Psychiatry Matrix
1/164
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
165 Terms
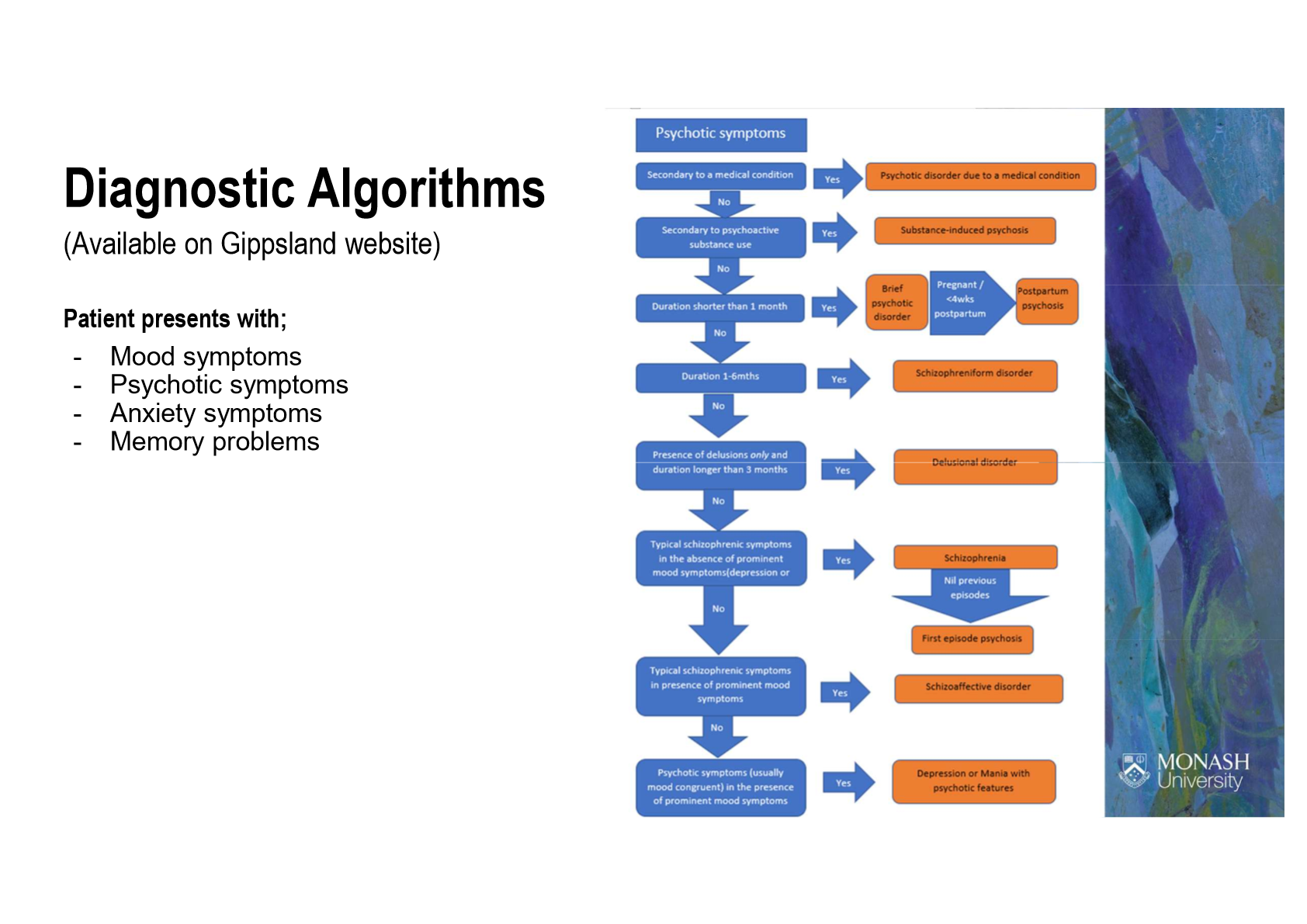
Psychosis
Impaired perception of reality through one or more of:
Hallucinations (sensory abnormalities w no stimuli)
Delusions (fixed false beliefs inconsistent to cultural/social norms)
Disorganised thinking, speech or behaviour
Primary Psychosis: results from psychiatric disorder (e.g. Schizophrenia)
Secondary Psychosis: results from general medical condition and/or the effect of a substance (inf., endocrine, neurological = stroke/tumour, autoimmune = SLE, B12 def.)
Psychotic Disorder: disease/condition producing psychosis
Schizophrenia Dx (R1)
Pos, Neg and Cognitive signs/sx of Psychosis persist for >6m, PLUS Social and Functional decline:
A) 2+ for >1m of:
1) Delusions, 2) Hallucinations, 3) Disorganised Speech
PLUS
4) Grossly Disorganised or Catatonic Behaviour, 5) Neg. Sx (dec. emotions)
B) Severe impact on function ability (work, care etc)
C) Duration persists >6m (Criteria A = >1m)
D) Ruled out Schizoaffective, Depressive or Bipolar
E) Ruled out attribution to effects of substances
RF: Genetics, Substances, Environmental/Psychosocial
Men = 18-25
Women = 25-35 (menarch) + >40 (menopause)
Late Onset Schizophrenia: >40-60, W>M, fewer neg. sx
Screening Tools:
PANSS (Pos + Neg Sx Scale)
BPRS (Bried Psychiatric Rating Scale)
Screen for organic cause (CRP, TSH, Urine)
MSE: A/B: poor, disorganised; M: abnorm; S: abnorm, delusions; C: low/distracted; R: __; I: impaired; J: impaired; P: hallucinations
Substance‑Induced Psychosis (R1)
Psychosis must be a direct consequence of substance USE or WITHDRAWAL
Sx development is related to the time the substance was last ingested, and sx duration is usually brief
Causes:
Recreational: Alcohol, Hallucinogens, Cocaine, Cannabis, Amphetamines
Medications: Analgesics (Opioids), Antihistamines, Sedatives/Hypnotics, Antidepressants (SSRIs), Benzo, Antiparkinsons (dopaminergics), Corticosteroids
Substance-Induced Psychotic Disorder: when sx outlast expected intoxication/withdrawal duration
However, >4wks indicates other psychotic disorder
Schizoaffective Disorder (R2)
Mix of Schizophrenia and Bipolar Disorder (Psychosis AND Mania) for >2wks
A) Period of either:
1) Major Depressive Eps
2) Manic Ep
3) Mixed Ep with Schizophrenia sx of Criteria A
B) Delusions or Hallucinations for >2wks in SAME period of illness as Criteria A WITHOUT Mood Sx
C) Sx of Mood Ep. for majority of illness period
D) Ruled out attribution to effects of substances
Schizophreniform Disorder (R2)
Schizophrenic sx/psychosis for a shorter duration of 1-6m
2/3 Pts develop Schizophrenia or Schizoaffective dis.
Criteria:
A) 2+ for >1m of:
1) Delusions
2) Hallucinations
3) Disorganised Speech
PLUS
4) Grossly Disorganised or Catatonic Behaviour
5) Neg. Sx (dec. emotions)
B) Severe impact on function ability (work, care etc)
C) Duration persists 1-6m
D) Ruled out Schizoaffective, Depressive or Bipolar
E) Ruled out attribution to effects of substances
Delusional Disorder (R3)
At least 1 delusion
No other prominent psychotic sx (hallucinations, disorganised speech, negative sx)
A) Nonbizarre delusions >1m (i.e., involving situations that occur in real life, such as being followed, poisoned, infected, loved at a distance, or deceived by spouse or lover, or having a disease)
B) Criterion A for Schizophrenia has never been met
C) Functioning/Behaviour not impaired apart from the ramifications of the particular delusion
D) Any assoc. Mood Eps. have been comparatively brief
E) Ruled out attribution to effects of substances
Nonbizzare Del: can be true +/or consistent w cultural/social norms
Bizzarre Del: canNOT be true +/or inconsistent w cultural/social norms
Grandiose Del: insists special powers/importance
Brief Psychotic Disorder/Episode (R3)
Psychosis for <1m
A) Presence of >1 of:
1) Delusions
2) Hallucinations
3) Disorganised Speech
4) Disorganised/Catatonic Behaviour
B) Duration is >1d BUT <1m with FULL functional return
C) Have Ruled out Mood Disorder With Psychotic Features, Schizoaffective Disorder, Schizophrenia or Substance Effects
RF: Stressful life event
Psychotic Disorders Mx
Screen for: past Dx of Psychosis, onset (sudden = 2°), head trauma, meds/drug hx, PMHx (Cushings, autoim, THYROID DISEASE!), Life Stressors, FHx
Ix: TFT, BMP, CBC, LFTs, ESR, ANA, Vit B12, Thiamine, HIV/Syphilis, Preg., Urine Tox, MRI/CT Head, EEG
Mx:
Psychosocial Intervs: better for neg/cog sx (CBTp)
Antipsychotic Medications:
1st Line:
SGAs: Aripiprazole, Risperidone, Olanzapine, Quetiapine
FGAs: Haloperidol, Chlorpromazine
Tx Resistant: Clozapine
Following failure of TWO different antipsychotics each for ≥ 6wks
Requires CBC for neutropenia risk monitoring
Must be titrated (cannot start/restart at full dose), abrupt cessation = rapid relapse
AEs = CONSTIPATION! → toxic megacolon (gastric hypomotility), myocard., Agranulocytosis (Severe Neutropenia → rare)
