Chapter 9, Airway Management, Ventilation, and Oxygenation, Wednesday June 10th
1/85
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
86 Terms
Chart not much testing on this;
Physiology
Introduction
An open airway, adequate ventilation, and sufficient oxygenation are necessary to sustain life.
You must recognize when to intervene to open and maintain the airway, provide artificial ventilation, and administer supplemental oxygen.
Fix oxygen first.
Cyonosis - look blue
Respiration
Pulmonary ventilation
External respiration
Internal respiration
Cellular respiration
Respiratory Physiology
Respiration is the process of gas exchange.
Oxygenation and removal of carbon dioxide occur as a result of external and internal respiration.
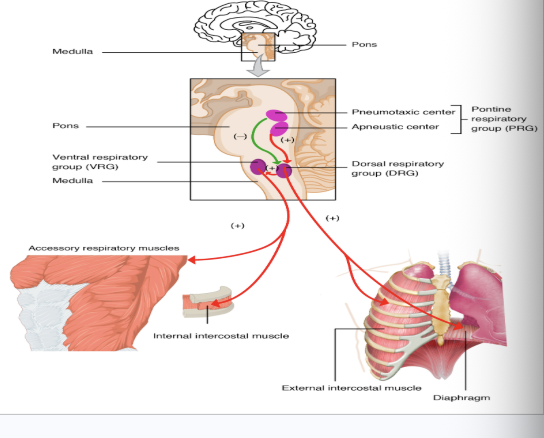
Pulmonary Ventilation
Control of Respiration
Medulla controls respiration
Normal Physiology
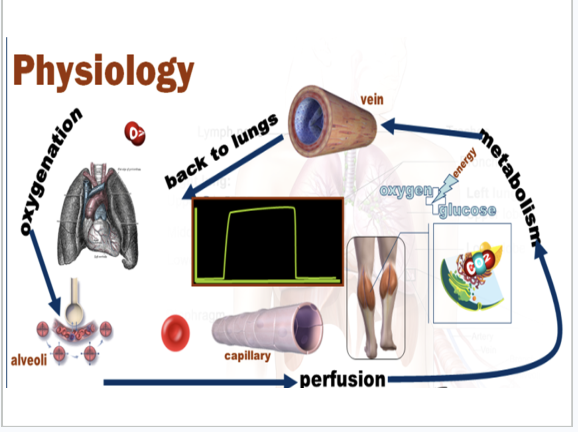
Normal respiratory physiology involves the continuous exchange of oxygen and carbon dioxide between the body and the environment. This process sustains cellular metabolism through four key steps: ventilation(breathing in and out), diffusion (gas exchange at the alveoli), perfusion (blood circulation), and regulation(neural control). [1, 2, 3]
1. Ventilation (Mechanics of Breathing)
Inspiration: An active process where the brainstem signals the diaphragm and external intercostal muscles to contract. This flattens the diaphragm and expands the rib cage, decreasing intrapleural and alveolar pressure below atmospheric pressure, forcing air into the lungs. [1, 2, 3, 4]
Expiration: A passive process at rest. The inspiratory muscles relax, and the lungs naturally recoil due to elastic tissue, increasing alveolar pressure above atmospheric pressure and pushing air out. [1, 2, 3]
Key Volumes: A normal adult at rest breathes 12–20 times per minute, moving a Tidal Volume (TV) of approximately 500 mL of air per breath. Roughly 150 mL stays in the "anatomical dead space" (conducting airways) and does not participate in gas exchange. [1, 2, 3]
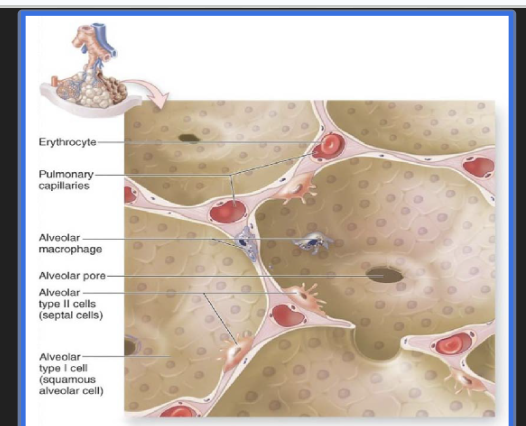
2. Diffusion (Gas Exchange)
Blood-Gas Barrier: Air travels down the trachea and branching bronchioles into the alveoli, which are surrounded by pulmonary capillaries. The barrier between them is extremely thin (comprising Type I alveolar pneumocytes, capillary endothelium, and fused basement membranes) to allow rapid diffusion.[1]
Pressure Gradients: Gases move passively from areas of high partial pressure to low partial pressure. Oxygen (O₂) diffuses from the alveoli into the deoxygenated blood, while carbon dioxide (CO₂) diffuses from the blood into the alveoli to be exhaled. [1, 2, 3]
3. Perfusion & Gas Transport
Ventilation-Perfusion (V : Q) Matching: For optimal gas exchange, ventilation (air reaching the alveoli) must closely match perfusion (blood flowing through the capillaries). The ideal overall ratio is approximately 0.8 at rest. [1, 2, 3, 4, 5]
Oxygen Transport: About 98% of oxygen binds to hemoglobin inside red blood cells, while the remaining 2% dissolves directly into the blood plasma. [1, 2, 3]
Carbon Dioxide Transport: CO₂ is transported out of the tissues in three ways: dissolved in plasma (approx. 7-10%), bound to hemoglobin (approx. 20-30%), and converted into bicarbonate ions (HCO₃⁻) in the blood (approx. 60-70%). [1, 2, 3, 4, 5]
4. Respiratory Regulation
Neural Control: Breathing is an involuntary process primarily governed by the respiratory centers in the brainstem (medulla oblongata and pons). The medullary center acts as the pacemaker, setting the basic respiratory rhythm. [1, 2, 3, 4, 5]
Chemical Control: Central and peripheral chemoreceptors constantly monitor the blood levels of CO₂, O₂, and pH. They primarily trigger adjustments to breathing rate and depth to maintain acid-base balance and expel excess CO₂ when metabolic demand increases.
