Neuro Unit 2 - Transcripts
1/507
Earn XP
Description and Tags
cont at 105
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
508 Terms
What is the basic job of an upper motor neuron (UMN)?
It carries motor signals from the brain toward the spinal cord and helps initiate/control movement
It does not directly innervate muscle
What is the basic job of a lower motor neuron (LMN)?
It carries motor signals from the spinal cord or cranial nerve motor nuclei to the muscle or target organ
It is the final common pathway for skeletal muscle movement
Why is the LMN called the final common pathway?
Because all voluntary skeletal muscle activation ultimately depends on the LMN reaching the muscle
The UMN cannot create movement without an intact LMN
Where do many UMNs originate?
Primary motor cortex in the precentral gyrus, just anterior to the central sulcus
Also premotor cortex and related cortical motor areas
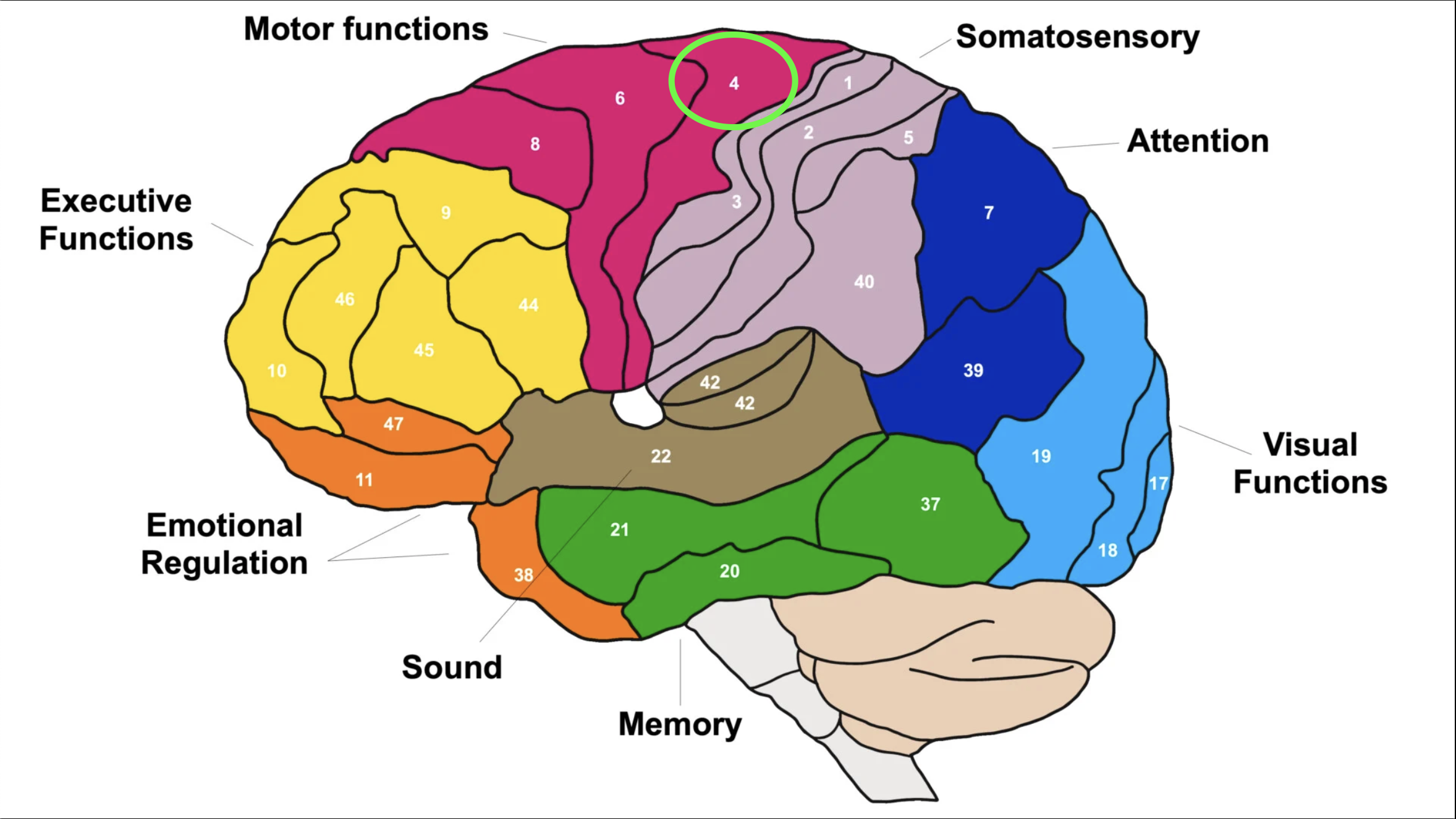
Which Brodmann area is the primary motor cortex?
