4. adapted from quizlet: ryanef123 MMCP 11 - Pulmonary Disease (Dr. Stephens)
1/176
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
177 Terms
What are some concerns?
- HPI: Pt is a 65 year old male presenting for new patient exam. He recently moved to the area and is in need of a new dentist. He reports that he has no dental concerns. You note that the patient has a cough.
- PMH: “Nothing that you need to worry about”
- PSH: Denies
- FH: NC
- Med: “An inhaler for when I get short of breath”
- Social: 2 drinks/night, 1 pack per day smoker, denies rec. drugs
- ROS: “I feel fine”
- Vital Signs: P: 110 BP: 128/88 O2 sat: 90%
EOE
- Well nourished
- No Facial Asymmetry
- Extraocular movements intact, no jaundice
- No facial masses
- Trachea midline
- Neck is soft with normal range of motion
- No Lymphadenopathy
- “Barrel chest” appearance
- Fingernail clubbing and yellow discoloration
IOE
- No gingival edema or erythema
- Floor of mouth is soft and flat
- No erythro/leukoplakia
- Uvula midline
- "Barrel chest" appearance
- Fingernail clubbing and yellow discoloration
- Tongue per image
ID the condition:
- Pulmonary disorders characterized by chronic airflow limitation from the lungs that is not fully reversible
- Presence of cough, sputum production, and dyspnea together with an abnormal measurement of lung function
Chronic obstructive pulmonary disease (COPD)
What are the two conditions that fall under COPD?
- Chronic Bronchitis
- Emphysema
What condition associated with chronic inflammation of the bronchi?
- Produces excessive tracheobronchial mucus production (at the bronchial level)
- Persistent cough with sputum for at least 3 months in at least 2 consecutive years in a patient in whom other causes of productive chronic cough have been excluded
Chronic Bronchitis
What has permanent enlargement of the air spaces in the lung (distal to the terminal bronchioles) that is accompanied by destruction of the air space (alveolar) walls without obvious fibrosis?
Emphysema
The diagnosis of COPD is the presence of what three things in addition to abnormal measurement of lung function?
- Cough
- Sputum production
- Dyspnea
What is the third leading cause of death worldwide?
Chronic obstructive pulmonary disease (COPD)
COPD affects ___% of adults
5%
COPD is more common in _______, but more deadly in _______
Women, men
ID the condition:
- High rate of long term disability and functional impairment
- - Second only to arthritis
- Prevalence, incidence, and hospitalization rates increase with age
- Average dental practice of 2000 patients is estimated to have about 100 patients who experience features of this
Chronic obstructive pulmonary disease (COPD)
What is the most important cause of chronic obstructive pulmonary disease (COPD)?
Tobacco smoking
(Smoking accounts for 85-90% of COPD deaths)
Despite the increased risk, only about one in five chronic smokers develops COPD. This suggests _______ susceptibility plays a role production of inflammatory mediators
Genetic
Besides smoking, what are two other risk factors for developing COPD?
- Long term exposure to occupational or environmental pollutants
