Ther III Exam 4 combined
1/250
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
251 Terms
What organs can be transplanted? (6)
heart
lung
kidney
liver
pancreas
intestine
CAUSES OF END STAGE ORGAN DYSFUNCTION
Kidney
Liver
Heart
Lung
Pancreas
Small bowel
HTN, DM
alcoholic cirrhosis, Hep B/C
ventricular failure, viral infxns
COPD, idiopathic pulmonary fibrosis
DM
short bowel syndrome, fx disorders
Living donors are only for ______ and ______ transplants
liver, kidney
IMMUNE SYSTEM
Innate →
Adaptive →
rapid, 1st line of defense
develop highly specific response, “immune memory”
INNATE IMMUNE SYSTEM
Physical → 3
Mechanical → 4
Cells (leukocytes) → 5
skin, GI tract, resp tract
urine flow, tears, saliva, normal flora
macrophages, neutrophils, mast cells, eosinophils, basophil
ADAPTIVE IMMUNE SYSTEM
Things that differentiate the adaptive immune
-
-
ability to _______ via cytokines
________ w each subsequent infxn
specificity
memory
amplify
evolves
ADAPTIVE IMMUNE SYSTEM
2 major arms →
→
Humoral → ABs, complement
cell-mediated → T lymphocytes
CELLS OF THE ADAPTIVE IMMUNE SYSTEM
_________ → specific for individual antigens, initiates T cell activation
_________ → antigen recognition and production of antibodies
T lympho
B lympho
B CELLS CAN DIFFERENTIATE INTO →
plasma cells → AB factories
memory B cells → long term immunity
______________ →
cell surface antigens expressed on all nucleated cells in the body
plays an important role in transplantation, cell interxns, self-recognition
human leukocyte antigens (HLA)
ANTIGEN PRESENTING CELLS → 3
macrophages
dendritic cells
B cells
T CELL ACTIVATION
Requires 3 SIGNALS for activation →
antigen presentation w MHC
co-stim signal CD 80/86
Interxn of IL2 w IL2 receptor
B CELL ACTIVATION →
T cell dependent / independent activation
B cell proliferation + maturation
B cell differentiation → plasma or memory
IMMUNOGLOBULINS (Antibody)
Glycoprotein contains 4 peptide chains
→
→
chains held together by _______ bonds
2 identical heavy chains
2 identical light chains
disulfide
INITIALLY, plasma cells secrete ________
IgM
On SECOND EXPOSURE, memory B lymphocytes predominately produce _______
IgG
IMMUNOGLOBULINS
_____ → long-term immunity
_____ → first antibody secreted post antigen exposure
_____ → in fluid secretions, GI, GU, resp tract
_____ → on mast cells (asthma, hay fever)
_____ → many immune fx, not completely understood
IgG
IgM
IgA
IgE
IgD
TYPES OF IMMUNOSUPPRESSIVE AGENTS
Induction
Maintenance
basiliximab OR thymoglobulin OR alemtuzumab
CNI, antimetabolites, steroids
INDUCTION: Antithymocyte globulin (rATG, Thymo)
Brand →
______ antibodies, directed against ___________
______ agent
Dose: 1.5 mg/kg ___________
Immunosuppressive effects last _______
PREMEDICATION before every dose →
Thymoglobulin
rabbit, T cell surf antigen CD3
depleting
IVPB per dose over a couple of days
months
APAP, diphenhydramine, methylpred
ANTITHYMOCYTE GLOBULIN (rATG, Thymo) ADEs
Cytokine release syndrome →
→
→
→
MONITORING → 4
fever, chills, malaise
leukopenia, TC
skin rash, serum sickness
infxn
CBC w diff, efficacy via ALC, toxicity via WBC & platelets, vital signs during admin
INDUCTION: ALEMTUZUMAB
Brand name →
Monoclonal antibody against _____
______ agent
Dose (off-label) 30 mg __________
t1/2 = 12 days → prolonged _______
Campath
CD52
depleting
IV/SQ during surg
lymphopenia
ALEMTUZUMAB (CAMPATH) ADES
Treatment
Infusion reactions (fever, chill, hypotension, rash, NVD, dyspnea) →
Neutropenia →
Anemia →
Thrombocytopenia →
premed w APAP, diphenhydramine, methylpred
filgrastim
erythropoetin
transfusion
INDUCTION: BASILIXIMAB
Brand name →
Chimerized MAb, ________
__________ agent
Dose: 20 mg __________
ADEs →
Simulect
IL2 receptor antag
non-depleting
IVPB on POD0 + POD4
fewer/less sev, NO CYTOKINE RELEASE SYNDROME
Which induction agent is non-depleting and doesn’t cause cytokine release syndrome?
