General gynae
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
Bacteria that commonly cause pre pubertal vaginal discharge
group A streptococcus (gram positive cocci)
How does ectopic ureter present in prepubertal girls?
clear watery discharge
other congenital abnormalities
What is a disulfiram reaction?
When metronidazole is taken with alcohol it interferes with the break down causing nausea, dizziness
Antibiotics treatment for PID
cetriaxone 1g IM or 2g IV
metronidazole 400 mg BD for 14 days
doxycycline 100mg BD for 14 days
Risk of infertility after PID
10% after one episode
20% after two episodes
Sign of TOA on ultrasound
Cogwheel
trichomonas vaginalis - presentation, diagnosis and management
Presentation - yellow frothy discharge, strawberry cervix
Diagnosis - microscopy
Management - metronidazole
What is a medical term for genital warts
condylomata accuminata
What vaccine is used for HPV and what types does it protect from?
Gardasil 9
6, 11, 16,18
31, 33, 45, 52, 58
Management of chlamydia - pregnant and non pregnant
Non - pregnant
doxycycline 100mg BD for 7 days or azithromycin
Pregnant
azithromycin 1g stat then 500mg OD for 2 days
What type of bacteria is gonorrhoea? diagnosis and management
gram -ve diplococci
diagnosis - NAAT
management - ceftriaxone 1g stat
Definition and causes of ophthalmia neonatum
conjunctivitis in newborn
first 5 days - gonorrhoea
after 5 days - chlamydia
couple of weeks - herpes
What is the causative organism of chancroid and presentation?
haemophilis ducreyi
Presentation
painful ulcers
lymphadenopathy
buboes (abscess)
Commonest cause of abnormal vaginal discharge?
bacterial vaginosis
What is the oral and topical management of bacterial vaginosis?
oral metronidazole 400mg BD for 7 days
or topical metronidazole gel 0.75% OD for 5 days
or topical clindamycin 2% OD for 5 days
What is the most common causative agent of candida?
candida albicans in 80%
What is the treatment of candida in acute presentation in pregnant and non pregnant?
Non pregnant - fluconazole 150mg PO stat
in pregnant - clotrimazole pessary 200mg for 3 days
What is the treatment of recurrent candida in pregnant and non pregnant?
In non pregnant
fluconazole 150mg PO x 3 every 72 hours
then fluconazole 150mg PO once a week for 6 months
In pregnant
imidazole pessary for 7 days
clotrimazole 500mg PV once a week
Diagnosis of PCOS
Rotterdam criteria
irregular cycles >35 days
hyperandrogegism - either clinical or biochemical high testosterone
ultrasound >20 follicles on one or more than 10 on both
high AMH used in young adults
first line medical management for PCOS in woman not wanting pregnancy
BMI<25
BMI >25
BMI<25 - COCP or mirena
BMI >25 - COCP + metformin
medical management for PCOS in woman wanting pregnancy - 1st 2nd and 3rd line
letrozole
clomiphene + metformin
gonadotrophin
WHO aim of cervical cancer eradication - number of cases
<4 cases per 100,000
What is the current global uptake of cervical cancer and what is the aim?
current 21%
aim 90%
What is the management of ovarian cysts in post menopausal women
<3cm no need to follow up
RMI <200, cyst 3-5cm, asymptomatic - follow up in 4-6 months
RMI <200, cyst >5cm or symptomatic - BSO
RIM > 200 - MDT + CTAP
chance of malignancy in pre menopausal ovarian cysts
3 in 1000
Tumour markers in pre menopausal cysts and when
if < 40yo and complex cyst
Ca 125, LDH, HCG, AFP
percentage of negative endometrial biopsies that will have endometrial hyperplasia
2%
Risk of endometrial cancer
hyperplasia without atypia in 20 years
hyperplasia with atypia in 20 years
<5%
29%
Patient with endometrial hyperplasia without atypia declines mirena, next line management and dose
continuous progesterone norethisterone 10-15mg/day
if endometrial hyperplasia without atypia is managed with continuous progesterone what is the follow up?