- Alpha-1 antitrypsin deficiency
What is a type of enzyme inhibitor that protects tissues from enzymes of inflammatory cells, especially neutrophil and elastase?
Alpha-1 antitrypsin
ID if the following is a characteristic of Emphysema or Chronic Bronchitis:
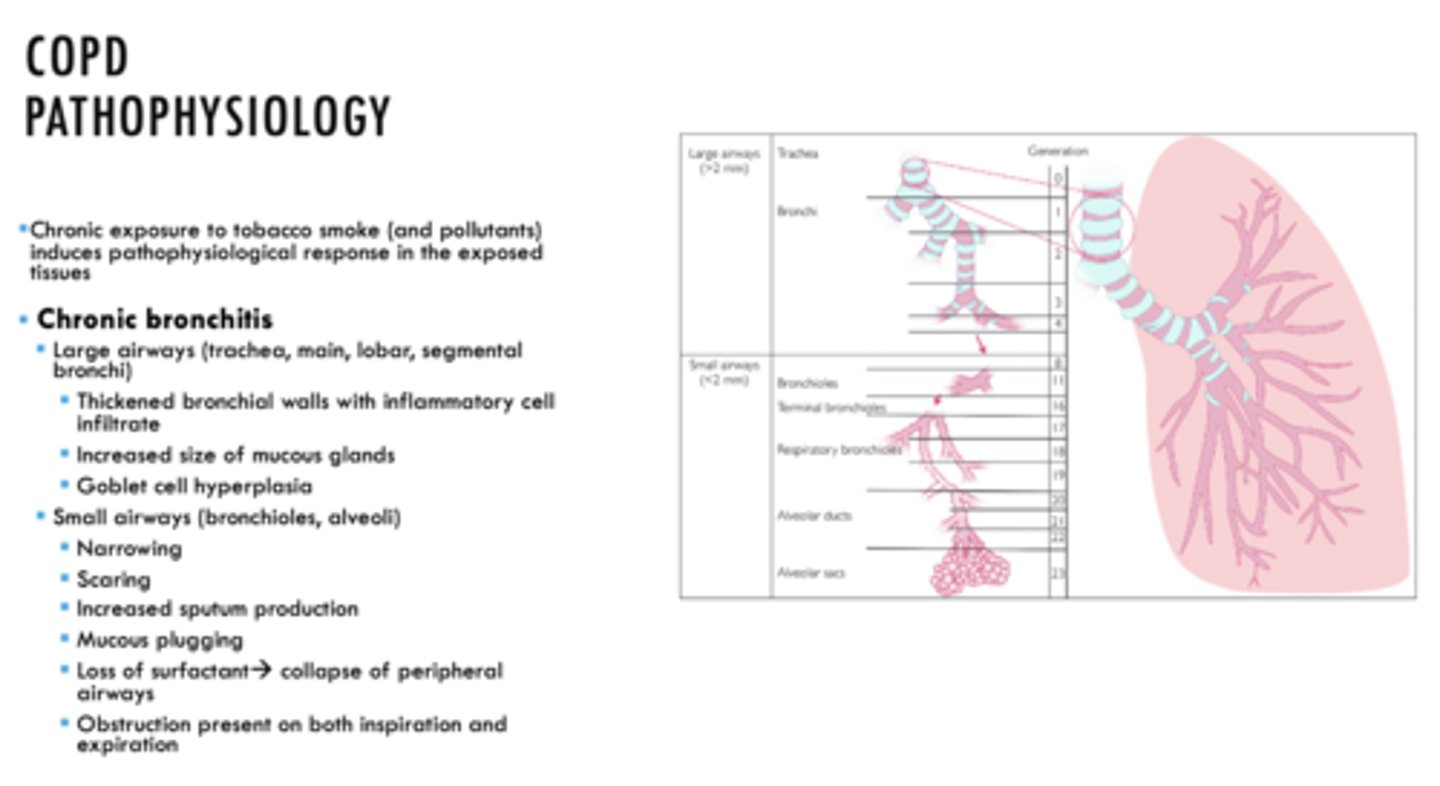
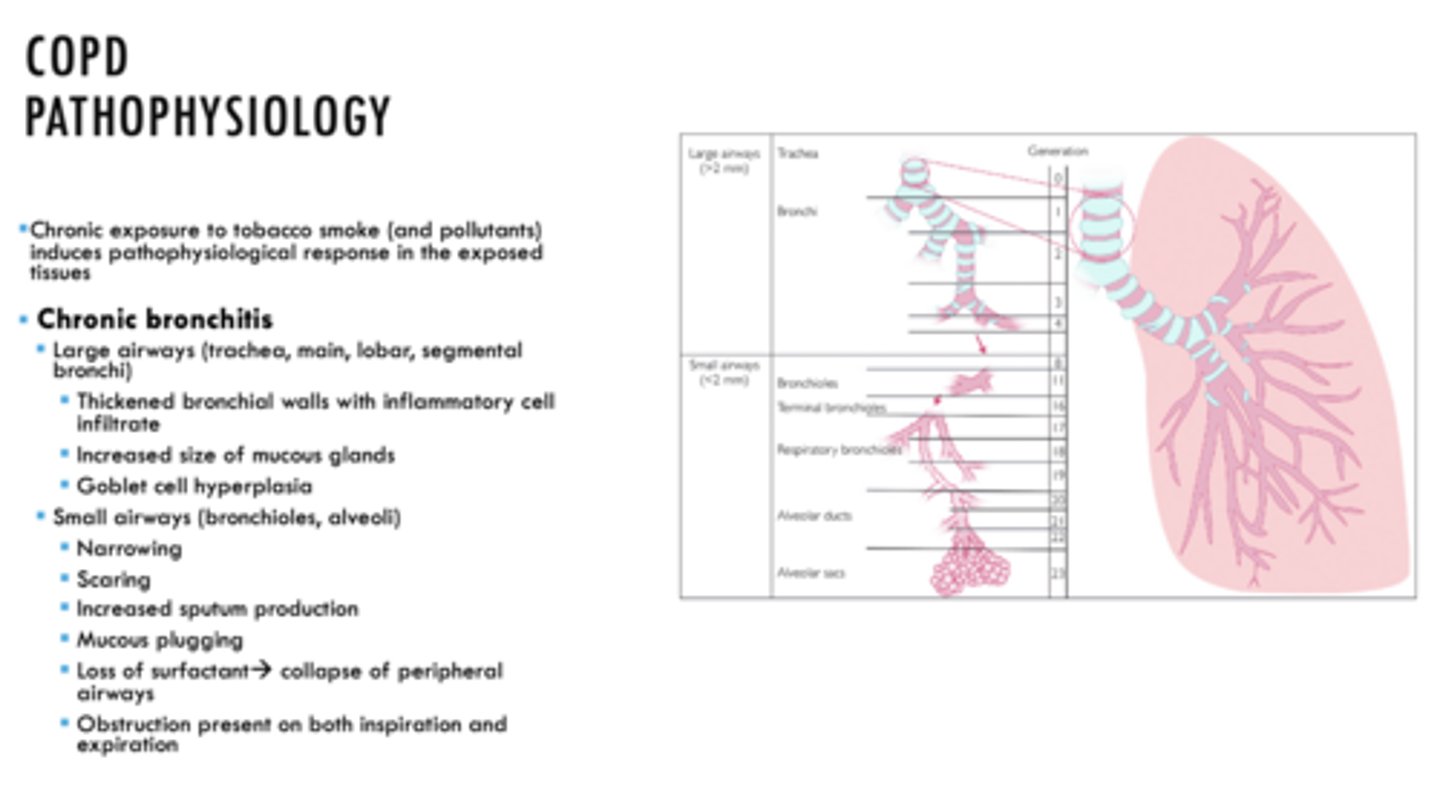
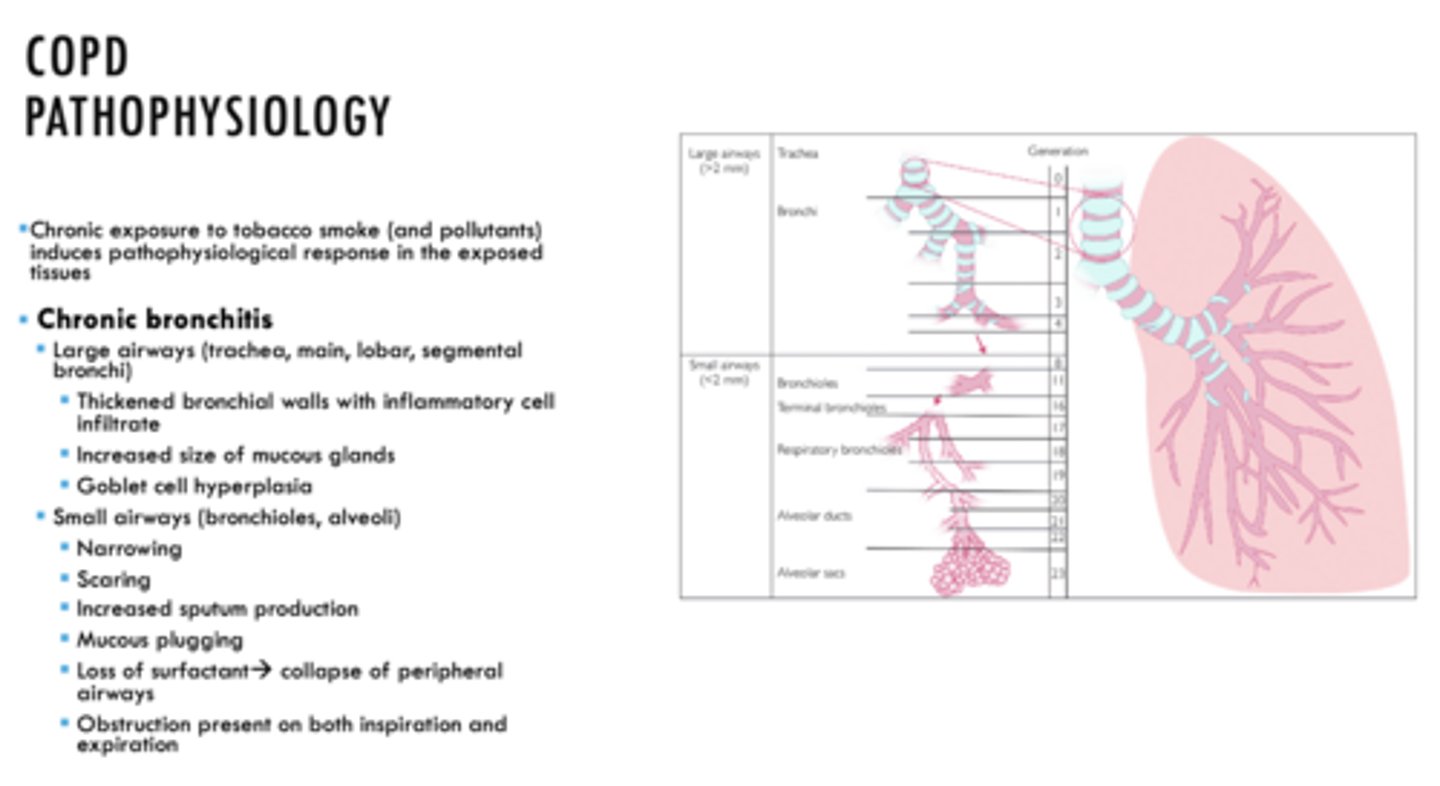
- In LARGE AIRWAYS (trachea, main, lobar, segmental bronchi)
- Thickened bronchial walls with inflammatory cell infiltrate
- Increased size of mucous glands
- Goblet cell hyperplasia
Chronic Bronchitis
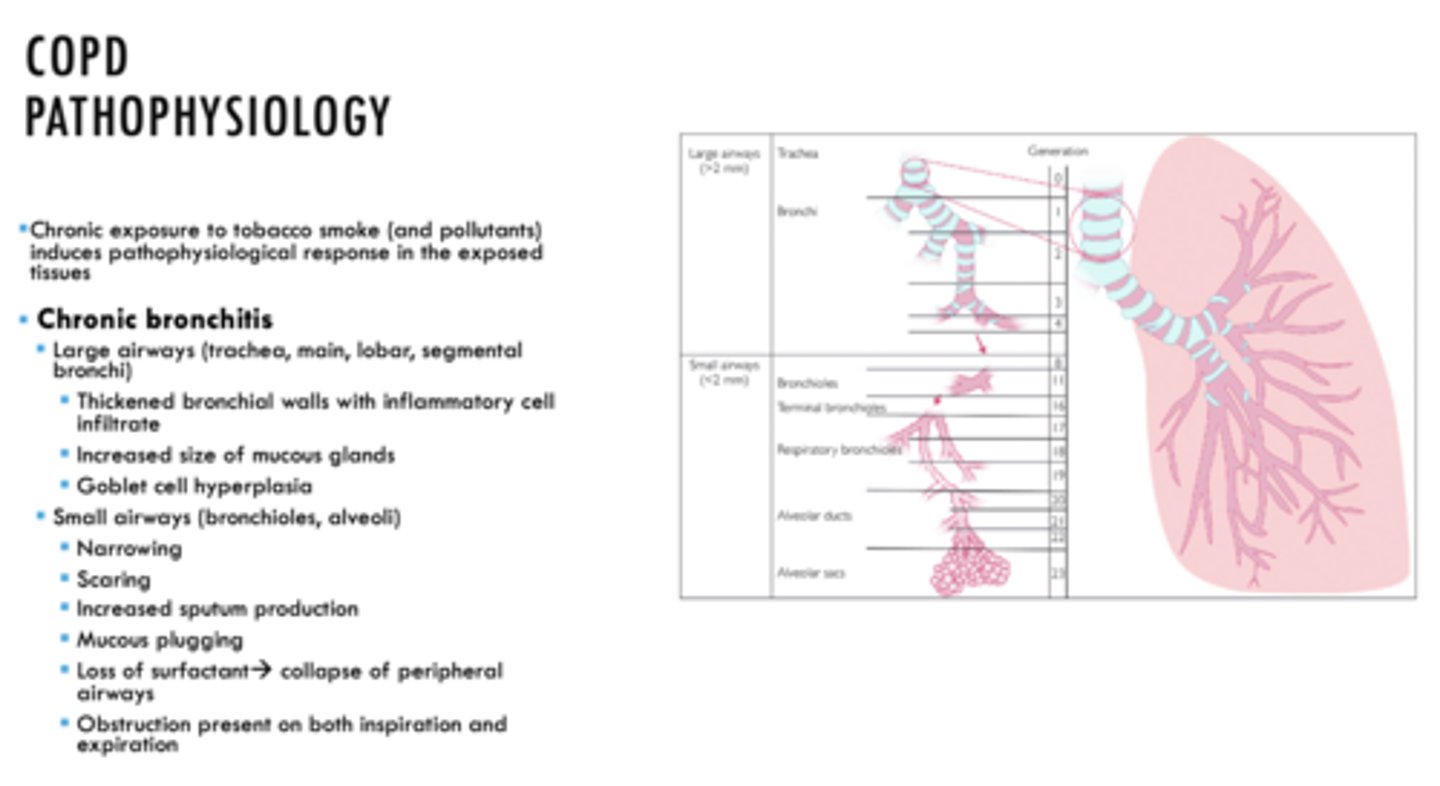
ID if the following is a characteristic of Emphysema or Chronic Bronchitis:
- Small airways (bronchioles, alveoli)
- Narrowing
- Scaring
- Increased sputum production
- Mucous plugging
Chronic Bronchitis
ID if the following is a characteristic of Emphysema or Chronic Bronchitis:
- In small airways, loss of surfactant causing collapse of peripheral airways
Chronic Bronchitis
ID if the following is a characteristic of Emphysema or Chronic Bronchitis:
- In small airways, obstruction present on both inspiration and expiration
Chronic Bronchitis
ID if the following is a characteristic of Emphysema or Chronic Bronchitis:
- Pathophysiological changes occur due to damage to lung parenchyma
- Obstruction results from collapse of unsupported and enlarged airspaces
Emphysema
ID if the following is a characteristic of Emphysema or Chronic Bronchitis:
- Damage to alveolar epithelium causing release of inflammatory mediators, attraction of activated macrophages and neutrophils which activate the release of elastase enzyme causing destruction alveolar walls
Emphysema
ID if the following is a characteristic of Emphysema or Chronic Bronchitis:
- Destruction of alveolar walls results in
- Enlarged airspaces distal to terminal bronchioles
- Loss of elastic recoil of lung
Emphysema
ID if the following is a characteristic of Emphysema or Chronic Bronchitis:
- Obstruction is evident on expiration
Emphysema
COPD shows progressive deterioration with periodic exacerbations. What is the key to improving outcomes of COPD?
Early intervention
The following are complications related to what?
- Continued exposure to pathogen à progressive dyspnea and hypercapnia to the point of debilitation
- Recurrent pulmonary infections (H. influenzae, M. catarrhalis, S. pneumoniae) common with bronchitis
- Acute exacerbations managed with Abx
- Pulmonary HTN requiring oxygen supplementation
- - Failure to manage --> cor pulmonale (R heart failure)
- Emphysema --> enlarged air spaces, thoracis bullae, pneumothorax
- Poor quality of sleep due to nocturnal hypoxia
- Coexisting HTN, ischemic heart disease, arrythmia, heart failure, MI, muscle wasting, osteoporosis
Site of damage for COPD
All of the following are signs and symptoms of COPD EXCEPT:
- Progressive, slow onset,usually beginning after age 40
- Hypertension
- Dyspnea
- Worsens with exercise
- Weight loss and decreased exercise capacity
- Cardiovascular disease
- Respiratory infections
- Osteoporosis
- Fractures
Hypertension
What is the initial symptom of COPD?