Normal Physiology

Abnormal Physiology of Respiratory System
Abnormal respiratory physiology refers to the inability of the respiratory system to adequately deliver oxygen to the tissues or remove carbon dioxide from the blood. It stems from disruptions in ventilation (air movement), perfusion (blood flow), or gas exchange, resulting in altered breathing patterns and impaired gas exchange. [1, 2, 3, 4]
Key Mechanisms of Impaired Gas Exchange
Hypoventilation: Breathing is too shallow or slow. The amount of inspired air is insufficient, causing alveolar carbon dioxide to rise and oxygen to fall. [1, 2]
Ventilation-Perfusion (V/Q) Mismatch: An imbalance between the air reaching the alveoli (\(V\)) and the blood perfusing the capillaries (\(Q\)). For example, pulmonary embolisms block blood flow, while pneumonia or mucus clogs block airflow. [1, 2, 3]
Diffusion Limitation: Thickening of the alveolar-capillary membrane (e.g., in pulmonary fibrosis) prevents oxygen and carbon dioxide from crossing efficiently. [1, 2, 3, 4]
Shunting: Deoxygenated blood bypasses the alveoli entirely and enters the systemic circulation without being oxygenated (e.g., severe atelectasis). [1, 2]
Functional Classifications of Lung Disease
Respiratory abnormalities are commonly divided into two main functional categories based on pulmonary function tests: [1, 2]
Obstructive Defects: Characterized by difficulty exhaling air due to increased airway resistance. Conditions like asthma and COPD result in a reduced \(FEV_1/FVC\) ratio. [1, 2, 3]
Restrictive Defects: Characterized by a reduced total lung capacity due to a physical inability to fully expand the lungs. Causes range from intrinsic lung tissue stiffening (e.g., pulmonary fibrosis) to chest wall deformities (e.g., kyphoscoliosis) or neuromuscular weakness. [1, 2, 3, 4, 5]
Consequences & Respiratory Failure
When compensation mechanisms fail, the body enters respiratory failure: [1]
Type I (Hypoxemic): Low oxygen (\(PaO_{2}\)) but normal or low carbon dioxide (\(PaCO_{2}\)).
Type II (Hypercapnic): Low oxygen (\(PaO_{2}\)) alongside abnormally high carbon dioxide (\(PaCO_{2}\)). [1, 2]
Pathological Breathing Patterns
Breathing patterns often change to compensate for biochemical or neural imbalances: [1, 2]
Tachypnea: Abnormally rapid breathing (e.g., in response to metabolic acidosis).
Cheyne-Stokes Respiration: Oscillating cycles of deep/fast breathing alternating with periods of apnea, often seen in central nervous system dysfunction or heart failure.
Hyperventilation: Breathing deeper and faster than metabolic requirements, leading to abnormally low carbon dioxide levels
Hypoxemia:
Hypoxemia is a low oxygen content in arterial blood
Inadequate ventilation of alveoli despite adequate lung perfusion
Inadequate lung perfusion despite adequate ventilation
Combination of both
Hypoxia
Hypoxia means inadequate oxygen is being delivered to the cells
Airway obstruction
Inadequate breathing
Shock (Hypoperfusion)
mild to moderate hypoxia
Restlessness, anxiety, and agitation
Tachypnea
Dyspnea
Pale, cool, clammy skin
Tachycardia
Elevation in blood pressure
Severe hypoxia
Tachypnea - abnormally rapid, shallow breathing. Normal respiratory rate is 12 to 12 breaths per minute for adults, tachypnea involves taking more than 20 breaths per minute.
Dyspnea - shorntness of breath or difficulty breathing. Tightnest in chest, air hunger, or inability to catch their breath. More than 20 to 25 breaths per minute
Cyanosis - is a bluish or purplish discoloration of the skin, lips, or nail beds caused by an abnormally low level of oxygen in the blood. It happens because oxygen-depleted blood is darker and takes on a blue tint, which becomes visible through areas with thin skin or high blood flow
Tachycardia/dysrhythmias/bradycardia - An arrhythmia is an umbrella term for any problem with the rate or rhythm of your heartbeat. Your heart may beat too quickly (tachycardia), too slowly (bradycardia), or irregularly. A healthy resting heart rate is generally between 60 and 100 beats per minute. [1, 2, 3, 4, 5]
Tachycardia (Fast Heart Rate)
Tachycardia occurs when the resting heart rate is faster than 100 beats per minute. [1, 2]
Types: Includes Atrial Fibrillation (AFib), Atrial Flutter, and Supraventricular Tachycardia (SVT).
Common Causes: Strenuous exercise, stress, fever, or underlying conditions like high blood pressure, thyroid issues, and heart disease. [1, 2, 3, 4, 5]
Bradycardia (Slow Heart Rate)
Bradycardia occurs when the resting heart rate is slower than 60 beats per minute. [1, 2, 3]
When it's normal: A slow heart rate can occur during sleep and is also common in highly trained athletes.