SGA > FGA
1st Gens (FGA) = dopamine receptors (muscular sx)
2nd Gens (SGA) = dopamine + serotonin (metabolic sx => monitor lipids, weight and BGLs)
Ari = young pts/ASD, acathesia (restlessness)
Risp = young pts/ASD, hyperprolactinaemia/galactorrhea
Olanz = weight gain/metabolic issues (O = wide)
Quet = sedating (Quet = Quiet)
Halo = Dystonia + NMS risk, EPSEs, hyperprolact., QT risk
Chlor = anticholinergic effects, photosens., HYPOtension
Bipolar I Disorder (R1)
Manic episodes >1wk OR causing hospitalisation NOT due to an organic/substance related cause
RF: FHx!!!, Age (18-30)
VERY High Risk of Suicide: Do Risk Assessment
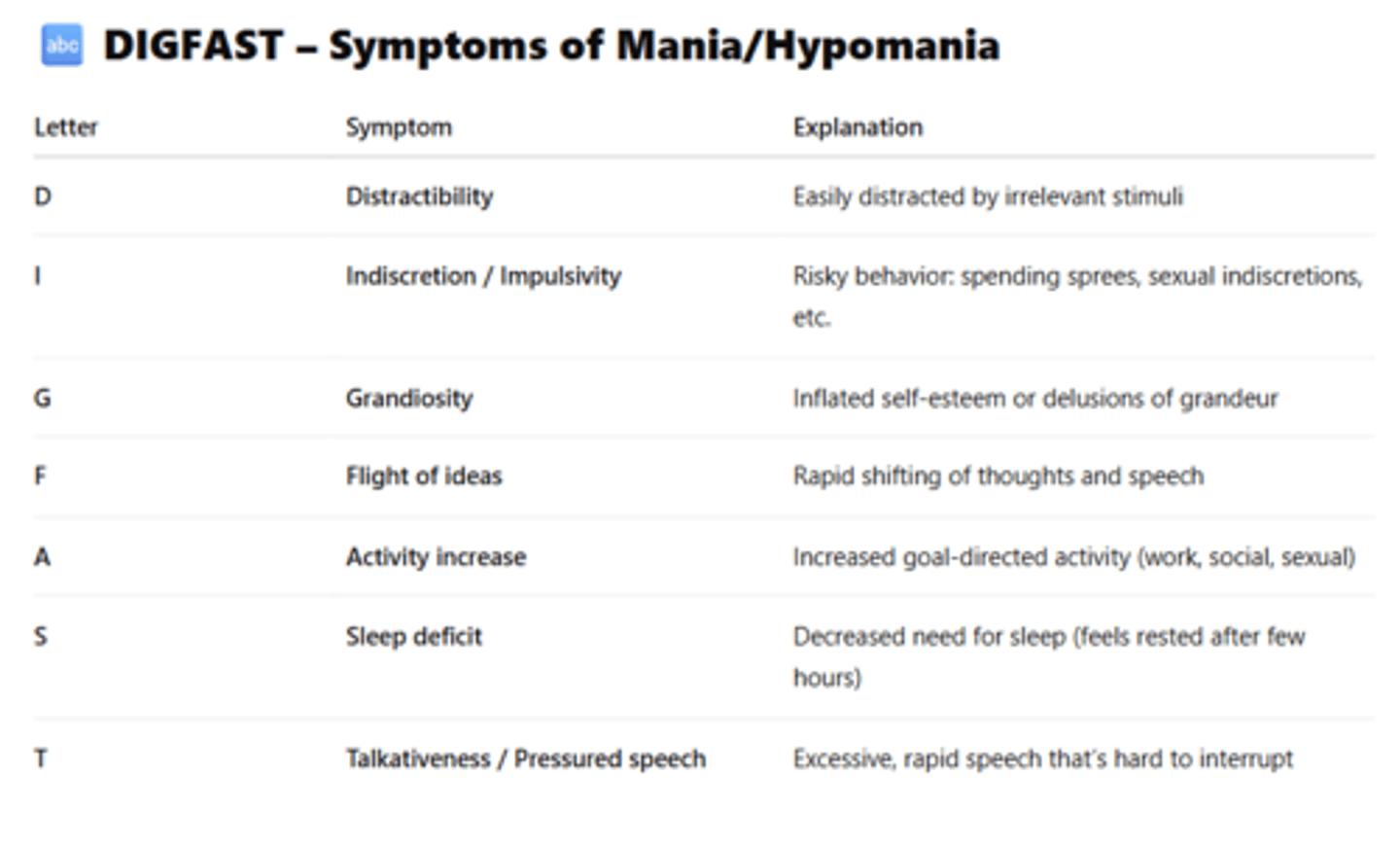
Manic Eps
Distinct periods of abnormally and persistently elevated, expansive, or irritable mood, PLUS abnormally and persistently increased energy or activity
3+ sx of DIGFAST:
Distractibility: attention draws easily to irrelevant stimuli
Impulsivity/High-Risk Behavior: excessive activities with painful consequences (e.g., buying sprees, sexual indiscretions)
Grandiosity: Inflated self-esteem
Flight of Ideas/Racing Thoughts
Activity Increase/Goal-Directed Activity: increased energy at work, school, or socially, +/- psychomotor agitation
Sleep Def/Decreased Sleep: feeling rested after only a few hours
Talkativeness: pressured speech
Bipolar II Disorder (R2)
Hypomanic (low levels of mania) >4d
PLUS
Major Depressive episode >2wks
WITHOUT
Full manic episode/Major functional impairment
Drug‑Induced Mania (R3)
Mania distinct from a primary bipolar disorder (non-substance-induced)
Sx preceding the substance use, or persisting for a SIGNIFICANT TIME (>1m) after cessation
Substance Abuse: Usually cocaine and amphetamines, can be caused by ETOH, cannabis, opioids etc
Medications: antiparkinsonian drugs, corticosteroids, thyroxine
Suspicious for pts with mania age >35yrs
Cyclothymic Disorder (R3)
Episodes of hypomania and depression that:
Do not meet the full DSM‑5 diagnostic criteria for hypomania or major depressive disorder
Present at least half the time during a 2‑year period with ≤ 2 months of symptom remission
Bipolar and Related Disorders Mx
Consider ceasing antidepressants which can cause mania, should only use (SSRIs preferred) WITH Mood Stabilisers
Address triggers (sleep dep,. substance use)
Electroconvulsive Therapy (ECT) for sev./med intolerant
Medications: Combination Therapy (1 + 2) for Mod-Sev.
Mood Stabilisers:
Lithium (1st line)
Valproate (Avoid in Preg.)
Lamotrigine (ONLY for depressive eps/depres-prominent)*
Antipsychotics: SGAs preferred (Aripip, Risp, Olanz, Quet)
Benzodiazepines: Lorazepam (for SHORT TERM and SEVERE: agitation, insomnia, behavioural disturbances)
Antidepressants: not usually used (may cause abnormal mood states/switching) but may be necessary for bipolar depression (Venlafaxine/strong antidepressants should be avoided)
Bipolar Depression: Quetiapine monotherapy, Lithium, Lamotrigine (more for prevention, slower onset), Lurasidone (often with lithium or valproate)
*Do NOT give high dose of Lamotrigine or Lam + Val due to high risk of SJS/TENS (skin burns)
Major Depressive Disorder (R1)
>5 sx from the 9 Sx Domains for >2wks including at least one of:
Depressed mood
Loss of interest or pleasure (anhedonia)
PLUS Functional Impact/Distress (Social, Occup. etc)
NOT attributable to a substance or medical condition
NO Hx of Mania/Hypomania Eps (rule out Bipolar)
The 9 symptom domains:
Depressed mood most of the day, nearly every day
Markedly reduced interest or pleasure in most activities
Significant weight loss or gain, or appetite change
Insomnia or hypersomnia
Psychomotor agitation or retardation (observable by others)
Fatigue or loss of energy
Feel worthless or excessive/inappropriate guilt
Reduced concentration or indecisiveness
Recurrent thoughts of death, suicidal ideation, or suicide attempt
Substance‑Induced Depressive Disorder (R3)
Clinically significant depressive syndrome that:
Develops during or soon after substance intoxication, withdrawal, or medication exposure
Is attributable to that substance
Is not better explained by a primary depressive disorder
Substance/Med is capable of causing depressive sx
E.g. ETOH, Opioids, Sedatives/Hypnotics, Stimulant Withdrawal, Other Prescribed Meds
Persistent Depressive Disorder/Dysthymia (R3)
Chronic depressive condition characterised by:
Depressed mood for most days for >2yrs
>1yr for children/adolescents (will be irritable > sad)
>2 additional depressive sx
No prolonged symptom‑free periods (not >2m)
No history of mania or hypomania
Disruptive Mood Dysregulation Disorder/DMDD (R3)
Childhood disorder characterised by severe, chronic irritability, rather than episodic mood elevation
A) Frequent Severe Temper Outbursts (Verbal/Behav)
B) Persistent Irritable Mood/Anger (close to 24/7)
C) Frequency of Temper Outbursts >3 times/wk
D) Duration >12m, No sx-free period >3m (consec.)
