ob4: care of women w complications during labor
1/68
Earn XP
Description and Tags
chap 9 & 10
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
69 Terms
induction
starting the labor
must confirm fetal maturity
Bishop Scoring System: considers factors of cervix & position of baby
augmentation
stimulating contractions
why would labor induction be done?
gestational HTN
ruptured membrane w/o onset of labor → infection
uterus infection
placental insufficiency
incompatible blood type → rH factor
prolonged pregnancy
fetal death
etc medical problems
why wouldn’t a labor induction be done?
placenta previa → c section
umbilical cord prolapse → need c section
abnormal fetal presentation → c section
high station of fetus → c section
active herpes → c section
abnormal structure of pelvis → c section
previous vertical c section → c section
non-pharm methods to stimulate contractions
walking
nipple stimulation (pituitary gland secretes oxytocin)
hot shower
acupuncture / acupressure
sexual stimulation
pharm methods to stimulate contractions
cervical ripening w/ cervidil, prostaglandin
oxytocin: augmentation (and helps stop bleeding after birth)
monitor fetal hr & contractions after administering oxytocin
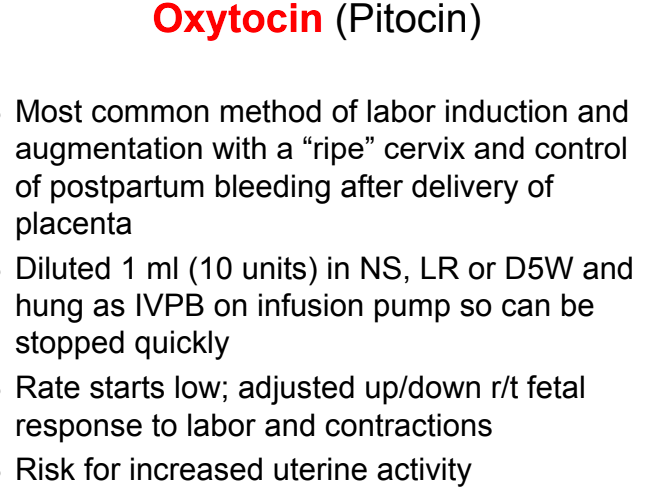
complications w oxytocin
oxytocin can cause contractions to be too intense → fetal compromise
& water intoxication
prepping the woman
explain procedure
obtain baseline, vitals, fetal HR
IV in place
remain in bed for 2hr
oxytocin 6-12 hr after insert removed
assess for uterine tachysystole
dilating the cervix
with cervidil, prostaglandin
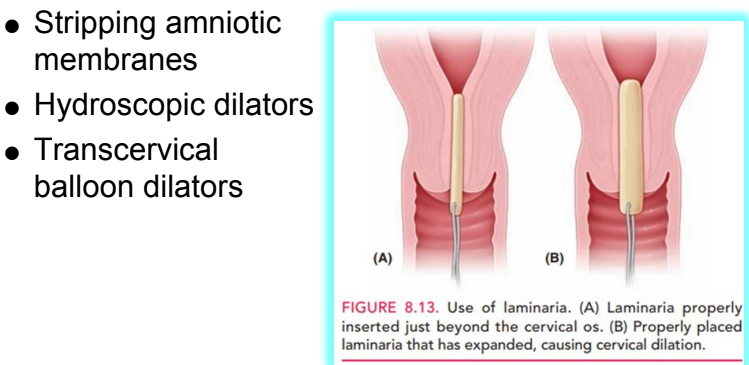
stripping amniotic membranes
hydroscopic dilators: placed lower uterine segment. mechanically swells to open
trans-cervical balloon dilator: like foley. insert & inflate balloon
amniotomy
artificial rupture of membranes - to stimulate/ enhance contractions
commits to delivery
stimulates prostaglandin secretion
