gas permeable lens designs and ordering of parameters
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
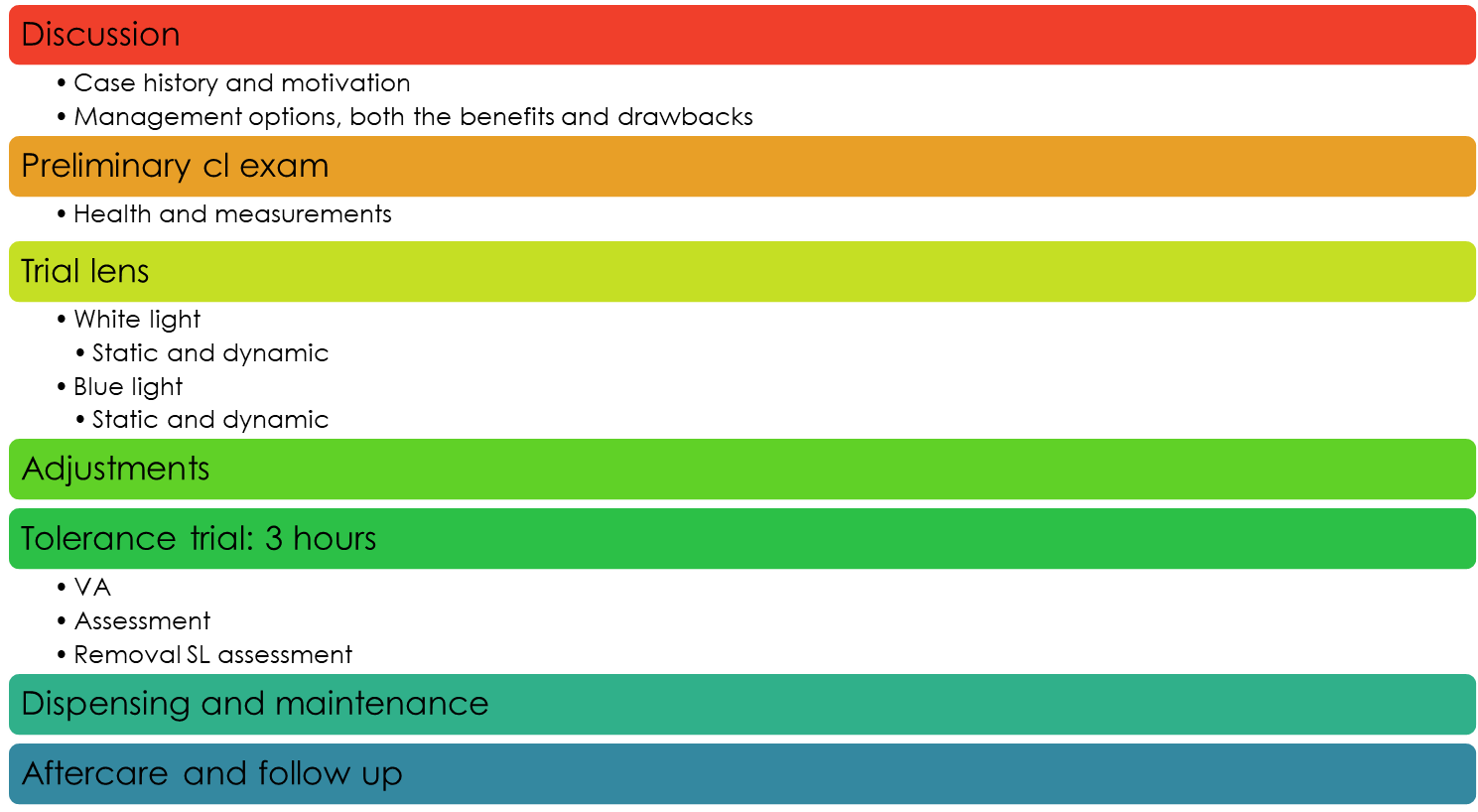
outline the routine examination protocol for a gas permeable lens
what should gas permeable lenses provide (5)
◦Good VA - in most cases as good as gls or better - and better than soft spherical lenses in terms of VA
◦Comfort and adequate wearing time
◦No ocular insult, maintain corneal integrity - lens should not damage any surface of eye
◦Maintenance of normal tear flow behind and over the lens
◦Normal facial appearance (posture) and invisibility - no head tilt - lenses should be essentially invisible
who should we fit GP lenses for/patient considerations (5)
◦Optimal anterior eye characteristics
◦High motivation
◦usually have moderate to high Rx
◦Corneal toricity: >0.25 D & <2.00 D - can be beyond this but basic fitting capped at 2
◦Residual cylinder <0.75 D
what are the benefits of GP lenses (7)
can be modified - can make adjustments once already ordered: change power up to +0.75D / peripheral curves can be flattened to increase EL / total diameter can be reduced / edges can be reshaped and polished
reduced contamination risk - reduces risk of infection - generally non-compliant with lens maintenance - even non-compliant have less risk
