy surgery
Occipital Lobe Seizures sx
flashing lights, elementary visual hallucinations
prominent blinking/eyelid fluttering
Parietal Lobe Seizures sx
may cause distortion of spatial perception; sensory and language changes
Frontal lobe Seizures sx
•may cause sudden speech difficulties and hyperkinetic movement, nocturnal
•Hypermotor and bizarre movements (proximal limbs, tonic), bicycling kicking, pelvic thrusting
•Gaze deviation and aphasia
•it may occur during sleep and lack post-ictal phase
Treatment of Focal seizures
Antiseizure medications for focal seizures:
• Lamotrigine, Levetiracetam, carbamazepine, oxcarbazepine, Valproic acid, phenytoin
Epilepsy surgery: temporal lobectomy etc
Generalized Seizures involve? determine onset with?
Involve seizure onset in both hemispheres
May need an EEG to determine onset in some cases
generalized seizures: in kids? generally?
Can have automatisms
Absence seizures in children
What is the most common generalized seizure type
tonic clonic (grand mal)
Treatment of generalized seizures
Lamotrigine, Levetiracetam, Valproic acid, topiramate, zonisamaide
Types of Motor Seizures
Tonic
Clonic
Atonic
Myoclonic
Tonic Seizure physical signs
rigidity and sudden stiffness of trunk and limbs
Muscle extension
Fall backwards
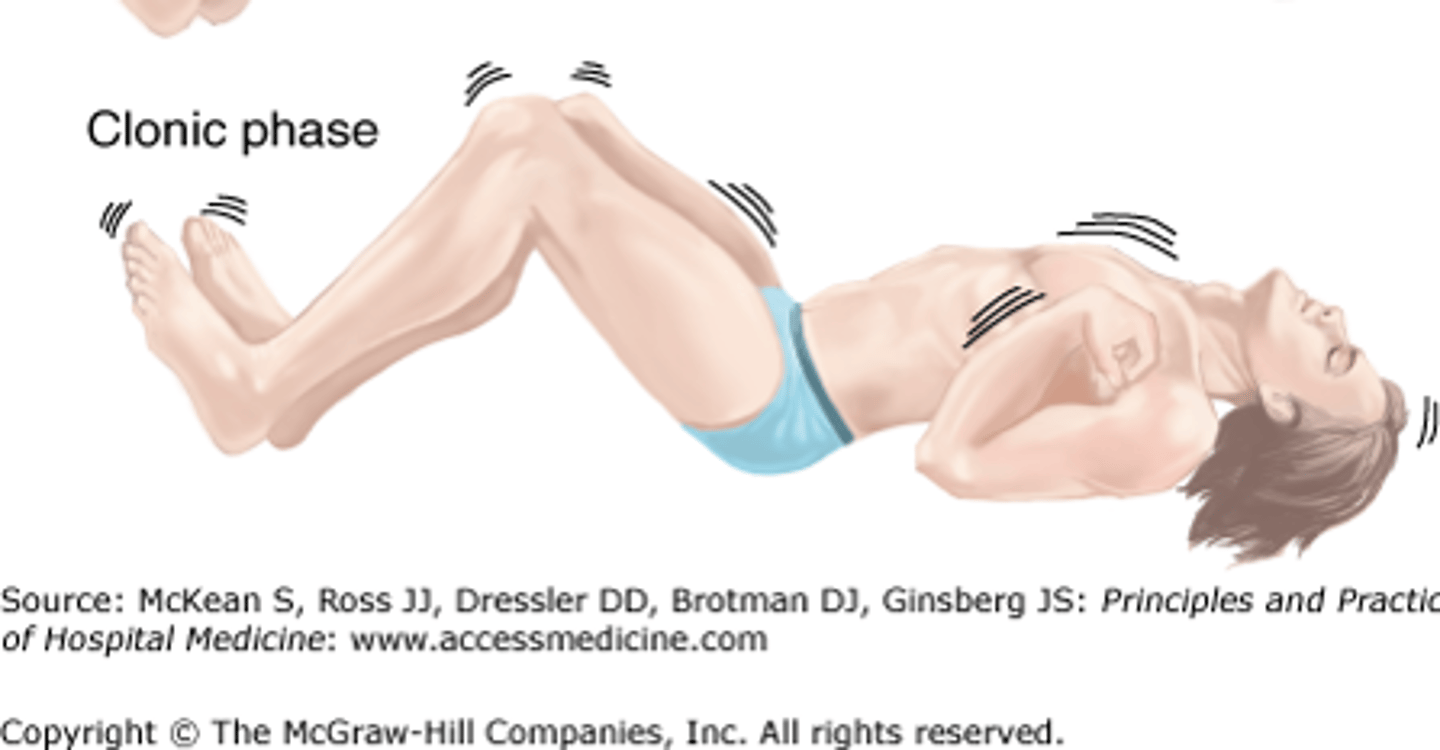
Clonic Seizures physical signs
jerking
sustained muscle contraction w/ alternation of relaxation
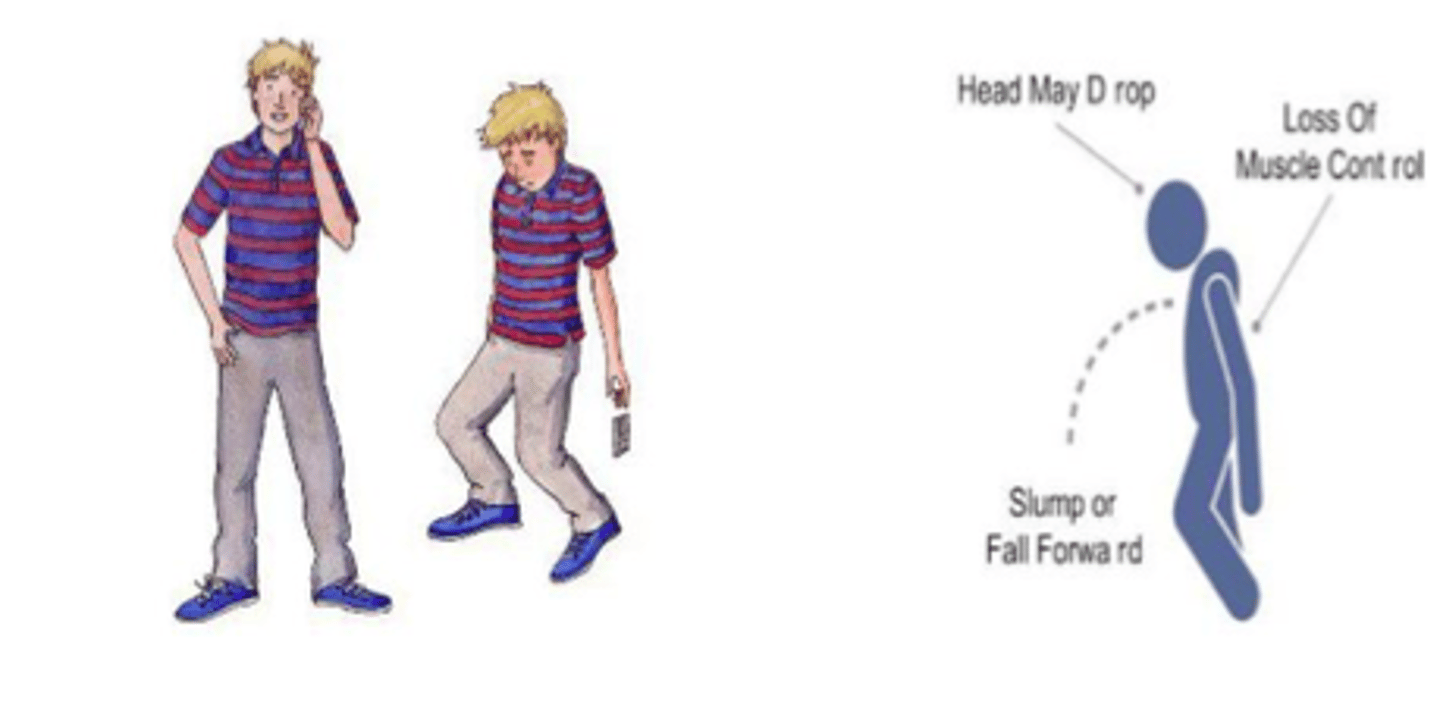
Atonic seizure signs
drop attacks
loss of tone
fall forward
Myoclonic seizure signs
Brief muscle contractions can occur singly or in clusters
Arms are affected
Consciousness is NOT impaired
What are absence seizures
Petit mal seizures. Brief lapse of consciousness.
When are absence seizures most commonly seen (AGE)
seen in childhood 4-10, usually stop by 20
BUZZ WORDS associated with Absense Seizures (signs & symptoms)
Staring, rhythmic eye blinking, automatisms
•Person not always aware of interruption in consciousness
•Break off in mid sentence
KIDS!
