Central Nervous System Infections
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
what are the 2 integral parts of infections for rabies
needs to get from bite site to salivary glands
needs to change behavior of animal
what is some general information about CNS homeostasis
non-renewable cells → highly metabolically active
solutes & waste products
CNS is physically separated from the body by
blood-brain barrier → selective regulated exchange
blood cerebrospinal fluid barrier
prevents effects of the body spreading to brain
what can CNS infections result in
meningitis → inflammation of meninges
e.g. bacterial, fungal
encephalitis → inflammation of brain tissue/parenchyma
e.g. viral, parasite
what is mechanical protection of the brain
bone & CSF
meninges - containing CSF
vertebral column protects spinal cord
what kind of contents can cross the BBB & BCSFB
signaling, nutrients, metabolites, blood vessels & nerves
what are the major routes for infection
blood vessels → major route of CNS infection
peripheral nerves
invasion via ears/sinuses & olfactory tract
penetrating injury/surgery
what are some layer protecting the CNS
hair, skin, bone, meninge (3 layers), brain tissue
subarachnoid space → contains CSF
located between arachnoid & pia mater
CSF → produced by choroid plexus
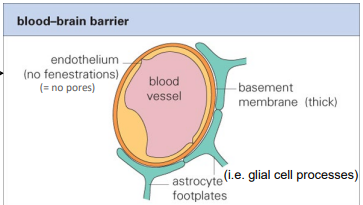
describe the BBB
tight junctions between capillary endothelial cells
thick basement membrane
astrocytes surrounding capillaries
no fenestrations (pores)
infection = encephalitis
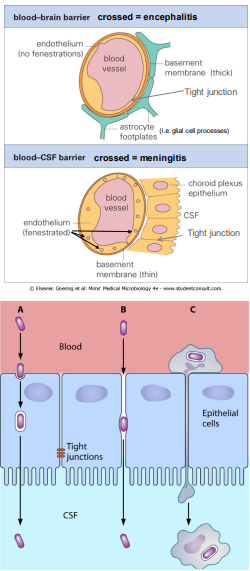
describe the BCSFB
endothelial cells of capillary
basement membrane → thinner than BBB
tight junctions between choroid plexus ependymal (epithelium) cells → looser junction than BBB
infection = meningitis
how can microorganisms cross the BBB/BCSFB
transcellular
infection → growing across ECs
passive transport via endocytosis
pericellular
transport between cells (if junctions weaken by inflammation)
trojan horse
inflammation allows infected WBCs to enter CNS
describe how microorganisms infect via peripheral nerves
enter via muscle or directly from peripheral nerves
travels towards CNS then to brain
facilitated by cytoskeleton & dynein (moves cargo towards CNS)
describe other methods of CNS invasion
via olfactory tract
nasal tract → olfactory tract → meningitis/encephalitis
via sinuses or middle/inner ear
infection tissue damage
direct inoculation
shunts, head wounds
describe the normal CNS immunity
protected by macrophages (meninges) & microglia (brain parenchyma)
fewer immune cells than other tissues
small number of T cells for surveillance
describe CNS during invasion
macrophages activate T cells
pro-inflammatory cytokines released
loosen tight junctions, recruit more immune cells
loose junction can compromise BBB/BCSFB
what are some side effects of immune response in CNS
swelling in brain
damage to nerves (irreparable)
low blood pressure
potential autoimmunity
how is the CNS monitored for infection
lumbar puncture → testing CSF for microbes
why might CSF appear cloudy
due to the presence of fungi or bacteria
fungi = rare
what are the clinical presentations of acute bacterial meningitis
fever
stiff neck
altered mental status
headache
how is acute meningitis diagnosed
history of patient
knowledge of current illness, vaccines
physical examination
blood culture
CSF EXAMINATION
what are the 3 main bacteria responsible for bacterial meningitis
Hemophilus influenzae
Streptococcus pneumoniae
Neisseria meningitidis
what is some information about Neisseria meningitidis
-gram (CSF) diplococcus bacterium
expresses lipopolysaccharides → inflam. response
thick capsule → prevent phagocytosis (blood survival)
untreated = septic shock
transmission = droplets
vaccines don’t protect against every serogroup
what is some information about Streptococcus pneumoniae
+gram coccus shaped bacterium
thick capsule → prevent phagocytosis (blood survival)
carried in throats of many healthy patients