E) Sx in >2 settings (sev. in >1): home, school, w peers
F) Dx age only bw 6-18yrs (onset sx before 10yrs)
G) Exclusion of Mania/Not Better Explained by Another Dx/Disorder or Substances/Med. Condition
Disruptive mood dysregulation disorder is a childhood condition characterised by severe, recurrent temper outbursts and persistent irritability lasting at least 12 months across multiple settings, with onset before age 10 and no history of manic or hypomanic episodes
Depressive/Mood Disorders Mx
Antidepressants:
SSRIs
SNRIs/Other ()
SSRIs:
Sertriline: all-rounder, 1st line, min AEs,
Fluoxetine: min AEs, more activating than Sert (gives energy)
Generalised Anxiety Disorder/GAD (R1)
>6m of Excessive Worry about Everyday Issues that:
Is disproportionate to any inherent risk
Causes distress or impairment
Is hard to control
>3 sx are present most of the time: SICK FT
Sleep disturbance
Irritability
Concentration poor
Keyed Up/Restlessness or nervousness
Fatigued easily
Tension (in muscles)
Panic Disorder (R2)
Recurring unexpected panic attacks over >1m
Patient remains persistently concerned/anxious about having another attack
Not Due to Subs/Med Conds/Other Mental Disorders
At least one panic attack is followed by ≥1 month of one or both of:
Persistent concern/worry about panic attacks or their consequences
Persistent concern or worry about
Panic Attacks: sudden onset of intense physical and cognitive symptoms of anxiety that may be triggered by specific cues or occur unexpectedly
Agoraphobia (R2)
A) Marked fear or anxiety for >6m regarding >2 of:
Using public transport (e.g. buses, trains, planes)
Being in open spaces (e.g. car parks, marketplaces)
Being in enclosed spaces (e.g. shops, cinemas)
Standing in line or being in a crowd
Being outside the home alone
B) Reason for fear is hard to escape/get help
C) Situations are avoided/endured w distress/need a companion due to provoking fear/anxiety
D) Fear is out of proportion to posed danger
E) Functional Impairment (social, occupational etc)
F) Not better explained by another disorder
Can be diagnosed with/without panic disorder
Specific Phobias (R2)
Intense fears of SPECIFIC OBJECTS or SITUATIONS persistent for >6m that are triggered upon actual or anticipated exposure to phobic stimuli
Exposure to the phobic stimulus almost always provokes immediate fear or anxiety
Situations w phobic cues are avoided/endured with intense anxiety
Excessive fears can cause functional impairments or lifestyle disruptions and is out of proportion
Mx: Exposure Therapy/CBT, Benzos for infrequent sx
Anxiety Disorders Mx
First Line: SSRIs
Buspirone
Short-term mx of anxiety sx (not for panic attacks)
Obsessive‑Compulsive Disorder (R1)
Presence of one or both of:
Obsessions: recurrent/persistent thoughts, urges or images that are intrusive/unwanted causing anxiety or distress (attempt to ignore/neutralise)
Compulsions: repetitive behaviours/mental acts in response to an obsession aiming to prevent/reduce anxiety or distress that pt feels driven to perform
Obsessions/Compulsions are Time Consuming (>1hr/d) or cause distress/impaired functioning
Not better explained by sub./condition/disorder
Mx = Pharm + CBT/ERP
Body Dysmorphic Disorder/BDD (R3)
A) Preoccupation with appearance: >1 perceived flaws or defects not observable/apparent to others
B) Repetitive Behaviours/Mental Acts (skin pick etc)
C) Clinically Significant Distress or Impairment
D) Not Better Explained by an Eating Disorder
Muscle Dysmorphia Specifier: Preoccupation that the body is too small or insufficiently muscular (M > F)
Mx = Pharm + ERP
Hoarding Disorder (R3)
A) Persistent Difficulty Discarding Possessions (value regardless, perceived need to save items)
B) Accumulation/Clutter due to difficulty discarding
C) Clinically Significant Distress or Impairment
D) Not better explained by sub./condition/disorder
Mx = CBT
Trichotillomania (R3)
A) Recurrent pulling out of hair, resulting in hair loss
B) Repeated Attempts to Stop
C) Clinically Significant Distress or Impairment
D) Not better explained by sub./condition/disorder
Mx = HRT
Excoriation Disorder (R3)
A) Recurrent skin picking, resulting in skin lesions
B) Repeated Attempts to Stop
C) Clinically Significant Distress or Impairment
D) Not better explained by sub./condition/disorder
Mx = Pharm + HRT
Obsessive‑Compulsive & Related Disorders Mx
Non-Pharm: CBT/ERP!/HRT
Pharm: SSRIs +/- Tricyclic Antis (Clomipramine)
Do not give citalopram to BDD
Clomipramine: Seratonin-Specific, Less Tolerated than SSRIs
ERP (Exp + Response Prev): systematic exposure to feared stimuli while preventing compulsive behaviours to reduce anxiety
HRT (Habit Revers Train): identifies triggers and substitutes behaviors
Post Traumatic Stress Disorder - PTSD (R1)
All 4 Groups of sx for >1m following exp. to trauma:
Intrusion symptoms ≥1 (memories, reactions, etc)
Avoidance ≥1 (memories, reminders/places etc)
Negative alterations in cognition and mood ≥2 (e.g. inhibited memory, blame, neg. beliefs/emotions)
Alterations in arousal and reactivity ≥2 (irritable, reckless, sleep disturbance, dec. concentration etc)
Sx cause functional impairment
Mx: Prazosin is effective for PTSD nightmares
Trauma: actual/threatened death, serious injury, or sexual violence through direct experience, witnessing, of learning of from close family/friend
Acute Stress Disorder (R2)
Sx for 3d-1m, within 4wks following exp. to trauma
Intrusion symptoms ≥1 (memories, reactions, etc)
Avoidance ≥1 (memories, reminders/places etc)
Negative alterations in cognition and mood ≥2 (e.g. inhibited memory, blame, neg. beliefs/emotions)
Alterations in arousal and reactivity ≥2 (irritable, reckless, sleep disturbance, dec. concentration etc)
Sx cause functional impairment
Adjustment Disorders (R2)
A) Emotional or behavioural sx within 3m of an identifiable stressor
B) Causes disproportionate distress or functional impairment
C) Not better explained by substance/condition/disorder
D) Resolves within 6m of the stressor ending
Trauma & Stress‑Related Disorders Mx
Mild/Mod Sx <3m: active monitoring, supportive
Severe <3m or Sx ≥3: Psych Therapy, Pharm
Trauma-focused cognitive behavioural therapy (TFCBT)
Eye movement desensitisation and reprocessing (EMDR)
Pharm:
1st Line: SSRIs, SNRIs (Venlafaxine, monitor BP), Mirtazapine (for insomnia), Prazosin ( PTSD nightmares)
Dissociative Identity Disorder (R3)
A) Presence of >2 distinct identities (alters) that control a person's behavior, often caused by severe, chronic childhood trauma
B) Causes recurrent amnesia/gaps in recall
C) Clinically Significant Distress or Impairment
D) Not a Normal Cultural or Religious Practice
E) Not Due to Substances or Medical Conditions
Dissociative Amnesia (R3)
A) Inability to Recall Important Information, usually following trauma/stress and is inconsistent with ordinary forgetting
B) Clinically Significant Distress or Impairment
C) Not better explained by sub./condition/disorder
Depersonalisation/Derealisation Disorder (R3)
A) Persistent or Recurrent Experiences of One or Both of:
Depersonalisation (robotic)
Derealisation (detachment)
B) Reality Testing Remains Intact
C) Clinically Significant Distress or Impairment
D) Not better explained by sub./condition/disorder
Dissociative Disorder Mx
Psychotherapy, CBT
Psychoeducation
Borderline Personality Disorder/BPD (R1) - Cluster B
Personality and Emotional Regulation Disorder
Pervasive pattern of instability in affect, self‑image, and interpersonal relationships with marked impulsivity
>5 of IMPULSIVE:
Impulsivity in >2 potentially self‑damaging areas (e.g. sex, money, substances)
Moodiness
Paranoia: Transient, stress‑related paranoid ideation or severe dissociative symptoms
Unstable self image/Identity disturbance
Labile intensive relationships: Unstable and intense interpersonal relationships
Suicidal: Recurrent suicidal behaviour, gestures, threats, or self‑mutilating behaviour
Inappropriate/intense anger or difficulty controlling anger
Vulnerability or abandonment
Emptiness: Chronic feelings of emptiness
Mood fluctuations over the course of the DAY/short periods (Bipolar = over longer periods/episodic/wks)
Feel unsafe in relationships, threat of abandonment
RF = genetics, trauma, difficult relationships
Usually emerges in adolescence or early adulthood
Is REVERSIBLE with Mx
Antisocial Personality Disorder (R2) - Cluster B
Pervasive pattern of disregard for and violation of the rights of others
Sx occur since age 15yrs, with dx made in adulthood
A) Pervasive Pattern of Antisocial Behaviour (failure to conform, impulsive, deceitful, reckless)
B) Age Requirement >18rs (must be an adult)
C) Evidence of Conduct Disorder Before Age 15
D) Exclusion Criteria: Antisocial behaviour does not occur exclusively during schizo/bipolar/mania
Narcissistic Personality Disorder (R2) - Cluster B
Pervasive pattern of grandiosity, need for admiration, and lack of empathy, beginning by early adulthood
>5 of:
Grandiose sense of self‑importance
Preoccupation with fantasies (success, power etc)
Belief of being "special" and unique
Requires excessive admiration
Sense of entitlement
Interpersonally exploitative behaviour
Lack of empathy
Envy of others/belief others envy them
Arrogant, haughty behaviours or attitudes
Traits are Pervasive, Inflexible, Maladaptive
Not better explained by Mood disorders (e.g. mania), Substance use or Cultural/Occupational norms
Obsessive‑Compulsive Personality Disorder (R2) - Cluster C
Pervasive pattern of preoccupation with orderliness, perfectionism, and control
>4 of:
Preoccupation with details, rules, lists, order, organisation, or schedules
Perfectionism that interferes with task completion
Excessive devotion to work and productivity (not explained by financial necessity)
Overconscientiousness, scrupulousness, and inflexibility about morality, ethics, or values
Inability to discard worn‑out/worthless objects, even with no sentimental value
Reluctance to delegate tasks or work with others
Miserly spending style toward self/others (hoards)
Rigidity and Stubbornness
Diagnosed in adulthood
Personality trait rather than anxiety disorder (OCD)
Limited insight but usually no obsession/compulsions
Paranoid Personality Disorder (R3) - Cluster A
Pervasive pattern of distrust and suspicion of others
>4 of:
Suspects, without sufficient basis, that others are exploiting, harming, or deceiving them
Preoccupied with unjustified doubts about the loyalty or trustworthiness of friends or associates
Reluctant to confide in others
Reads hidden demeaning or threatening meanings into benign remarks or events
Persistently bears grudges (unforgiving of insults, injuries, slights)
Perceives attacks on character or reputation
Recurrent suspicions, without justification, of the fidelity of a spouse/sexual partner
Disturbance does not occur exclusively during: Schizophrenia, Bipolar/Mania, Other Psych Disorder
Schizoid Personality Disorder (R3) - Cluster A
Pervasive pattern of detachment from social relationships and a restricted range of emotional expression
> 4 of:
Neither desires nor enjoys close relationships, including being part of a family
Almost always chooses solitary activities
Min-No interest in sexual experiences with another
Takes pleasure in few/any activities
Lacks close friends/confidants, except 1st‑degree relatives
Appears indifferent to praise/criticism from others
Shows emotional coldness, detachment, or flattened affectivity
Disturbance does not occur exclusively during: Schizophrenia, Bipolar/Mania, Other Psych Disorder
NOT Attributable to ASD or Medical/Neuro Condition
Schizotypal Personality Disorder (R3) - Cluster A
Pervasive pattern of social and interpersonal deficits, marked by: acute discomfort with close relationships, cognitive/perceptual distortions, eccentric behaviour
> 5 of:
Ideas of reference (exclude fixed delusions)
Odd beliefs or magical thinking (e.g. superstitions, clairvoyance, belief in special powers)
Unusual perceptual exp. (incl. bodily illusions)
Odd thinking/speech (e.g. vague, circumstantial, metaphorical, or over‑elaborate)
Suspiciousness or paranoid ideation
Inappropriate or constricted affect
Behaviour/appearance that is odd, eccentric, or peculiar
Lacks close friends/confidants, except 1st‑degree relatives
Excessive social anxiety (familiarity does not dec.)