life style issues - sports
better VA - for all px - particularly: astigmatic px / irregular astigmatism / low levels of uncorrected cyl with soft CLs
less deposit build up
less surface dehydration
some conditions can only be fitted with GP - only these lenses will work for them as they have irregular corneas - keratoconus / traumatised corneas / post-grafts
what are the potential disadvantages of GPs we need to consider (8)
Initial discomfort - adaption time of 2 weeks - for particularly sensitive corneas 3-4 weeks
Precise fitting required, skill level higher and requires more time to fit - higher risk of loss and of px blinking/rubbing lens out / OZ - flare and glare when blinking
Stringent regulations concerning the use and disinfection of diagnostic lenses
Foreign bodies - will scratch the cornea
Not without complications : 3 & 9 o’clock staining / Lens adhesion / GPC / Corneal warpage
Breakage & scratching - more costly to replace - although a stronger material can be scratched with incorrect cleaning - need good px education
Greasing with some patients
Instability of some materials - parameters can be changed with incorrect cleaning (too much pressure)
what is the most basic of GP designs used
tri curve lenses - base curve (central curve) / secondary/intermediate curve / peripheral curve
Mono- and bicurve lenses can be manufactured but are not often fitted
Curves can be added, called multicurve lenses - can have ones with 6/7 curves etc…
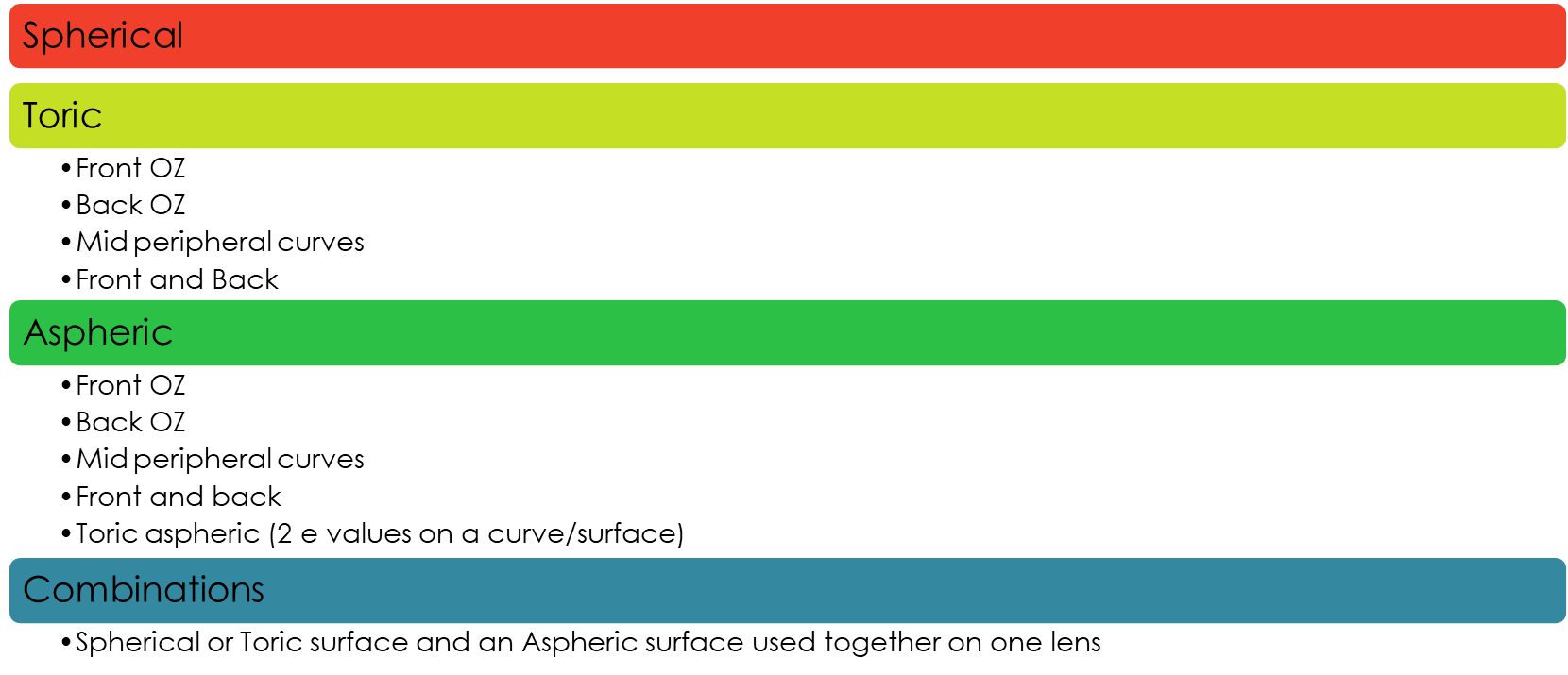
explain how we can customise the parameters (2)
Each surface can be cutomised independently as toric or aspheric or toric aspheric, as can each curve separately - could have a toric base curve but a spheric front curve - designed to fit the shape/curve of the cornea
Objective: measure ocular dimensions to aid in the design of a GP lens
define the parameters in this diagram
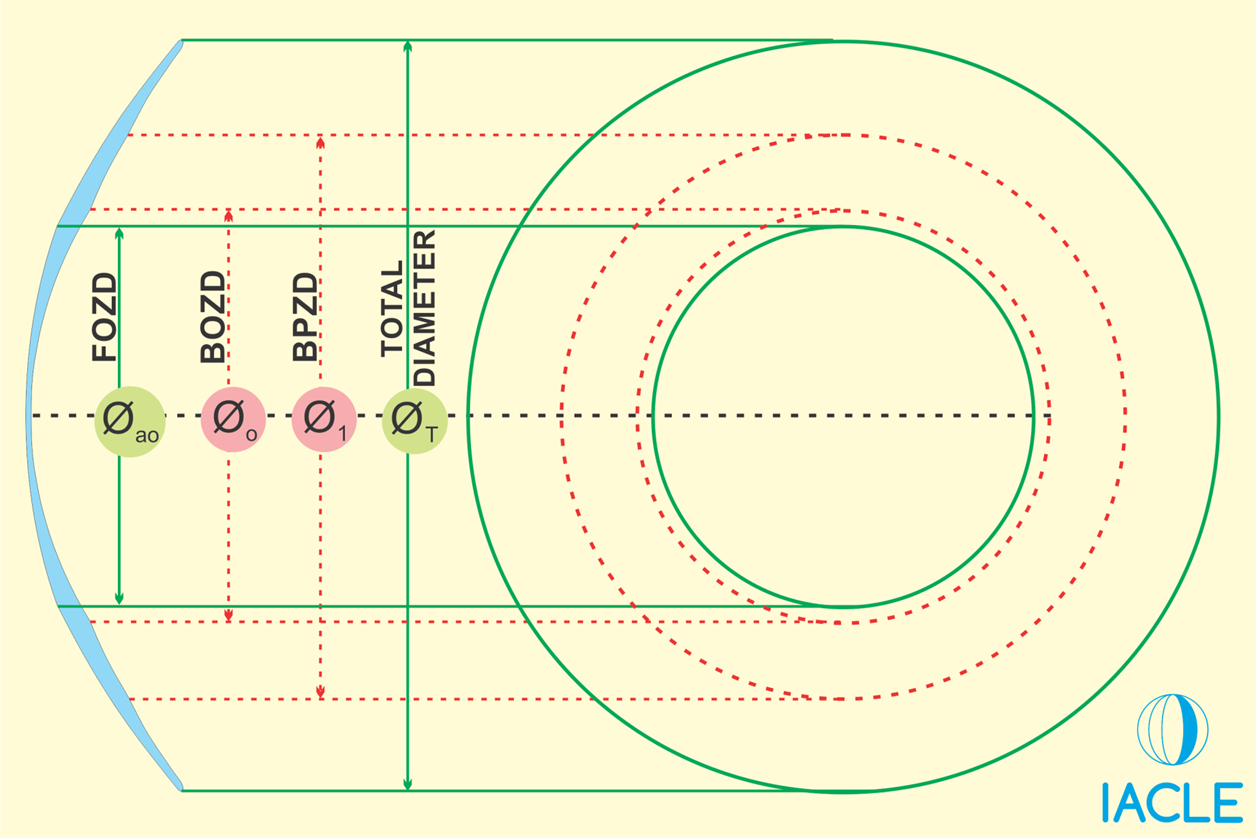
green solid lines - front curves
red dash lines - back curves
optic zone - centre green circle at front and red dash circle at back
total diameter - full width of lens
explain what BOZD, FOZD, and BPZD are
BOZD - back optic zone diameter - diameter of the central back optic zone (the base curve area) - Determines how much of the central cornea is covered by the base curve - affects fit, centration, and tear pattern
FOZD - front optic zone diameter - The diameter of the front optic zone (on the front surface) - Determines the optical area for vision - needs to cover the pupil in all lighting conditions - The usable “seeing” zone on the front of the lens.