EEG signs of absence seizure
bursts of 3 Hz synchronous & symmetrical spike-waves
Treatment of Absence Seizures (Petit Mal)
Ethosuximide (Zarotonin)
Valproic acid (Depakene)
Generalized Tonic Clonic Seizures (Grand Mal)
epidemiology
•Mostly seen in ages 10-25 (associated with genetic generalized epilepsy)
•New onset of generalized epilepsy is uncommon in adults: often is a focal to bilateral tonic clonic seizure that generalizes
•Frequency ranging from daily to once every few months or years
•The prognosis for remission can vary, with some individuals experiencing only a single seizure, while others may go into status needing multiple ASMs
•Three risk factors for seizure recurrence: are the number of seizures, underlying neurological disorder, and an abnormal electroencephalogram
Phases of grand mal seizure (in order)
1. Tonic phase (20 sec -1 minute)
2. Clonic phase (30 to 90 seconds)
3. Post-ictal
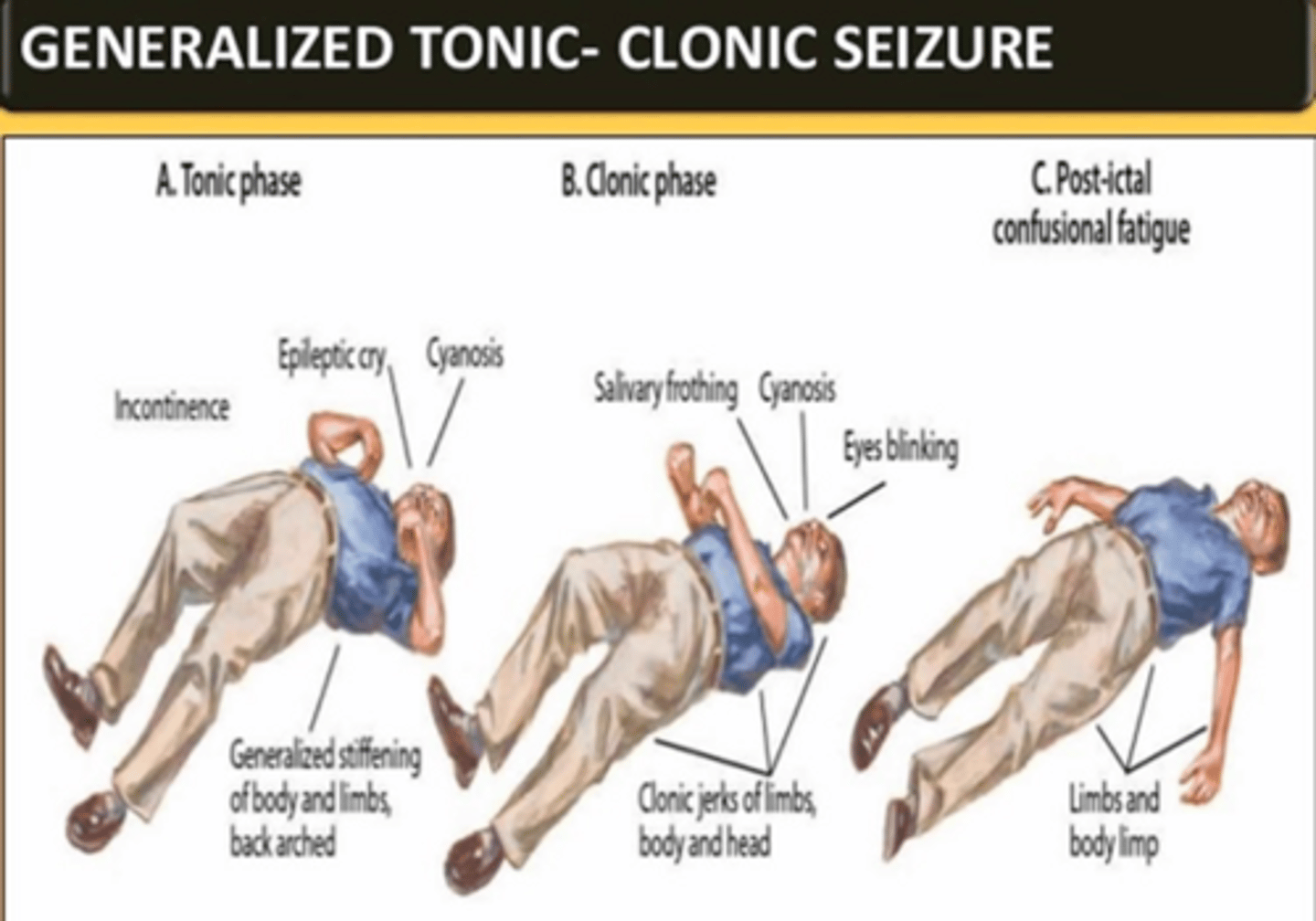
What occurs during the tonic phase of grand mal seizure
muscle rigidity and stiffness
•Sudden LOC followed by respiratory arrest
•Involuntary crying out from contraction of respiratory muscles
•Extension of muscles
•Associated cyanosis
What occurs during the clonic phase of grand mal seizure
Brief, violent, generalized flexor contractions alternating with progressively longer muscle relaxation
•Possible cheek or tongue biting
•Foamy salivation
•Possible loss of bowel or bladder control
What occurs during post-ictal phase of grand mal seizure
can be in deep sleep, confusion & somnolence, muscle soreness
Treatment of Grand Mal (Tonic/ Clonic) Seizure
Lamotrigine (Lamictal)
Levetiracetam (Keppra)
Topiramate (Topamax)
Valproate (Depakene)
Atypical Absence
•More changes in tone that regular absence
•More gradual start and prolonged episodes
•May be associated with developmental delay
•Slower spike-wave patterns
•About 12 to 13 percent of children develop generalized tonic clonic, however should be reevaluated if patient has absence seizures
Status Epilepticus
Convulsive Status is? timeline?
