Exam 1: L2 Approach to Anemia
1/171
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
172 Terms
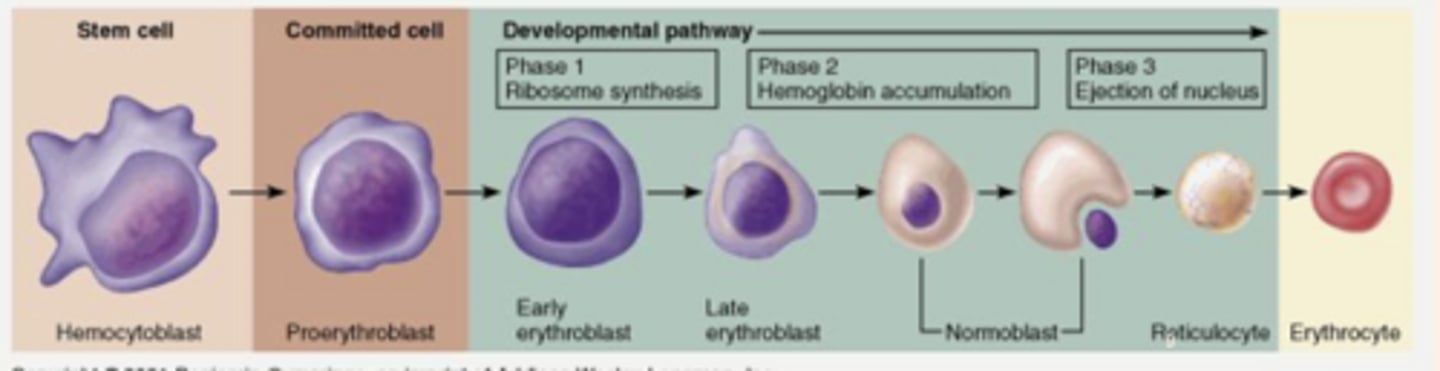
the normal production of RBCs
Erythropoiesis
Erythropoiesis =
________ delivery --> _____ stimulation --> RBC _____________ and _____________ --> ______________ release
low O2 delivery --> EPO stimulation --> RBC proliferation and maturation --> reticulocyte release
in the process of Erythropoiesis stem cells first turn into...
proerythroblasts
what happens during Erythropoiesis while the cell is in the proerythroblast stage?
EPO binds to marrow erythroid precursors (proerythroblasts) inducing cell maturation
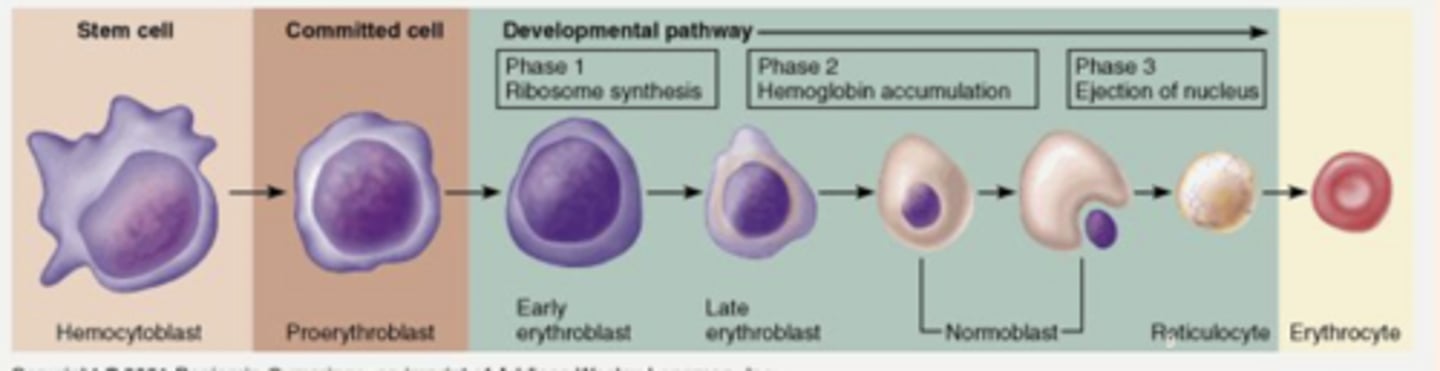
what happens during Erythropoiesis while the cell is in the early and late erythroblast stages?