biopsy in 6 months, repeat biopsy in 6 months - should be two negative
then annual follow up
What is the follow up for women with endometrial hyperplasia with atypia who refuse TAH + BSO but agree to IUS
biopsy every 3 months until two negative biopsies
then every 6-12 months until hysterectomy
Woman with endometrial hyperplasia with atypia who wants to conceive has IUS, what is the follow up and when should she conceive?
biopsy every 3 months until 1 negative biopsy , if negative then IVF
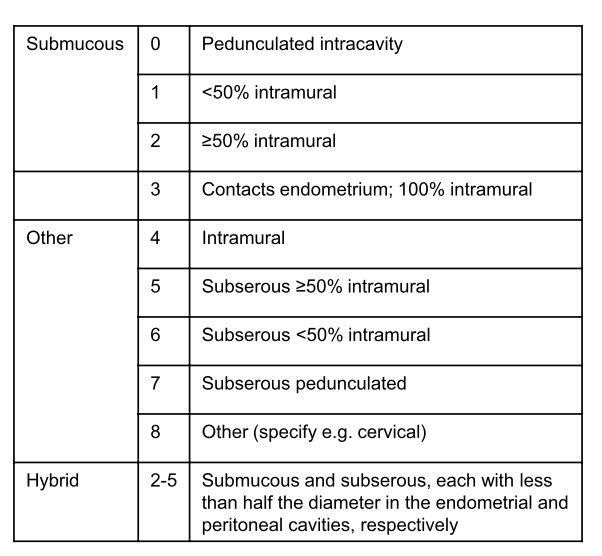
Classification of fibroids
mode of action of TXA
prevent plasminogen to plasmin
What is the most common malignant ovarian cyst in adolescents? How does it present?
Juvenile granulose cell tumour
oestrogen secreting so precocious puberty
Tumour markers:
granulosa cell tumour
epithelial tumour
sertoli leydig (2)
embryonal (2)
dysmerginoma (2)
yolk sac
immature teratoma
granulosa cell tumour - oestrogen
epithelial tumour - CA 125
sertoli leydig (2) - testosterone and AFP
embryonal (2) - HCG and AFP
**dysmerginoma (2) - LDH and HCG
yolk sac - APF
immature teratoma - AFP and LDH
post menopausal woman with PMB but thin endometrium on scan what is the chance of cancer?
0.5%
Incidence of PMS normal vs severe
40% of women
5% severe
Diagnosis of PMS
symptom diary for 2 months or
GnRH analogue for 3 months will help symptoms
Management of PMS
- CBT, exercise, Vitamin B6
continuous drospirenone COC
low dose 10mg SSRI
higher dose SSRI
oestrogen patches with micronised progesterone
GnRH analogue 6 months + HRT - ensure DEXA
TAH + BSO + HRT ensure DEXA
Criteria name to diagnose IBS
Rome IV
Endometrioma wanting to conceive
spontaneous - cystectomy but might effect reserve
ART - offer IVF without cystectomy
Endometriosis findings on TVUS
ground glass echogenecity
absence of solid components
no papillary projections
Dose of progesterone in cyclical vs continuous HRT? What is the first and second steps if unscheduled bleeding takes place?
cyclical - 200mg OD for 2 weeks
increase to 3 weeks
if lasts for more than 3 months and ET >7mm - biopsy
continuous - 100mg OD
increase to 200mg OD
if lasts > 6 months and ET>4mm - biopsy
Treatment of lichen sclerosis
topical clobetasol 0.05% or betamethasone 0.05%
Most common causes of veno-venous and veno arterial ECMO
veno-venous
acute respiratory distress syndrome
veno arterial
pulmonary embolism
myocardial infarction
adolescent <16 lacks capacity, who can consent for treatment?
one parent or legal guardian is enough to sign
however if parent refuses treatment , act in the best interest of patient
McCune Albright syndrome
precocious puberty
cafe au lait spots
at what figo classification of fibroids should myomectomy be in 2 stage surgery
stage 2 > 50% intramural
ryeqo mode of action and side effect
GnRH antagonist
osteoporosis
When using oxytocin in labour how should hyponatraemia be managed?
125-130
80ml per hour fluid intake
VBG in 4 hours
<125
30 ml per hour
VBG in 2 hours
stop oxytocin