When it's a concern: It becomes problematic if it causes symptoms like dizziness, fainting, or chest pain because the heart isn't pumping enough oxygen-rich blood to the body. [1, 2, 3, 4, 5]
Tachy-Brady Syndrome
This is a specific heart rhythm disorder where the heart’s natural pacemaker malfunctions, causing the heart rate to dangerously fluctuate between both extremes. Patients with this condition often require specialized management
Severe confusion/AMS - Severe confusion or sudden altered mental status (AMS) is always a medical emergency. It is not a diagnosis but a symptom indicating a brain function disruption from an underlying crisis like a stroke, severe infection, or hypoxia.
Loss of coordination
Sleepy appearance
Head bobbing
Slow reaction time
Hypoxia results in bradycardia instead of tachycardia
Pediatric differences
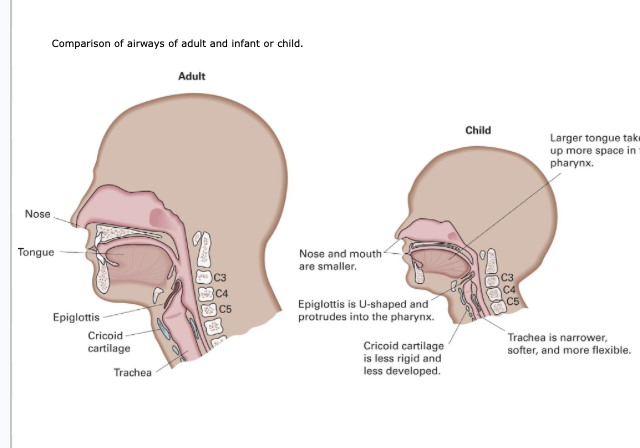
Pedi Resp A&P Differences
Chest wall is pliable
Increased reliance on diaphragm
Lungs are easily overinflated in artificial ventilation
Limited oxygen reserves
High metabolic rate and oxygen needs
Hypoxia is the most common cause of cardiac arrest
Hypoxia may result in bradycardia, instead of tachycardia
Very sensitive to changes in oxygenation and perfusion
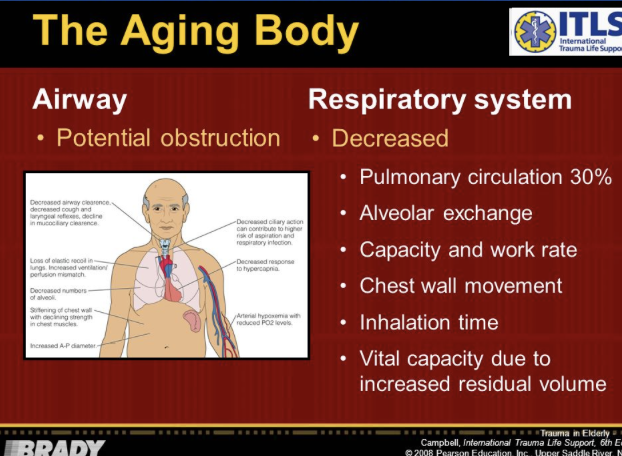
Geriatric Differences
The aging body
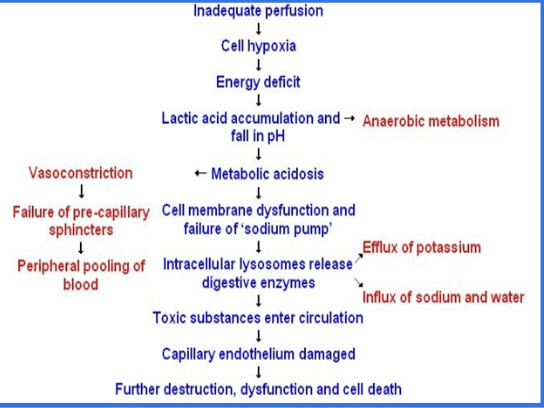
Respiratory Pathophysiology
Cellular Hypoxia
Inadequate Oxygen delivered to cells
Disturbance in ventilation or respiration
Anaerobic metabolism results in:
Insufficient energy production
Buildup of lactic acid
Cell dysfunction→ ischemia→ injury → death
Ischemia is a medical term for a condition where blood flow and oxygen supply to a specific part of the body are restricted. It is typically caused by narrowed arteries or blood clots, and if left untreated, it can lead to severe damage or tissue death (infarction). [1, 2, 3, 4]
Impaired Pulmonary Ventilation
Etiology: why
Interruption of nervous control
Damage to thorax
Increased airway resistance
Loss of airway patency
Impaired Gas Exchange
Etiology
Gas exchange may be impaired by:
↓ ambient oxygen content
Lung disease
Drowning
Toxic gases
Neurological impairment (injury or degenerative process)
when people drown, epiglottis shuts down.
Hypoperfusion
Poor perfusion also leads to cellular hypoxia.
It may be caused by:
Obstructed forward movement of blood
Hypovolemia
Hypovolemia is a medical condition characterized by an abnormally low volume of circulating blood or extracellular fluid in the body. It is primarily caused by significant fluid loss through trauma, internal bleeding, severe vomiting, diarrhea, or excessive sweating, and requires immediate management to prevent circulatory failure
Airway Assessment
Airway Assessment and Management
Patency
Conscious Pt- if speaking- airway patent (in general)
Altered or Unconscious
You must open the mouth to assess the airway
Clear the airway of liquids or foreign bodies
POSITIONING- Conscious or unconscious
Hear gurgling, hear fluid, suction it out.
Signs of an Open Airway
Air can be felt and hard moving in and out of the mouth and nose
The patient is speaking in full senates or with little difficulty
The sound of the voice is normal for the patient
Signs of a Blocked or Inadequate Airway
Abnormal upper airway sound (stridor, snoring, crowing, or gurgling)
An awake patient who is unable to speak
evidence of a foreign body airway obstruction (tongue, food, vomit, blood, or teeth in the upper airway, mouth or nose)
swelling to the mouth, tongue, or oropharynx.
