Effusion & fluid analysis
1/36
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
What are the features of the body cavity fluid?
Little fluid (<5 ml) is present in these cavities in small animals
Ultrafiltrate of blood
Low cellularity and protein concentration
Lined by mesothelial cells
What does the rate of fluid formation depend on?
Starling’s forces = gradients of hydrostatic and oncotic pressures between the vessels and the body cavities
The degree of mesothelial and endothelial permeability
The integrity of lymphatic drainage
How do you carry out body cavity fluid analysis?
Gross —> colour & turbidity
Total nucleated cell count (TNCC) —> EDTA tube → haematology analyser
WBC, RBC and haematocrit
Total protein concentration
Refractometer
Cytological examination
Direct/ sediment smear
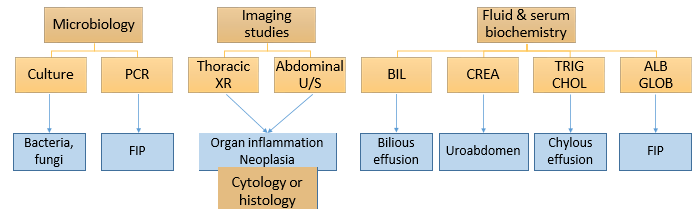
What other tests would you want to carry out other than just cytology?
Biochem - cholesterol, creatinine ect.
Microbiology - culture and PCR
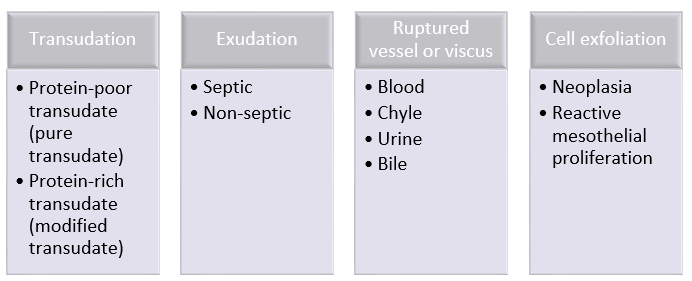
What are the different classifications of body cavity effusions?
What cells are being shown in the normal body cavity fluid cytology?

Mesothelial cells
Macrophages
Lymphocytes
Neutrophils
(very few cells in the normal body cavity)
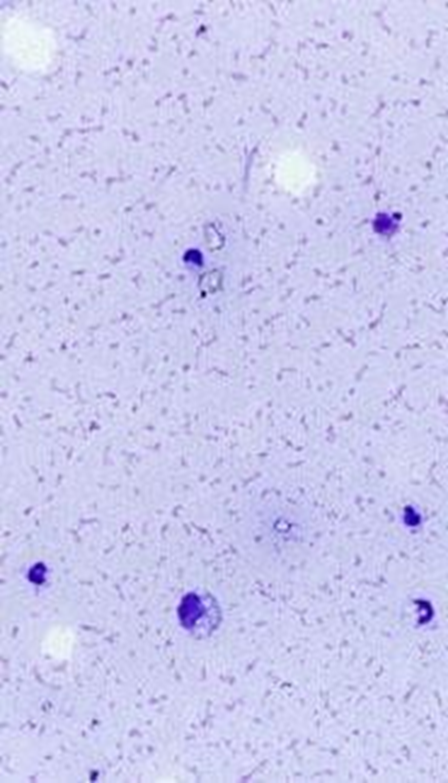
What are the features of Protein-poor (pure) transudate?
Clear & colourless
TNCC <1.0 x10^9/L
TP < 25 g/L
Macrophages & lymphocytes typically predominate; fewer neutrophils; rare mesothelial cells
^^ cytospin prep
What causes protein-poor transudate?
Inc hydrostatic pressure
Cardiac failure
Portal hypertension
Overhydration (excessive fluids)
Venous thrombus
Dec osmotic pressure
Severe hypoalbuminaemia (protein losing nephropathy, protein losing enteropathy, hepatic insuf)
Organ rupture
Uroabdomen, bilious effusion (will become exudate)
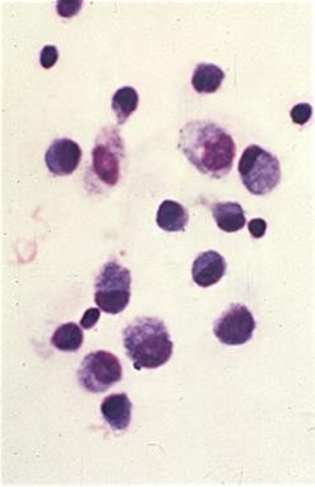
What are the features of Protein-rich (modified) transudate?