Brodmann area 4 = precentral motor cortex / primary motor cortex
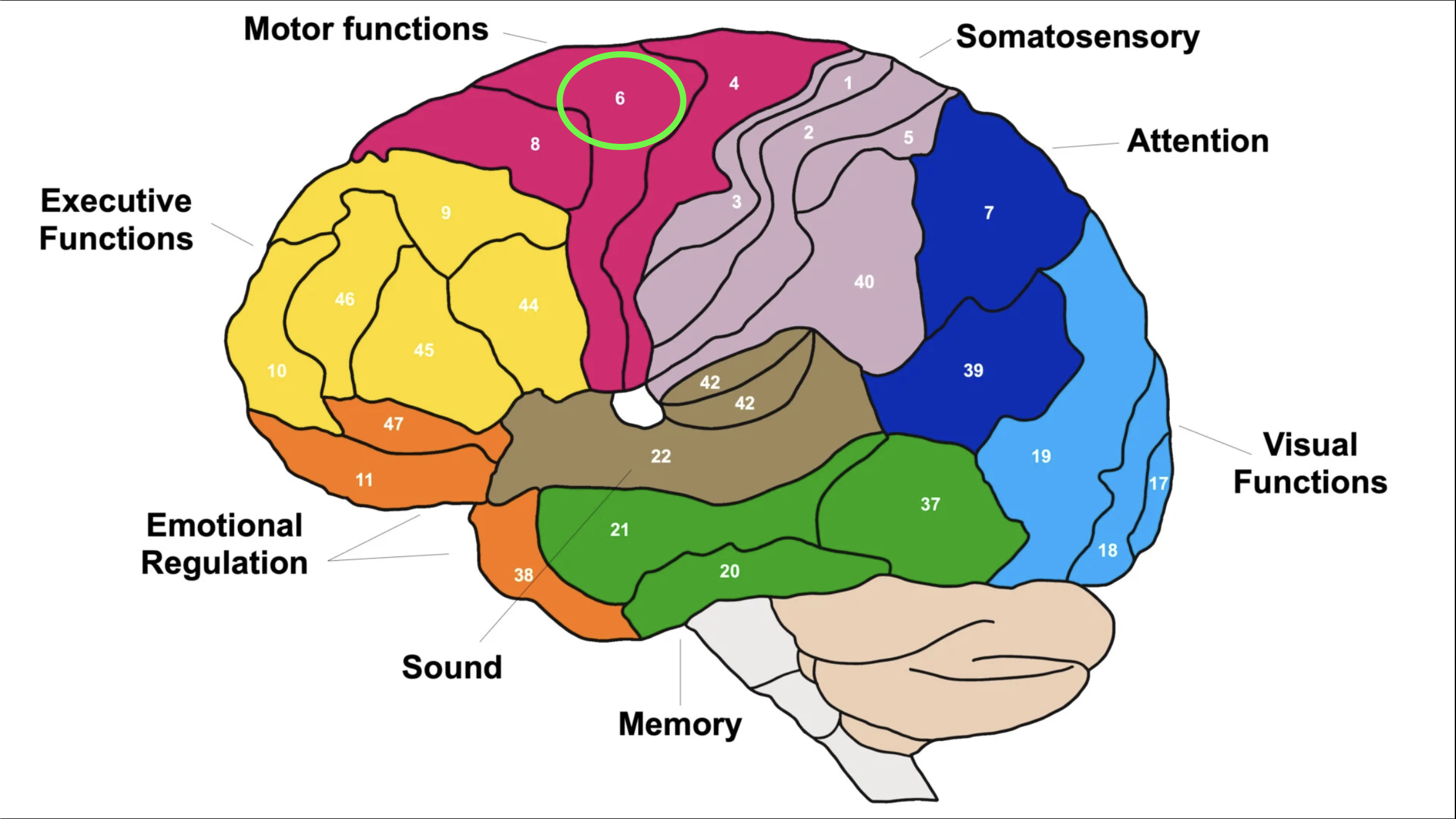
Which Brodmann area is the premotor area?