Convulsive Status is a medical emergency!
≥5 minutes of continuous seizures, or
≥2 discrete seizures between which there is incomplete recovery of consciousness
Long-term consequences of Status Epilepticus
Long-term consequences (after 30 mins): neuronal death, neuronal injury, and alteration of neuronal networks
Etiology of Status Epilepticus
•Most cases of status epilepticus in adults are due to an acute underlying structural brain lesion or a toxic or metabolic disturbance
•Patient with known epilepsy or low ASM levels
Clinical Manifestation of Status Epilepticus? If no return to baseline?
tonic and/or clonic motor activity and loss of consciousness
•If no return to baseline, obtain EEG
•it may show continuous spike and wave activity indicative of generalized seizure activity.
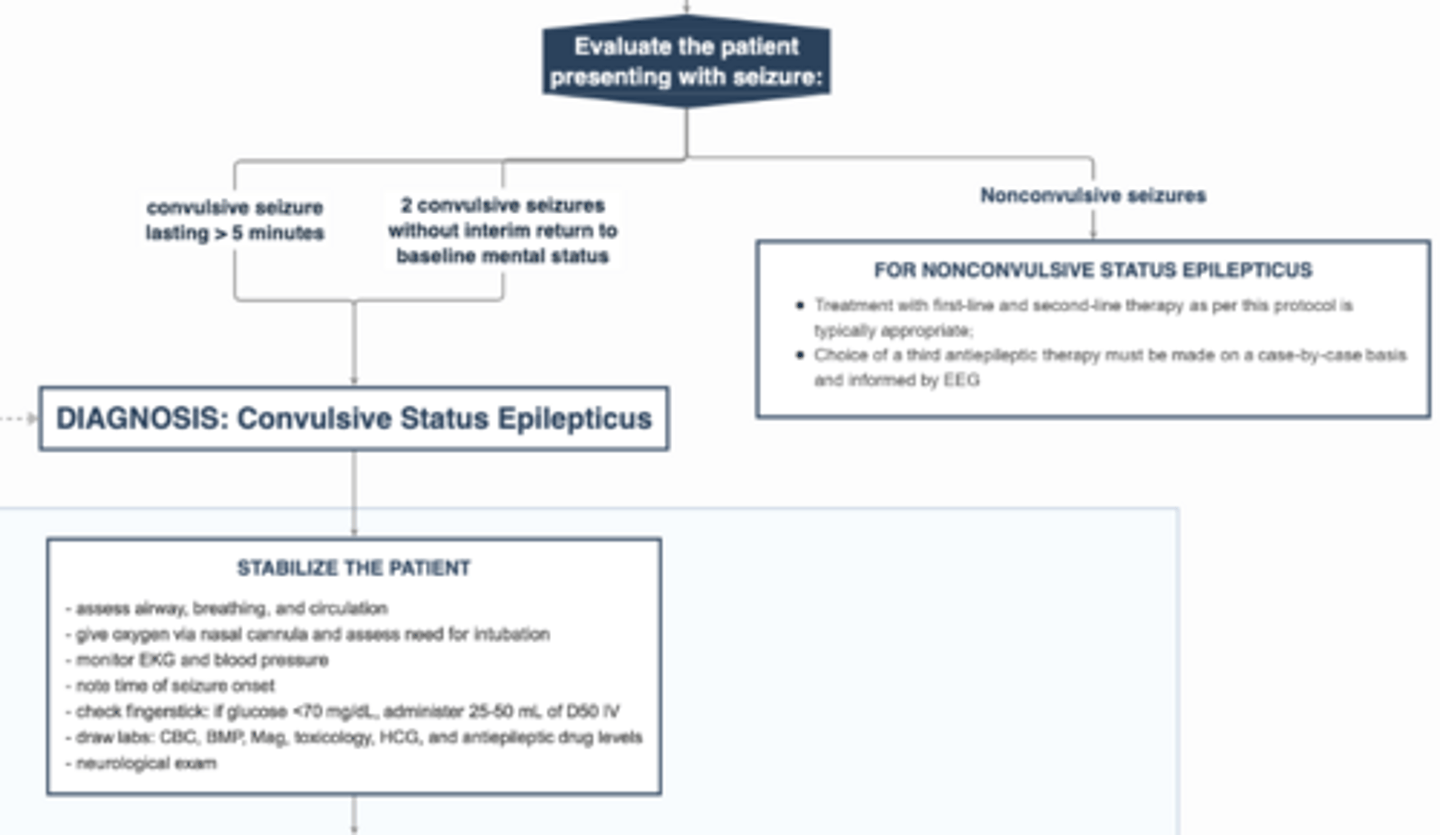
Nonconvulsive status epilepticus (NCSE
• challenging diagnosis. It typically manifests as an altered mental status with confusion, psychosis, lethargy, or coma
•a condition of ongoing or intermittent seizure activity without convulsions, without recovery of consciousness between attacks, and lasting more than 10 minutes. Diagnosis is made in EEG
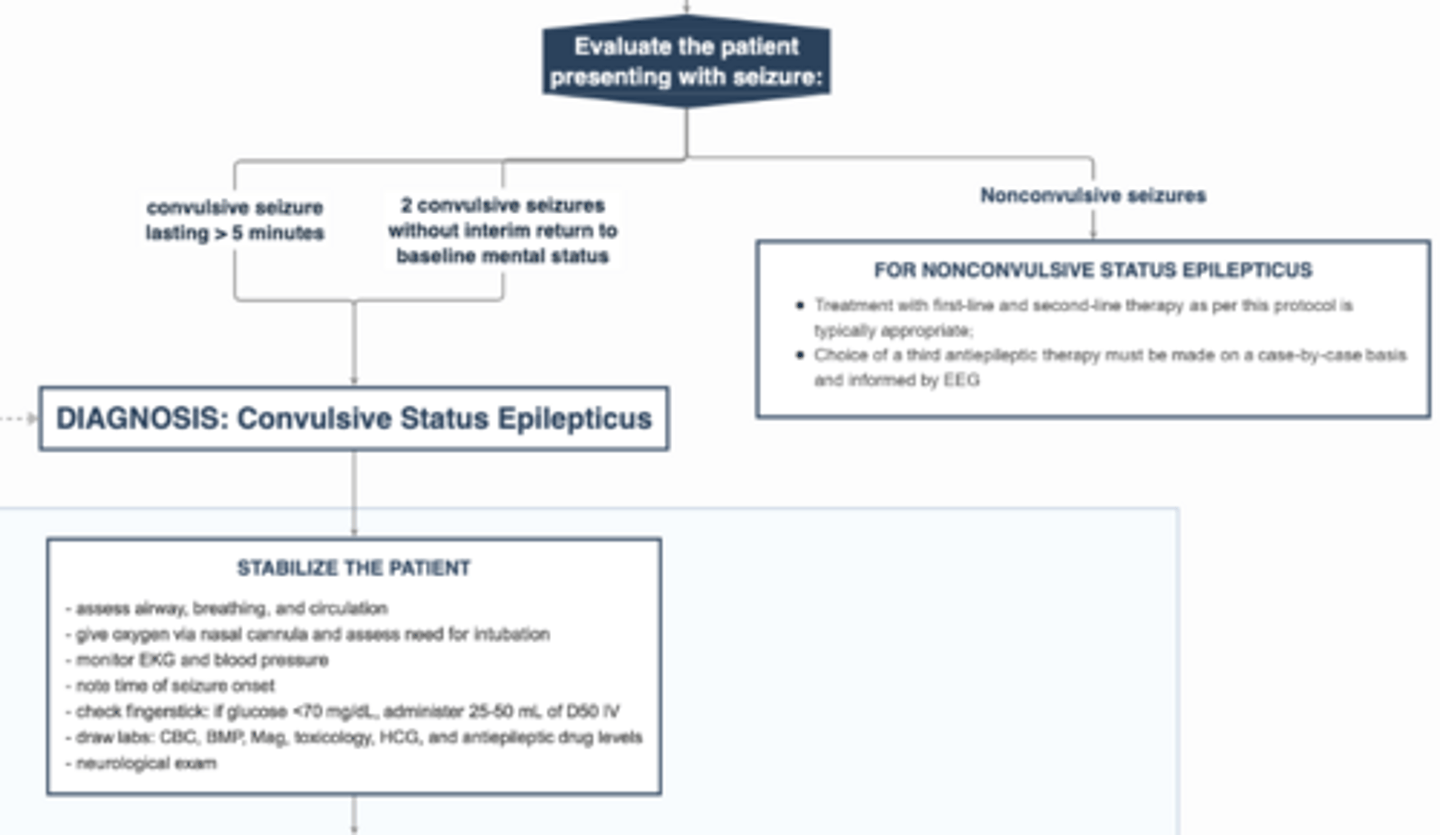
Management of status epilepticus
IV access = lorazepam (ativan)
no IV access = midazolam
ensure patent airway
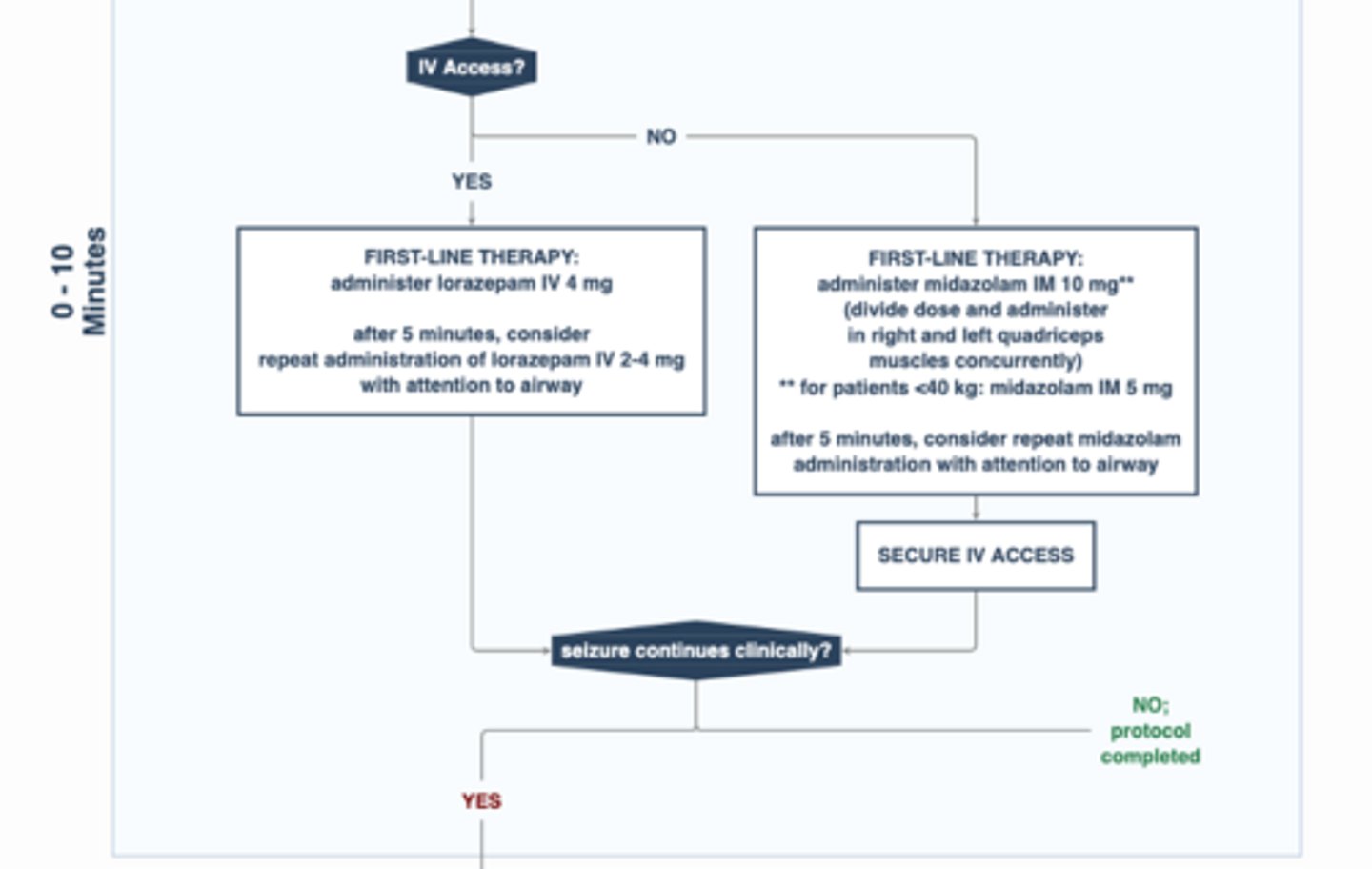
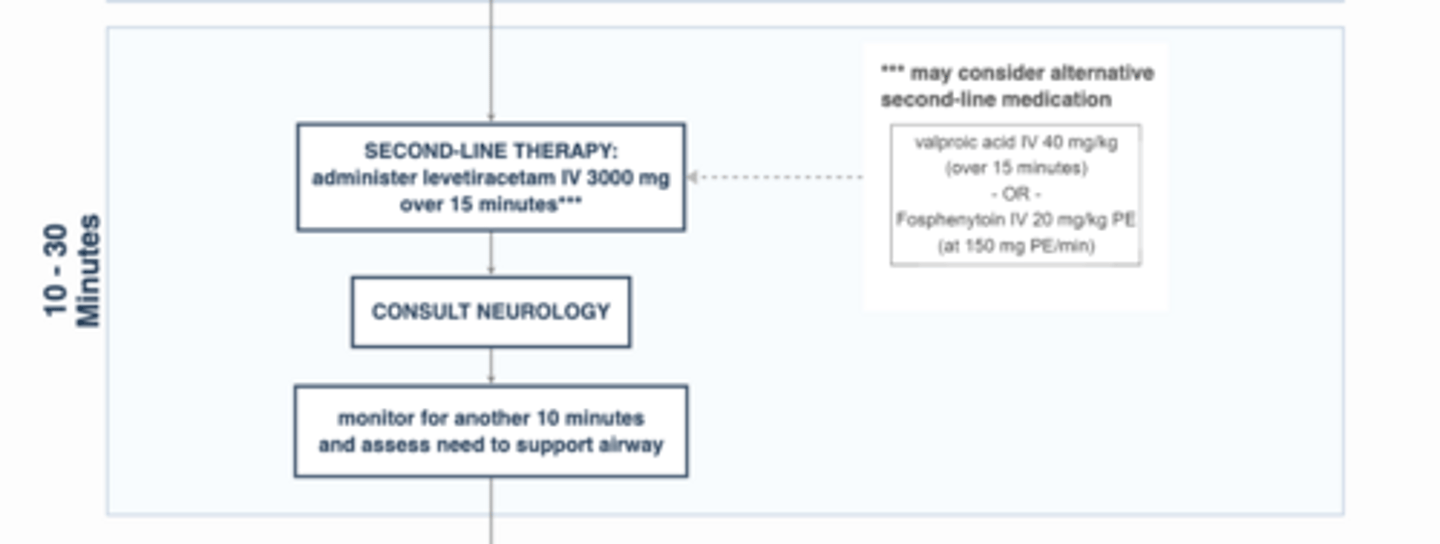
second line management of status epilepticus
Second line: Load ASM
1. Levetiracetam (Keppra)
2. Depakote/Depacon (valproic acid)
3. Fosphenytoin