Upper Airway sounds.
Snoring
caused by the tongue obstructing the airway
Crowing
caused by muscle spasms around the larynx
Gurgling
caused by liquid in the airway
Stridor - something in there.
swelling of the larynx
Airway Assessment and Management
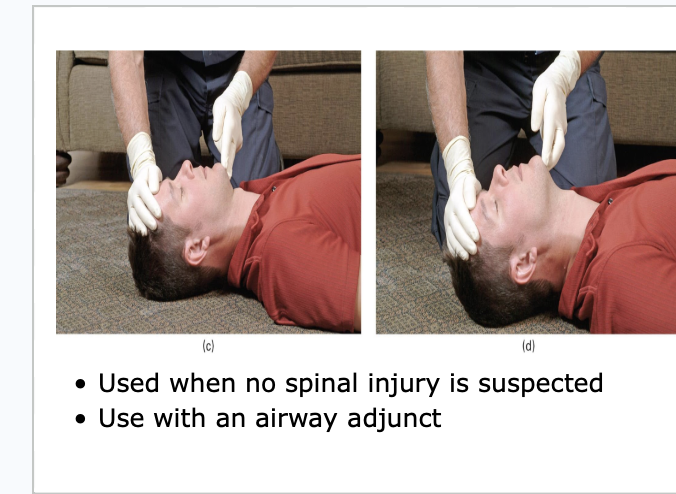
Opening the airway
Manual maneuvers
Once open- maintain open
Suction
Rigid and soft
Mechanical airways
Oral and Nasopharyngeal

Picture
Picture

Picture

Unpatient Airway
Open the airway

Jaw Thrust Maneuver
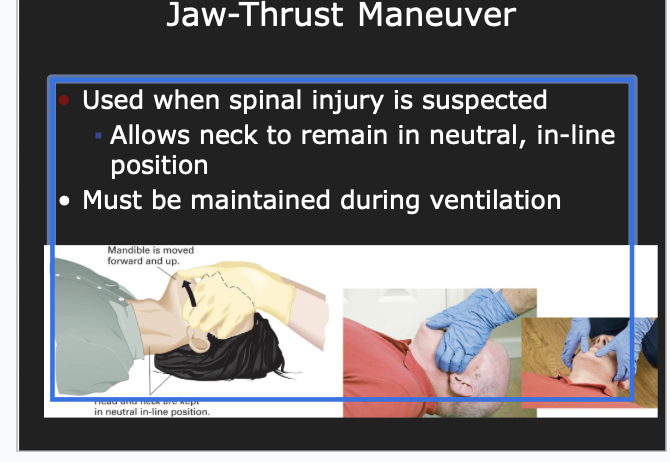
picture

Recovery Position

Suction
Gurgling indicates liquid in the airway.
Use suction to remove blood, vomitus, secretions, and any other liquids, food particles, or objects from the mouth and airway
Suction devices must generate enough negative pressure to remove fluids from the airway
Suction Equipment
May be mounted in the ambulance or portable
Must generate enough vacuum and airflow to clear the airway
Must have wide-bore, thick tubing, a collection bottle, and water supply
Catheters
Rigid (Yankauer/DuCanto)
Soft (French Tip)
Tubing (for large secretions in mouth)

Suction Pearls
Rigid catheter -the mouth and oropharynx
Soft catheter - nose, nasopharynx, mouth and oropharynx
Tubing- large secretions
Insert only as far as you can see into the mouth.
Avoid touching the back of the oropharynx.
Suction < 15 sec on removal of catheter
No more than 15 seconds of suctioning.
Airway Adjuncts
Used in conjunction with manual airway maneuvers
Does not take the place of keeping airway open with head-tilt, chin-lift or jaw-thrust
If the patient becomes more responsive or gags, remove the adjunct.
Includes oropharyngeal and nasopharyngeal airways
The proper size airway adjunct must be selected.
Airway adjuncts do not protect from aspiration into the lungs.

Oropharyngeal Airways
Oropharyngeal airways are used in patients who are unresponsive, without a gag reflex.
The device must be sized properly
Measure from corner of mouth to tip of ear
Place either directly with tongue blade -or-
Insert bevel up and rotate when you meet resistance of soft palate
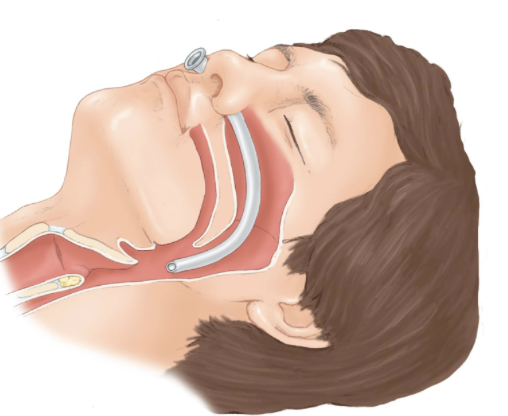
Nasopharyngeal Airways
Oropharyngeal airways are used in patients who are unresponsive, without a gag reflex.
The device must be sized properly
Measure from corner of mouth to tip of ear
Place either directly with tongue blade -or-
Insert bevel up and rotate when you meet resistance of soft palate
May cause gagging or vomiting
Does not prevent aspiration
Insertion
May cause trauma to nasal mucosa; must be lubricated
Measure from tip of nose to ear
Insert in nare (usually right) with bevel toward septum

Creates channel: Nasal
If one adjunct, positioning, and airway maneuvers are not sufficient, you may combine them
Breathing Assessment and Management
Topics
Breathing Assessment
Deciding to Ventilate
Techniques of Artificial Ventilation
Special Considerations
Oxygen Therapy
Assessment of Breathing
Establish a patent airway
Assess the adequacy of the patient's breathing
Inadequate breathing leads to poor gas exchange in the alveoli inadequate oxygenation.