invasion of blood & meninges is rare
what is some information about hemophilus influenzae
-gram non/capsulated coccobacillus bacteria
expresses LPS → large inflammatory response
healthy people may carry non-capsule type in throat
rarely enters blood & meninges
describe the treatment for bacterial meningitis
3rd generation [broad spectrum] cephalosporin
often dexamethasone for reduced inflam. response
switch following species identification & testing
describe TB meningitis
gradual onset → develops over several weeks
symptoms: malaise, anorexia, neck stiffness
always a focus of infection elsewhere (e.g. lungs)
CSF = clear but ↑protein, ↓glucose, ↑WBCs
treatment needs to be fast to prevent serious issues
describe fungal meningitis
primary infection site = lungs → blood → meningitis
low birth weight babies → suppressed cell-mediated immunity
major cause: cryptococcus neoformans
describe protozoal meningitis/encephalitis
rapid onset, usually fatal
amoeba enters nose, olfactory tract → meningitis
can infect healthy individuals
describe viral meningitis
milder disease than bacterial meningitis
symptoms: headache, fever, photophobia
CSF = aseptic (non-bacterial meningitis)
PCT testing
usually recover without drugs (rest & support)
what are some common effects of encephalitis
cerebral dysfunction - abnormal behavior, seizures
focal neurological effects - loss of sensation, muscle weakness, partial paralysis
altered consciousness - hallucinations
describe the general pathogenesis of bloodborne viruses
viruses commonly access the CNS via the blood
leaves blood via BBB → infects glial cells
causes damage/dysfunction
immune response
monocytes & lymphocytes go from blood to brain
can clear infection but also cause immune pathology
what are some clinical features of viral encephalitis
fever & headache
seizures depending on region of brain
alter conscious state - “acting funny” to coma
focal neurological signs - depends on affected brain regions
describe the management for viral encephalitis
immediate treatment
HSV therapy
restricting fluids to lower pressure in brain
anti-seizure medication
describe herpes simplex virus
primary infection → lesions or cold sores
enters sensory nerves, travels to dorsal root ganglion or trigeminal ganglion
can be reactivated by stress or illness
ganglion typically returns to lesions, can travel to CNS leading to encephalitis
describe diagnosis & treatment of HSV using CSF
CSF may have ↑lymphocytes, RBCs
medical imaging can also find evidence of HSV
PCR of CSF can help identify HSV
treatment
prompt treatment with acyclovir before diagnosis confirmed
what are some clinical features of rabies
bite/scratch from animal
slow incubation → virus must reach peripheral nerves
no immunological response → hidden in nerves
virus spreads from peripheral nerves → CNS
what are the main symptoms of rabies
behavioral changes
flu-like symptoms
spasms, fits, hallucinations
coma, respiratory failure
death
how is rabies diagnosed
detect viral antigen by immunofluorescence/RT-PCR
skin biopsies, saliva or CSF
what is some information on HIV
retrovirus, may invade CNS after initial infection
↑WBCs in CSF
as disease progresses → subacute encephalitis with dementia may occur
describe post vaccinal/post infectious encephalitis
infection of CNS by “slow virus” years after infection
incomplete replication due to partial control by host
usually triggered by immune response to host & virus
what is spongiform encephalopathy
common pathology of prion diseases
appearance of gaps in brain tissue
misfolding of proteins
describe the parasite toxoplasma gondii
parasite ingested from sources like uncooked meat, contaminated water
can localize to brain → eye damage
what is clostridium tetani (tetanus)
bacteria that secrete a toxin that causes damage to CNS
toxin travels to CNS via retrograde transportation up motor neurons to CNS
overactive moto neurons → stimulate contraction pathway
rigid paralysis