Cough
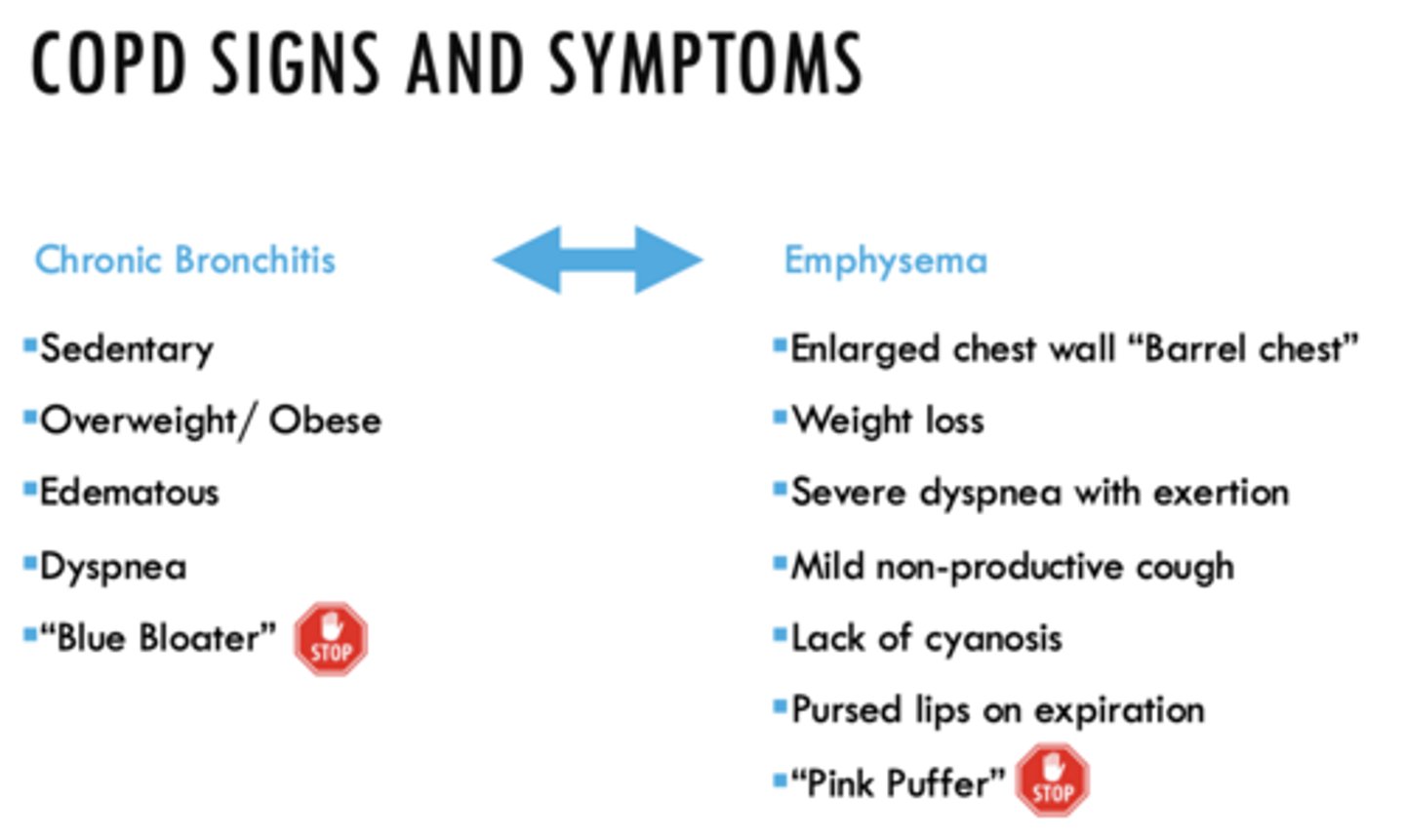
ID if the following sign/symptom is a characteristic of Emphysema or Chronic Bronchitis:
- Sedentary
Chronic Bronchitis
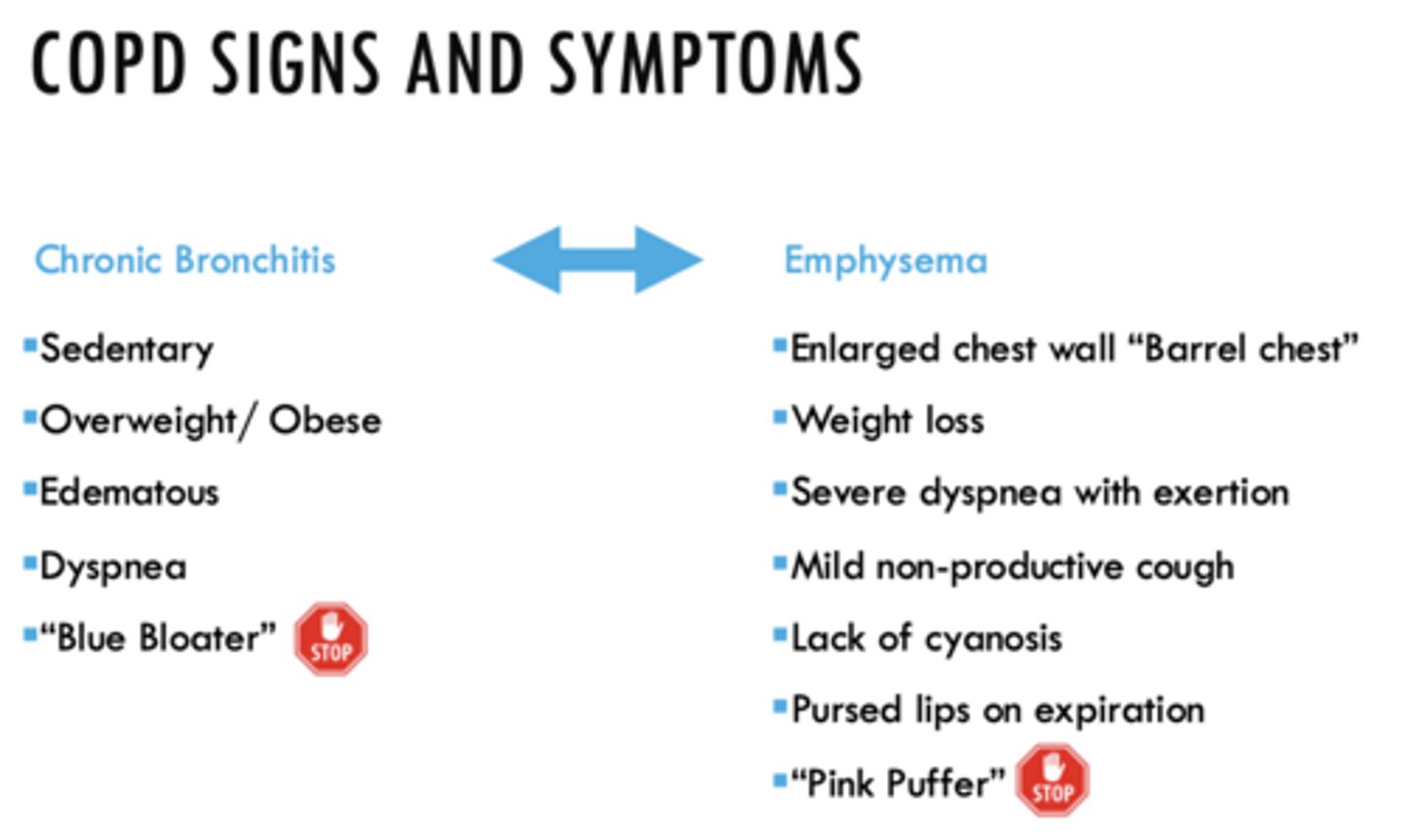
ID if the following sign/symptom is a characteristic of Emphysema or Chronic Bronchitis:
- Overweight/ Obese
Chronic Bronchitis
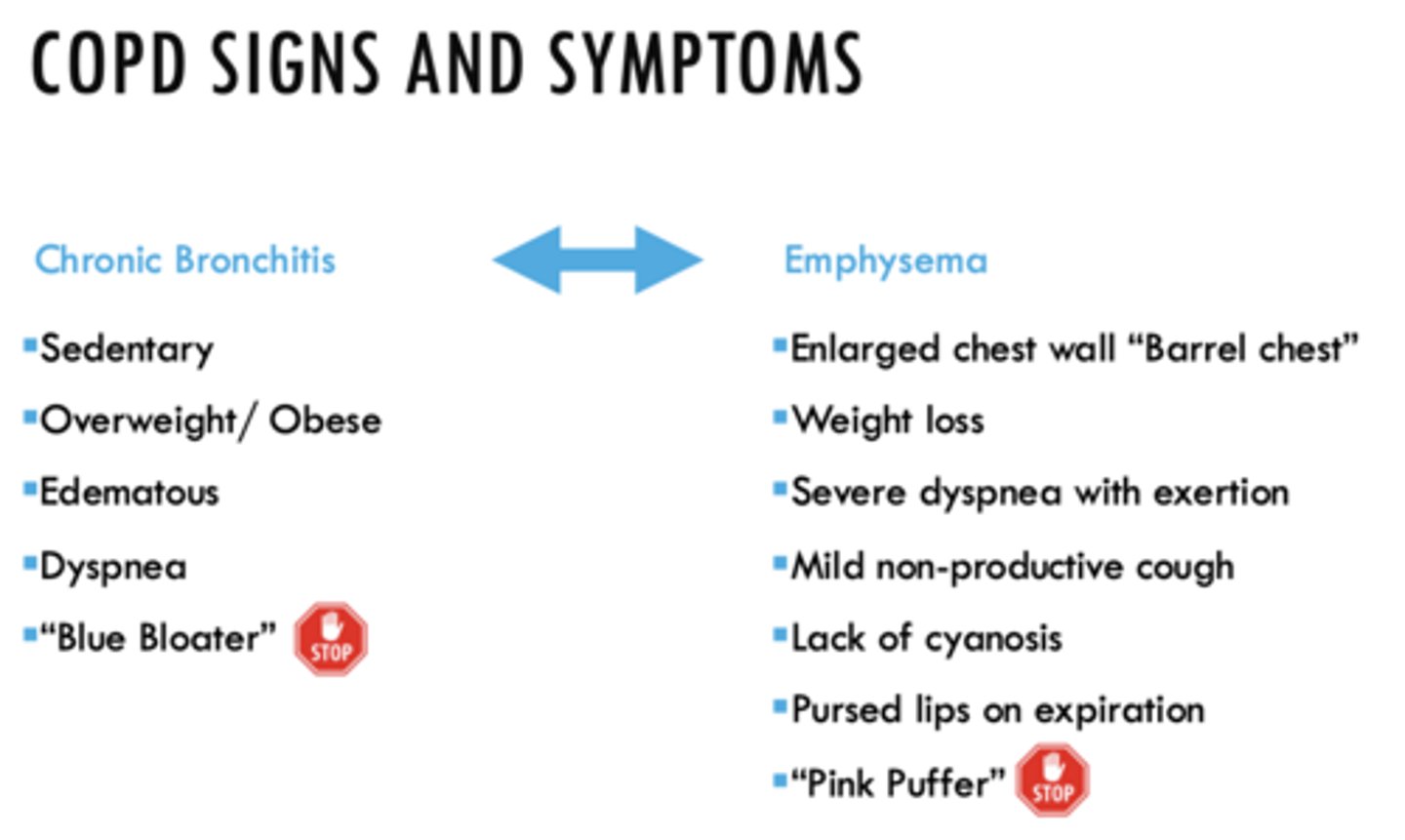