Focus on the rate of breathing, the volume of each breath, and rhythm
Minute Volume
A function of both respiratory rate and tidal volume
A change in either respiratory rate or tidal volume affects minute volume.
Minute volume = RR x TV
5-8L/min (10+L/min - hyperventilation)
What would cause changes in tidal volume and respiratory rate?
Alveolar Ventilation
Alveolar ventilation is the amount of air breathed in that reaches the alveoli.
Alveolar ventilation = (tidal volume – dead space air) × respiratory rate
Dead air space does not change when tidal volume decreases.
Rapid respirations can decrease the tidal volume.
Anything above 12 or under 8 breaths per minute is inadequate breathing. Also dependent on patient
Dead space: Upper airways to lower airways. Air is there but is not moving.
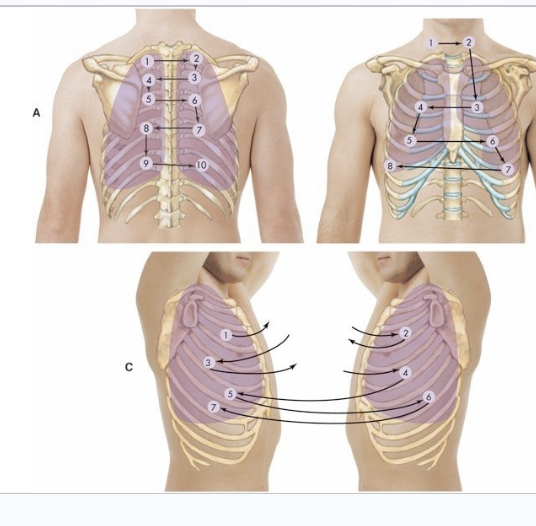
Assessing for Adequate Breathing
ASSESS
Rate
Rhythm
Quality
Depth
by looking, listening/auscultating, feeling
Are they getting adequate breathing to the bases of the lungs. Make sure air is moving to bases and top as well.
Breathing Patterns
diabetic patients: hyperglycemic
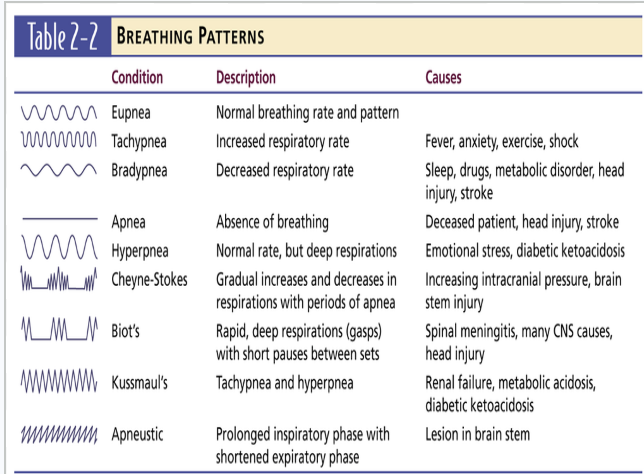
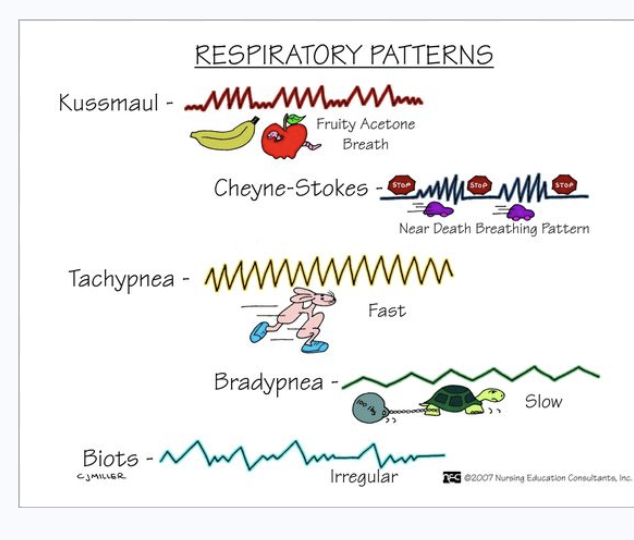
Respiratory patterns
Signs of Adequate Breathing
normal respiratory rate
clear and equal breath sounds bilaterally
adequate air movement heard and felt from nose and mouth (tidal volume)
good cheer rise and fall with each ventilation (tidal volume)
Respiratory Distress vs. Failure vs. Arrest
Respiratory distress
Breathing can be adequate, but if the patient is working harder to breathe
Hypoxia→ cells in brain begins to die within 4 to 6 minutes.
Inadequate breathing can be categorized as respiratory failure or respiratory arrest.
Patients with respiratory failure or arrest require immediate positive pressure ventilation.