basiliximab (Simulect)
METHYLPREDNISOLONE
MOA: down regulate cytokine gene expression (in particular, ____) → -T cell proliferation
Redistribution of _______ = -antigen presentation
________ effect
IL2
monocytes (APC)
antiinflam
MAINTENANCE IMMUNOSUPPRESION
Calcineurin inhibitors →
Antiproliferative agents →
Corticosteroids →
mTOR inhibitors →
Costimulation blockers →
tacrolimus, cyclosporine
mycophenolate, azathioprine
prednisone
sirolimus, everolimus
belatacept
CALCINEURIN INHIBITORS (CNIs)
Tacrolimus PO 0.05-1 mg/kg/dose q12h → conversion to IV, SL
Cyclosporine PO 3-5 mg/kg/dose q12h → conversion to IV
Which brand of cyclosporine is non modified form (NOT INTERCHANGEABLE)?
*Dose medications based on _______! (NTI)
IV = ¼ PO, SL = ½ PO
IV = 50% PO over 2-6h cont inf
Sandimmune
levels
CALCINEURIN INHIBITORS ADES
→
→
→
Metabolism →
tacrolimus → hyperglycemia, alopecia, neurotox
both → NEPHROTOX, HTN, infxn, EL abnormalities
cyclosporine → gingival hyperplasia, hyperlipidemia, hirsutism, gout
CYP3A4, Pgp
CYP3A4 INHIBITORS → 6
clarithromycin, erythromycin
azoles
diltiazem, verapamil
protease inhib (-navirs)
grapefruit
CBD products
CYP3A4 / PGP INDUCERS → 4
rifampin
phenytoin
carbamazepine
St john wort
PGP INHIBITORS → 5
clarithromycin, erythromycin
azole
verapamil
amiodarone, dronedarone, propafenone
carvedilol
3A4 / Pgb inhibitors will _____ CNI concentations
inc
3A4 / Pgb inducers will ______ CNI concentrations
dec
ANTIMETABOLITES
Agents =
MOA: inhibit _________
*Dose adjust medications based on _______!
mycophenolate (Myfortic, CellCept), azathioprine (Imuran)
cell cycle prolif
side effects
MYCOPHENOLATE
ADEs → 5
DDIs →
GI upset, leukopenia, anemia, TC, TERATOGENIC
birth control
AZATHIOPRINE
ADEs → 6
DDIs →
leukopenia, anemia, TC, pancreatitis, hepatotox, squamous skin cell CA
allopurinol
MAINTENANCE: STEROIDS
Dose →
ADEs → 4
prednisone 5-10 mg daily
hyperglycemia, HTN, insomnia, +weight
mTOR INHIBITORS
MOA: regulates synthesis of proteins necessary for cell cycle progression from G1 → S phase, blocks IL2 signal transduction → regulates cell growth & proliferation
Agent 1 + dosing →
Agent 2 + dosing →
*Dose medications based on _______!
ADEs → 5
*BBW: +risk of ________ in first 30 days post transplant
DDIs →
sirolimus (Rapamune) → 2 mg PO daily
everolimus (Zortress) → 0.75 mg q12h
levels
TC, anemia, proteinuria, hyperlipidemia, -wound healing
hepatic artery/renal artery thrombosis
CYP3A4, Pgp
What 2 classes are CYP3A4 / Pgp substrates?
CNIs, mTOR
Which class should NOT be used within the 1st month of transplant?
mTOR
BELATACEPT
MOA:
Dosage form:
Frequency: month 0-3 on days 1,5 + weeks 2,4,8 → Month 4-12 ______
**may be used in _________ patients only!!
BBW
costim blocker
IV inf
q 4w
EBV+
lymphomas & other infxns
Which 2 classes has low rejection risk?
CNIs, antimetabolites
Which drug can you not use if you are EBV negative?