complications: prolapse of umbilical cord, infection, abruptio placentae
abruptio placentae
s&s: abdominal/back pain, vaginal bleeding, low bp
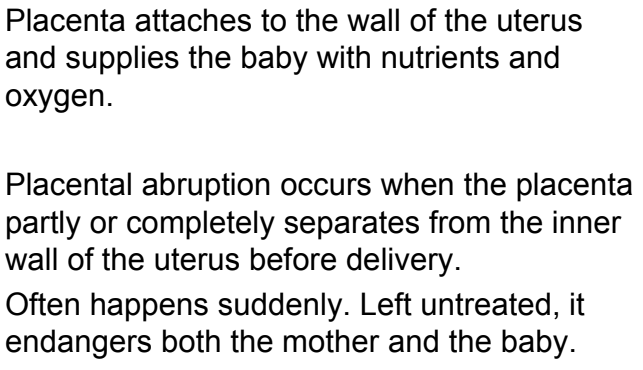
amnioinfusion
compression for umbilical cord
reduction of variable decels
dilution of meconium stained amniotic fluid
version
method used to change fetal presentation
before: determine: herpes previous vertical c-section. abnormal placental placement. disproportional uterine/pelvic size. twins
slow contractions with: tocolytics (ex: mg)
external: perfect at 37 weeks, but before onset of labor. ultrasound, clockwise.
internal: emergency, during labor.
episiotomy
surgical enlargement of perineum - prevent tearing/ if baby too big
numbing: pudenal block
alternative: perineal massage & stretching exercises before
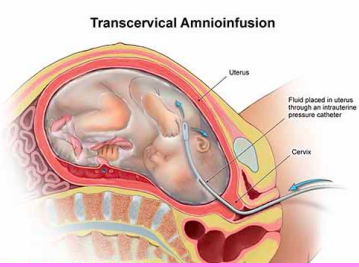
perineal lacerations
1st degree: superficial vaginal mucosa / perineal skin
2nd: vaginal mucosa, perineal skin, & deeper tissues
3rd: same as 2nd + anal sphincter
4th: extends through anal sphincter into rectal mucosa
care for episiotomy / laceration
1st: cold packs to reduce bruising & edema
after 12-24hr: heat & sitz baths
motrin & tylenol
monitor sister for infection
clean w: peri bottle, witch hazel
give stool softener to avoid straining
forceps extraction
traction & rotation of fetal head when mother can no longer push
done at 2nd stage - 10cm dilated
may be used during c-section
risk of injury to baby
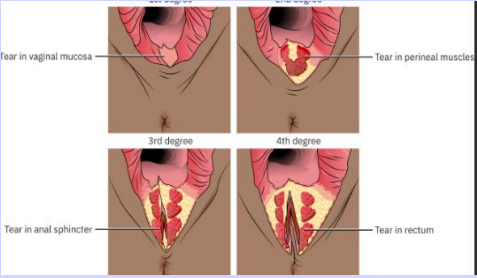
vacuum extracted birth
suction applied to baby’s head to assist expulsion
baby needs to be far enough along birth canal
only if occiput presentation (back of head facing vagina)
baby may render cephalic hematoma / bruising (chignon)
fetal maturity
ability to survive outside uterus - assessed by amniotic fluid analysis: L/S Ratio
surfactant needed for oxygenation
2:1 ratio
3:1 ratio: for diabetics
prep for c-section