Causes of Respiratory Distress/Failure
Stroke - brain injury
Myocardial infarction - heart attack
Drug overdose - opioid overdoses especially
Toxic inhalation - hydrogen cyanade gas
Electrocution
Suffocation - walking into a room filled with gas
Traumatic injuries - phrenic nerve
Infection of the epiglottis - blockages
Airway obstruction - blockages
epligottis is horrible for kids because there airways are small
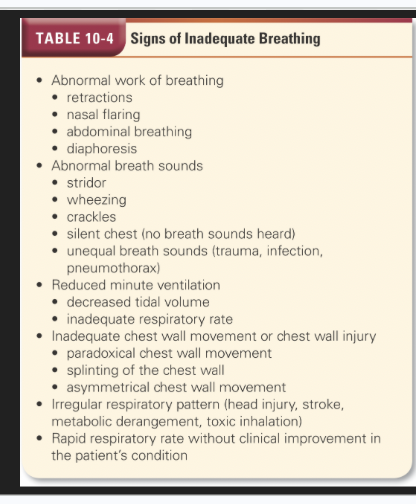
Signs of Inadequate breathing
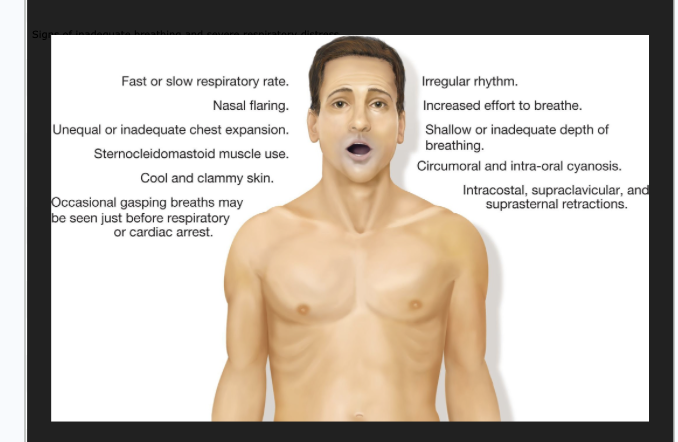
Picture
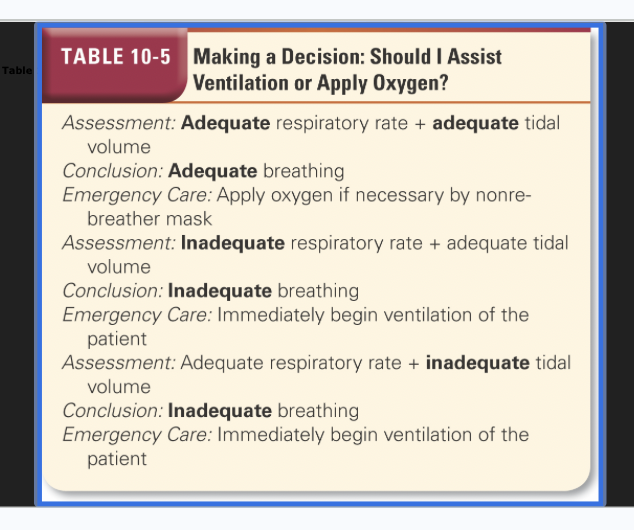
Oxygen Therapy and Artificial Ventilations
Making a Decision: Should I assist ventilation or Apply oxygen?
Effects of Positive Pressure Ventilation
PPV does not rely on negative pressure
Air is forced into the alveoli.
PPV ↑ airway wall pressure
PPV can lead to gastric distention by overcoming esophageal opening pressure,
Negative pressure from spontaneous breathing assists blood return to the heart
PPV decreases cardiac output.
If nothing moving give PPV. You can give epinephrine 0.3.
Force air into their alveoli - do this through CPAP ;BVM
Rules of Threes for Ventilation - skipped in slideshow
Three providers
Three inches
Three fingers
Three airways
Three PSI
Three seconds
Artificial Ventilation
You must be able to maintain a good mask seal.
2 EMTs
Pull face into the mask
The device must deliver an adequate volume of air to inflate the lungs.
Chest Rise
Adequate Ventilation
Perfusing
Newborns- 40-60/min
Infants/young children- 12-20/min or once every 3-5 seconds
Adults- 10-12/min or once every 5-6 seconds
Deliver each breath over 1-2 seconds
If spontaneously breaths- sync to pt’s rate
Cardiac arrest
Newborns→ 3:1
Infants, children and adults---> 30 to 2
Consistent tidal volume, sufficient to cause chest rise
Heart rate returns to normal
Color improves
Inadequate Ventilation
Ventilation rate is too fast or too slow.
The chest does not rise and fall.
The heart rate does not return to normal.
Color does not improve.
Does airway need to be repositioned?
Additional provider needed?
Cricoid Pressure needed?
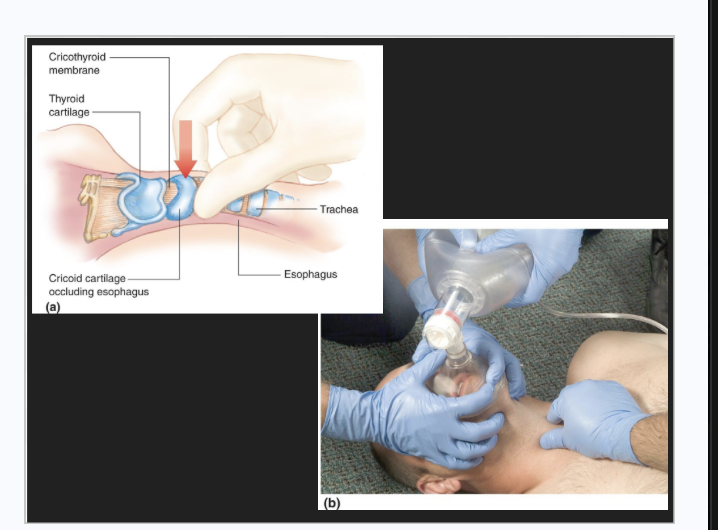
Sellicks Manuever - skipped in slideshow
Cricoid pressure is not recommended for routine use, but can be used in some situations.