Brodmann area 6 = premotor area
What is the overall goal of the UMN system?
Precise control of movement, especially predominantly contralateral control of movement
What is the UMN's direct neural target?
The UMN communicates with the alpha motor neuron / LMN, not directly with the target organ
Where do UMNs terminate in the spinal cord?
They terminate/synapse in the ventral horn of the spinal cord, where LMNs receive the signal
What structures are included in a motor neuron?
Cell body/soma
Axon
Dendrites
Neuromuscular junction/motor end plate
What are the major adjustment centers for descending UMN activity?
The cerebellum and basal ganglia
They help adjust movement by influencing excitation/inhibition of LMN output
How does sensory information influence motor output?
Ascending sensory data interacts with descending motor data and helps adjust LMN output to muscle
What are the two major UMN pathway categories?
Pyramidal systems
Extrapyramidal systems
What makes a tract part of the pyramidal system?
It travels through the pyramids of the medulla
Examples include corticospinal and corticobulbar tracts
What tracts are included in the pyramidal system?
Corticospinal tract
Includes lateral and anterior divisions
Corticobulbar tract
What is the main movement system within the pyramidal tracts?
The corticospinal tract, especially for voluntary skilled movement
Corticospinal = movement
What does the corticobulbar tract control?
Motor control of the head and neck through cranial nerve motor nuclei
Corticobulbar = head & neck via cranial nerves
What does extrapyramidal mean?
Outside the medullary pyramids
These tracts fine-tune movement and are more involved in unconscious/involuntary motor control
Name the main extrapyramidal descending tracts.
Reticulospinal: posture and muscle tone
Rubrospinal: limb flexor movement
Vestibulospinal: balance and posture
Tectospinal: reflex head/neck turning
What neurotransmitter is key at the neuromuscular junction?
Acetylcholine (ACh)
Which Brodmann areas are Broca's areas?
Brodmann areas 44 and 45
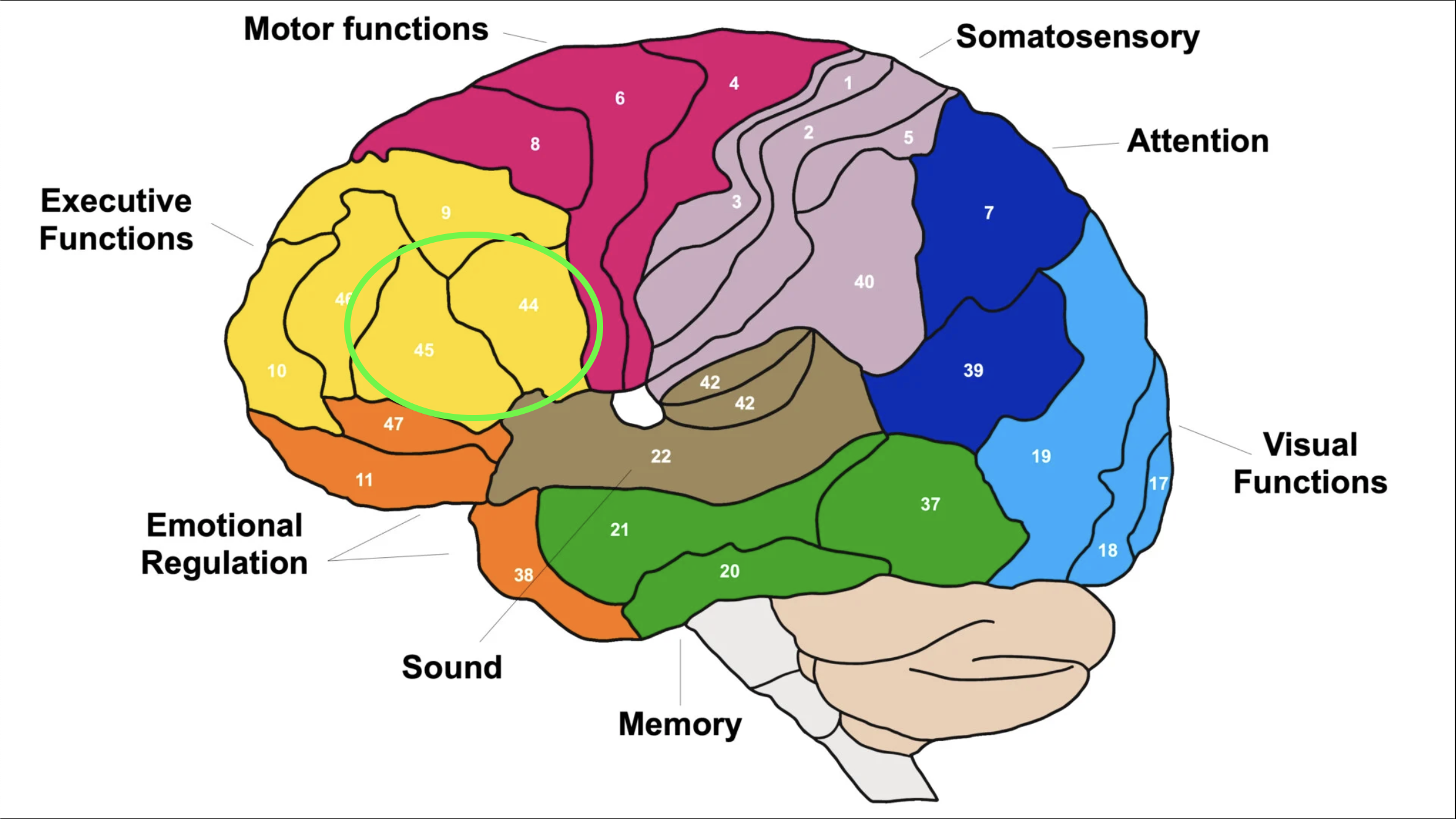
What is Broca's aphasia?
The patient generally understands language but has difficulty producing speech/language effectively
Which Brodmann area is Wernicke's area?
Brodmann area 22
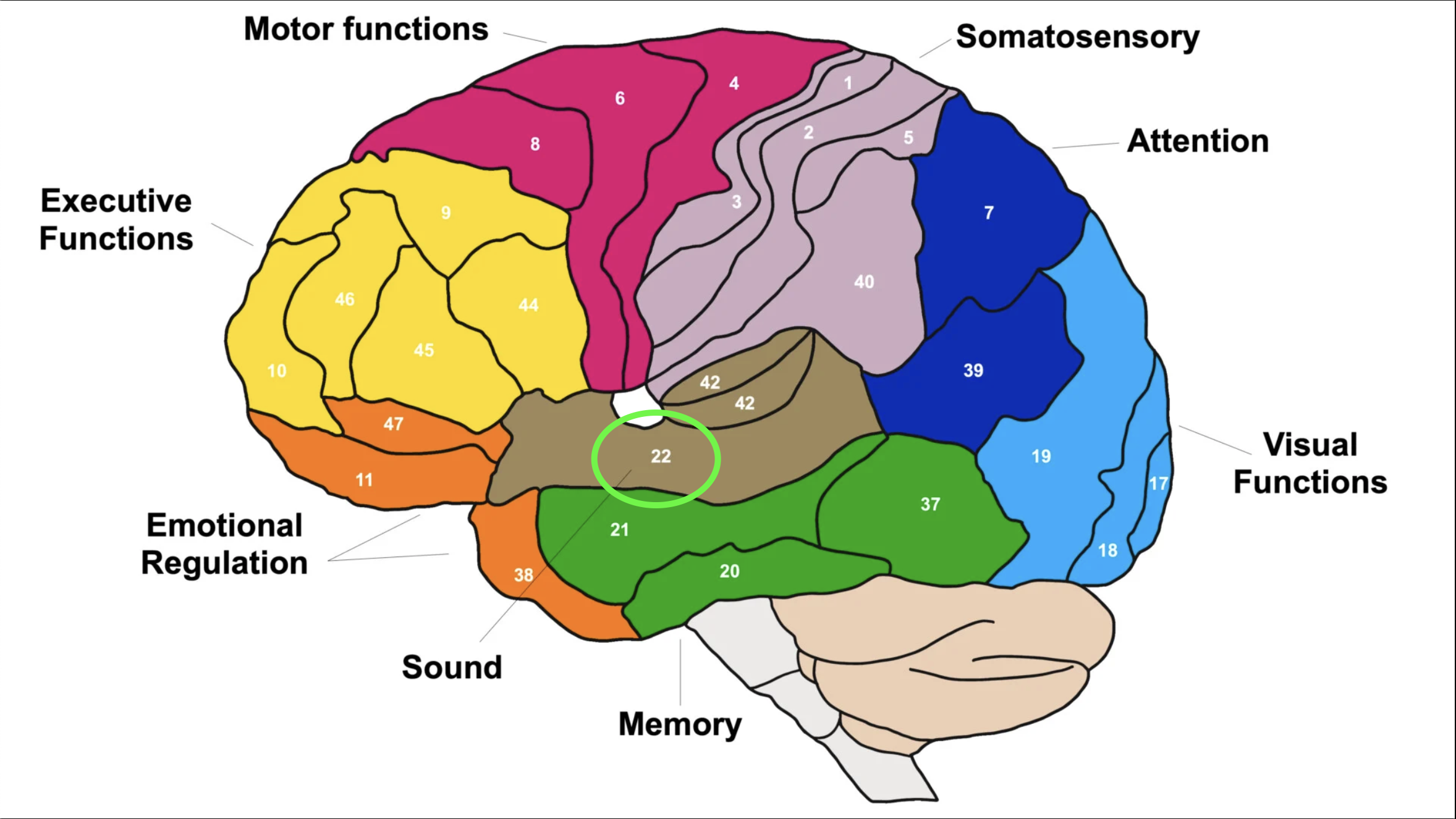
What is Wernicke's aphasia?
Fluent speech that does not make sense, impaired language comprehension, and unreliable history if the patient is alone
Broca vs Wernicke aphasia: what is the quick difference?
Broca: understands but cannot produce well
Wernicke: fluent but nonsensical and poor comprehension
How are spinal tracts named?
Usually by origin → termination
Examples:
Spinothalamic = spinal cord to thalamus
Corticospinal = cortex to spinal cord
What are tracts?
Bundles of long axons traveling within CNS white matter
What should you know for each descending tract?
Location in the spinal cord