ID if the following sign/symptom is a characteristic of Emphysema or Chronic Bronchitis:
- Edematous
Chronic Bronchitis
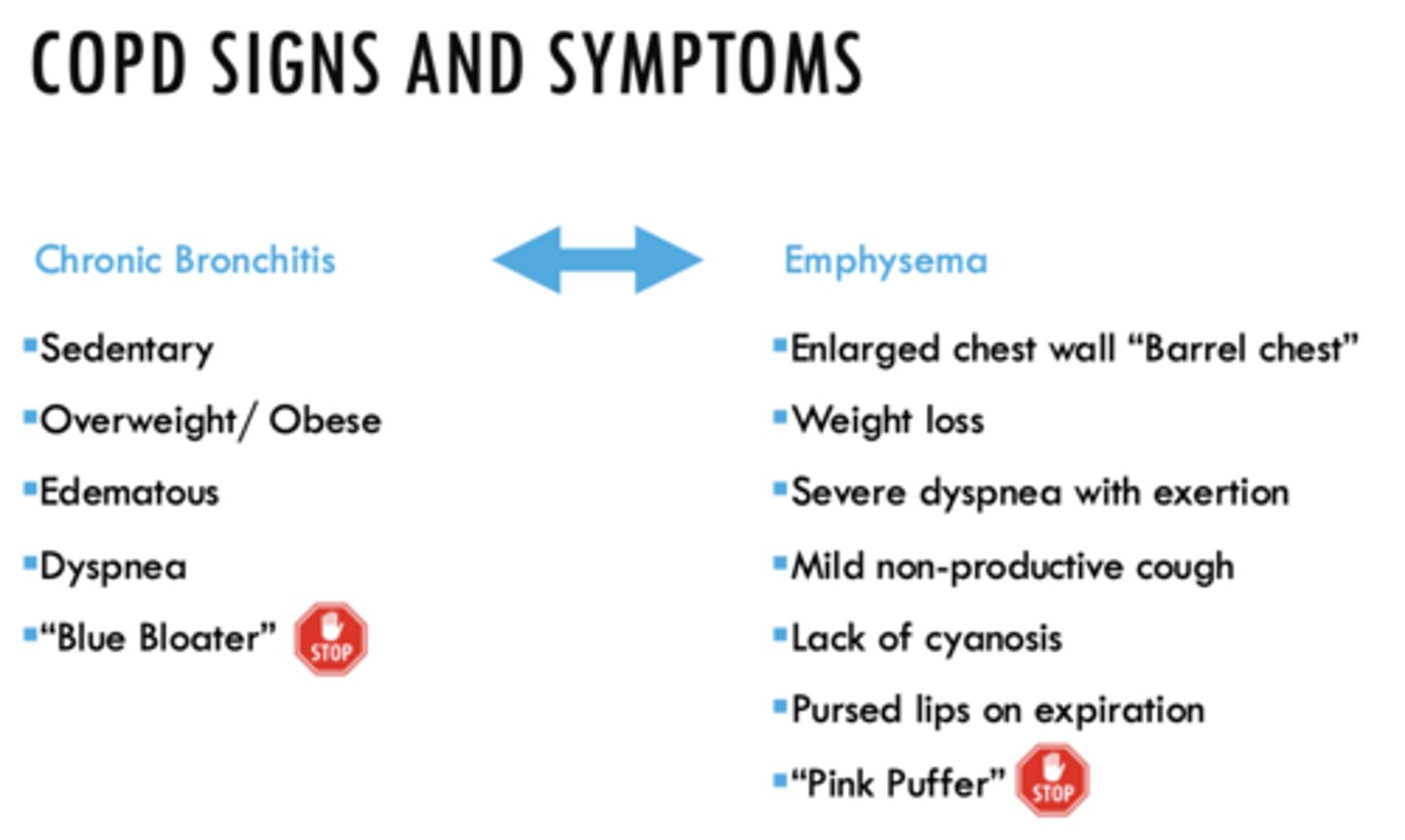
ID if the following sign/symptom is a characteristic of Emphysema or Chronic Bronchitis:
- Dyspnea
- “Blue Bloater”
Chronic Bronchitis
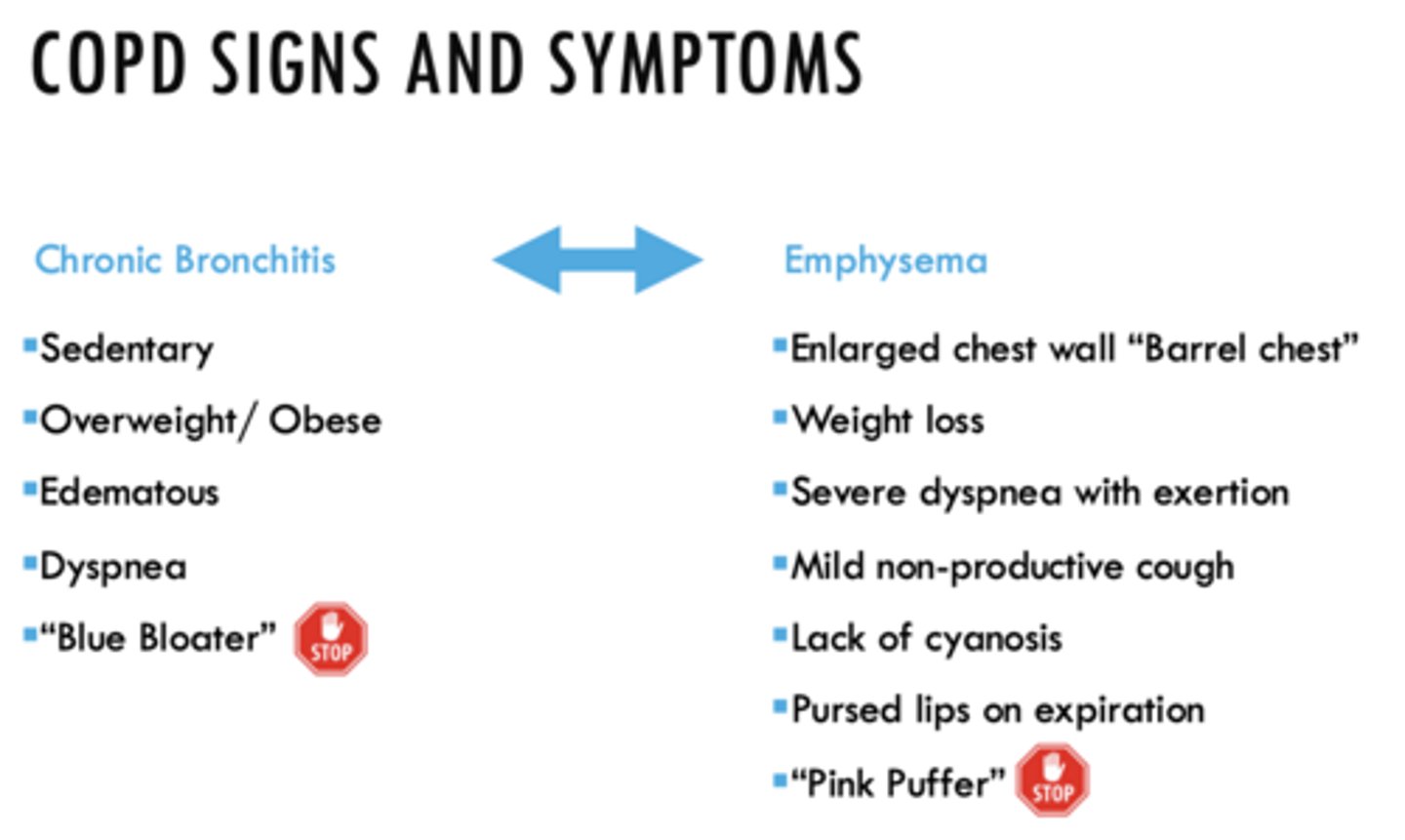
ID if the following sign/symptom is a characteristic of Emphysema or Chronic Bronchitis:
- Enlarged chest wall “Barrel chest”
Emphysema
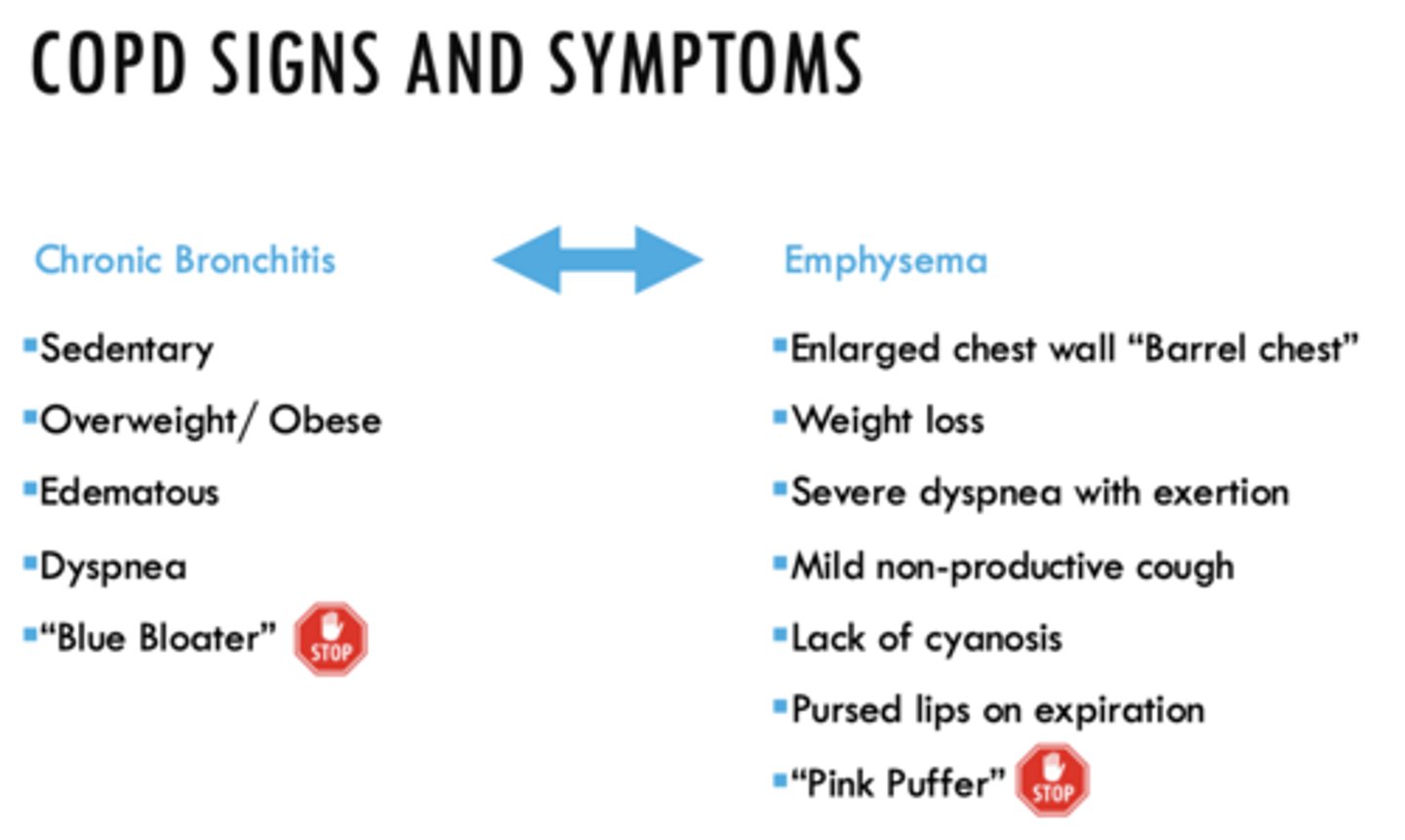
ID if the following sign/symptom is a characteristic of Emphysema or Chronic Bronchitis:
- Weight loss
Emphysema
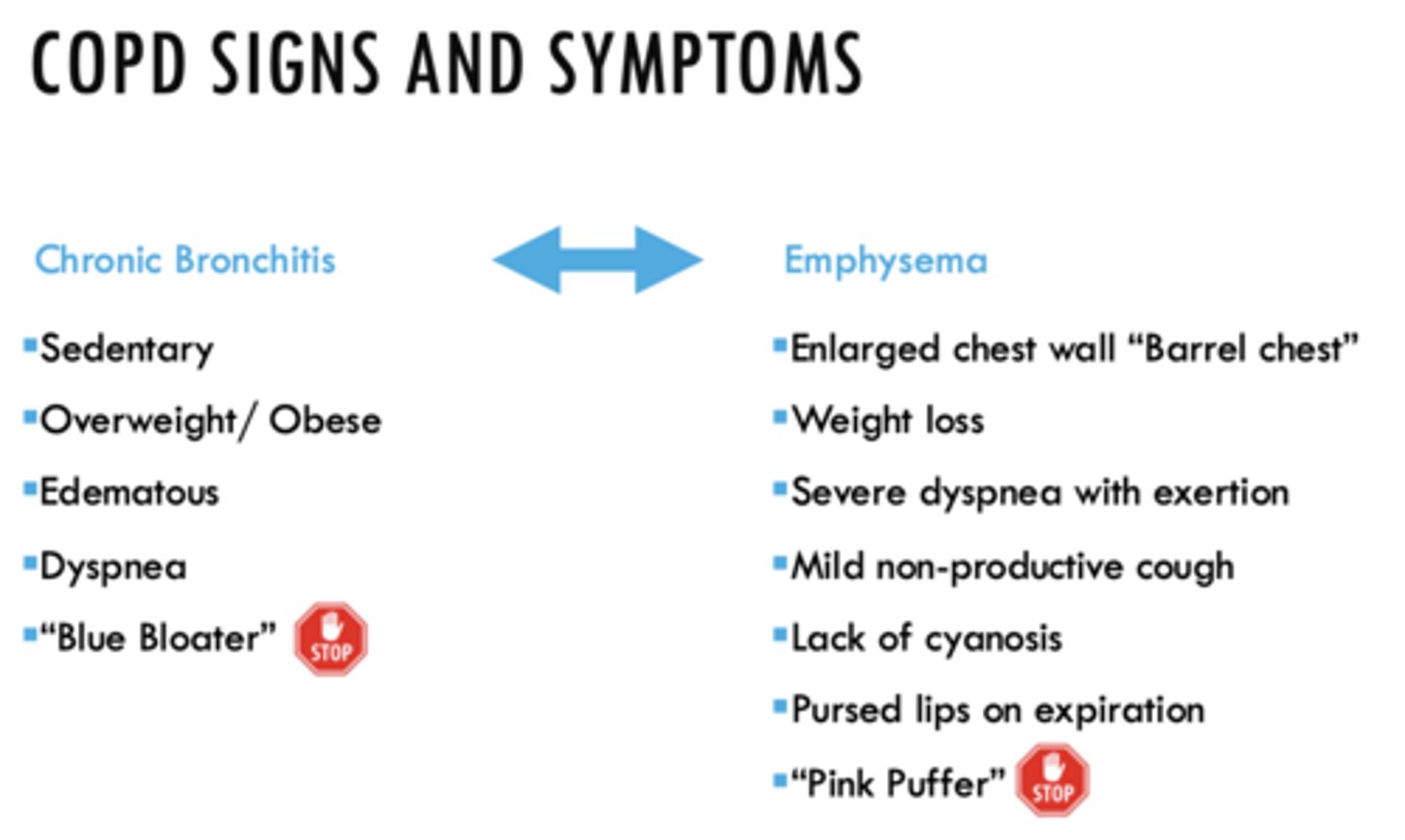
ID if the following sign/symptom is a characteristic of Emphysema or Chronic Bronchitis:
- Severe dyspnea with exertion
- Mild non-productive cough
Emphysema