lab to identify anemia / blood-clotting abnormalities
cbc, blood type
baseline vitals & FHR
IV & hep lock
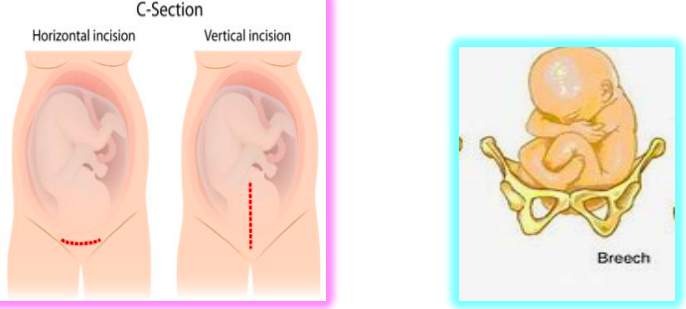
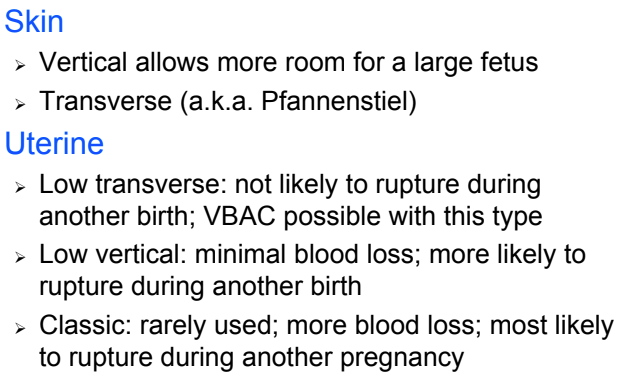
types of incisions
c-section
nursing care in recovery room
monitor vitals q5min for 1st hour (identify hemorrhage or shock)
check fundus for firmness, midline
assess drainage → circle it to see if it gets bigger
assess lochia (discharge)
monitor I&O → uterine will not contract/be firm if bladder is full
abnormal / dysfunctional labor
dystocia: difficult labor
risk: advanced maternal age, over-distended uterus. abnormal presentation
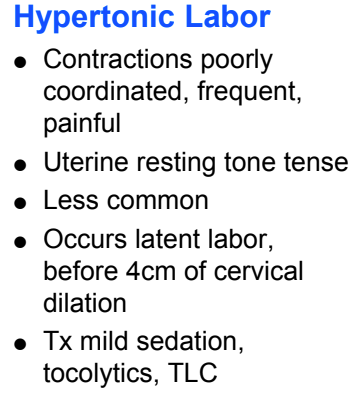
problems with powers of labor
hypertonic
problems with powers of labor
hypotonic
nursing care for abnormal fetal presentation
LOP or ROP positioning: most common cause
multi-fetal pregnancy dyfunctional labor
effects of hormones release
uterus uses more glucose for energy
diverts blood from uterus
can increase tension of pelvic muscles, interfering w/ descent
can increase pain perception
can promote relaxation
abnormal duration of labor
can cause post-partum hemorrhage
precipitated birth
completed in less than 3 hours
frequent, intense contractions → may lead to fetal compromise
may have uterine rupture, cervical lacerations, hematoma
fast labor → may cause baby injury ex intracranial hemorrhage
premature rupture of membranes
more than 1 hour before labor contractions begin
signs of impeding preterm labor
shortened cervix on ultrasound at 20 weeks
dx: cervical effacement & dilation 2cm+
presense of fibronectin at 22-24 weeks
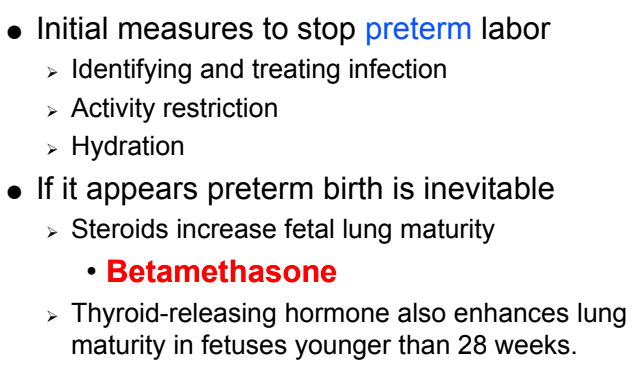
how to stop preterm impending labor
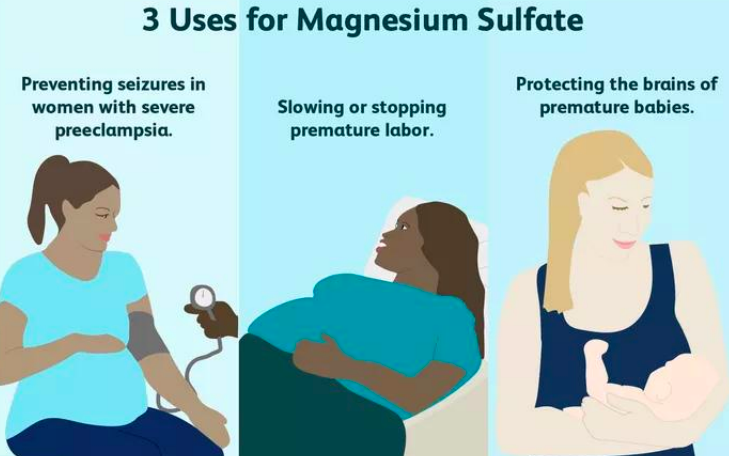
tocolytic therapy
goal: stop contractions - keep fetus in utero until lungs are mature
tx: mg IV, beta blockers po, calcium channel blockers po, postaglandin inhibitor
stopping preterm labor
contradictions of tocolytic therapy