Disturbance does not occur exclusively during: Schizophrenia, Bipolar/Mania, Other Psych Disorder
NOT Attributable to ASD or Medical/Neuro Condition
Histrionic Personality Disorder (R3) - Cluster B
Pervasive pattern of excessive emotionality and attention‑seeking
> 5 of:
Uncomfortable when not the centre of attention
Interactive behaviour with others is often inappropriate, sexually seductive or provocative
Rapidly shifting/shallow expression of emotions
Consistently uses physical appearance to draw attention to self
Style of speech is excessively impressionistic and lacking in detail
Self‑dramatisation, theatricality, and exaggerated expression of emotion
Suggestibility: easily influenced by others or circumstances
Considers relationships to be more intimate than they actually are
Traits must not occur exclusively during: Mood Disorders (e.g. mania) or Substance Intoxication
Must be pervasive and enduring, not situational
Avoidant Personality Disorder (R3) - Cluster C
Pervasive pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation
> 4 of:
Avoids occupational activities that involve significant interpersonal contact (due to fears of criticism, disapproval, or rejection)
Unwilling to get involved with people
Shows restraint within intimate relationships
Preoccupied with being criticised or rejected in social situations
Inhibited in new interpersonal situations
Views self as socially inept, personally unappealing, or inferior to others
Unusually reluctant to take personal risks/engage in new activities
Must not be better explained by: Social anxiety disorder alone, ASD, Mood disorders
Must be pervasive and enduring, not situational
Dependent Personality Disorder (R3) - Cluster C
Pervasive and excessive need to be taken care of, leading to submissive and clinging behaviour and fears of separation
> 5 of:
Difficulty making everyday decisions without excessive advice and reassurance from others
Needs others to assume responsibility
Difficulty expressing disagreement
Difficulty initiating projects or doing things independently
Goes to excessive lengths to obtain nurturance and support
Feels uncomfortable or helpless when alone
Urgently seeks another relationship when one ends
Unrealistic preoccupation with fears of being left to take care of themselves
Traits must not be better explained by: Major depressive dis, Anxiety dis, Medical illness
Must be pervasive and enduring, not situational
Personality Disorder Mx
Psychotherapy = 1st line!
Create Crisis/Risk Management Plan
Adjunct Pharmacotherapy for Comorbidites (SSRIs for Depression/Anxiety etc)
Cluster Subtypes:
Cluster A: odd or eccentric
Cluster B: dramatic, emotional and erratic
Cluster C: anxious or fearful
Anorexia Nervosa (R1)
Restriction of caloric intake relative to requirements leading to:
Low body weight for age, height, gender and developmental status
An intense fear of gaining weight
A body image disturbance/Overvaluation of weight or shape as an expression of self-worth
Two Subtypes:
Restrictive: no binging, limiting food intake, compulsive exercise
Binge Eating and Purging: recurrent episodes of binge eating (uncontrolled overeating) and purging (eg self-induced vomiting, laxative or diuretic misuse)
Often have medical and psychological comorbidities (eg osteopenia, pancreatitis, depression, anxiety)
Hospitalise when BMI <15, BP <80 systolic, dec. vitals
Life-threatening Weight Loss: BMI <15 in adults, <75% of median BMI for age + sex in children/adolescents
Precipitous Weight Loss: LOW >1kg for two consecutive weeks
Bulimia Nervosa (R1)
Severe preoccupation about weight and body shape
Recurrent episodes of binge eating, loss of control over eating
Compensatory mechanisms to prevent weight gain (self-induced vomiting, fasting, excessive exercise)
Body weight in the adequate to obese range
Binge eating and compensatory behaviours occur at least once weekly for >3m
RF: women in 20s/30s, trauma hx
Common Signs: Parotid Hypertrophy, Tooth Erosion
Feeding & Eating Disorder Mx
CBT/Psychotherapy
Nutritional replenishment/Re-feeding
Dietitian Referral
Pharm:
AN: No evidence for pharmacological mx
BN: SSRIs (1st = Fluoxetine, Citalopram, Fluvoxamine, Sertraline) - for young adults
Mx comorbidities (depression etc) and beware of pregnancy
Alzheimer's Disease (R1)
Chronic, progressive neurodegenerative disorder with global, non-reversible impairment in cerebral functioning
A) Neurocognitive Decline + Memory Impairment
B) Insidious onset with gradual, steady decline
Deteriorating course over up to 8-10yrs
Brain lesions: neurofibrillary tangles, senile plaques, neuronal loss, brain atrophy, acetylcholine synth defects
Most common dementia but can coexist with others
RF = Age, FHx, Genetics, Down's Syn., Hyperlipidaemia, Cerebrovascular disease, Drugs, Unfinished School
Vascular Dementia (R1)
Chronic progressive impairment of cognitive function caused by loss of brain parenchyma
Predominantly from cerebrovascular causes (infarction, haemorrhage, small-vessel changes)
Damage to grey and white matter
Signs:
Loss of Executive Functions (planning etc) > Memory
Motor and mood changes are often seen early
RF: age >60, obesity, HTN, smoking, DM
IX: MRI Brain, Ix causes of cog decline (UEC, BGL, B12)
Treat early and aggressively to prevent further cerebrovascular disease/address causes
Frontotemporal Dementia (R2)
Neurodegenerative Dementia causing disruption in personality and social conduct ± primary language disorder (2nd most common after AD)
Sx: Parkinsonism (50% of pts), Language Impairment, Personality/Social Behaviour Decline, Altered Eating Habits, Inattentiveness, Impulsivity
Note: does not usually present w memory loss
RF: Age 45-65 (mid-life), FHx, Genetics
Lewy Body Dementia (R2)
Neurodegenerative disorder with Lewy Bodies characterised by:
Parkinsonism (Bradykinesia, Tremor, Rigidity)
Progressive cognitive decline (with fluctuations)
Prominent executive dysfunction
Behavioural and sleep disturbances (REM disorder)
Visuospatial impairment
Ix: Pathology shows presence of Lewy Bodies (Autopsy?), CT/MRI Head, Screening
Mx:
Behavioural = Cholinesterase Inhibitors (Donepezil and Rivastigmine are best for behavioural sx without motor sx exacerbation)
REM Disorder = Clonazepam/Melatonin
Motor Sx = Levodopa/Carbidopa