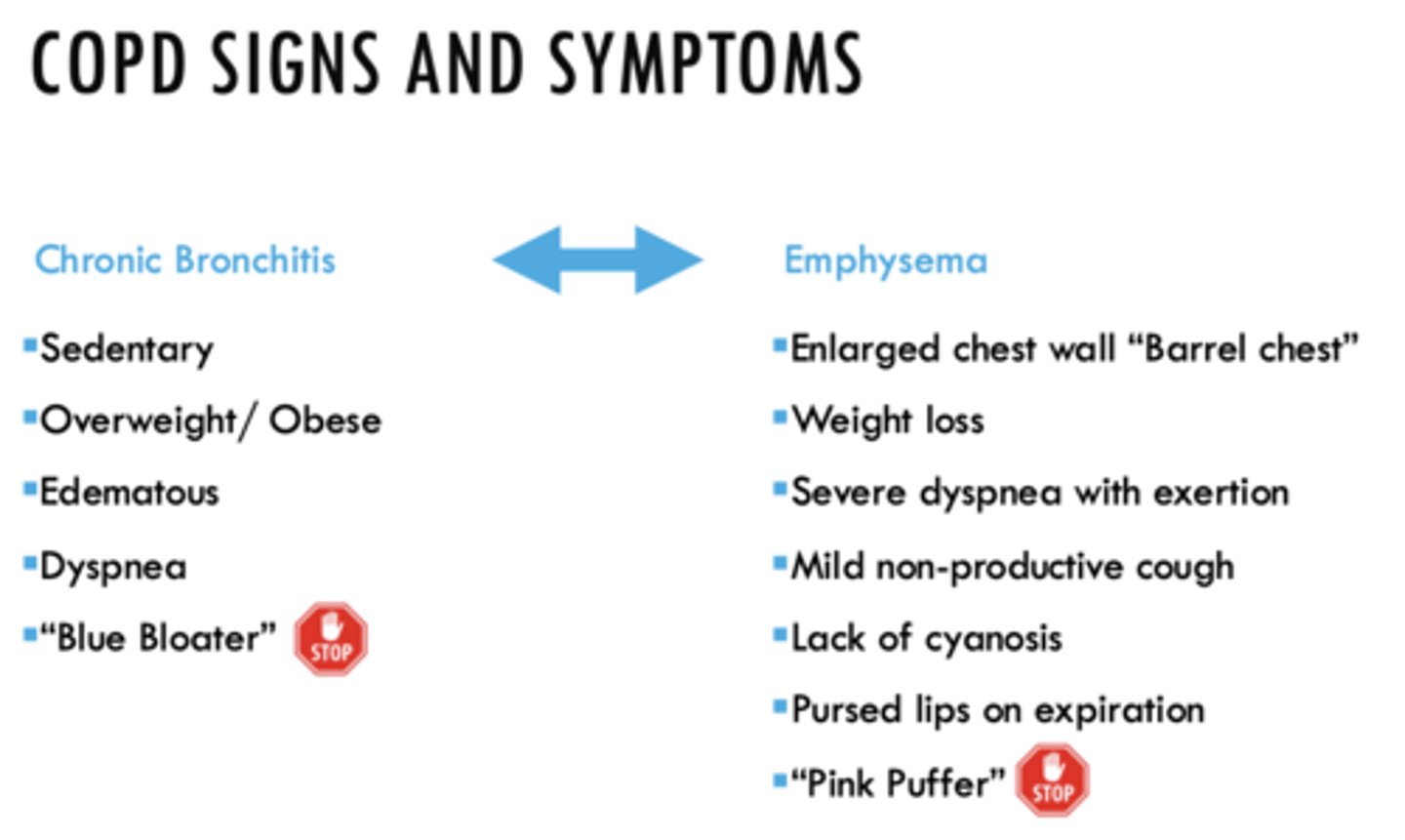
ID if the following sign/symptom is a characteristic of Emphysema or Chronic Bronchitis:
- Lack of cyanosis
- “Pink Puffer”
Emphysema
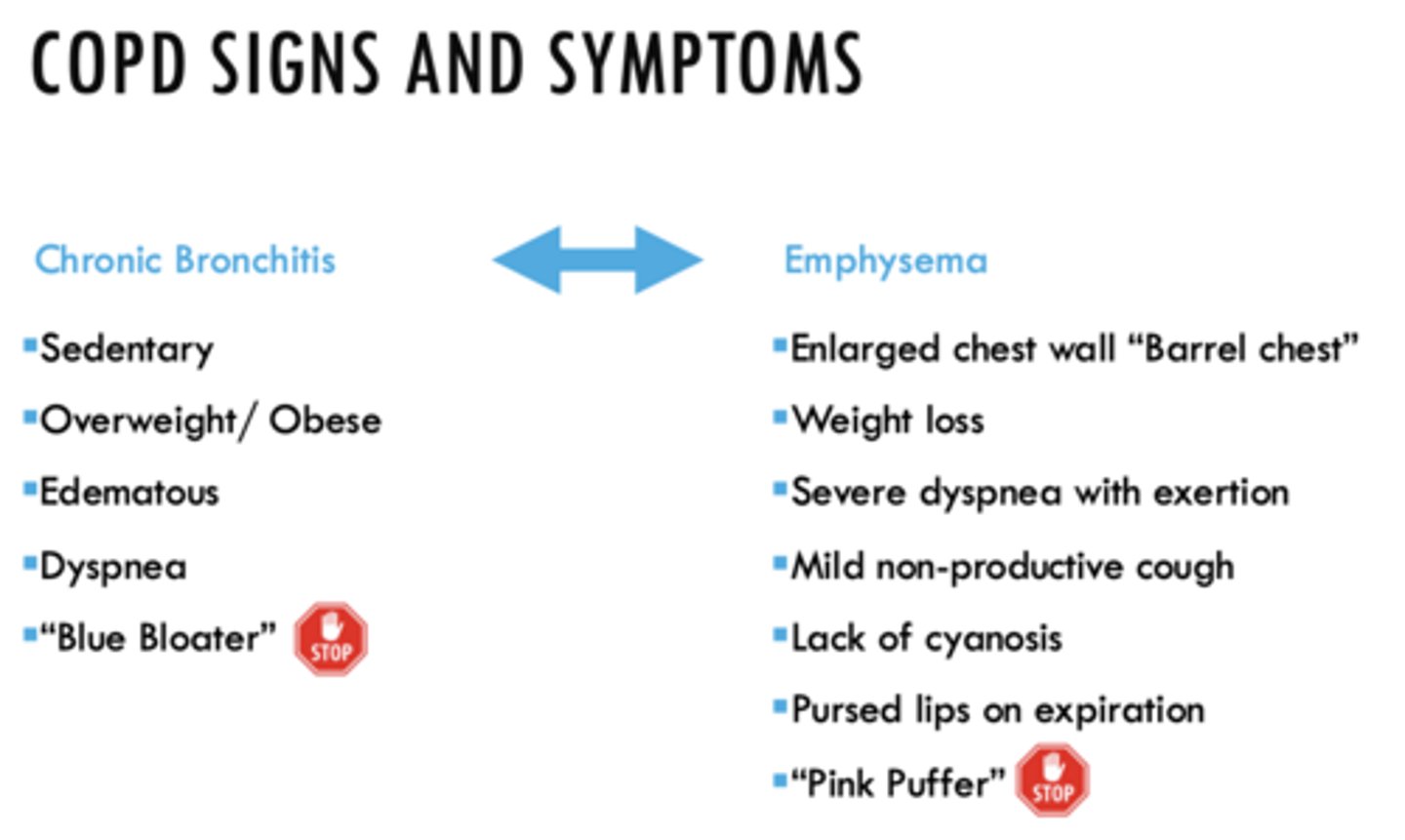
ID if the following sign/symptom is a characteristic of Emphysema or Chronic Bronchitis:
- Pursed lips on expiration
Emphysema
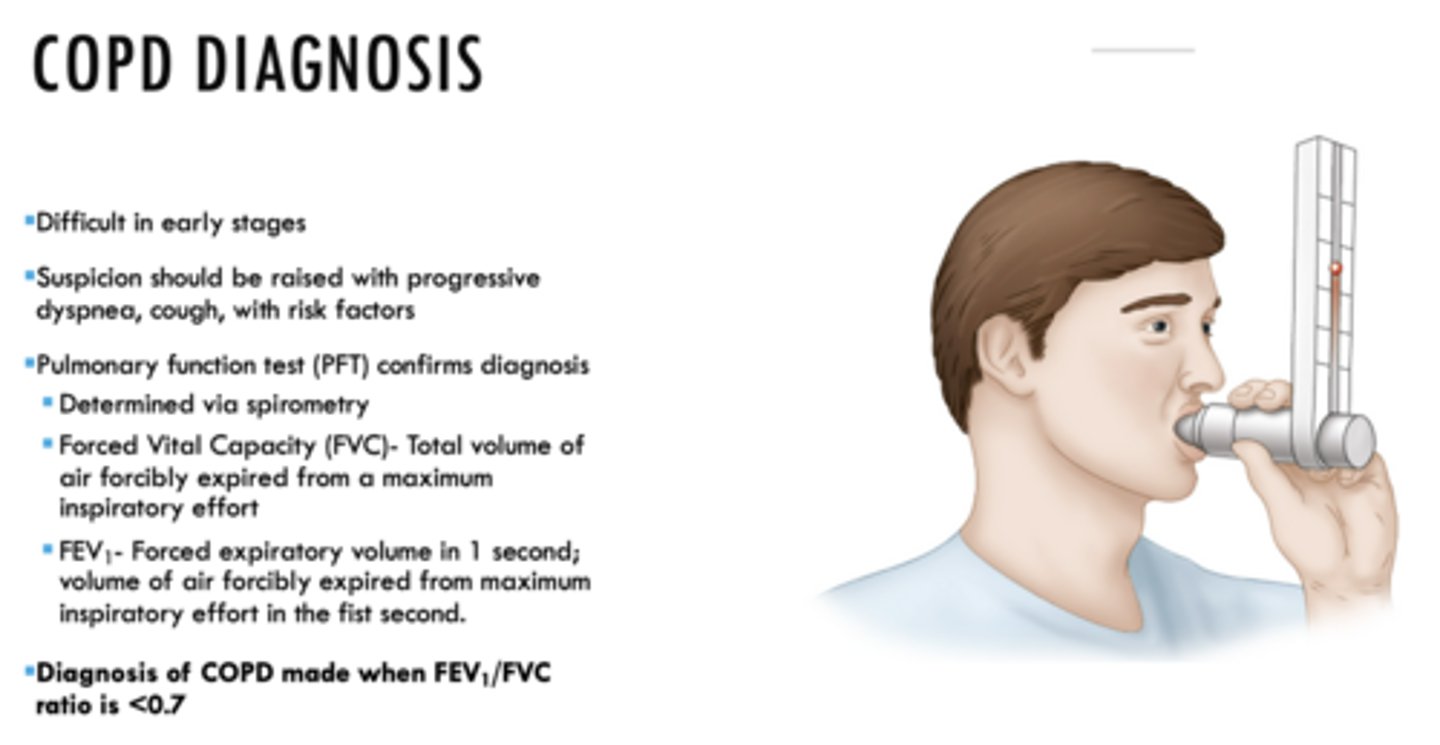
How is COPD diagnosed?