Whether it crosses/decussates
Function
What does the lateral corticospinal tract control?
Fine, skilled limb movement
It crosses in the medulla at the medullary pyramids
What does the anterior corticospinal tract control?
More axial/upper body control: UE, head, neck, shoulders, and upper trunk depending on lecture framing
What does the tectospinal tract do?
Reflexive head turning in response to visual/auditory stimuli and support of postural control
¼ extrapyramidal descending tracts
Where does the tectospinal tract cross?
It crosses in the midbrain
What are the main functions of the reticulospinal tracts?
Posture, balance, tone/postural preparation, and regulation of pain awareness
¼ extrapyramidal descending tracts
Do the lateral and medial reticulospinal tracts cross?
They generally do not cross
What are the main functions of the vestibulospinal tracts?
Posture, balance, antigravity control, and maintaining head position when the base of support changes
¼ extrapyramidal descending tracts
Which ascending tracts are part of the DCML system?
Fasciculus gracilis
Fasciculus cuneatus
What does fasciculus gracilis carry?
Sensory input from below about T6/T7
Lower limb/lower trunk position, deep touch, vibration, and proprioception
What does fasciculus cuneatus carry?
Sensory input from above about T6/T7
Upper limb/upper trunk position, deep touch, vibration, and proprioception
What is the Dorsal Column–Medial Lemniscus (DCML) system?