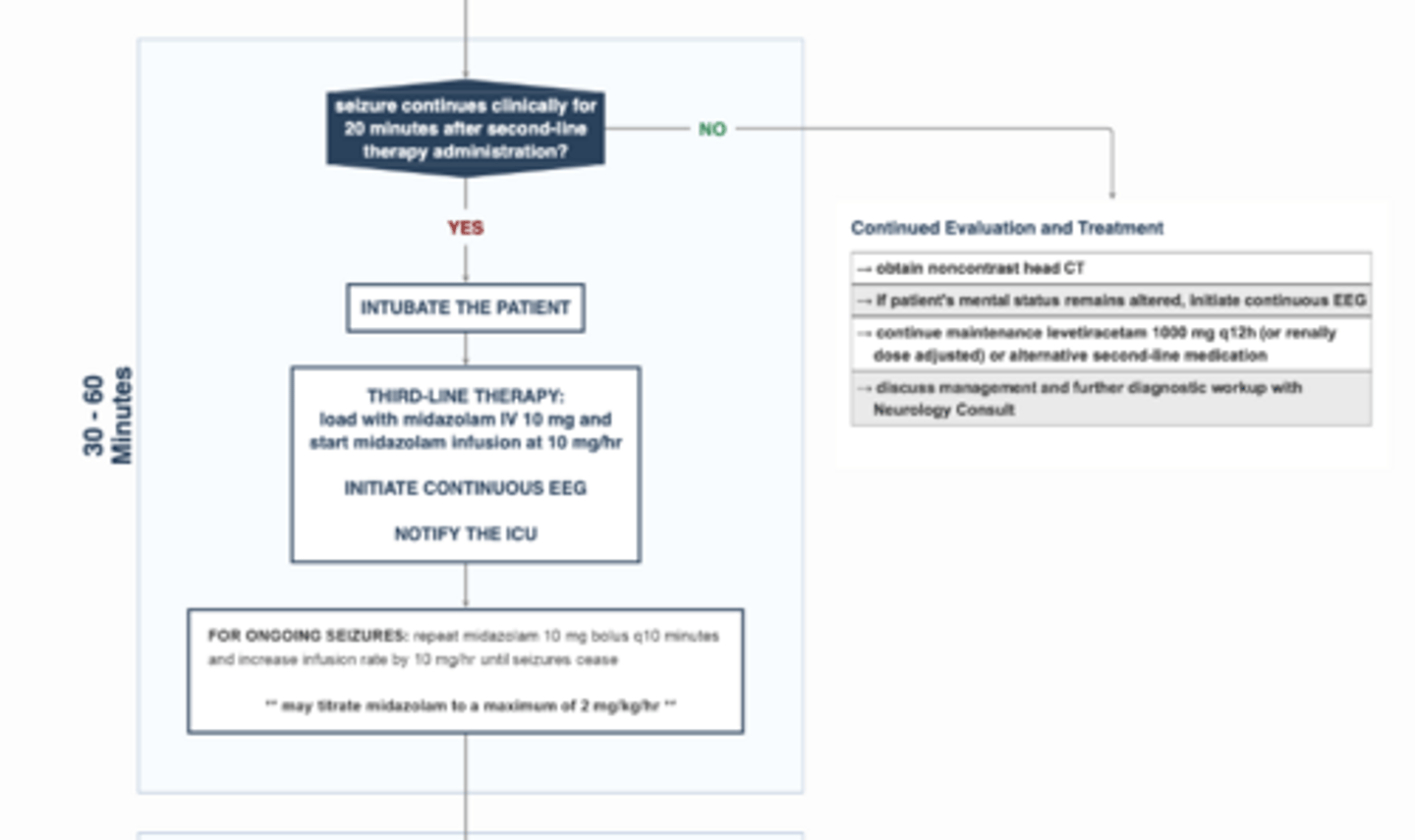
more seizure management
intubation
midazolam
continuous EEG
notify ICU
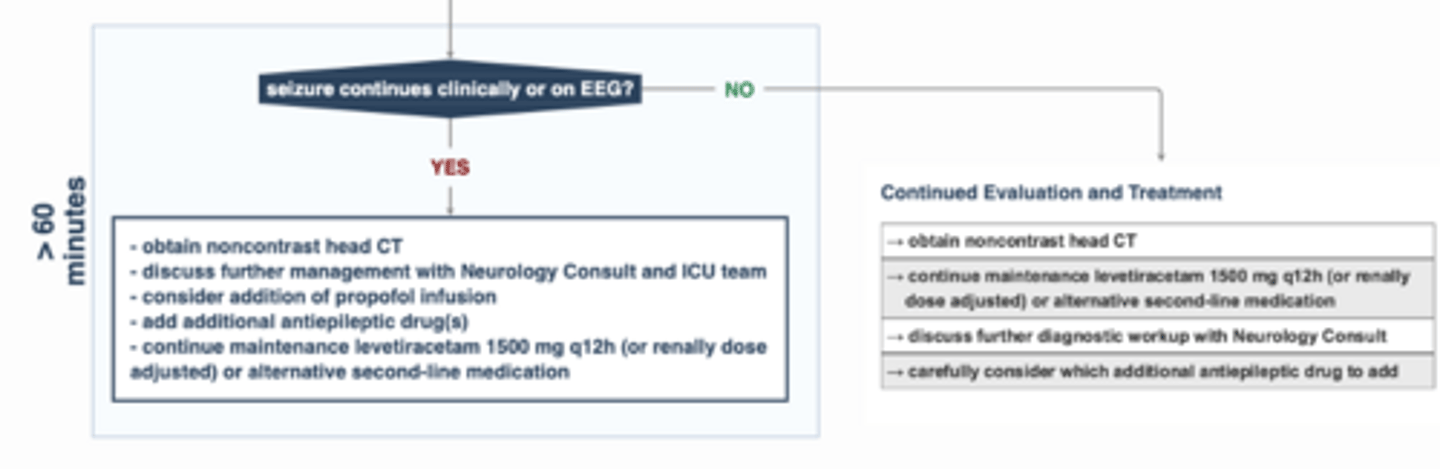
>60 minutes of seizure
Non contrast head CT
Add propofol or pentobarb with EEG
History for seizure activity (general)
Prodrome or Aura?
Seizure activity
•Convulsions, tongue biting, awareness
•Was there a Witnesses or video recording
•Timing: age of onset, awake vs sleep
•Duration: should not be longer than 5 minutes
Postictal: state of confusion, can last mins to hours. Aphasia, hemianopsia, or numbness. Todd paralysis or postictal paresis.

Postictal - Todd paralysis or postictal paresis
postictal paresis is weakness of a hand, arm, or leg that appears following a focal motor seizure involving the one side of the body