Lewy Bodies: toxic clumps formed by damaged alpha-synuclein proteins folding into irregular shapes (linked to progressive dopamine loss in the brain)
Dementia due to Parkinson's Disease (R3)
Significant cognitive decline after >1yr of motor sx due to Parkinson’s Disease
Often overlap with Lewy Body Dementia (cognitive decline and motor sx begin and progress together)
Dementia due to Prion Disease (R3)
Very rapidly progressive fatal dementias due to prions
Disease is spontaneous, genetic or acquired
Sx: Behavioural/psychiatric changes, memory impairment, visual disturbances, myoclonus, ataxia, language/hearing issues, movement dysfunction
RF: genetics, prion-contaminated surgical instruments, blood products/transfusions, UK Beef 1980-1996
Ix: pathology = definitive, MRI B
No cure - only palliative management (mortality = 1yr)
Dementia due to Huntington's Disease (R3)
Autosomal dominant slow-progressing neurodegenerative disorder often presenting mid-life
Sx: chorea, incoordination, cognitive decline, personality changes, psychiatric sx (resulting in immobility, mutism, and inanition)
Prognosis: 20yrs from dx
RF: genetics/FHx (pre-test genetic counselling/testing is recommended)
Dementia due to HIV (R3)
HIV-Associated Neurocognitive Disorder (HAND)
Rare neurodegenerative disorder resulting from HIV infection (virus attacks brain cells causing inflammation and damage)
Does not directly infect neurons but indirectly causes cognitive damage → subcortical dementia
More common in the later stages of HIV infection (7% of pts), but rare due to antiviral treatments (ART)
Severity levels:
Asymptomatic Neurocognitive Impairment (ANI)
Mild Neurocognitive Disorder (MND)
HIV‑Associated Dementia (HAD) = severe form
Signs and Sx:
Cognitive Features
Bradyphrenia (slowed thinking), Impaired attention/concentration, Executive dysfunction (planning/decisions), Memory retrieval problems (rather than storage)
Motor Features
Gait instability, Poor coordination, Slowed movements, Tremor
Behavioral / Psychiatric Features
Apathy, Depression, Irritability, Social withdrawal
Unlike Alzheimer’s disease, language and visuospatial skills are preserved
Neurocognitive Disorder Mx (Dementia)
Supportive: Exercise/Physical Activity, Memory Aids, CBT
End of life care
Pharmacological:
Acetylcholinesterase Inhibitors: (Donepezil, Galantamine Rivastigmine)
Transdermal patch > oral
Improve/stabilise cognition, alertness and function (Good for Mild to Severe)
AEs: GIT sx, Brady, Neuro/Insomnia/Vivid dreams
NMDA Receptor Antagonists: (Memantine)
SHORT-TERM improve/stabilisation in cognition/function
Good for Moderate to Severe
Supportive Pharm:
SSRIs: comorbid depression, agitation/aggression
Trazodone/Melatonin: insomnia
Vascular Prevention: Antiplatelets (Aspirin), Anticoagulants (Apixiban, Rivaroxaban)
Lewy Body Motor Sx = Levodopa/Carbidopa
Antipsychotics for acute mx of behavioural disturbance in dementia should be avoided increased risk of AEs/mortality
Delirium (R1)
Disturbance in attention and awareness developing over a short period of time, is a change from baseline and fluctuates throughout the day (
Acute deterioration of mental state characterised by fluctuating sx of impaired attention, cognition and consciousness, typically developing over hours to days
Three Main Types:
Hyperactive (agitation, restless, delusions, hallucinations)
Hypoactive (quiet, withdrawn) - most common
Mixed (alternates b/w hyper and hypo)
Ix: identify cause (bloods, BGL, ECG, temp, urine)
Mx: reverse causes, low stimuli environment
Avoid physical/chemical restraints (meds can worsen delirium)
IV Thiamine 3-5d if alcohol withdrawal
Antipsychotics if severe distress/hyperactive
Haloperidol, Olanzapine, Risperidol = Non Parkinson’s/Lewy Body Dementia
Quetiapine = Parkinson’s/LB Dementia
Demoralisation (R1)
Clinical/dysphoric state of existential distress characterized by:
Helplessness
± Hopelessness
± Subjective incompetence/Loss of meaning or purpose
Often arising from chronic illness, severe stress, or perceived failure to cope
Unlike depression, focus is on subjective incompetence rather than anhedonia (pervasive loss of interest)
Mx: psychotherapy, supportive care
Suicidality/Suicide Attempt (R1)
Two Types:
Impulsive: short time between idea and action
Planned: long time between idea and action (stages include idea, plan/research, prep etc)
RF: static (fixed, historic), dynamic (fluctuates in duration and intensity)
Mx: safety planning, psycotherapy, verbal de-escalation, consider involuntary tx, limit access to toxic drugs (overdose)
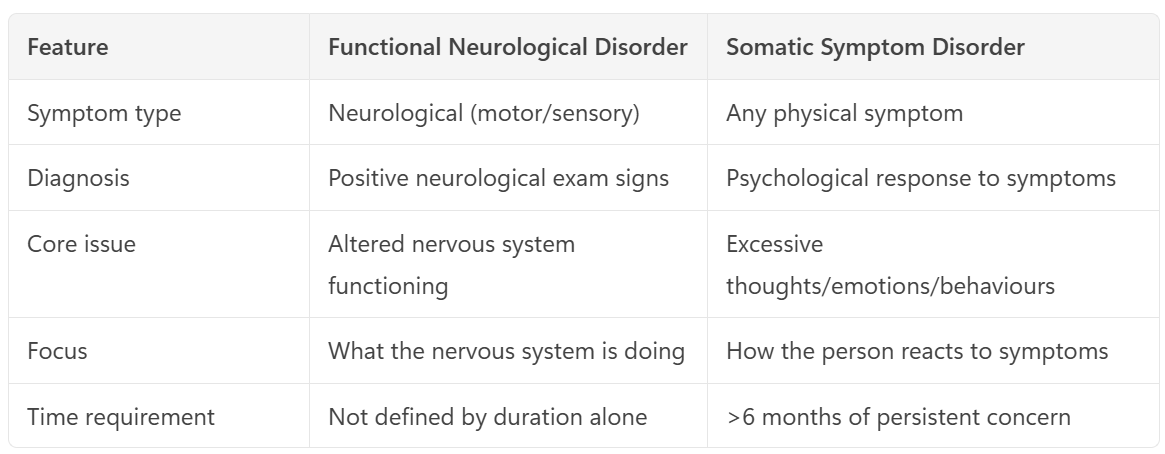
Somatic Symptom Disorder (R2)
Neuropsychiatric condition causing somatic sx associated with significant distress or impairment
Distressing physical sx (pain, fatigue, GI symptoms, etc.) that disrupt daily life, with/out medical explanation
Excessive and persistent psychological responses
Sx for >6m
Underlying cause not understood, psychological stressors may be a RF
Mx: CBT, Physiotherapy
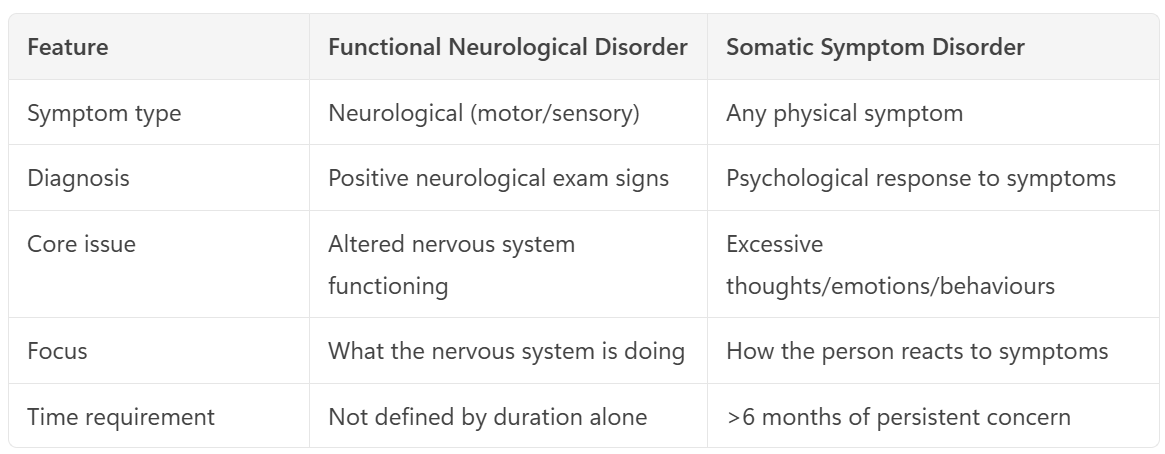
Functional Neurological/Conversion Disorder (R2)
Neuropsychiatric condition causing somatic sx associated with significant distress or impairment
Specific neurological (motor/sensory) signs and functional impairment
Problems with movement or sensation (e.g. weakness, tremor, numbness, non‑epileptic seizures, speech/gait problems) that look like neurological disease (inconsistent findings)
Underlying cause not understood, psychological stressors may be a RF
Dx: ‘rule in’ features on neuro exam
Sx improve with distraction
Inconsistency on exam
Patterns not matching known neuroanatomy
Mx: CBT, Physiotherapy, SSRIs etc (comorbid anx/dep)
Illness Anxiety Disorder (R2)
Disorder of health-related fear
Persistent fear/belief of having/developing a serious illness
Excessive fear of illness with minimal to no physical/somatic sx
Preoccupation with illness lasts ≥ 6m
Behaviours include: Repeated reassurance-seeking, Excessive internet searching, Frequent doctor visits or avoidance of medical care
Mx: CBT, Anxiety Mx (SSRIs etc)
Psychological Factors Affecting Medical Conditions (R2)
A) Medical condition/symptom is present
B) Psychological/behavioural factors adversely affect the medical condition in one of:
Influence the course of medical illness (e.g. cause exacerbation or trigger)
Interfere with tx (e.g. poor adherence)