Clear & colourless to amber or pink
TNCC 1.0-5.0 x10^9/L
TP >25 g/L
Macrophages, lymphocytes, neutrophils; variable numbers of mesothelial cells (dep on irritation —> binucleated, on L of image)
^^^ cytospin prep
What causes Protein-rich transudate?
Increased systemic or local hydrostatic pressure
Congestive heart failure
Portal hypertension
Venous thrombus
Neoplasia
Organ torsion or volvulus
Other
FIP (see later)
Chronic protein-poor transudate
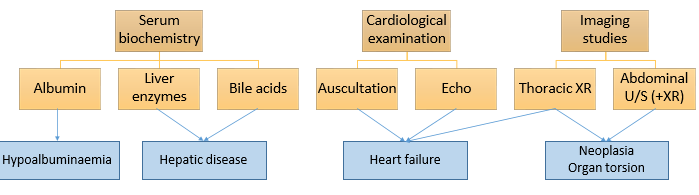
Further investigation of transudate
What are the features of an exudate?
Turbid, amber, yellow or brown
TNCC >5.0 x10^9/L
TP >25-30 g/L
Mostly neutrophils, fewer lymphocytes & macrophages; variable numbers of mesothelial cells
^^^ direct smear
What causes an exudate?
Septic
Bacteria —> haematogenous / lympho spread, FB, penetrating wounds, from other tracts
Fungi —> systemic mycosis
Protozoa —> toxoplasmosis, neosporosis, leishmaniosis
Parasites —> cestodes
Non-septic
Organ inflam (e.g. pancreatitis, steatitis, inflammatory/necrotic neoplasm)
Irritants (e.g. urine, bile)
FIP
Eosinophilic (very rare)
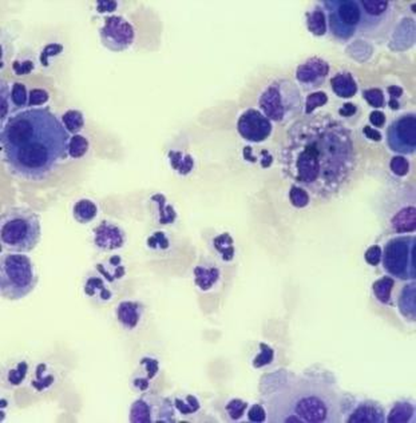
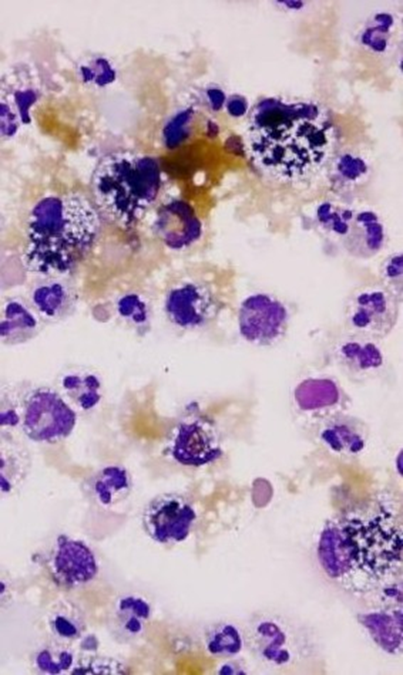
What is being shown here?