Pulmonary function test (PFT): FEV1/FVC
(Determined via spirometry)
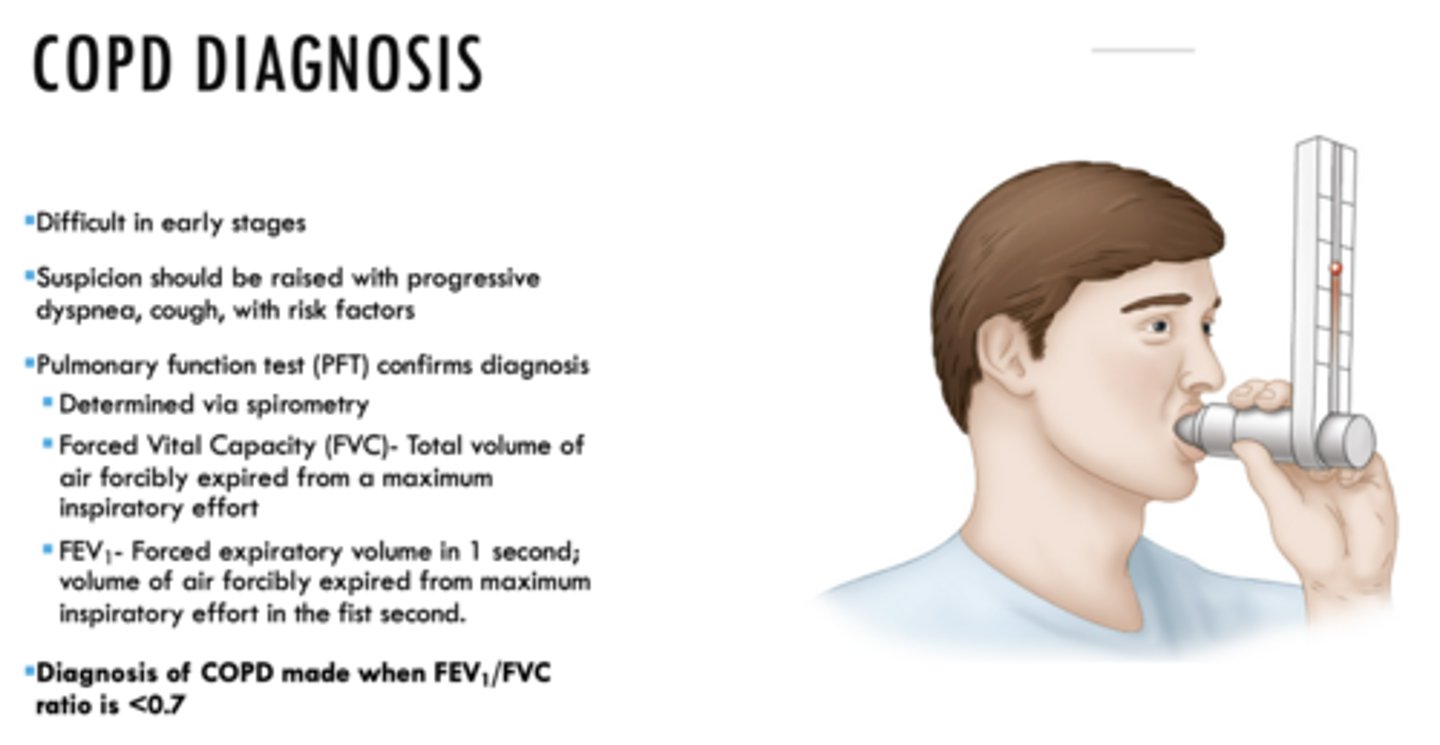
Diagnosis of COPD made when FEV1/FVC ratio is _____
<0.7
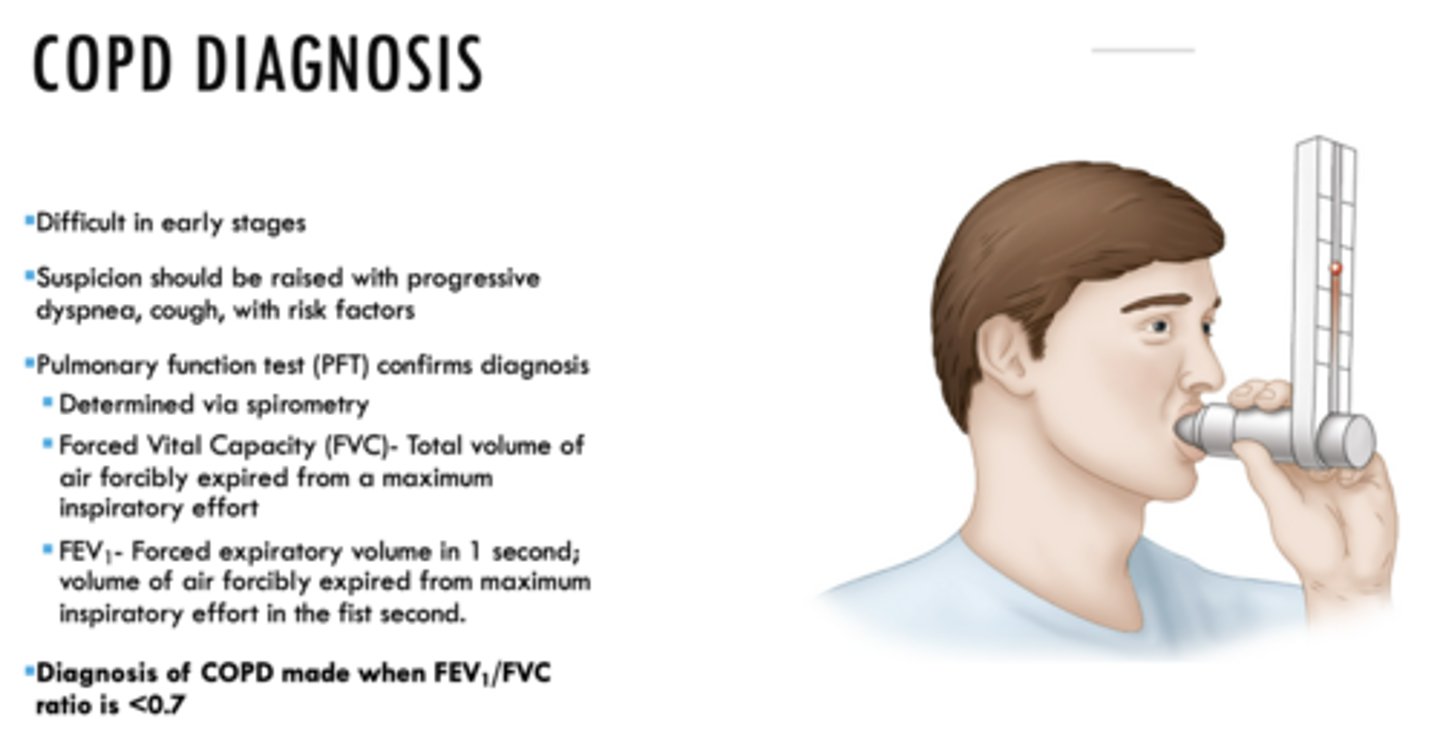
What is the total volume of air forcibly expired from a maximum inspiratory effort?
FVC
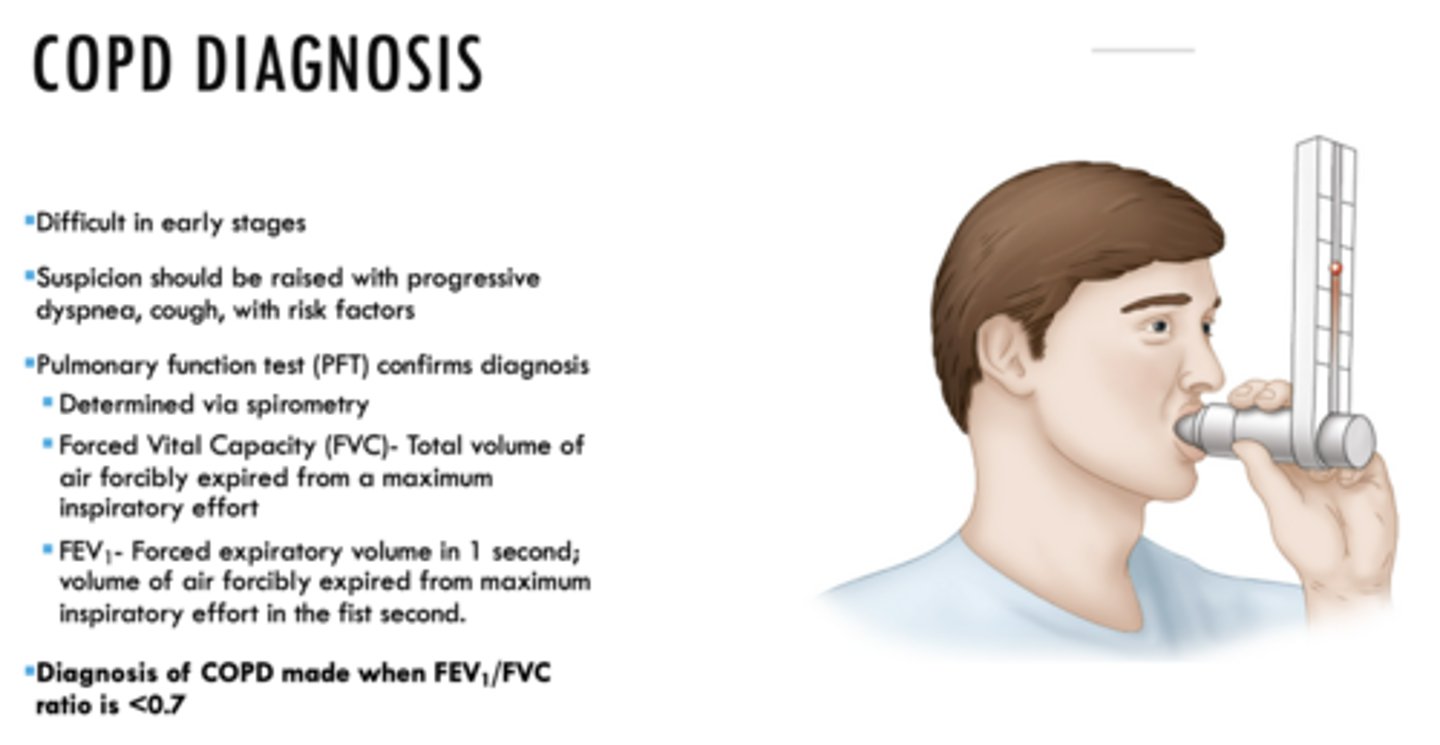
What is the forced expiratory volume in 1 second; volume of air forcibly expired from maximum inspiratory effort in the first second?