folate and vitamin B12 assist in proliferation of the erythroblasts
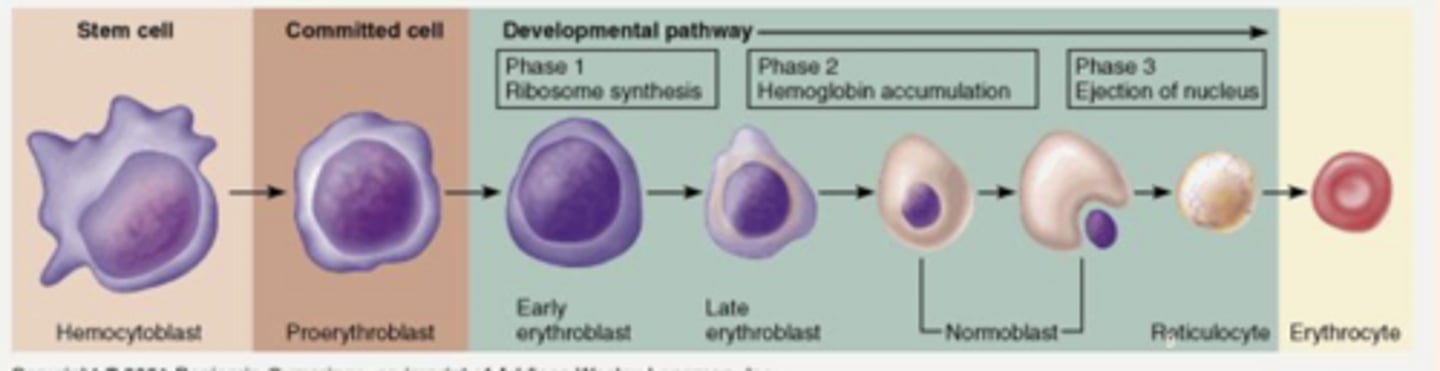
what happens during Erythropoiesis as the cell goes from late erythroblast --> normoblast?
Iron assists in the accumulation of hemoglobin.
It is the iron molecule that binds O2 to hgb
where does the Erythropoietin (EPO) come from?
kidenys
EPO binds to marrow erythroid precursors called ____________ inducing cell maturation
Proerythroblasts
Folate and Vitamin B12 assist in the proliferation of ______________
erythroblasts
Iron assists in the accumulation of ____________
hemoglobin
what binds O2 to hgb
iron
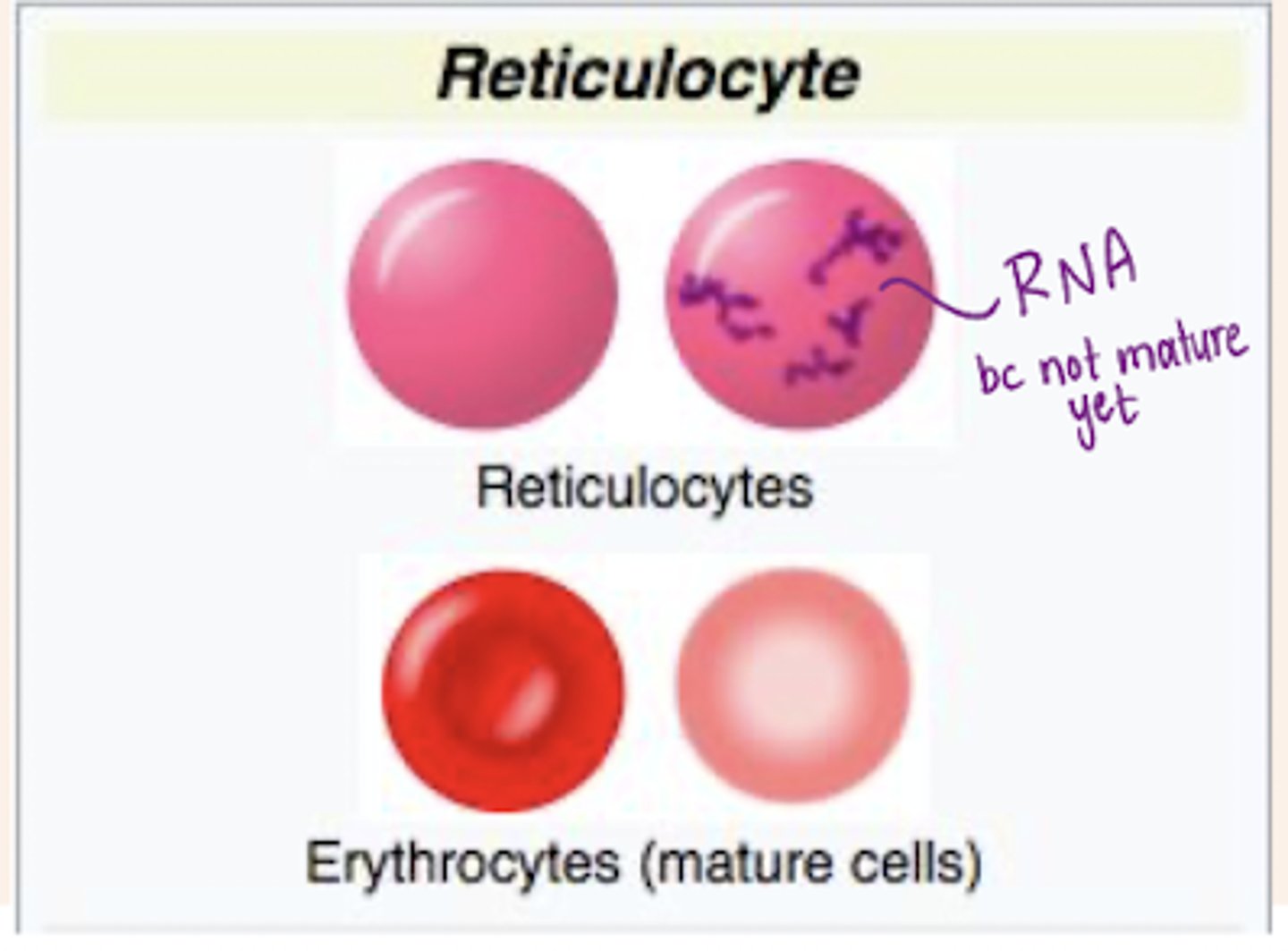
What is a reticulocyte?
It is an immature red blood cell (RBC).
How does a reticulocyte differ in shape from a mature RBC?
- not biconcave like a mature RBC
- slightly bluer than RBCs
- larger than RBC
What does a reticulocyte contain that is not present in mature RBCs?
It contains RNA, RNA is absorbed before maturing to a RBC.
What is the total lifespan of a reticulocyte?
4-5 days.
How long does a reticulocyte spend in the bone marrow?
3 days.
How long does a reticulocyte spend in the blood?
1-2 days.
What is the normal reticulocyte count range?
0.5-1.5%.
if you are losing blood will you have more or less reticulocytes?
more because your body is trying to make more RBCs fast
what are the 3 optimal conditions for Erythropoiesis?
- normal EPO production
- normal erythroid marrow function
- adequate Hgb accumulation
what is the end result if any of the physiologic processes needed for Erythropoiesis become defective?
decreased RBC production or faulty RBC production