education for woman w/ infection or preterm labor
report temp above 100.4
avoid sex & orgasms
avoid breast stimulation
note any contractions, reduced fetal activity (report <10 kicks in 12hr)
DES: estrogen used to treat vaginal cancer
prolonged pregnancy
longer than 41 weeks
placenta may become insufficient & baby becomes bigger
meconium may be expelled → respiratory distress
hypoglycemia → jittery, irritable, poor feeding, difficulty thermoregulation
tests to diagnosis prolonged pregnancy
prolapsed umbilical cord
complete, palpated, occult
occult: cannot be seen/ felt → detected because of decels
tx: c section
placenta accreta
abnormal placenta attachment (covering the cervix)
s: profuse bleeding
tx: blood transfusion & fluids → c section
uterine rupture
uterine wall tears → baby slips into abdomen
causes severe bleeding in the mother, sufficating baby
amniotic fluid embolism
amniotic fluids (w vernix, meconium, fetal hair) enters circulation & obstructs vessels in lungs
s: abrupt hypotension, respiratory distress, coagulation abnormalities, chest pain, crackles/wheezing
tx: intubation, ventilation, monitor I&O
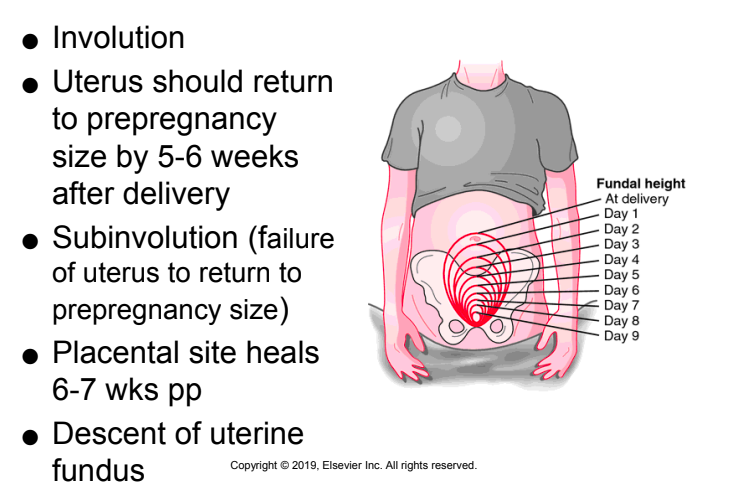
post-partum changes
uterus
involution: uterus returning to regular size 5-6 weeks post - 1cm descent per day
will experience post uterine-contractions. common w breastfeeding
placental site heals 6-7 weeks post
lochia / discharge
rubia: lasts 3 days
serosa: 3rd - 10th day
alba: clear, mucus like. 3rd - 10th day
less lochia w c-section
absence is abnormal!
perineum: watch for - REEDA (redness, edema, ecchymosis, discharge, approximation)
what should you do if uterus is flaccid/ boggy post?
massage & see if woman needs to use bathroom
med used to stop heavy bleeding post?
methylergonovine - IM or PO
tips w breast feeding
continue breast feeding & switch breasts
prevent mastitis
nursing care post birth
how long after birth can you begin ovulating post birth?