belatacept
COMMON IMS REGIMEN
→
→
→
_____ tablets/capsules per day
tacrolimus 3 mg q12h (goal level 8-10) → 3 cap
mycophenolate 1000 mg q12h → 4 tab
prednisone 5 mg daily → 1 tab
15
Consequences of medication noncompliance → 3
acute rejection episodes
organ loss
death
HYPERACUTE REJECTION
within few min - few hours
Result of destruction of transplant by preformed _____ antibodies to donor vascular endothelium
Tissue damage occurs through → 2
IgG
AB-depend cytotox, complement cascade
ACUTE CELLULAR REJECTION
in first few months
Caused by infiltration of allograft by _____
_____ and ______ effect on graft
Gold standard of dx →
Relatively easy to treat →
T cells
inflam, cytotoxic
biopsy of graft
methylpred 500 mg IV daily x3, steroid resistant = thymoglobulin
ANTIBODY MEDIATED REJECTION
more difficult to treat → 4
plasmapheresis
IVIG
rituximab
bortezomib
Pneumocystis jiroveci (PJP OR PCP) PROPHYLAXIS
*Drug of choice to prevent PCP pneumonia →
Doses usually given for ________
Alternatives for prophylaxis → 3
SMX/TMP
6-12m
dapsone, atovaquone, pentamidine
PCP PROPHYLAXIS ALTERNATIVES comments
Dapsone
Atovaquone
Pentamidine
check G6PD def (hemolysis dose related), monitor CBC weekly x6m then q6m
take w high fat meal, anemia/neutropenia
bitter/metallic taste
DRUG OF CHOICE TO TREAT PCP →
Alt tx choices →
SMX/TMP → add prednisone if pAO2<70
dapsone, atovaquone
VIRAL RISK STATUS FOR CYTOMEGALOVIRUS (CMV)
In Donor / Recipient format
High risk
intermediate risk
low risk
(+/-)
(+/+), (-/+)
(-/-)
CYTOMEGALOVIRUS (CMV)
Prophylaxis agent 1 + risk use →
Prophylaxis agent 2 + risk use →
valganciclovir → high + intermed
letermovir → high
Letermovir is ineffective against HSV, must co-administer with _______
acyclovir
CYTOMEGALOVIRUS (CMV) TREATMENT
Preferred for severe tissue invasive CMV →
Preferred for CMV viremia →
Refractory CMV → PO → special note
Refractory CMV → IV → special note
ganciclovir
valganciclovir (V for viremia)
maribavir → drug assoc dysgeusia
cidofovir, foscarnet → avoid if possible due to nephrotox
FUNGAL PROPHYLAXIS
Center specific based on risk
_________ 5 mL swish & swallow TID → preventing oral and esophageal candidiasis
_________ 200 mg daily → risk of invasive fungal infxns, must account for DDIs
nystatin
fluconazole
Which class do you dose based on side effects?
antimetabolites (mycophenolate, azathioprine)
Which type of rejection episode is treated with IV methylprednisone?
A. hyperacute
B. acute cellular
C. antibody mediated
B
ETIOLOGY OF CANCER
Carcinogenesis → the 4 steps
initiation → irrevers
promotion → REVERSIBLE
conversion → irrevers
progression → irrevers
which step of carcinogenesis is reversible?
promotion
CARCINOGENS
Lifestyle → 4
Environmental → 2
Chemical → 3
Infectious agents → 4
smoking, alc, UV light, high fat diet
UV radiation, ionizing radiation
immunosupp drugs, certain antineoplastics, coal tar
hep B/C, HIV, HPV, H pylori
6 HALLMARKS OF CARCINOGENESIS
_________ sustaining proliferative signaling
_________ evading growth suppressors
_________ activating invasion & metastasis
_________ enabling replicative immortality
_________ inducing angiogenesis
_________ resisting cell death
oncogenes
tumor supp genes
hematogenous & lymphatic spread
telomerase & senescence
VEGF
oncogenes & tumor supp genes
Protooncogenes (precursor of oncogene)
Examples → 4
RAS, EGFR, HER2, VEGF
Tumor suppressor genes
Examples → 2
retinoblastoma (Rb), BRCA1/2
__________ → location of tumor is not specified
agnostic
________ intent: long term remission, no recurrence
________ intent: improve symptoms, QoL, and overall survival
curative
palliative
Following applies to SOLID tumors (eg breast, lung, colon)
__________ therapy: given BEFORE definitive tx (usually surgery) → purpose
__________ therapy: given AFTER definitive tx → purpose
These terms generally apply to __________ (ie. resectable) disease only
neoadjuvant → shrink tumor
adjuvant → prevent recurrence
non-metastatic
Following apply to HEMATOLOGIC malignancies
________ therapy (given first) → induce remission w no visible evidence of cancer
________ therapy (start after ^) → eradicate any remaining cancer cells
________ therapy → prevent recurrence
induction
consolidation
maint
WHICH IS TRUE OF THE NCCN GUIDELINES?
A. They are strictly evidence-based
B. They are updated frequently
C. They only contain guidelines for treatment of cancer
D. They require a paid subscription
B
T or F:
THE NCCN GUIDELINES ARE THE ONLY GUIDELINES AVAILABLE FOR THE ONCOLOGY SETTING.