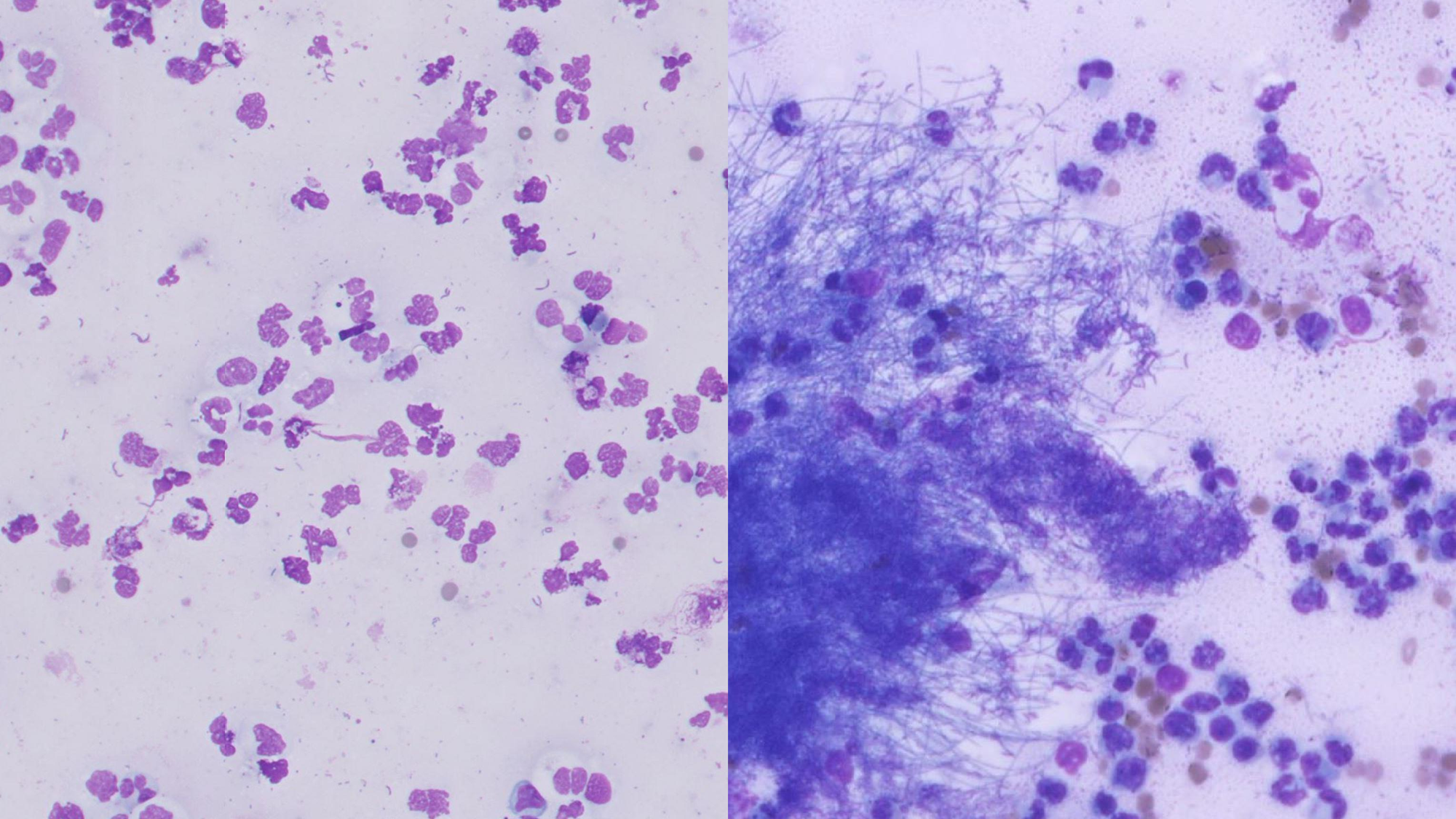
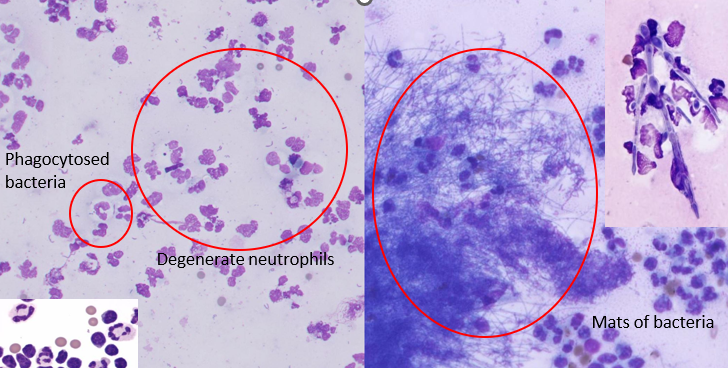
Degenerate neutrophils when encounter bacteria
Fungal hyphae on R
What further investigations are needed if exudate is suspected?
What are the features of FIP fluid?