what is Anemia?
the reduction of one or more of the major RBC measurements (Hgb, HCT, or RBC)
Kinetic Approach to Anemia
addresses the mechanism responsible for the fall in hgb concentration
Morphologic approach to anemia
categorizes anemias based on alterations in RBC characteristics and the reticulocyte response
according to the kinetic approach, anemia can be caused by one or more of the following three mechanisms:
- decreased RBC production (reduced erythropoiesis)
- increased RBC destruction (hemolysis)
- acute or chronic blood loss
under normal, healthy, steady conditions; the RBC production is directly related to RBC _______________
destruction
under normal, healthy, steady conditions; the average daily RBC production = ____% of red cell mass
1%
according to the kinetic approach, the lack of nutrients such as _____, _____, and _________ can decrease RBC production
iron, B12, folate
examples of bone marrow disorders that reduce RBC precursors leading to decreased RBC production?
aplastic anemia, pure RBC aplasia, myelodysplastic syndromes, tumor infiltration
what can cause bone marrow suppression reducing RBC precursors leading to decreased RBC production?
drugs, chemo, irradiation
low levels of __________ hormones decrease stimulation of RBC production
trophic hormones
ex: EPO (chronic renal failure, thyroid hormone (hypothyroidism), and androgens (hypogonadism)
Acute/chronic ______________ affects iron concentration, reduces EPO and decreases RBC life span leading to decreased RBC production
inflammation
according to the kinetic approach to anemia, that are the three main things leading to increased RBC destruction?