The DCML system is an ascending sensory tract that carries fine/discriminative touch, vibration, and conscious proprioception
Where does the DCML system cross?
In the medulla
What does the lateral spinothalamic tract carry?
Pain and temperature
What does the anterior spinothalamic tract carry?
Crude/gross touch, pressure, and poorly localized/indiscriminate touch
What does the spinoreticular tract carry?
Pain sensation related to tissue injury
What do the spinocerebellar tracts carry?
Unconscious proprioceptive information from muscle to the cerebellum
Which spinocerebellar tract remains ipsilateral?
Posterior/dorsal spinocerebellar tract
Which spinocerebellar tract crosses?
Anterior spinocerebellar tract
Later detail: it crosses twice, so it functionally ends up ipsilateral in the cerebellum.
What structures are included in the LMN system?
Alpha motor neuron
Gamma motor neuron
Neuromuscular junction/motor end plate
Muscle spindle
Golgi tendon organ
Free nerve endings
Muscle
Where is the Golgi tendon organ located?
In the tendinous portion of muscle
Where is the muscle spindle located?
Within the central portion/belly of the muscle
Where do alpha and gamma motor neurons synapse?
In the ventral horn of the spinal cord
What is a motor unit?
One alpha motor neuron and all the muscle fibers it innervates
When an alpha motor neuron activates, what happens to its muscle fibers?
ACh is released at all of its NMJs, and all fibers innervated by that alpha motor neuron contract
Why do eye muscles have fine motor control?
They have very small motor units, sometimes about 2 muscle fibers per alpha motor neuron
Why are gastrocnemius-soleus motor units less precise than eye muscles?
They may have ~2,000 muscle fibers per alpha motor neuron, so one neuron controls many fibers
What is alpha-gamma coactivation?
Simultaneous activity of alpha and gamma motor neurons so extrafusal contraction occurs while the muscle spindle stays sensitive to stretch
What does the alpha motor neuron innervate?
Extrafusal skeletal muscle fibers
The muscle fibers responsible for force, bulk, power, and contraction
What does the gamma motor neuron innervate?
Intrafusal fibers in the muscle spindle, helping maintain stretch sensitivity during contraction
What is the role of the gamma motor neuron?
It adjusts muscle spindle sensitivity
Helps regulate alpha motor neuron activity/tone
What are motor pools?
Clusters of alpha motor neurons in the ventral horn that innervate specific muscles or muscle groups
Anterior vs posterior motor pools: what do they mostly innervate?
Anterior motor pools mostly innervate extensors
Posterior motor pools mostly innervate flexors
What is a myotome?
A group of muscles innervated by a single spinal nerve/root level
How does the somatic nervous system connect to skeletal muscle?
One LMN projects directly to skeletal muscle
How does the autonomic nervous system differ from the somatic motor system?
ANS uses a two-neuron chain
Preganglionic neuron → ganglion → postganglionic neuron → target organ
In a UMN lesion, why is there minimal to no muscle atrophy?
Because the LMN and muscle remain connected, so there is not true denervation of the muscle
What does paresis mean?
Weakness
What does hemiparesis mean?
Weakness on one side of the body with the other side relatively maintained, commonly seen after stroke
Why do UMN lesions often cause hyperreflexia?
The spinal reflex arc is intact, but descending UMN regulation/inhibition is lost, so the reflex becomes exaggerated
What DTR grade suggests hyperreflexia?
3+ or 4+ instead of normal 2+
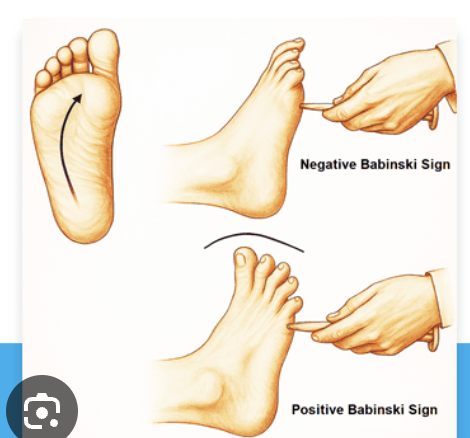
What is the normal adult Babinski response?