Factors constitute additional well established health risks for the individual
Influence the underlying pathophysiology, precipitating or exacerbating sx
C) Not better explained by another mental disorder
Factitious Disorder (R3)
Patient consciously pretends to have physical sx without a clear secondary gain
A) Falscification of physical or psychological signs/sx or induction of injury or disease, associated with identified deception
B) The individual presents themself as unwell, injured or impaired
C) The deceptive behaviour is evident even in the absence of obvious external rewards
D) The behaviour is not better explained by another mental disorder e.g. delusional disorder
Can be Factitious disorder imposed on another (by proxy)
Malingering (R3)
Patient consciously pretends to have physical sx with a clear secondary gain
A) Falscification of physical or psychological signs/sx or induction of injury or disease, associated with identified deception
B) The individual presents themself as unwell, injured or impaired
C) The deceptive behaviour is evident even in the presence of obvious external rewards
D) The behaviour is not better explained by another mental disorder e.g. delusional disorder
Can be Factitious disorder imposed on another (by proxy)
Medication‑Induced Symptoms (R1)
Corticosteroids:
Psychiatric AEs = euphoria, hypomania, depression, disturbances of mood, cognition, sleep and behaviour
Delirium/psychosis are less common
Yasmin (OCP), Beta Blockers:
Increased risk of depression
Ketamine
Dissociation associated with confusion, fear or euphoria
Levodopa (Dopamine Agonist):
AEs = depression, psychotic sx, impulse control disorders (e.g. gambling, hyper-sexuality, overspending, binge eating, inappropriate internet use)
Isotretinoin (Roaccutane - Acne):
Dry skin & mucus membranes, depression
Levetiracetam (Keppra - Anticonvulsant):
Behavioural changes (e.g. agitation, irritability, depressed mood, anxiety)
Endocrine‑Induced Symptoms (R1)
Pheochromocytoma:
Classic triad of episodic headaches, tachycardia and sweating
Can cause anxiety symptoms (e.g. panic attacks)
Cushing's Syndrome:
Central obesity, proximal muscle wasting & hypertension
Can cause depression, mania and psychosis
Polycycstic Ovarian Syndrome:
Dx requires >2 of: Oligo/anovulation, Clinical or biochemical evidence of hyperandrogenism & polycystic ovaries
Hyperparathyroidism
‘Bones, stones, abdominal moans and psychic groans’
Sx: renal stones and decreased bone density, fatigue, depressed mood, psychosis, cognitive dysfunction
Hyperthyroidism:
Palpitations, heat intolerance, weight loss & sweating
Anxiety, insomnia, depression, mania, psychosis
Hypothyroidism:
Bradycardia, weight gain, cold intolerance, hair loss, fatigue, depression
Addison’s Disease:
Fatigue, weight loss, salt craving, hyperpigmentation & hypotension
Depression, psychosis, anxiety, mania (less common)
Encephalopathy (R2)
Diffuse disease of the brain (infection or inflammation) altering brain function or structure
Causes: Infections, Autoimmune Reactions, Metabolic Dysfunction (hepatic enceph), Toxins, Raised Intracranial Pressure, Chronic Progressive Trauma, Poor Nutrition, Hypoxia
Autoimmune Encephalitis: enceph. associated w abs against neuronal cell surface/synaptic proteins (tumours etc)
First Manifestation of Auto Enceph. is psychiatric/psychotic sx (acute/subacute changes to mood, behaviour, personality, cognition, consc. state)
Red Flag = Enceph sx + Psychiatric Sx
Mx: immunosuppression, address cause (tumours etc), psychiatric meds for sx
Brain Tumours (R2)
Sx: generalised sx (headache, seizure), raised intracranial pressure (headache, N/V), focal neurological deficits (weakness, sensory loss), cognitive deficits (memory, mood)
Sx can often be mistaken for depression
Acquired Brain Injury (R2)
Any injury to the brain occurring after birth
Traumatic (TBI): head-strike, concussion, shear forces (damage axons, not seen on imaging)
Non-Traumatic: encephalitis, meningitis, stroke, substance abuse, brain tumour, hypoxia (MI, overdose etc)
Sx: depend on type and location of injury
Physical: Motor/speech/sensory changes, amnesia, epilepsy
Cognitive: memory, impulse control, planning, judgement, concentration, abstract thought, attention
Mental Health: mood/substance use disorders, anxiety, sleep disturbance, psychosis, aggression
Psychosocial: loss of identity, relationship breakdown, financial stressors, social isolation
Neurocognitive Disorders: Alzheimer's, Parkinson's
Mx: reduce stimulation, avoid triggers, pain mx, pharm
Pharmacological: Psychotropics (start low go slow), Antipsychotics, Benzos; Consider BB, Valproate, Carbamazepine
HIV-Related Sequelae (R3)
Long-term health complications resulting from HIV infection, including opportunistic infections (e.g., tuberculosis, pneumonia) and mental disorders
Common comorbid mental disorders with HIV disease:
Delirium
Minor cognitive-motor disorder (MCMD)
HIV-associated dementia
Major depression
Bipolar disorder (including AIDS mania)
Schizophrenia (increased risk with HIV)
Substance abuse/dependence
Post-traumatic stress disorder (PTSD)
Personality Disorder
Increased suicide risk
Post-Partum Depression (R1)
Onset of a depressive episode/illness within 4 weeks of childbirth
Episodes of postnatal depression last 3-6m (may be m-yrs)
Psychiatric emergency requiring prompt referral
Sx: depressed mood, anhedonia, weight changes, sleep disturbance, psychomotor problems, low energy, excessive guilt, loss of confidence or self-esteem, poor concentration, or suicidal ideation
Exclude postnatal psychosis and bipolar disorder in all pts
RF: minimal social support, antenatal anxiety, PMHx depression or pregnancy loss, preterm birth
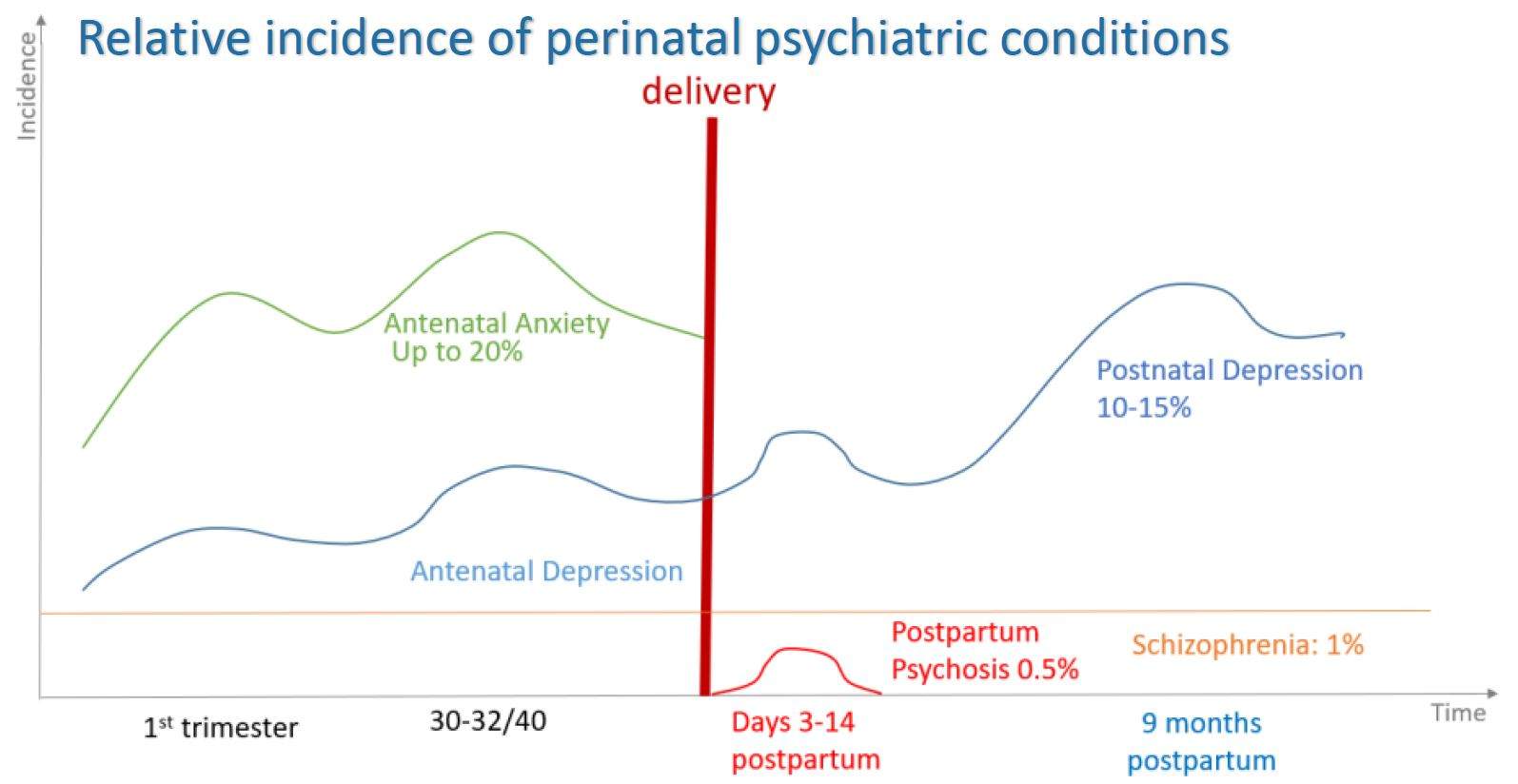
Post-Partum Psychosis (R1)
Psychiatric emergency! (Inc. risk of suicide/infanticide, abuse)
Arrange immediate psychiatric evaluation/safety assessment
Presents within 4wks of delivery
Sudden change in mental status, agitation, confusion, or insomnia, accompanied by mood features such as anxiety, mania, irritability, or depression
Pt typically does not recognise their behaviours/thoughts as abnormal
Sx: delusions, hallucinations, bizarre behaviour, depressed mood, mania, mood liability, insomnia
RF: bipolar disorder, prior eps, FHx, primiparity, sleep dep.