BPZD - back peripheral zone diameter - The diameter out to the end of the peripheral curve(s) on the back surface - Controls edge lift - affects tear exchange and comfort - How far the peripheral curves extend from the centre
what is an aspheric surface in terms of eccentricity (3)
a surface that as an e value (eccentricity)
an e value indicates the rate of change of that cornea from central cornea to peripheral cornea
determines the flattening from the center to the periphery
what e value would indicate a cornea is significantly aspheric (2)
0.7 or more
in this case we would match the CL asphericity to the cornea
what would the e value be of a perfectly spheric eye
e value = 0
no asphercity - working with a circle/perfectly round - r value (radius of curvature) is equal on every surface
what is responsible for tear exchange (4)
radial and axial edge clearance
always a tear layer between cornea and lens
size of this gap = clearance
clearance is what allows tears to move in and out under the lens → tear exchange (oxygen + debris removal)
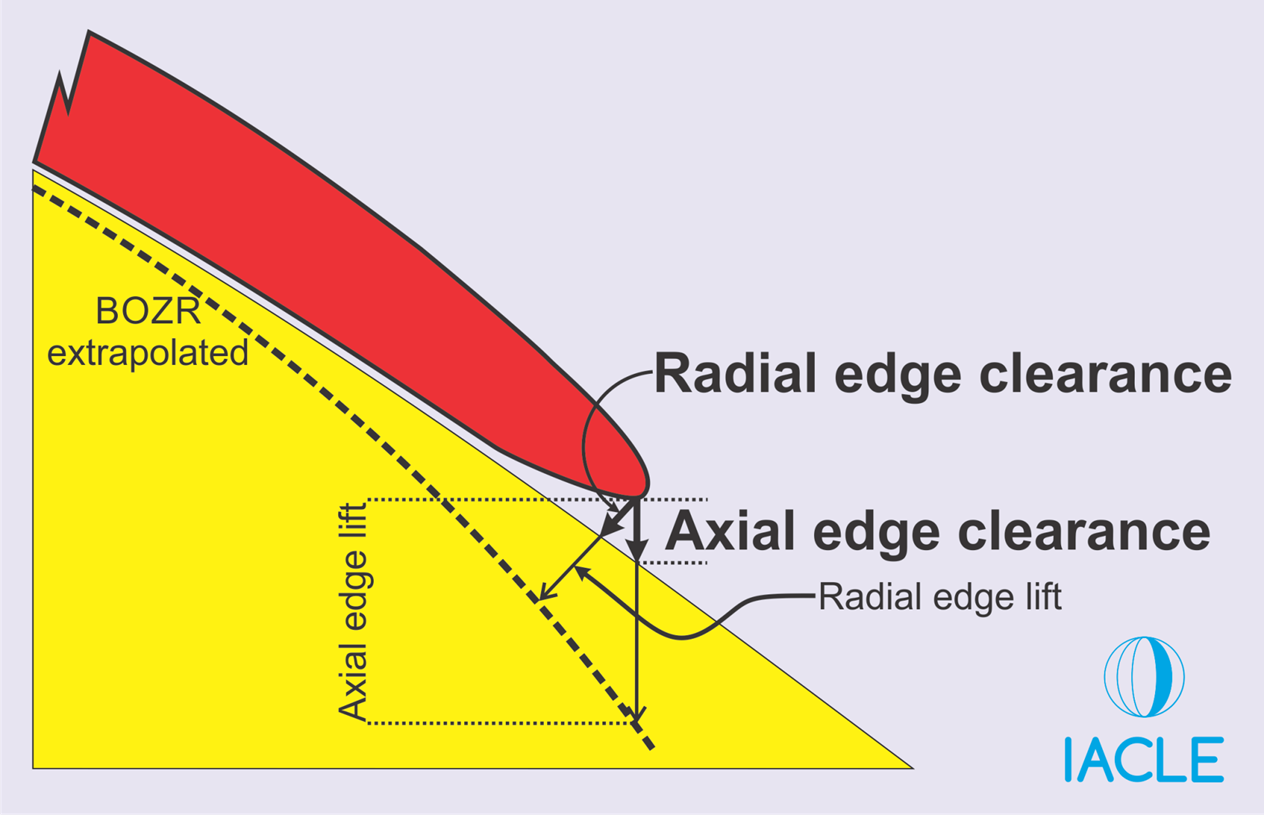
describe the terms radial and axial edge clearance
The terms axial & radial clearance are used to describe the distance between the CL & the cornea for each of the CL zones - this clearance is responsible for tear exchange
axial edge clearance - measured centrally under the BOZD - straight down the OA — too much AC - excessive pooling (steep fit) — too little AC - bearing/touch (flat fit) — bright green pool centrally = increased AC / dark/black touch = decreased AC
radial edge clearance - occurs in mid-peripheral and peripheral zones
explain the relationship between edge lift and tear reservoir
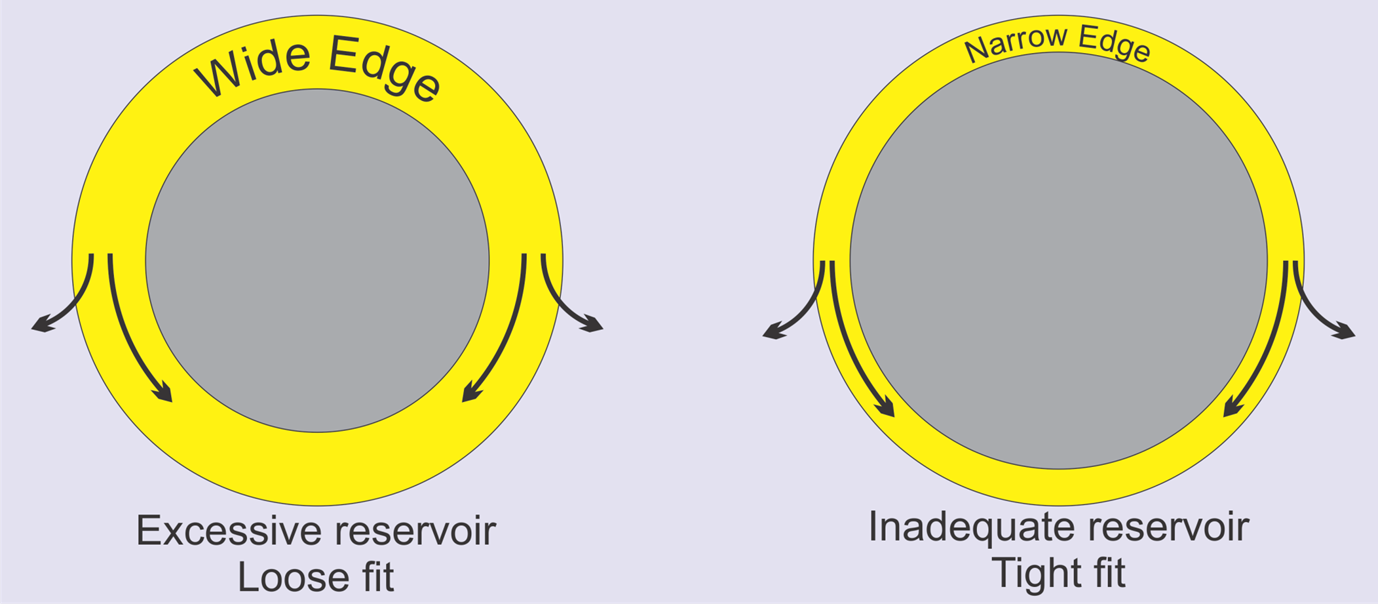
wide edge - increase the volume of tears stored in the reservoir - excessive reservoir - stability of CL fit can be affected adversely - loose fit
with a narrow edge - decrease volume of tears stored in reservoir - inadequate reservoir - tight fit
A balance between these forces is required.
what is the ideal edge lift width
0.2-0.4mm
explain edge shape vs lens comfortability
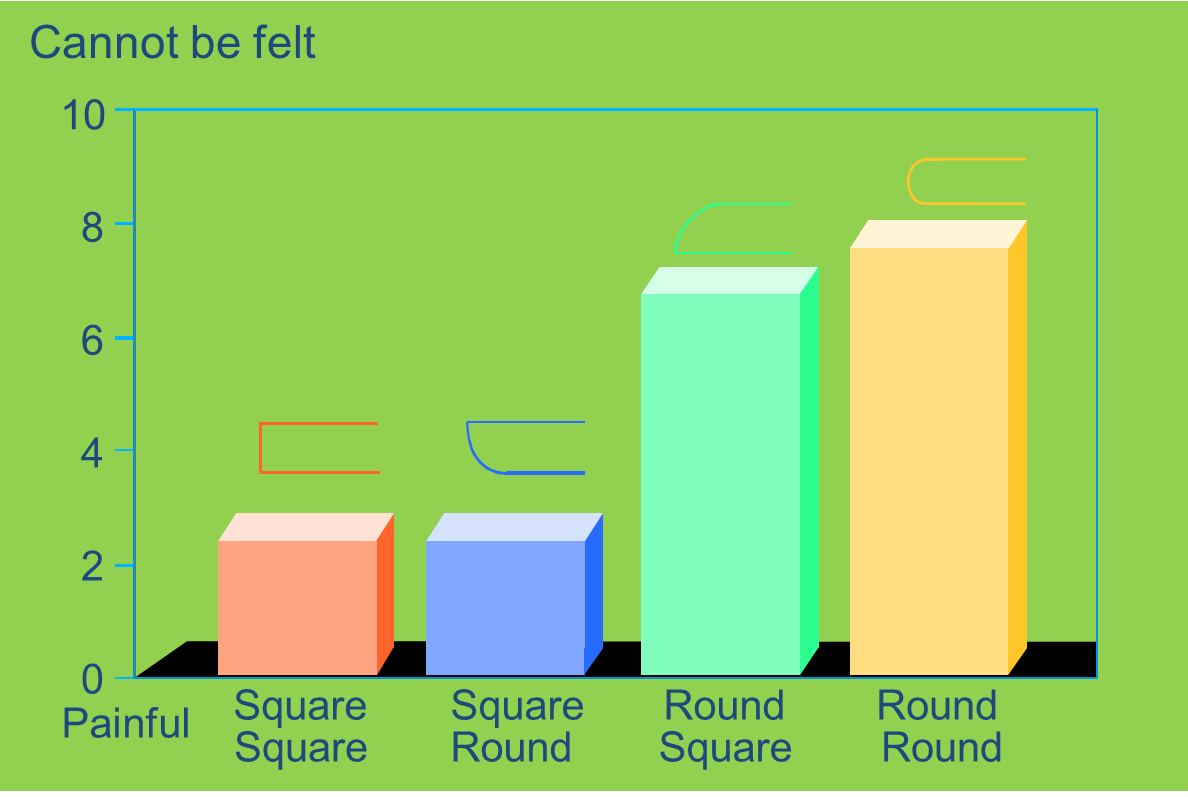