Adult intubation
Pediatric patient when an extra EMT is available
BURP- backwards, upward, rightward pressure
Avoiding Gastric Inflation
Leads to regurgitation and aspiration, and impaired ventilation
Reduce the tidal volume delivered and use supplemental oxygen to maintain oxygenation with a smaller tidal volume
MORE isn’t necessarily BETTER
Mouth to Mask Ventilation
Advantages
A single EMT can maintain a good seal with the mask.
Eliminates direct contact with the patient
One-way valve prevents exposure to the patient's exhaled air.
Provides adequate tidal volume
Supplemental oxygen can be administered.
Disadvantages
The mask is perceived by some EMTs as having an increased risk of infection.
The EMT providing ventilation may fatigue.
Doesn't allow for the highest possible concentration of oxygen to be delivered


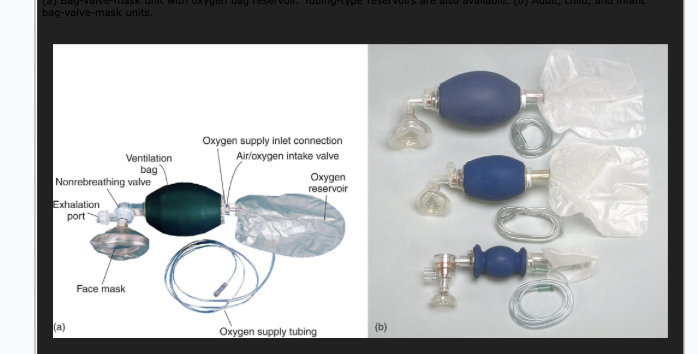
Bag Valve Mask
Select the appropriate size and use only enough volume to cause the chest to rise.
Two-person technique is preferred.
Position the mask, use an "E-C" technique.
A second EMT squeezes the bag
Can deliver close to 100% oxygen
May allow medication administration
Ventilating a Spontaneously Breathing Patient
Recognize the need to ventilate a patient who is breathing, but breathing inadequately.
Complications include uncooperative patients, inadequate mask seal, and overinflation of the lungs.
Explain the procedure to the patient.
Ventilate to achieve the normal rate and/or tidal volume.
FROPVD - skipped in slideshow
Flow-restricted, oxygen-powered ventilation device
A manually triggered ventilation device
Delivers 100% ventilation
Can be used by one EMT using a two-handed technique to seal the mask
Only for adult patients, not currently allowed in MA

CPAP
Continuous positive airway pressure
A form of noninvasive positive pressure ventilation
CPAP can help avoid the need for endotracheal intubation in some patients.
Used in awake, spontaneously breathing patients who need ventilatory support
Oxygen should be titrated to the patient's SpO2 reading, and signs and symptoms.
Positive pressure is measured in cmH2O.
Positive pressure helps inflate collapsed alveoli and improve oxygenation.
Decreases the work of breathing
Helps displace fluid in alveoli in left ventricular failure
Delivered at 2 to 20 cmH2O
Begin at ~5 and titrate to pt response
Patient criteria
Awake and can obey commands
Can maintain his airway
Breathing on his own, respiratory distress
Has signs and symptoms of moderate to severe respiratory distress, or early respiratory failure
Putting a lot of pressure into chest. Squeezes vena cava, slows return of blood to heart which lowers blood pressure. That’s why patients need to have good blood pressure to put this on.
PEP; holds alveoli open. Five pep is enough to hold alveoli open. Posive and expiatory pressure.
Also improves oxygenation and saturation. Opening up more collapsed alveoli.
pneumonia, asthma, Congestive heart patients. used it on an ALS patient.
CPAP Contraindications
Apnea or agonal respirations
Inability to follow commands
Inability to maintain an airway
Unresponsive
Shock with cardiac insufficiency
Upper GI bleeding
Pneumothorax or chest trauma
Tracheotomy
Facial trauma
Increased intrathoracic pressure
Cardiac arrest
Vomiting
Don’t put CPAP if any of this above. Any trauma, no CPAP.
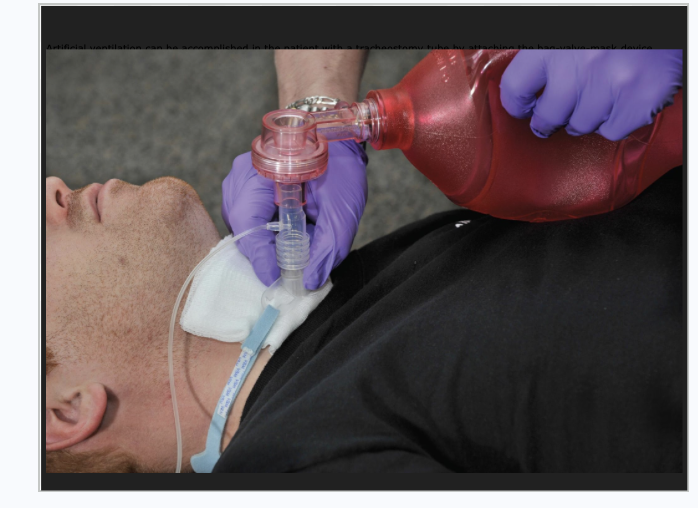
Special Considerations in Airway Management and Ventilation
stomas
trachaeostimy.
capnagrophy - measure the perfusion
Facial Injuries
Swelling can occlude the airway.
Use an airway adjunct if needed.
Avoid a nasopharyngeal airway in patients with mid-face trauma.
Bleeding may require frequent suctioning.
might require constant suctioning
Obstructions
Foreign body airway obstruction
If a patient is choking but is effectively moving air, instruct him to cough; administer high-concentration oxygen.
If air exchange is poor, manage as for a complete airway obstruction.
For a child or adult, perform abdominal thrusts for complete airway obstruction.