Yellow & hazy / cloudy
Usually < 5.0 x109/L, but can be higher
High, often >45 g/L (very high yet poorly cellular)
Usually neutrophils predominate; variable numbers of macrophages; few lymphocytes, but can rarely predominate
How do you diagnose FIP?
Rivalta test
distilled water + vinegar → precipitation line if +ve
lower specificity
Fluid albumin : globulin
>0.8 = FIP excluded; <0.4 = FIP likely
Serum a1-acid glycoprotein >1,5g/L
Direct IFA for FCoV within effusion macros / RT PCR for FCoV in fluid
Supportive of FIP
(don't have a test that is diagnostic —> indicated infected with FCoV but may not develop into FIP)
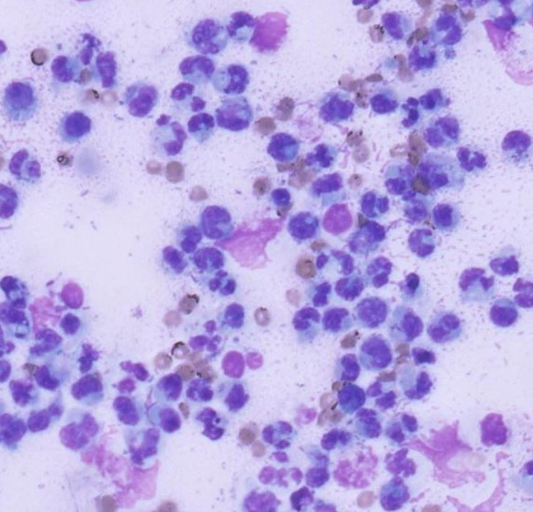
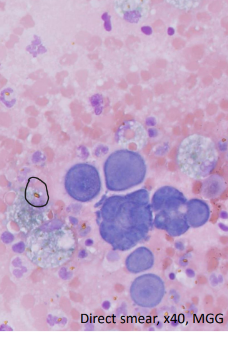
What are the features of the fluid of a haemorrhagic effusion?
Serosanguinous to red
RBC / HCT similar or slightly less than peripheral blood
TP similar / slightly less than peripheral blood
Blood (± platelets); macrophages + erythrophagia and/or HGB breakdown products (circled) ; variable numbers of mesothelial cells
What can cause haemorrhagic effusion?
Trauma
Neoplasm —> imaging/ neoplastic cells on cytology
Organ torsion
Coagulopathy —> coagulation profile
Idiopathic / Iatrogenic
How can haemorrhagic effusion be investigated?
CBC / coagulation profile
Imaging studies
Search for neoplastic cells on cytology
How do you differentiate between true and iatrogenic haemorrhage?
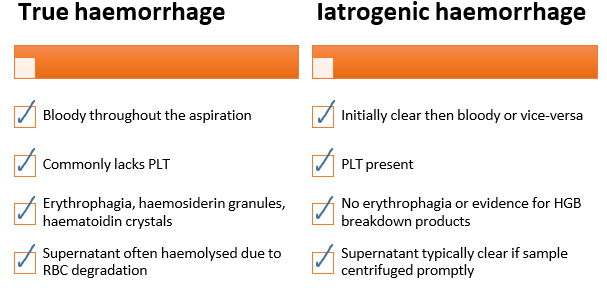
PLT = platelets
Erythrophagic = destruction of RBCs by macros
How would you describe a chylous effusion?
Milky
TNCC and TP variable
TP high
Lymphocytes predominate; with time, the numbers of neutrophils and macrophages increase; occasional mesothelial cells, but numbers increase with time
What further tests can you do for a chylous effusion?
Fluid TRIG > Serum TRIG (usually much higher)
Distinguished from pseudochylous effusion
What are the causes of chylothorax?
CV dx
Mediastinal mass (e.g. lymphoma, thymoma, granuloma)
Diaphragmatic hernia
Lung torsion
Chronic coughing
V+
Iatrogenic / idiopathic
What are the features of the fluid in bile effusions?
Brown, orange, yellow or green
TNCC & TP —> Starts as transudate & quickly becomes exudate
Neutrophils predominate; variable numbers of macrophages & mesothelial cells; yellow to green to blue-black granular material (bile) or amorphous, smooth, blue material (mucus)
How do you confirm the presence of bile inside the body cavity?
Fluid bilirubin > serum bilirubin
Caused by rupture of gallbladder or common bile duct
What are the features of the fluid in uroabdomen?
