ECG types
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
20 Terms
normal sinus rhythm

sinus tachycardia

sinus bradycardia

atrial flutter
No P waves instead flutter waves (sawtooth pattern) are formed at rate of 250-350bpm
Only some impulses conduct through the AV node, usually every other impulse
Heart rate: 75bpm
Rhythm: regular
P waves: flutter/sawtooth appearance
PR interval: none/unable
QRS complex: narrow 0.06 seconds
atrial fibrillation
No organised atrial depolarisation, so no normal P waves (impulses are not originating from the sinus node)
Atrial activity is chaotic resulting in an irregularly irregular rate, R-R interval is irregular
Red flag for blood clots and strokes
Heart rate: 100bpm
If above classified as fast AF
Rhythm: irregular
P waves: unclear, many
PR interval: unable
QRS complex: narrow at 0.08 seconds

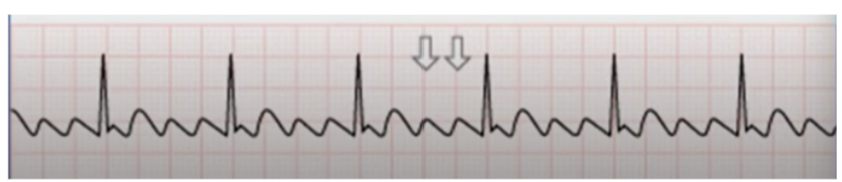
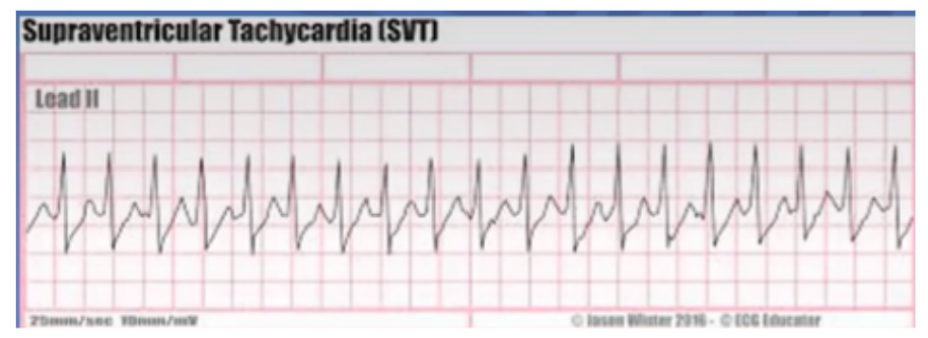
supraventricular tachycardia
Can’t see P waves
Narrow QRS
Continues until broken
Heart rate: 190bpm
Rhythm: regular
P waves: unknown (rhythm too fast)
PR interval: unknown
QRS complex: narrow 0.06 seconds
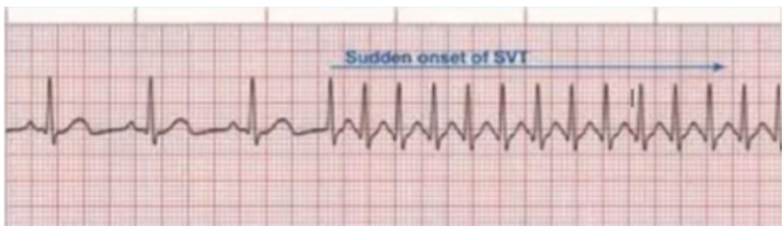
paraoxysmal SVT
Heart rate suddenly speeds up
Premature atrial contraction
P waves are lost
Narrow QRS
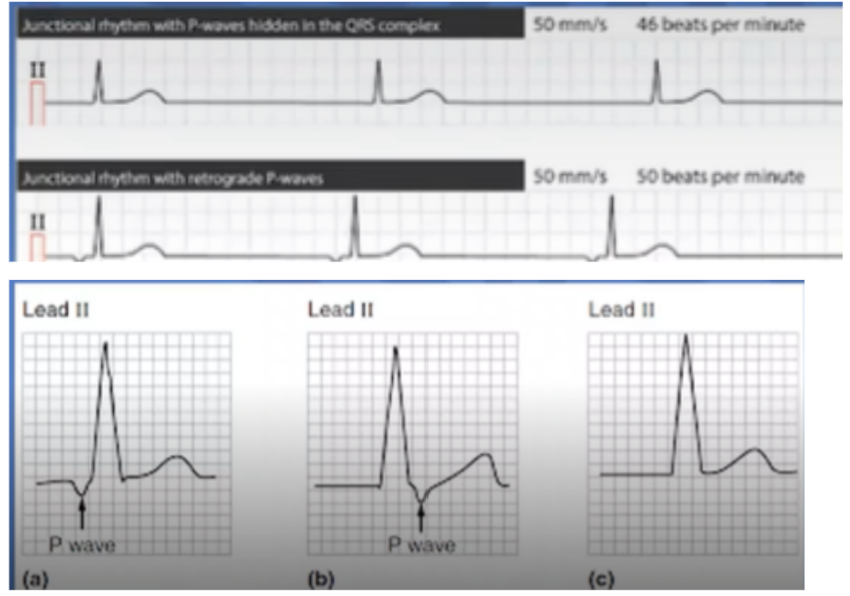
junctional rhythm
Pacemaker in the AV junction of bundle of HIS region
Electrical impulse travels backwards to depolarise atria so if p wave is seen it is inverted
Normal rate = 40-60bpm
>60 = accelerated junctional
>100 = junctional tachycardia
<40 = junctional escape
Heart rate: 40-60bpm
Rhythm: regular
P waves: inverted or missing
PR interval: unknown
QRS complex: narrow <0.12 seconds
sinus rhythm with 1st degree AV block
Prolonged conduction delay in the AV node or Bundle of HIS
PR interval = >20 seconds
Usually asymptomatic
Heart rate: 60
Rhythm: regular
P waves: present
PR interval: 0.36 seconds
QRS complex: 0.08 seconds (narrow)