history - triggers?
•strong emotions, intense exercise, loud music, and flashing lights, fever, the menstrual period, lack of sleep, pregnancy, and stress.
•Can have no triggers as well
Epilepsy Risk Factors (SH/PMH/FHx)
•CNS structural changes: neoplasm or malformation, Birth complications, premature, Family history, febrile seizures, autism, developmental delays
•SH: Drug and alcohol use
•PMH: Neurologic hx, immunosuppression, cancer, past epileptic events
•FHx: A positive family history of seizures is a risk factor for epilepsy. In particular, absence seizures and myoclonic seizures may be inherited
Physical Exam for seizures
•Look for signs of injury: tongue bite or injury
•Post ictal confusion
•Todd's Ictal paralyses
•Hyperreflexia
•Can have a normal exam
Differential Dx for transient neurologic event
•TIA: Rapid loss of neurologic function due to interrupted blood flow; typically "negative” symptoms (eg, weakness, numbness, aphasia, visual loss)
•Panic Attack: Palpitations, dyspnea, chest pain, lightheadedness, sense of impending doom;
•Migraine Aura: Positive and/or negative neurologic symptoms, most often visual and sensory, evolving > 5 min
•Psychogenic nonepileptic seizure: seizure like activity w/o EEG correlate, eyes closed, no post ictal
•Generalized: cardiac problem causing lack of blood to brain?
•Syncope: Transient loss of consciousness, loss of postural tone; has prodrome of lightheadedness, temperature, sweating, palpitations, pallor; myoclonic jerks or tonic posturing may occur, no post ictal confusion
•Narcolepsy