Yellow, clear to turbid
TNCC & TP starts as transudate & quickly becomes exudate
Neutrophils predominate; variable numbers of macrophages & mesothelial cells; urinary crystals may be seen
How do you confirm uroabdomen?
Fluid creatinine > serum creatinine
Caused by rupture of urinary tract (usually bladder)
How do neoplasms cause effusions?
Compression of blood vessels & lymphatics
Inflam
Haemorrhage
Necrosis
Cell exfoliation
Inc vasc permeability
(can be associated with diff types of effusion)
What is being shown here?
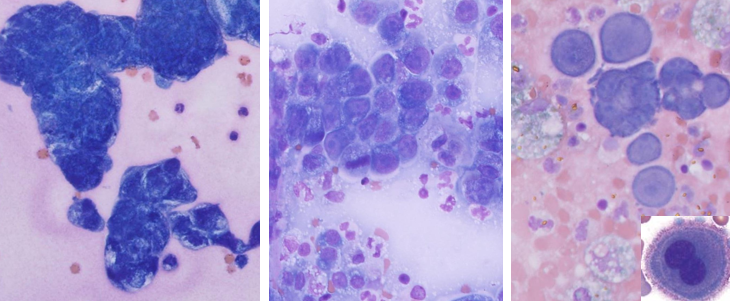
Neoplasia in cytology
Top right = reactive mesothelial cells, not neoplasia
What are the features of synovial fluid?
Lubricates joint surfaces
Provides O2 & nutrients to chondrocytes in articular cartilage
Removal of chondrocyte waste
What is synovial fluid usually like?
<0.5 mL with gel-like consistency
What is the normal synovial fluid count in dogs vs cats?
Dogs = <3000/uL
Cats = <1000/uL
How do you analyse synovial fluid in cytology?
What is normal?