F
WHICH CLASS OF DRUGS IS NOT AN IMMUNE CHECKPOINT INHIBITOR (ICI)?
A. CTLA-4 inhibitor
B. CD-19 inhibitor
C. PD-1 inhibitor
D. PD-L1 inhibitor
B
WHICH IS MOST CORRECT REGARDING THE ONSET OF ICI-INDUCED IRAES?
A. During IV infusion
B. Within weeks after starting therapy
C. 1-2 days after starting therapy
B
WHICH ORGAN SYSTEM MAY BE AFFECTED BY IRAES?
A. Hepatic
B. Dermatologic
C. Endocrine
D. All of the above
D
STEROIDS MAY BE USED FOR TREATMENT OF WHICH IRAE?
A. Hypothyroidism
B. Hyperglycemia
C. Dermatitis
C
WHICH IS TRUE REGARDING STEROID TAPERING IN PATIENTS WITH ICI-INDUCED IRAES?
A. Taper should begin after one week of therapy, regardless of symptom control
B. Taper may be rapid (over 1-2 weeks)
C. Taper should be slow (over at least 4 weeks)
C
WHICH IS NOT A CHRONIC STEROID TOXICITY?
A. Osteoporosis
B. Infection
C. Leukocytosis
D. Cataracts
C
2 most commonly used PD-1 inhibitors →
Type
nivolumab (Opdivo), pembrolizumab (Keytruda)
IgG
CHECKPOINT INHIBITORS: ADEs
IrAEs →
Onset: within _______ of starting therapy, sometimes delayed up to 1 year
May affect _____ organ systems
_______ associated with more severe IrAEs than PD-1 or PD-L1 inhibitors
^ _____ inhibitor
immune-related AEs
weeks-3m
multiple
ipilimumab
CTLA4
IRAEs SYSTEMS INVOLVED (most common)
Pulmonary
Endocrine
GI
Skin
Liver
pneumonitis
hypothyroid, hypophysitis, hypopituitarism, adrenal insuff
colitis
pruritus, rash
transaminitis, hepatitis
IRAES MANAGEMENT
IrAEs may require treatment with _________
DO NOT USE FOR …
corticosteroids
hypothyroid, hyperthyroid, hyperglycemia
IRAES MANAGEMENT
Grade 1 mild
Grade 2 moderate
Grade ¾ sev-life threatening
consider holding immunotherapy, loperamide, Lomotil, hydration, close monitor
HOLD, pred/methylpred
HOLD, consider DC, methylpred, if no improv add infliximab or vedolizumab
TUMOR GROWTH MODELS
__________ model is the most established
Caveat: assumes all cancers are _________ to treatment and that resistance to treatment & metastases do not occur
__________ = proportion of actively dividing cells
__________ = amount of time it takes for 1 cell or group to divide / double in size
__________ = certain % of cancer cells that will be killed with each course of chemo
Tumor growth is _______
Gompertz
equally responsive
growth fraction
doubling time
cell kill hypothesis
exponential
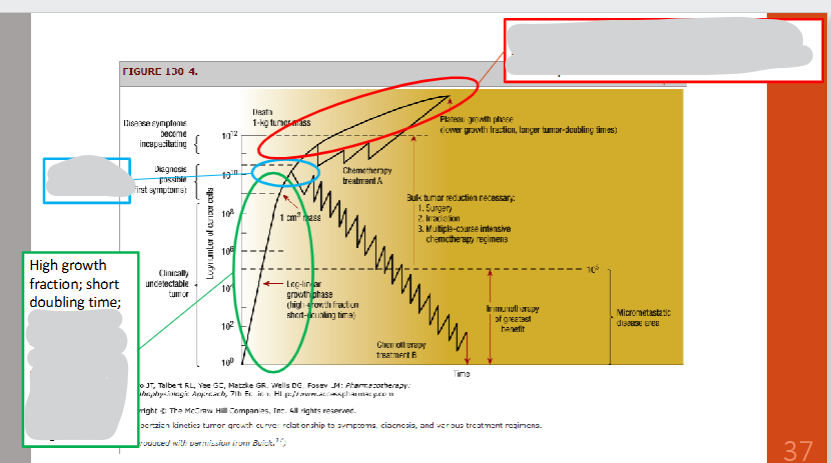
TUMOR GROWTH MODEL SUMMARY
Green oval
Blue oval
Red oval
Downward zig zag → chemo is often continued after tumor is undetectable to ensure a maximal # of cells are killed and to prevent recurrence
high GF + short DT → chemo most effective, tumor less likely dx
clinically detectable → ideally dx tumors before they reach this size
-GF + longer DT → chemo less effective
cell kill hypothesis
Patient with acute leukemia achieves a complete remission after his first cycle of chemo. Which term describes this chemotherapy?