Mx: Psychotropics + ECT
Tx/monitoring should continue for at least 6-12m following remission given the high risk and dangers of relapse
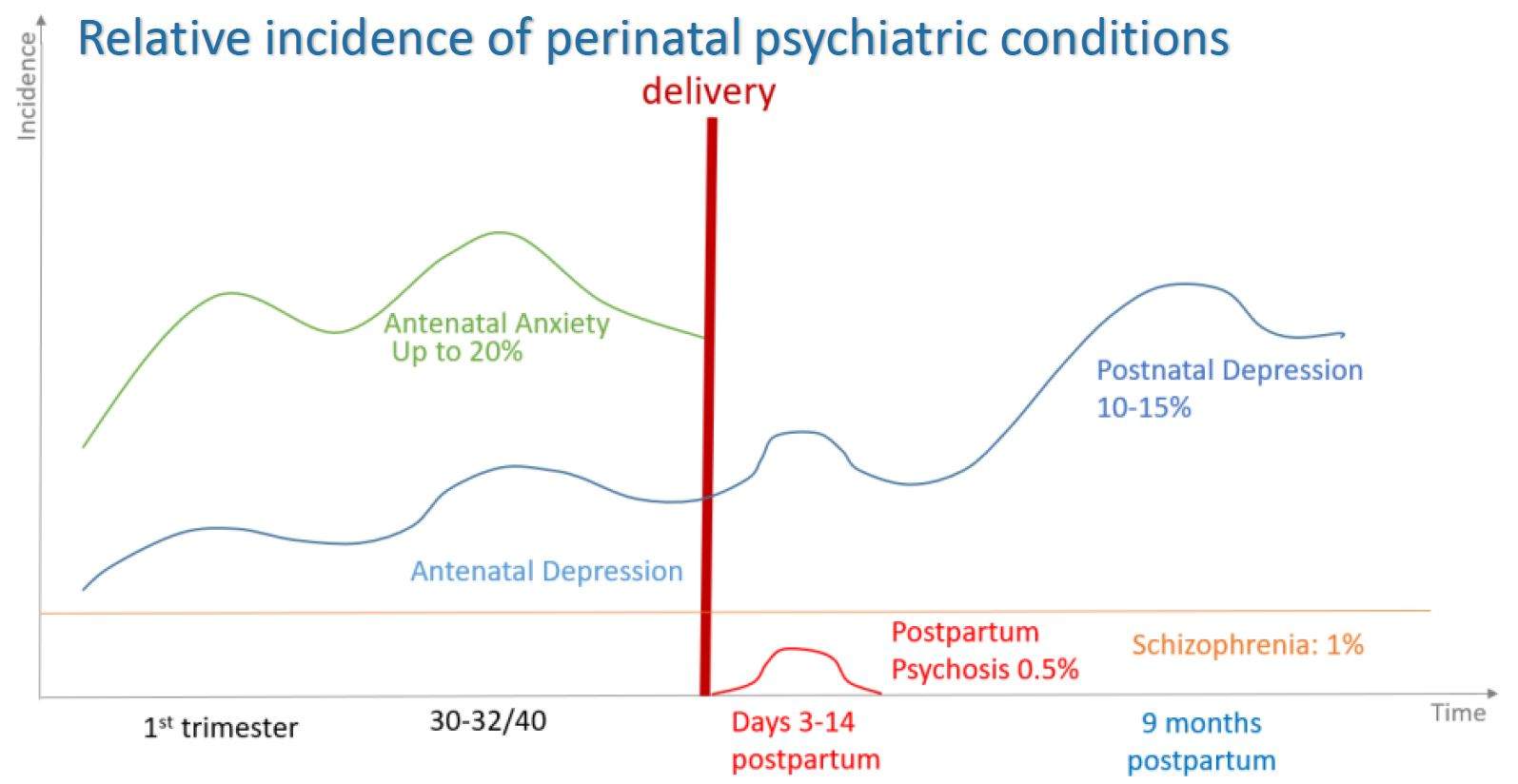
Baby Blues (R2)
Mild lowered mood/tearfulness in the days post-partum (3-5d after birth)
Cause unknown but believed to be due to rapid hormone changes
Affects up to 80% of women
Often coincides with onset of lactation (1-2d post-partum)
Should shift within 3-7d and is not usually an emergency presentation (caution for developing anxiety or depression)
Sx: mood swings, teariness, feeling overwhelmed and/or anxious
Perinatal Obsessive-Compulsive Disorder (R3)
Egodystonic intrusive images of harming the baby
'Infant-focused' obsessions without compulsions
Often associated with avoidance behaviours
Obsessions are often of ego-dystonic aggressive thoughts towards the child or of some misfortune coming to the child
Obsessions about accidental harm to the infant and other infant-focused obsessions, checking compulsions, self-reassurance and seeking reassurance from other
Onset and exacerbation of pre-existing OCD both linked to post-partum period
Increased risk of harm to self (not usually to child) and secondary depression
Perinatal Psychiatry Mx
Psychotherapy including relationship therapy
Pharm:
SSRIs
Usually first-line for depression, including during breastfeeding
Avoid some Anti-Depressants such as paroxetine
Psychiatric Referral
May be necessary for patients who do not respond to treatment
Urgent psychiatric assessment is warranted if:
There is a risk of self-harm or harm to the child at any time
A postnatal psychosis, manic or mixed ep. is suspected
Intellectual Disability (R1)
Onset during developmental period and includes both intellectual and adaptive functioning deficits PLUS the following criteria:
A) Deficits in intellectual functioning confirmed by clinical assessment and standardized intelligence testing
B) Deficits in adaptive functioning leading to failure to meet developmental and sociocultural standards for personal independence and social responsibility
Without support, deficits limit functioning in >1 activity of daily living (e.g. communication, socialising, independent living) across multiple environments
C) Onset of deficits during developmental period
RF: Genetic (Klinefelter’s, Down’s, Fragile X), Perinatal (maternal DM, inf. prematurity), Malnutrition, Trauma
Autism Spectrum Disorder/ASD (R1)
A) Persistent deficits in social communication and social interaction across multiple contexts
Deficits in social-emotional reciprocity
Deficits in nonverbal communicative behaviors used for social interaction
Deficits in developing, maintaining, and understand relationships
B) Restricted, repetitive patterns of behavior, interests, or activities with >2 of:
Stereotyped or repetitive motor movements, use of objects, or speech
Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns)
Highly restricted, fixated interests that are abnormal in intensity or focus
Hyper/hyporeactivity to sensory input or unusual interest in sensory aspects of the environment (e.g. apparent indifference to pain/temperature, adverse response to specific sensations)
C) Sx must be present in the early developmental period
D) Sx cause clinically significant impairment in social, occupational, or other important areas of current functioning
E) Disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay
Intellectual disability and autism spectrum disorder frequently co-occur
To make comorbid diagnoses of ASD and intellectual disability, social communication should be below that expected for general developmental level
Must also rule out causes of speech delay (e.g. deafness)
Attention‑Deficit and Hyperactivity Disorder/ADHD (R2)
Persistent pattern of inattention and/or hyperactivity–impulsivity that interferes with functioning or development:
Inattention:
>6 sx of inattention in <16rs, >5 sx for >17yrs/adults
Sx of inattention have been present for >6m
Sx are inappropriate for developmental level
Hyperactivity and Impulsivity:
>6 sx of hyperactivity-impulsivity <16rs, >5 sx for >17yrs/adults
Sx of hyperactivity-impulsivity have been present for >6m
Sx are disruptive and inappropriate for the person’s developmental level
Additional Criteria:
Several inattentive or hyperactive-impulsive sx were present before age 12
Several sx are present in >2 settings (e.g. home, school or work; w friends/relatives)
Clear evidence that the sx interfere with/reduce quality of social, school, or work functioning
Sx are not better explained by another mental disorder and do not happen only during the course of schizophrenia or another psychotic disorder
Three Main Types:
Combined
Predominantly Inattentive
Predominantly Hyperactive-Impulsive
RF: prematurity, FHx, substance use hx, epilepsy/ABI
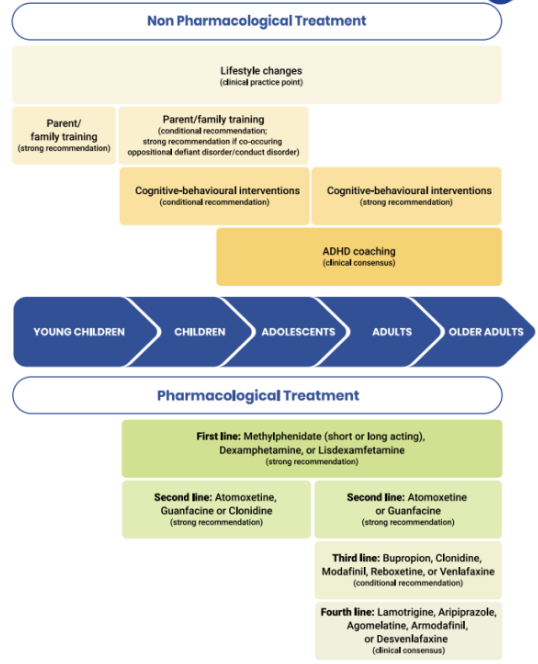
Mx: Stimulants - Meth/Dex/Lis (1st), Atomoxetine, Guanfacine, Clonidine
Global Developmental Delay (R3)
Children under the age of 5yrs old, who fail to meet developmental milestones across a range of intellectual functioning
Pts are too young to partake in standardised intellectual testing
Will require reassessment as the child grows older
Specific Learning Disorder (R3)
A) Difficulties in learning and using academic skills, with >1 of:
Inaccurate, slow of effortful reading
Difficulty understanding the meaning of what is read
Spelling difficulties
Expression (grammar) difficulties when writing
Difficulties with numbers or calculation
Difficulties with mathematical reasoning
B) Substantially below what is expected for individual's age
C) Learning difficulty begins in school-age years
D) Not better explained by another condition or sensory disability
Developmental Coordination Disorder (R3)
A) Learning and execution of coordinated motor skills is below expected level for age, given opportunity for skill learning
B) Motor skill difficulties significantly interfere with activities of daily living and impact academic/school productivity, prevocational and vocational activities, leisure and play
C) Onset is in the early developmental period
D) Motor skill difficulties are not better explained by intellectual delay, visual impairment or other neurological conditions that affect movement
Communication Disorders (R3)
Group of disorders characterised by deficits in speech, language and/or communication
Speech: expressive production of sounds
Language: form, function and use of conventional system of symbols in rule governed form of communication
Communication: any verbal or nonverbal behaviour/expression (intentional or unintentional) that influences the behaviour, attitudes or ideas of another person
Types of Communication Disorders:
Language Disorders: difficulties in the acquisition and use of language
Speech Sound Disorder: disorder of speech sound production
Childhood-Onset Fluency Disorder (Stuttering): disturbance in the normal fluency and time patterning of speech
Social (Pragmatic) Communication Disorder: difficulties in the social use of verbal and nonverbal communication
Tic Disorder (R3)
Tourette's Disorder:
A) BOTH multiple motor AND >1 vocal tics have been present at some time during the illness
B) Tics may wax and wane but have persisted for >1yr
C) Onset before age 18
D) Not attributable to another condition/substance
Persistent (Chronic) Motor or Vocal Tic Disorder:
As above except:
Single/multiple motor
OR
Vocal tics (not both)
Provisional Tic Disorder:
A) Single/multiple motor &/or vocal tics
B) Present for <1year
C) Onset before age 18
D) Not attributable to another condition/substance
E) Criteria for above 2 disorders have never been met
Stereotypic Movement Disorder (R3)
A) Repetitive, seemingly driven, and apparently purposeless motor behaviour
B) Interferes with social, academic or other activities and may cause self-injury
C) Onset in early developmental period
D) Not attributable to another condition
Neurodevelopmental Disorder Mx
Psychotherapy: Social Skills Training, Occupational Therapy, Counselling
Pharm:
ASD: for severe behavioural issues
Risperidone: calms aggressive behaviours etc
ADHD: Stimulants are first line!