3 weeks
around 6 weeks if breast feeding
cardiovascular changes post birth
diuresis: increased urinary output - 3000 cc/day
diaphoresis
bradycardia (50-60 bpm first 48hr)
edema in feet & hands (due to iv fluids)
coagulation & blood value changes post birth
chills & orthostatic hypotension post birth
immune system changes post birth
Rh- mother needs: Rhogam within 72hr
Rubella vaccine: avoid pregnancy 3 months post-vacc
etc changes post birth
Edinburgh Postnatal Depression Scale
max scale 30
possible depression: 10 or greater
post birth is aka
perinatal
neonatal transition to life
phase 1: reactivity. 0-30 min post
phase 2: decreased responsiveness. 30min - 2hr post
phase 3: 2nd reactivity. 2hr - 8hr post
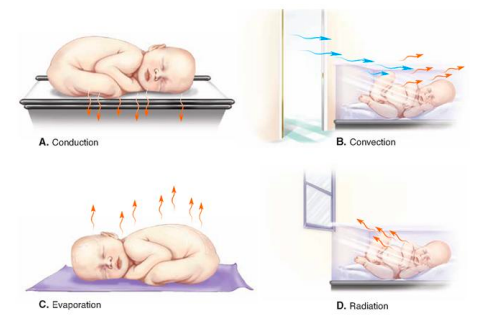
prevent heat loss in newborns
identifying maturity in newborn
skin
if vernix stays on → pre-term
lanugo all over → pre-term (black babies usually have more)
genitalia undeveloped / labia majora & minora equal size
how do you take temperature in newborn?
axillary
normal vitals for newborn
110 - 160 beats pm
30 - 60 breaths pm
bp: 65 - 95 / 30 - 60
risk for neonatal hypoglycemia
pre-term & post-term at risk. less than 5lb & more than 9lb. moms that have gestational diabetes
< 45 indicated hypoglycemia
hypoglycemic signs: jitterness, lethargic, low temp, respiratory difficulty, sweating, high-pitch cry, seizure
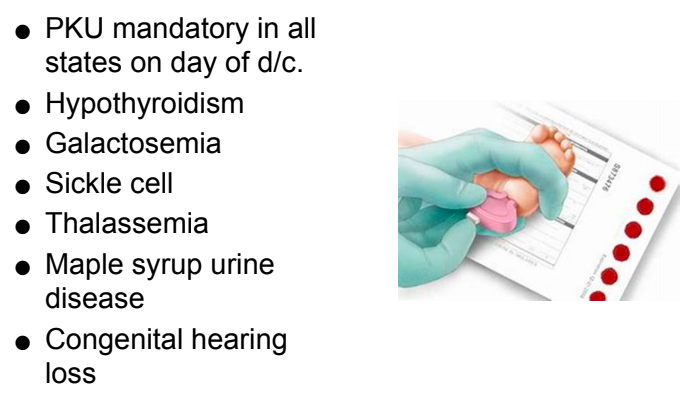
screening tests
if circles merge, test is invalid
skin care + bonding & attachment
do not wait until baby cries to feed → watch for cues
calling infant by name
holding infant face-to-face, skin-to-skin
talking genty
benefits of breastfeed
maintains temp bc skin to skin
uterus returns to normal size faster
will loose weight faster
antibodies for baby
evaluating intake of infant
recognizing hunger in newborns
storing & freezing breast milk
how often should one breastfeed if using formula: q3 - 4hr
room temp milk should not be left un-refrigerated for more than 3hrs
can be left in fridge for 24hr & freezer up to 3 months
newborn discharge care