- inherited hemolytic anemias
- acquired hemolytic anemias
- hypersplenism (enlarged spleen)
what are some examples of inherited hemolytic anemias?
hereditary spherocytosis, sickle cell disease, thalassemia major
what are some examples of acquired hemolytic anemias?
Coombs'-positive autoimmune hemolytic anemia, thrombotic thrombocytopenic purpura (TPP), malaria, paroxysmal nucturnal hemoglobinuria
how does hypersplenism (enlarged spleen) lead to increased RBC production?
it leads to a compensatory feedback loop where the bone marrow works overtime to replace cells removed by the spleen since there is more SA in the spleen with more RBCs in the spleen and less RBCs doing their jobs so the bone marrow gets triggered to release more
what is the most common cause of anemia?
blood loss
what are 4 ways we can lose blood?
- gross blood loss
- occult blood loss
- latrogenic blood loss
- underappreciated menstrual blood loss
what can cause gross blood loss?
trauma, surgery, melena, hematemesis, severe menometrorrhagia
what can cause occult blood loss?
slowly bleeding ulcer or carcinoma
what can cause Iatrogenic (HA) blood loss
repeated diagnostic testing, hemodialysis losses, excessive blood donation
in addition to loss of RBCs with persistent bleeding, ________ deficiency occurs which further worsens anemia
iron
with blood loss / hemorrhage would the reticulocyte count increase of decrease?
increase
with decreased RBC production would the reticulocyte count increase of decrease?
decrease
with increased RBC destruction would the reticulocyte count increase of decrease?
increase
the morphologic approach to anemia included classifying anemia based on RBC ________ such as _______, _______, and ______
based on RBC indices such as MCV (size), MCH (hgb/color), MCHC
MCV =
mean corpuscular volume
average volume of RBCs
MCH =
mean corpuscular hemoglobin
MCHC =
mean corpuscular hemoglobin concentration
what are the anemias associated with a high/low MCV?
microcytic, macrocytic, normocytic
reticulocytes are (larger/smaller) than a mature RBC, therefore reticulocytosis will result in a (high/low) MCV
reticulocytes are larger than a mature RBC, therefore reticulocytosis will result in a high MCV
what are the anemias associated with a high/low/norm MCH?
hypochromic, hyperchromic, normochromic
what is the MCV level of macrocytic anemia
<100 fL
5 causes of macrocytic anemia
- folate and B12 deficiency
- medications that interfere with nucleic acid synthesis (lack of intracellular RNA deradation)
- abnormal RBC maturation
- alcohol abuse
- liver disease
how can folate and B12 deficiency lead to macrocytic anemia?
prevents adequate proliferation of erythroblast resulting in abnormally large RBC
what are two drugs that interfere with nucleic acid synthesis leading to macrocytic anemia?
zidovudine and hydroxyurea
what can cause abnormal RBC maturation and lead to macrocytic anemia?
myelodysplastic syndrome, acute leukemia
how does alcohol abuse lead to macrocytic anemia?
results in a folate deficiency
how does liver disease lead to macrocytic anemia?
results in lipid deposits on RBC increasing surface area
what are the MCV levels for microcytic anemia?