round round is the most comfortable edge shape - however note it is 8/10 - not 10/10 - so can still be felt by the px
what measurements do we need to take when fitting a GP lens (4)
diameters:
BOZD - known as OZ
TD - total diameter
radii:
BC - base curve
e value
how do we obtain the diameter measurements (3:3)
BOZD/OZ:
◦the actual prescription/power is here that the px sees through
◦For this reason, the pupil needs to be inside the OZ
◦Scotopic pupil +1mm (minimum) - average OZ = 7-8mm
TD:
◦HVID-2mm (rule of thumb)
◦The lens is smaller than the cornea
◦Most common is 9.3-9.4mm, up to 10.5mm - more complex the eye larger the TD is
how do we obtain the radii measurements (4:4)
BC:
◦Taken from K readings or SimK
◦Responsible for centration
◦0.1 steeper than flattest K for spherical or low astigmatic eyes - for example k readings of 7.4/7.6 - flattest k is 7.6. 0.1 steeper is 7.6-0.1 = 7.5
◦High astigmatism >=2.5 DC use toric base curve - On flattest K - (bc1) // 1/3(K1-K2)+ Steepest K - (bc2)
E value:
◦Based on topographical overview
◦Aspheric design are meant for alignment fits - very little tear film behind the lens
◦Can mask astigmatism to a greater degree than spherical BC - (up to 4D)
-Often chosen for abnormal or irregular corneas
ordering template for GP lenses
RE | Parameter | LE | Calculation |
BC (radius) | 0.1 steeper than flattest K | ||
OZ (diam) | Scotopic pupil +1mm minimum TD-1.4mm as a maximum | ||
2R | Often 1mm flatter than BC | ||
2CD | OZ + 0.8mm | (TD-OZ)/2 in your design | |
PCR |
| Can alter as per fit, 0.05mm increments Often 1.5mm flatter than secondary curve | |
TD | HVID-2mm as a guideline Manufacturer’s guide selection | ||
gRey for Right eye | Colour | bLue for Left eye | Visitint recommended to differentiate lenses |
Dk/t mid to high | Material | e.g. A brand Boston | Mid Dk/t is sufficient in trials High Dk/t for final lens |
Tear film calc | Prescription | Not related to spectacle refraction | |
e.g. FST | Design | e.g. bitoric | Dependent on visual and fit requirements |
give an example of when we would have to calculate a toric base curve