For an infant, perform chest thrusts and back blows for a complete airway obstruction.
Denial Appliances
Take dentures out
Oxygen Therapy
100% oxygen is stored in cylinders.
Cylinder volume varies.
Pressure in a full cylinder is 2,000 psi.
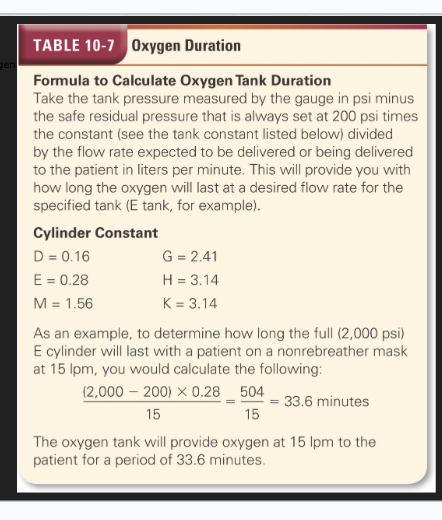
For long transports, calculate the duration of flow for the cylinder.
Safety when using, storing….
Oxygen Duration
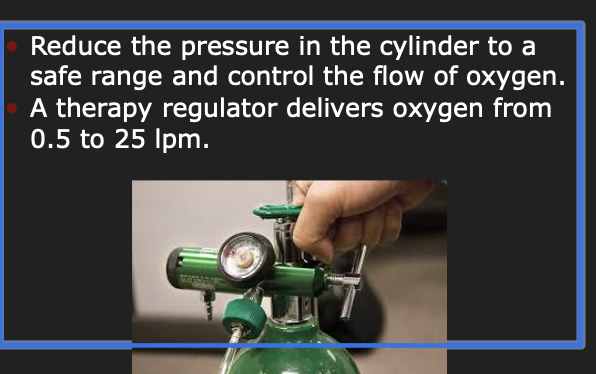
Regulators
Oxygen Therapy Indications
Signs of hypoxia and adequate respirations including AMS, SpO2 < 94%
When in doubt, give oxygen.
Never withhold oxygen from a patient who needs it!
Titrate oxygen to patient’s needs
Normal O2 saturation - 98 percent
Oxygen Therapy Decision Making
Too much oxygen can worsen conditions especially CVA and ACS
Vasoconstriction, free radicals
worse M&M
Begin administration at 2 lpm by nasal cannula.
Oxygen Delivery Devices
Nasal Cannula
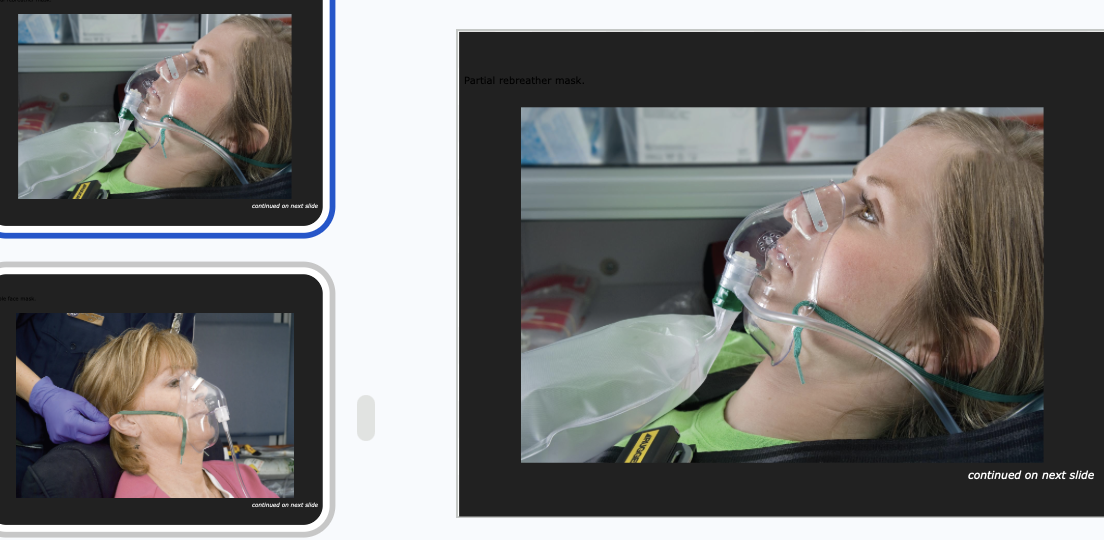
Non-rebreather mask
Simple face mask
Partial rebreather mask
Venturi mask
Tracheostomy mask
Nasal Cannula
A nasal cannula is used to deliver a lower concentration of oxygen.
The flow rate is 2lpm - 6lpm
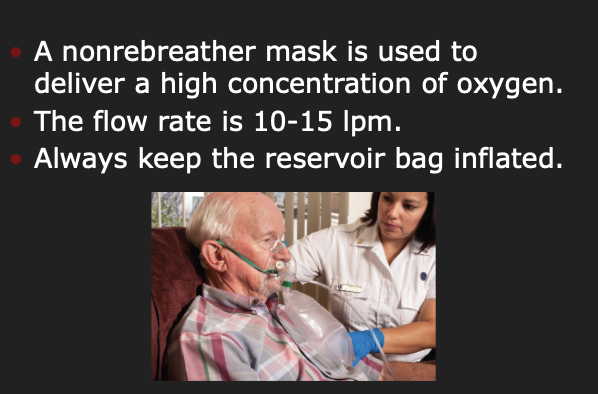
NRB Mark
Oxygen Humidifiers
Ventury mask. different color. Give certain percentage
Flaled chest - ventilate them