Put in EDTA tube & plain tube (for culture)
Prepare direct fresh smears
Proteinaceous background
Should be less than 2 cells per HPF
Predominance of mononuclear cells (small lymphocytes, macrophages and synoviocytes)
What are the different types of joint disease?
Suppurative joint cells —> neutrophils more than 10% = neutrophilic inflam
Infectious or immune, neoplasia, drug induced
Non-suppurative —> increased (typically mildly) numbers of mononuclear cells (lymphocytes, macrophages, synoviocytes)
What can cause non-suppurative joint disease?
Secondarily to orthopaedic disease (e.g. cranial cruciate ligament rupture, hip dysplasia, elbow dysplasia, patella dislocation)
Trauma
Genetic
Obesity
Diet
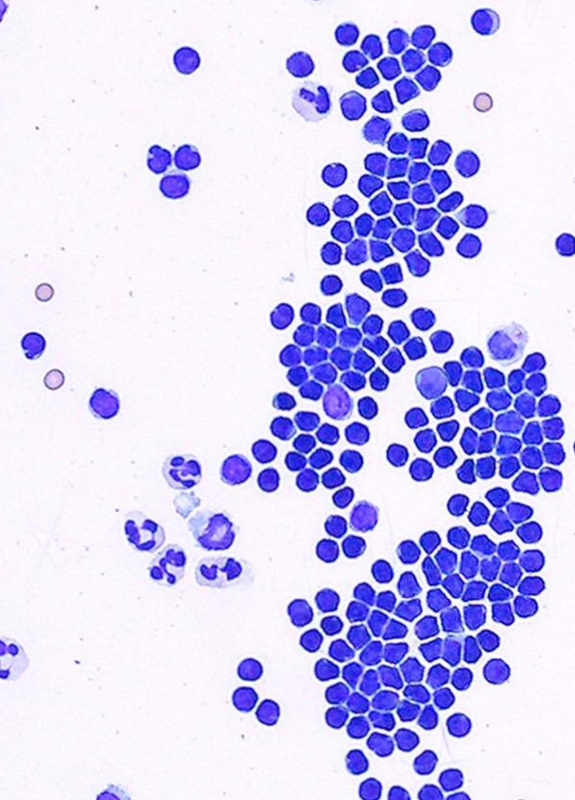
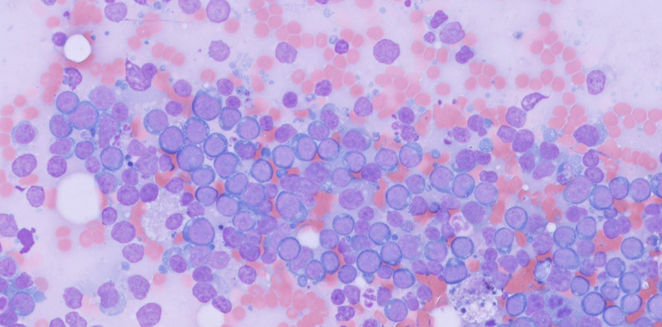
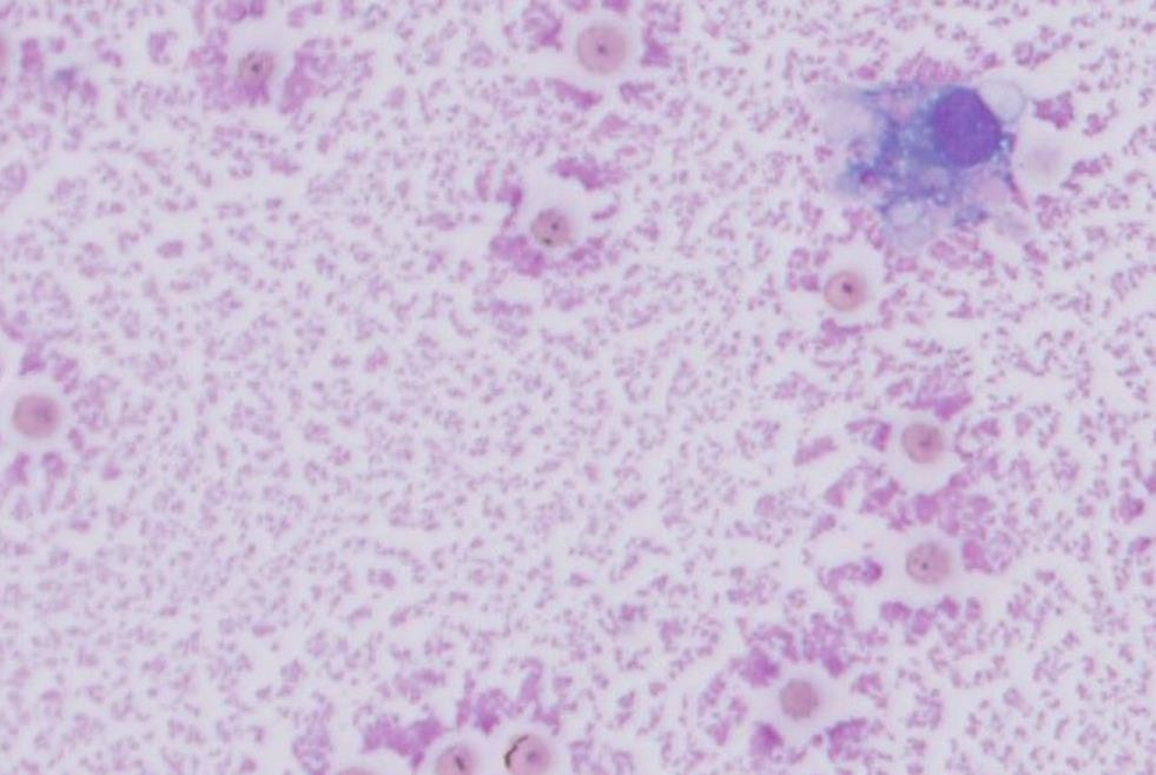
What is being shown in each of these images?
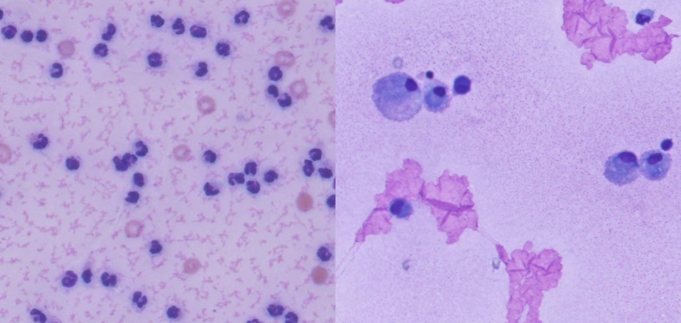
Left - suppurative joint disease = high cellularity (neutros)
Right - non-suppurative joint disease = macros & small lymphos