Hallux flexion, often with possible withdrawal
What is a positive Babinski sign?
Hallux extension toe, often with toe fanning/splaying
An UMN sign in adults
How do you test Babinski?
Use a cutaneous stimulus along the lateral plantar foot, then across the metatarsal heads toward the medial side
What is clonus?
Involuntary, repeating, rhythmic contraction of a muscle group in response to sustained stretch
How do you test gastrocnemius/ankle clonus?
Apply a light sustained upward pressure into dorsiflexion at the ball of the foot and watch/feel for rhythmic beating
What is sustained clonus?
Rhythmic beats continue as the stretch is maintained
Sustained clonus is pathologic
Why is clonus clinically useful?
It is a quick screen that raises concern for possible UMN involvement
What is spasticity?
Velocity-dependent resistance to quick passive stretch, strongly associated with UMN lesions
How do you test for biceps spasticity?
Move the elbow into extension at increasing speed and feel for velocity-dependent resistance from the biceps
How do you test for triceps spasticity?
Move the elbow into flexion at increasing speed and feel for velocity-dependent resistance from the triceps
What scale is commonly used to grade spasticity?
Modified Ashworth Scale
What is selective motor control?
The ability to isolate and coordinate intended muscle activation without unwanted co-contraction or abnormal synergy
What is co-contraction?
Agonist and antagonist muscles fire at the same time when they should normally take turns
Why do abnormal synergies occur after UMN lesions?
Loss of descending inhibition/fractionation disrupts normal alpha-gamma regulation, so muscles are coupled abnormally
What is a common upper extremity flexor synergy pattern after stroke?
Elbow flexion, wrist flexion, and upper limb held close to the chest
In LMN lesions, why does muscle atrophy occur?
There is disruption/denervation between the LMN/alpha motor neuron and muscle itself
What type of paralysis is associated with LMN lesions?
Flaccid paralysis
What happens to reflexes in LMN lesions?
Hyporeflexia or areflexia because the reflex arc/output pathway is disrupted
What is a fasciculation?
Visible or felt involuntary spontaneous twitching caused by activation of part or all of a motor unit
May be benign or abnormal
What is a fibrillation?
Muscle fiber-level activity from an unstable/denervated muscle membrane
Typically detected on EMG and associated with neuropathic/myopathic conditions
Fasciculation vs fibrillation: which is often visible?
Fasciculation (twitch) is often visible/felt
Fibrillation usually requires EMG detection
Why is EMG useful in weakness?
It helps determine:
Motor unit death/dysfunction
Whether the cause is neurogenic, myopathic, ALS, trauma, electrolyte imbalance, etc
What causes fibrillations physiologically?
Denervation/axonal death can create unstable muscle membranes and small ineffective depolarizations at the muscle fiber level
List classic UMN lesion signs
Weakness/paresis
Minimal atrophy
Hyperreflexia
Positive Babinski
Clonus
Spasticity
Abnormal synergies/loss of selective motor control
List classic LMN lesion signs.
Atrophy
Flaccid paralysis/weakness
Hyporeflexia or areflexia
Fasciculations
Fibrillations/denervation findings
Why is spinal cord injury usually considered an UMN lesion?
If the lesion is within the spinal cord above the anterior horn cell, descending UMN pathways are disrupted while LMN/reflex circuits below may remain intact
Which disorder is both UMN and LMN?
Amyotrophic lateral sclerosis (ALS)
Why are cranial nerves tricky when classifying UMN vs LMN?
Their nuclei are central in the brainstem, but their effector organs are outside the CNS, so cranial nerve motor output can be considered LMN
Give examples of UMN-related disorders from the lecture.
Cerebral palsy
stroke
multiple sclerosis
CNS tumors
seizures/epilepsy
dementia/Alzheimer's
Parkinson's disease
infection/meningitis
Huntington's
Friedreich's ataxia
SCI
What is cerebral palsy?
Damage to the immature brain occurring in utero, during the perinatal period, or immediately after birth
What structure is involved in Parkinson's disease?
Substantia nigra
Clinical signs include rigidity
What movement disorder is especially associated with cerebellar lesions?
Ataxia