when high astigmatism - 2.50D+ and if there is a large difference between 2 k readings of 0.4 or more - this is because 0,4mm = 2.50D difference
lens will not fit well - will start to rock - so need to calc curvatures to fit lens better to cornea which is a back surface toric - will have 2 diff curvatures on back surface of OZ
K - RE 7.2/7.7@180 - can see there is a 0.5mm difference
bc1 - will be the flattest k = 7.7
bc2 - 1/3(7.7-7.2) +7.2 = 7.37
example of an order form trial lens
Patient information
◦HVID = 12mm
◦Pupils = 3/5mm
◦K - RE 7.2/7.7@180 / LE 7.4/7.6@180
◦Rx - RE -8.00/-2.50 x 180 / LE -9.00/-0.75 x 180
RE | Calc | Parameter | LE | Calc |
7.7/7.37 | •On flattest •1/3(7.7-7.2) +7.2 | BC | 7.5 | 0.1 Steeper than 7.6 |
6mm | 5+1mm | OZ | 6mm | 5+1mm |
10mm | 12-2mm | TD | 10mm | 12-2mm |
Grey | Colour | Blue | ||
-7.25 | Assuming an alignment fit | Power | -8.00 | Vertex corrected (each eye) |
80+ Dk/t | With tear exchange the requirement for Dk/t is lower | Material | 80+ Dk/t | Your lab will have a choice |
BST | DC= 2.50 lens would rock The front could be adjusted if the lens fitted and the O/R indicated a need for visual improvement | Design | Tricurve | Unlikely to have to adjust either surface for toricity. -0.75 DC will be absorbed by tear film |
what are the different lens designs we can fit (4)
what to order when - explain what the back and front surface are for
back surface is for fit:
BC is designed to follow the cornea
Tear film will fill up any irregularities
Higher corneal cylinder will require a toric back surface – so lens fits cornea better (2.50+)
front surface is for vision:
Once the initial fit for the back surface is determined, the over-refraction will determine if optimal vision is obtained with spheres or spherocylindrical powers
>-0.75 Cylinder over-refraction requires a front surface toric
however - if low vision/irregular cornea – if no visual improvement then do not make front surface toric – as slightly uncomfortable –so if not needed don’t do – need a prism ballast to keep lens at visual axis - added thickness
what is a bitoric design
If the back surface is toric and the front surface is toric, the design is BITORIC