2nd degree type I AV block
Mobitz 1/wenckebach
Irregular
More Ps than QRSs
PRI progressive lengthens then drops QRS
Heart rate: 60bpm
Rhythm: irregular
P waves: present, more than QRS
PR interval: progressively lengthens then drops QRS
QRS complex: narrow

2nd degree type II AV block
Mobitz 2
Regular
More Ps than QRSs
Consistent PR interval
Typically very bradycardic
Heart rate: 38bpm
Rhythm: regular
P waves: present, more than QRS
PR interval: consistent
QRS complex: narrow

3rd degree AV block
There is complete block of conduction in AV junction
Atria and ventricles form impulses independently of each other
Without impulses the ventricles intrinsic pacemaker kicks in at around 30-45bpm
Can result in no pulse eventually
Heart rate: 38bpm
Rhythm: regular QRSs and P waves but no relationship between the two
P waves: present
PR interval: variable
QRS complex: dependent, wide in this example

idioventricular escape rhythm
Causes: heart blocks, medication side effects, hyperkalemia
Rhythm originates in ventricles
Wide QRS complexes >0.12 seconds
Heart rate: 25bpm
Rhythm: regular
P waves: absent
PR interval: absent
QRS complex: wide, 0.16 seconds

accelerated idioventricular rhythm
has a faster rate

ventricular tachycardia
Impulse originating in ventricles
No P waves, wide QRS
Re-entrant pathway looping in a ventricle
“Normal” rate = >100bpm
<100bpm = accelerated idioventricular rhythm or ventricular escape

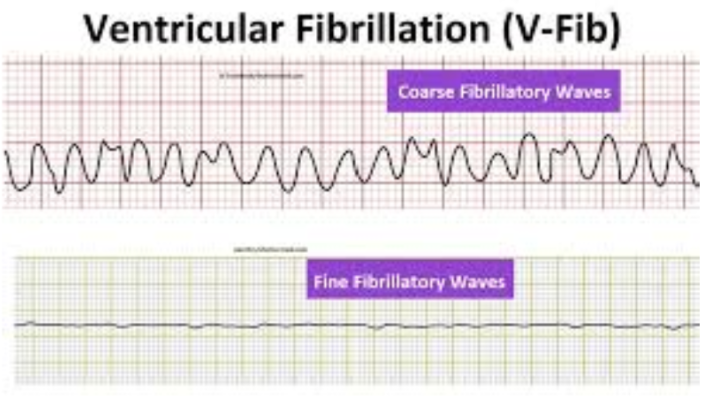
ventricular fibrillation
Completely abnormal
No rhythm
Coarse or fine:
sinus tachycardia causes
exercise, pain, anxiety
shock (hypovolaemic, septic, cardiogenic)
pulmonary embolism
anaphylaxis
fever/infection
heart failure
drugs (salbutamol, stimulants)
sinus bradycardia causes
inferior myocardial infarction
increased vagal tone
drugs (beta-blockers, digoxin)
hypothermia
atrial fibrillation causes
hypertension
ischaemic heart disease
mitral valve disease
hyperthyroidism
infection/sepsis
ventricular fibrillation
myocardial infarction
severe electrolyte disturbance
cardiomyopathy
cardiac arrest