A. adjuvant
B. induction
C. consolidation
B
(leukemia = hematologic
first cycle = induction)
Patient with metastatic breast cancer receives her first line of chemotherapy. Which term describes this chemotherapy?
A. adjuvant
B. induction
C. consolidation
D. none of the above
D
(neoadjuvant)
Which occurs the EARLIEST in the process of carcinogenesis?
A. conversion
B. promotion
C. progression
B
LUNG CANCER COMPARISON
NON-small cell lung cancer (NSCLC)
Proportion of lung cancers
Natural history
Therapy response
Pathology
Smokers
Actionable molecular alterations?
85-95%
slower, 50% metastases
mod sens to radiation, low sens to chemo
adenocarcinoma > squamous cell > large cell
+incidence of squamous cell
YES
LUNG CANCER COMPARISON
Small cell lung cancer (SCLC)
Proportion of lung cancers
Natural history
Therapy response
Pathology
Smokers
Actionable molecular alterations?
10-15%
faster, 60-70% metastases, death in 2-4m w/o tx
high sens to radiation/chemo (but responses do not last)
classical SCLC
higher incidence > NSCLC
NO
LUNG CANCER RISK FACTORS
_________ exposure
_________
_________
Occupational/environmental exposure (petroleum, nickel, arsenic, etc)_________ disease (PF, COPD, asthma)
_________
tobacco
asbestos
ionizing radiation
lung
genetics
UNITED STATES PREVENTIVE SERVICES TASK FORCE (2021)
Screening Guidelines
______
______
______
age 50-80
>20 pack yr hx
current smoker or quit w/in 15 yrs
NO
(15 pack year hx, quit 20 yrs ago)
LUNG CANCER S/S
6 →
Laboratory abnormalities → 4
SCLC →
____________ syndrome (tumors pressing on/blocking the vein causing swelling in face/neck/upper body + breathing difficulties)
cough, -weight, dyspnea, chest pain, hemoptysis (coughing up blood), hoarseness
hyperCa, anemia, leukocytosis, TC
SIADH, cushing’s
superior vena cava
TREATMENT MODALITIES FOR NSCLC/SCLC
________
________ (RT)
Systemic therapy →
Systemic therapy →
Systemic therapy →
surgery
radiation therapy
chemo → plat doublet (cisplatin/carboplatin + another chemo agent)
Checkpoint inhib (CPI)
Targeted therapy → NSCLC ONLY
NSCLC TREATMENT (NON-SMALL)
Stage I, II, III (resectable)
Treatment of choice =
Higher risk patients will also receive neoadjuvant and/or adjuvant therapy →
Higher risk patients will also receive neoadjuvant and/or adjuvant therapy → if EGFR +
Higher risk patients will also receive neoadjuvant and/or adjuvant therapy → if ALK +
surgery
plat doublet ± CPI, or CPI
osimertinib ± plat doublet
alectinib
NSCLC TREATMENT (NON-SMALL)
Stage III (unresectable) →
Plat doublet + RT followed by durvalumab or osimertinib x 1yr
NSCLC TREATMENT PEARLS
DO NOT USE … for SQUAMOUS non-small cell lung cancer → why?
DO NOT USE … for SQUAMOUS non-small cell lung cancer → why?
pemetrexed (Alimta) → not effective
bevacizumab (Avastin & biosimilars) → pulm hemorrhage
NSCLC TREATMENT PEARLS
For metastatic disease + PD-L1 expression > 50%, _______________ is an option
prolongs survival and is less toxic compared to platinum doublet chemo
CPI monotherapy (eg. pembrolizumab / Keytruda)
PLATINUM AGENTS
Higher incidence of … ADEs (dose-limiting side effect)
→ 3
cisplatin → ototox, nephrotox, NV
carboplatin → myelosupp
oxaliplatin → PN
CISPLATIN-INDUCED NEPHROTOXICITY
Risk factors → 2
PREVENTION → 3
TREATMENT →
concomitant nephrotoxins (NSAIDS!), lack of adequate hydration
avoid cisplatin, hydration (pre + post cisplatin), avoid nephrotoxins
DC cisplatin, supp care
PEMETREXED
Brand name =
MOA: __________ targets TS, DHFR, GARFT
EFFECTIVE FOR __________ ONLY (eg. adenocarcinoma)
ADEs + prevention →
→
Alimta
antifolate
NON squamous
hematologic, vomiting/diarrhea → folic acid, vit B12
skin rash → dexamethasone