explain the significance of the tear film with hard lenses in comparison to soft contact lenses (4)
In hard lenses in situ - can have a significant tear lens depending on its fitting relationship to the cornea
power the tear film contributes - is enough to add to the optic system – can acc allow us to see very well
If a rigid CL decentres, any tear lens (spherical or sphero-cylindrical) can acquire a prismatic component as well – induced prismatic effect – visual disturbance
however in SCL - soft lens drapes cornea – tear film very thin – in a SCL has no contribution to optics
explain how the BC determines the tear film that is created (3)
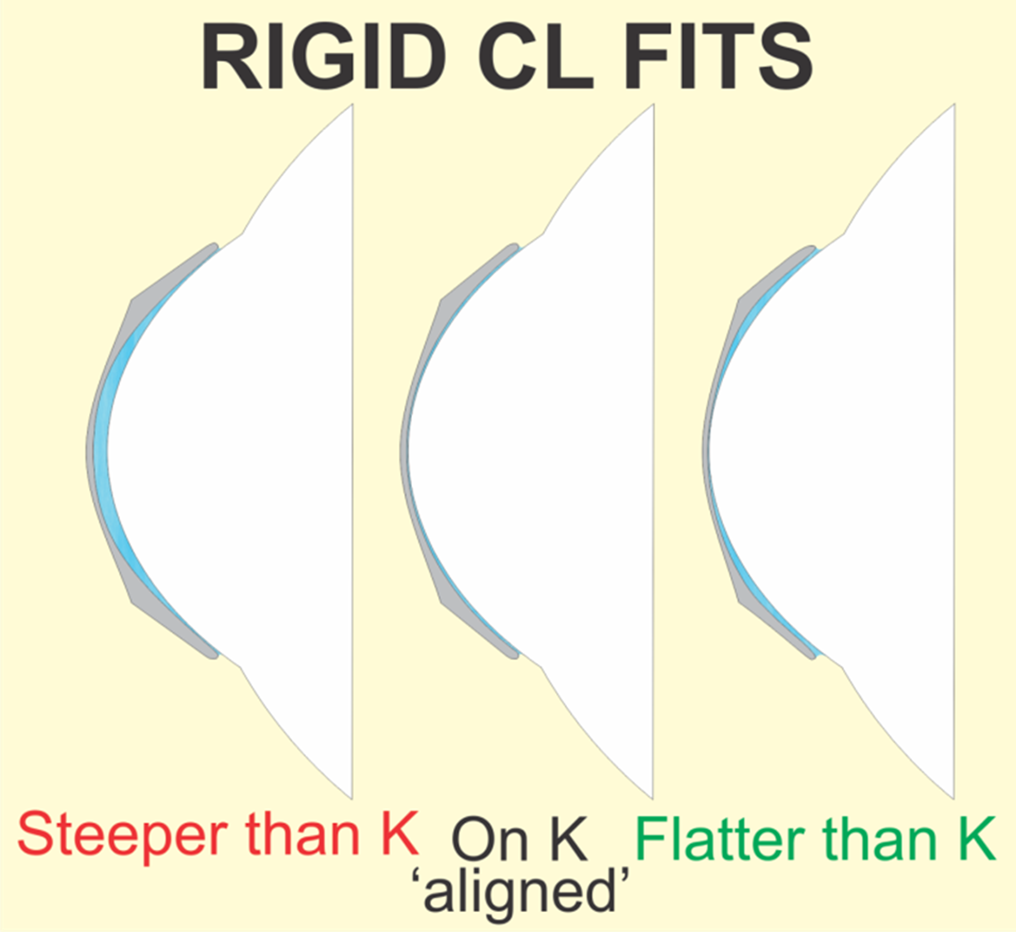
if we choose a lens with BC steeper than K = create a positive power tear layer
alignment fit BC - tear lens same thickness - no significant tear film power
flatter than K = negative power
explain why we usually choose a BC that is steeper in relation to adherence incidence (3)
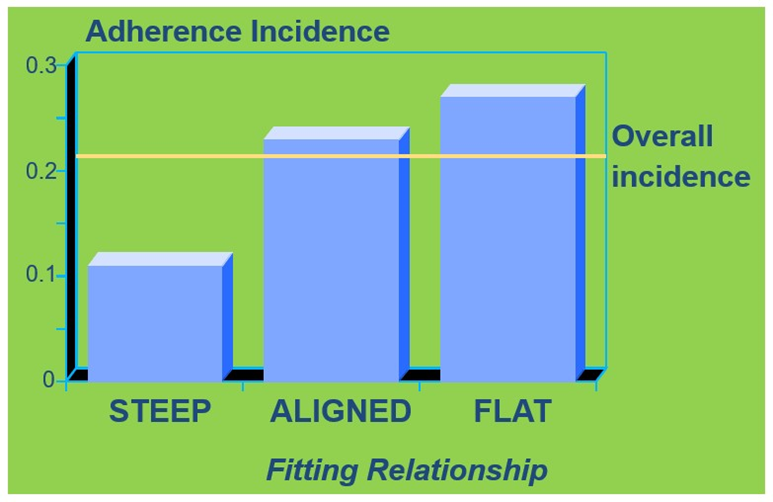
Adherence – lens binds to eye and doesn’t move - we do not want this to be the case - need movement in a lens still
as shown in graph - aligned and flat fit have a higher incidence than steeper
this is why we accept steeper fits to avoid adherence
what is the rule of thumb of the tear lens
When the BOZR of a rigid CL is FLATTENED by 0.05 mm: the tear lens power is altered (decreased) by -0.25D
When the BOZR of a rigid CL is STEEPENED by 0.05 mm: the Tear Lens power is altered (increased) by +0.25D
Additional optical power of opposite sign is required in the CL to off-set the effects of the induced tear lens.
Note: The Tear Lens is treated as being THIN in these calculations
explain how corneal astigmatism is neutralized in relation to the tear lens (4)
base curve of contact lens - back surface can be spherical (the OZ)
this back surface generates the front surface of the tear film power
in this way the tear lens is sphericalised - by the back surface of a spherical rigid CL
These factors combined - a major reduction in corneal astigmatism when a spherical rigid CL is worn - a large amount of corneal astigmatism is absorbed