Stimulants: Methylphenidate (short or long acting - Ritalin), Dexamfetamine, Lisdexamfetamine
Improve attention and impulses
Should not be given to pts <6yrs
Atomoxetine, Guanfacine, Clonidine (for aggression)
Bupropion, Clonidine, Modafinil, Reboxetine, Venlafaxine
Lamotrigine, Aripiprazole, Agomelatine, Armodafanil, Desvenlafaxine
Methylphenidate: Ritalin = SA or LA, Concerta = Extended Release (less potential abuse, only use if responsive to immediate-release MPH)
Dexamfetamine: No response to MPH, higher risk of AEs, Lisdexamfetamine (Vyvanse) = LA
Atomoxetine: Strattera (Noradr. Reup. Inh.), cannot combine w other stimulants, only if stimulants not tolerated, good for co-morbid anxiety/psychosis/tics, AEs = prolonged QT + stunt growth, low risk of misuse
Guanfacine: Intuniv (Alpha-Adrenergic Rec. Ag), if Stimulants or Atomoxetine not tolerated, if tic disorder, Adjunct w Stimulants if poor response, AEs = Hypotens/Bradyc/Sedation
Clonidine: Catapres, good for aggression and sleep disturbance, not good for inattention, shorter half life than guanfacine (similar role), AEs = Hypotens
Must monitor ADHD sx, Height/Weight, BP/HR, AEs etc
Anorexia/Bulimia Nervosa in Paediatrics/<12yrs (R1)
AN: Developmental Emergency! (Affect growth/development)
Weight Assessment uses Growth Charts more than BMI
BN: weight is usually near-normal, binges may be smaller/chaotic/poorly defined, compensatory behaviours may be less extreme/inconsistent
Differences in Presentations:
2/3 have similar psychological sx to adult patients
Key differences:
Limited Insight
Less likely to report fear of weight gain or being fat
Less likely to understand the seriousness of their illness
More likely to present with non-specific somatic symptoms
More likely to have unspecified eating disorder (or ARFID)
Less likely to use vomiting or laxatives
Lose weight more rapidly
More likely to have a lower percentage of ideal weight
Increased proportion of boys in this age group
Cx: Growth retardation, Osteoporosis, Infertility/Amenorrhoea, Alterations in brain development/cognitive impairment, Depression/Anxiety/OCD
Mx: FBT (Family-Based Tx), Nutritional/Fluid Resus
Higher focus on weight restoration before insight
Refeeding Syndrome:
Potentially fatal shifts in fluids and electrolytes that may occur in undernourished children/adolescents being re-fed
Hallmark biochemical feature is hypophosphataemia
Risk in Nutritional and Fluid resus/re-introduction
Avoidant-Restrictive Food Intake Disorder/ARFID (R3)
Pattern of food avoidance or restriction that is not associated with excess concern about body image and results in at least one of:
Significant weight loss in adults
Failure to meet developmental height and weight targets in children or adolescents
Significant nutrient deficiency
Dependence on enteral feeding or oral nutrition supplements
Marked interference with psychosocial functioning
Mx: behavioural refeeding, graded food exposure, cognitive therapies
Pica (R3)
Persistent craving and consumption of non-food item (e.g. dirt, paint chips, ice, hair) with no nutritional value for >1m
Often occurs in children, pregnant women, or individuals with developmental disabilities
Rumination Disorder (R3)
Presence of persistent or recurrent regurgitation of recently ingested nonacidic gastric contents, which are subsequently swallowed (most often) or spat out, for at least 6m
Pressurisation of the abdominal cavity caused by contraction of the abdominal muscles, overcoming the lower oesophageal sphincter.
Causes regurgitation of gastric contents into the oesophagus and pharynx
Regurgitation may appear as vomiting, but there is an absence of nausea and retching
Distinguished from GORD if regurgitation ceases if gastric contents become acidic, and if sx do not respond to PPIs
Enuresis (R3)
A) Repeated voiding of urine into bed/clothes - whether involuntary or intentional
B) Clinically significant either based on frequency, significant distress &/or impairment in functioning
C) At least 5 years old (or equivalent developmental level)
D) Not attributable to a substance or another medical condition.
Can be either nocturnal, diurnal or both
Encopresis (R3)
A) Repeated passage of stool into inappropriate places (e.g. clothing/floor - whether involuntary or intentional)
B) Clinically significant either based on frequency, significant distress &/or impairment in functioning
C) At least 4 years old (or equivalent developmental level)
D) Not attributable to a substance or another medical condition (unless this is constipation overflow)
Oppositional Defiant Disorder (R3)
A) Pattern of angry/irritable mood, argumentative/defiant behavior, or vindictiveness >6m with >4 sx from any of the following categories, and exhibited during interaction with at least one individual who is not a sibling.
Angry/Irritable Mood: Often loses temper, touchy/easily annoyed, angry/resentful
Argumentative/Defiant Behavior: Often argues with authority figures/adults, actively defies/refuses to comply, deliberately annoys others, blames others
Vindictiveness: Has been spiteful or vindictive at least twice within the 6m
B) Disturbance in behavior is associated with distress in the individual/others in his or her immediate social context (e.g., family, peer group, work colleagues), or it impacts negatively on social, educational, occupational, or other important areas of functioning
C) The behaviors do not occur exclusively during the course of a psychotic, substance use, depressive, or bipolar disorder
Also, the criteria are not met for disruptive mood dysregulation disorder.
Conduct Disorder (R3)
A) A repetitive and persistent pattern of behavior in which the basic rights of others or major age appropriate societal norms or rules are violated, as manifested by the presence of at least three of the following 15 criteria in the past 12 months from any of the categories below, with at least one criterion present in the past 6 months:
Aggression to People and Animals: Often bullies, threatens, intimidates others, initiates physical fights. Has used a weapon, been physically cruel to people/animals, stolen, forced someone into sexual activity
Destruction of Property: Has deliberately engaged in fire setting with the intention of causing serious damage, deliberately destroyed others’ property
Deceitfulness or Theft: Has broken into another’s house/building/car, often lies to obtain goods/favors/avoid obligations, stolen items without confronting a victim
Serious Violations of Rules: Often stays out at night before age 13, truant from schoo before age 13, has run away from home overnight at least twice
B) The disturbance in behavior causes clinically significant impairment in social, academic, or occupational functioning.
C) If the individual is age 18 years or older, criteria are not met for antisocial personality disorder
Reactive Attachment Disorder (R3)
Attachment trauma causing extreme withdrawal and rarely seeks comfort/support from primary caregivers
A) Consistent pattern of inhibited, emotionally withdrawn behaviour towards adult caregivers, manifested by both:
Rarely seeks comfort when distressed
Rarely/minimally responds to comfort when distressed
B) A persistent social & emotional disturbance characterised by at >2 of:
Minimal social/emotional responsiveness to others
Limited positive affect
Episodes of unexplained irritability, sadness/tearfulness (even in non-threatening interactions with adult caregivers)
C) The child has experienced a pattern of extremes of insufficient care, including at least one of:
Social neglect/deprivation with persistent lack of basic emotional needs being met (e.g. comfort, stimulation and affection)
Repeated changes of primary caregivers that limit opportunity to form stable attachments
Rearing in an unusual setting that limit opportunity to form selective attachments (e.g. institutions)
D) The care described in criterion C is assumed to be the reason for symptoms in criterion A & B
E) Does not meet criteria for ASD
F) The disturbance is evidence <5 years old
G) Developmental age is at least 9 months old
Disinhibited Social Engagement Disorder (R3)
Attachment trauma leading to an overfamiliarity with people
A) Pattern of behaviour where child actively approaches and interacts with unfamiliar adults, exhibiting at >2 of:
Reduced or absence reticence in approaching and interacting with unfamiliar adults
Overly familiar verbal/physical behaviour
Diminished checking back with adult caregiver when venturing away (even in unfamiliar circumstances)
Willingness to go off with unfamiliar adults with minimal hesitation
B) Criterion A behaviours are not limited to impulsivity
C) The child has experienced a pattern of extremes of insufficient care, including at >1 of:
Social neglect/deprivation with persistent lack of basic emotional needs being met (e.g. comfort, stimulation and affection)
Repeated changes of primary caregivers that limit opportunity to form stable attachments
Rearing in an unusual setting that limit opportunity to form selective attachments (e.g. institutions)
D) The care described in criterion C is assumed to be the reason for symptoms in criterion A & B
E) Developmental age is at least 9 months old