<80 fL
microcytic anemia is often associated with low _________ due to a decrease in _____ content in the small RBC
microcytic anemia is often associated with low MCH due to a decrease in hgb content in the small RBC
most common causes of microcytic anemia (2):
- iron deficiency
- alpha or beta thalassemia minor
MCV levels of normocytic anemia
between 80 and 100 fL
normocytic anemia often required evaluation by a ___________ ________
peripheral smear
causes of normocytic anemia include:
- chronic kidney disease
- anemia of chronic disease/inflamation
- mild iatrogenic "hospital" anemia
how does mild iatrogenic "hospital" anemia occur?
recurrent venipuncture, blood loss from surgery, hemodilution with IV fluids, blunted erythropoiesis due to acute illness
true or false: anemia alone is not a diagnosis but merely a sign of an underlying condition
true
what is the primary function of RBCs?
delivering oxygen to tissues
what is the physiologic effect of a lack of RBCs?
tissue hypoxia with a compensatory response
physiology of anemic symptoms is directly related to decreased ___________ delivery to tissues
oxygen
symptoms reflect a fall in hgb concentration, in both ______ and ________
severity and speed
acute, moderate-severe blood loss will cause?
hypovolemia and a more severe clinical presentation of anemia
what are the two main ways the body compensated for anemia?
- increase in oxygen extraction, maintains normal oxygen delivery until Hgb reaches 8-9 g/dL
- increase in stroke volume (SV) and heart rate (HR)
while compensating for anemia the body maintains normal oxygen delivery until...
Hgb reaches 8-9 g/dL
What percentage of oxygen do tissues extract from hemoglobin in a steady state?
25%
What can anemia or hypoperfusion increase oxygen extraction from hemoglobin up to?
60% (maximum)
What happens to stroke volume (SV) and heart rate (HR) in response to anemia?
They increase to compensate for anemia.
What does the increase in stroke volume and heart rate maintain?
O2 delivery at rest.
At what hemoglobin level does O2 delivery become compromised in a healthy heart without hypovolemia?
When hemoglobin falls below 5 g/dL.
anemia symptoms occurring at rest indicate a lower ________ or the heart's inability to ___________
anemia symptoms occurring at rest indicate a lower H&H (hgb and HCT) or the heart's inability to compensate
common signs and symptoms of anemia
varying degrees of fatigue
-unusual exertional tachycardia/dyspnea
- tachycardia/dyspnea at rest
- palpitations
- auditory pulsations
- bounding pulses
- pallor
s/s of anemia complicated by volume loss
- easy fatigability
- muscle cramps
- dizziness/syncope
- lethargy
- progressive hypotension/shock/death
true or false: anemia is never normal
true, the etiology should always be sought
what are the four questions you should ask yourself if you suspect anemia?
1. is the patient bleeding (past or present)? if so where?
2. is there evidence of increased RBC destruction (intravascular or extravascular)?
3. is there bone marrow suppression? if so why?
4. is the patient nutrient deficient in iron, folate, or B12? if so, why?
What is the first question to ask if you suspect anemia?
Is the patient bleeding (past or present)? If so, where?
What is the second question to ask if you suspect anemia?
Is there evidence of increased RBC destruction (intravascular or extravascular)?
What is the third question to ask if you suspect anemia?
Is there bone marrow suppression? If so, why?
What is the fourth question to ask if you suspect anemia?
Is the patient nutrient deficient in iron, folate, or B12? If so, why?
when evaluating for anemia what should your history be geared toward?
ruling in/out your etiologic differential diagnosis (Ddx)
what are the three ways to evaluate the onset of anemia symptoms?
- New onset most often related to an acquired d/o
- Life long anemia w/wo family history is likely inherited
- Compare recent to remote H&H/RBC indices
constitutional signs of malignancy
Recent unintentional weight loss, loss of appetite, fever, night sweats
Symptoms of or hx of medical condition associated with anemia
- Melena - Upper GI bleed, bleeding ulcer
- Large hematochezia - Lower acute GI bleed
- Menorrhagia - Dysfunctional uterine bleeding
- Renal failure
- Rheumatoid arthritis
- CHF
What is melena associated with?
Upper GI bleed, bleeding ulcer
What does large hematochezia indicate?
Lower acute GI bleed
What is menorrhagia?
Dysfunctional uterine bleeding
Which autoimmune condition is associated with anemia?
Rheumatoid arthritis
What heart condition is associated with anemia?
Congestive heart failure (CHF)
when approaching anemia with patient history, in addition to medical condition history you should consider _____________, __________ and _______ histroy as well as __________ use
ethnicity, family and social history as well as medication use
what substances/medications should be evaluating in regards to anemia
- EtOH
- ASA, NSAIDS, blodo thinners
physical exam findings in Anemia - skin
- pallor
- jaundice
- petechiae
- bruising