what are the limits however in neutralizing corneal astigmatism (3)
gross differences in CL & corneal curvatures are dysfunctional/physically unacceptable - cannot have a spherical surface on a largely toric eye - lens will not fit
practical limits apply to the amount of corneal astigmatism that can be corrected by a simple rigid spherical CL
practical limits depend on the topography of the cornea but a limit of about 2.5 - 3.0 D is widely accepted
how much astigmatism is neutralized by a spherical rigid CL (5)
RULE-OF-THUMB: Approximately 90% of anterior corneal astigmatism is neutralised by the presence of a spherical rigid CL.
However, all other sources of ocular astigmatism remain unaltered - astigmatism in other than the cornea
if there is a small amount of astigmatism elsewhere will still come through in the residual astigmatism.
If the anterior cornea is astigmatic but the manifest ocular Rx is spherical - a spherical rigid CL in situ will disclose the ‘internal astigmatism’ as a residual astigmatism - removal corneal component and internal component remains
with an axis at 90 ° to the corneal astigmatism & of about 90% its magnitude (90% of the corneal cylinder magnitude as residual astigmatism)
explain the over refraction of rigid CLs (3)
impossible to separate tear lens power from OR
final rx to order - final fit – only order one lens power which is made up of : Ocular Rx = BVPTrial + Tear Lens Power + Over-Rx
final lens power is comprised of multiple things cannot separate from each other
application of tear film optics - what do we do if we make a BC FLATTER (3)
FAP
◦If you change the BC flatter you will need to compensate for the negative tear lens created by adding plus power to the lens you order
◦FLAT ADD PLUS
◦For every +0.1mm you add to the BC to flatten it, add +0.50 to the script
application of tear film optics - what do we do if we make a BC STEEPER (3)
SAM
◦If you change the BC steeper you will need to compensate for the positive tear lens created by adding minus power to the lens you order
◦STEEP ADD MINUS
◦For every -0.1mm you take away from the BC to steepen it, add -0.50 to the script