FEV1
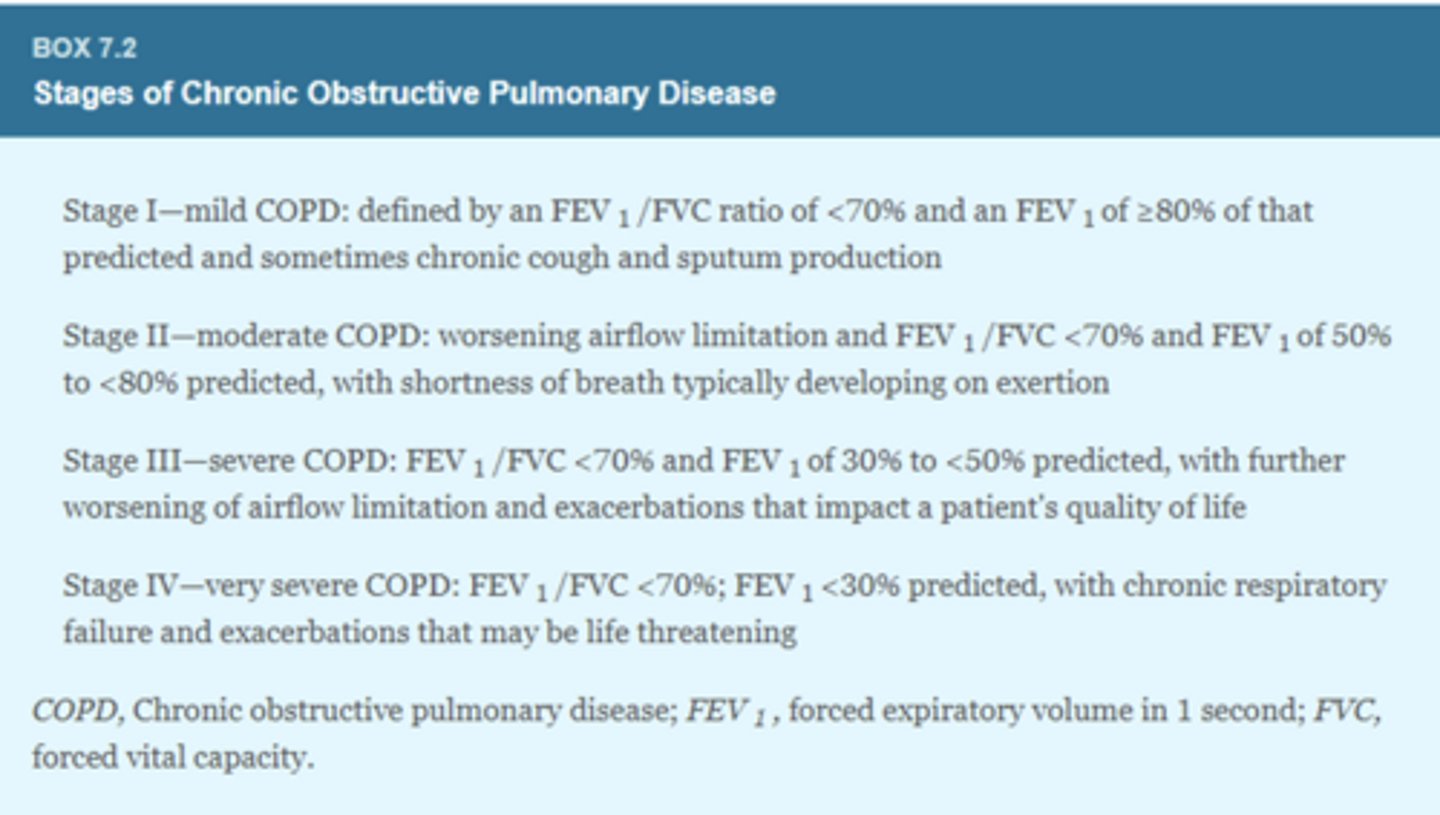
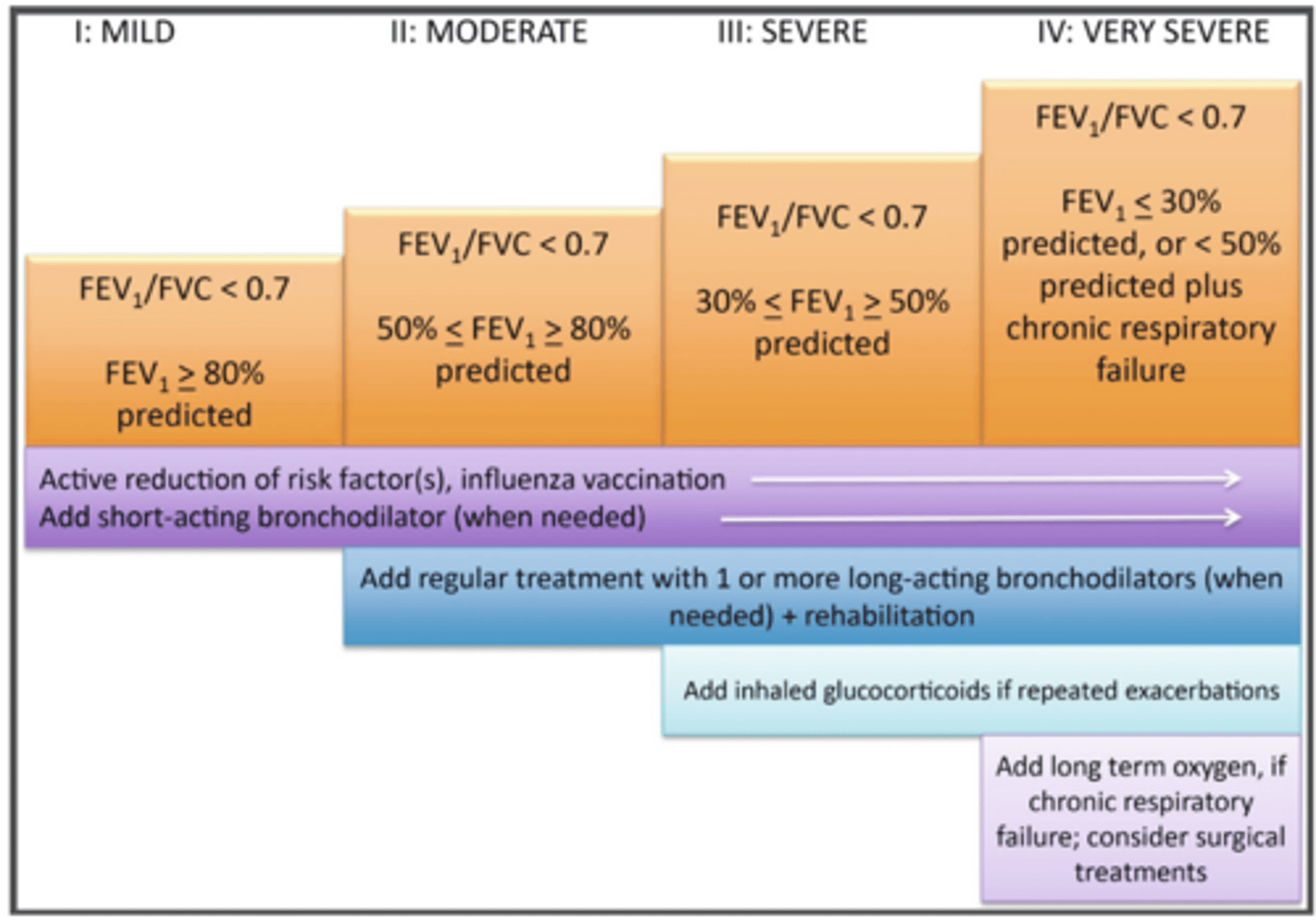
ID the stage of COPD:
- FEV1/FVC ratio <70% and FEV1 of >80% of that predicted and sometimes chronic cough and sputum production
Stage I
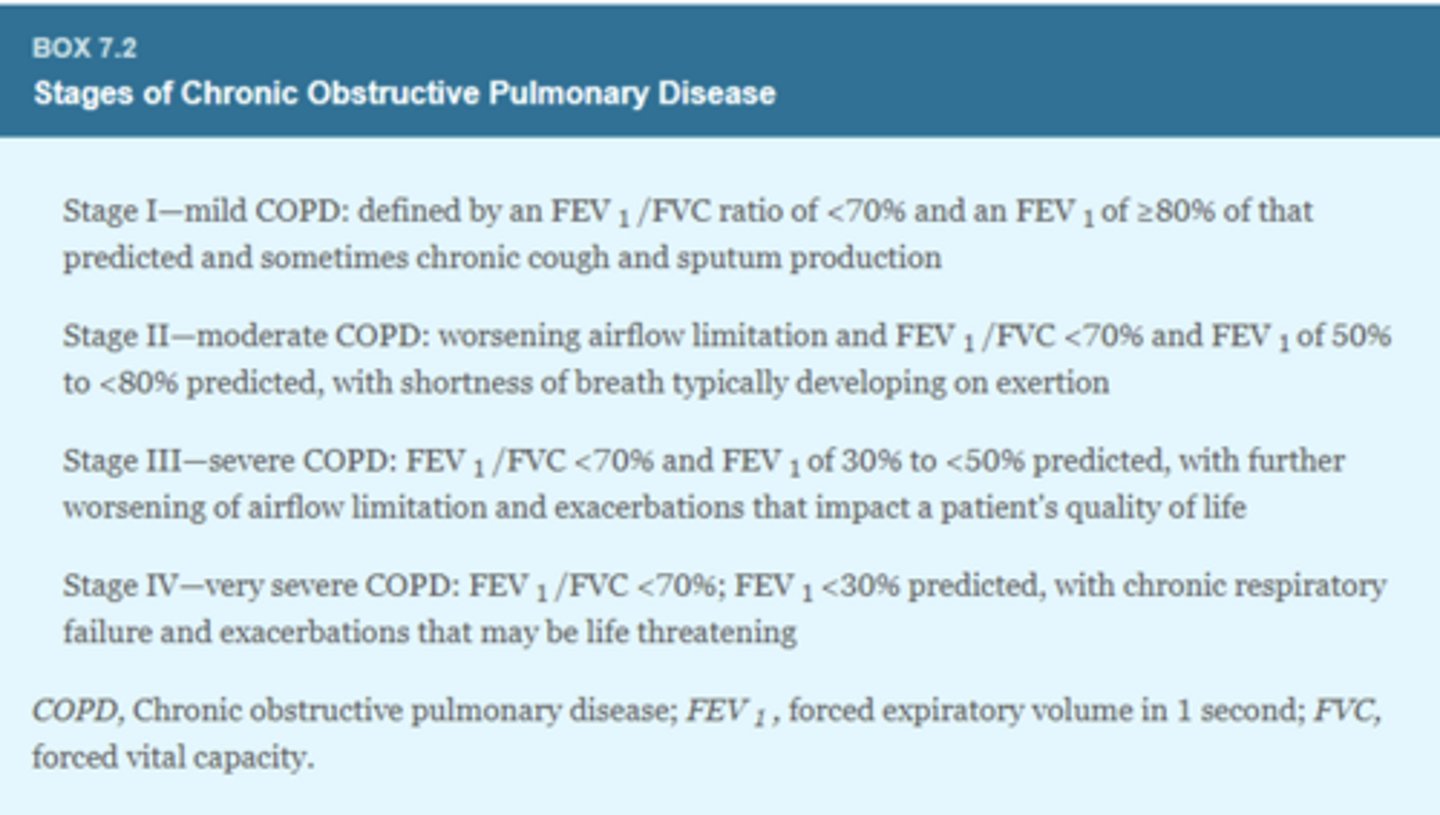
ID the stage of COPD:
-FEV1/FVC ratio <70% and FEV1 of 50-80% of that predicted,
- Worsening air flow limitation with shortness of breath on exertion
Stage II
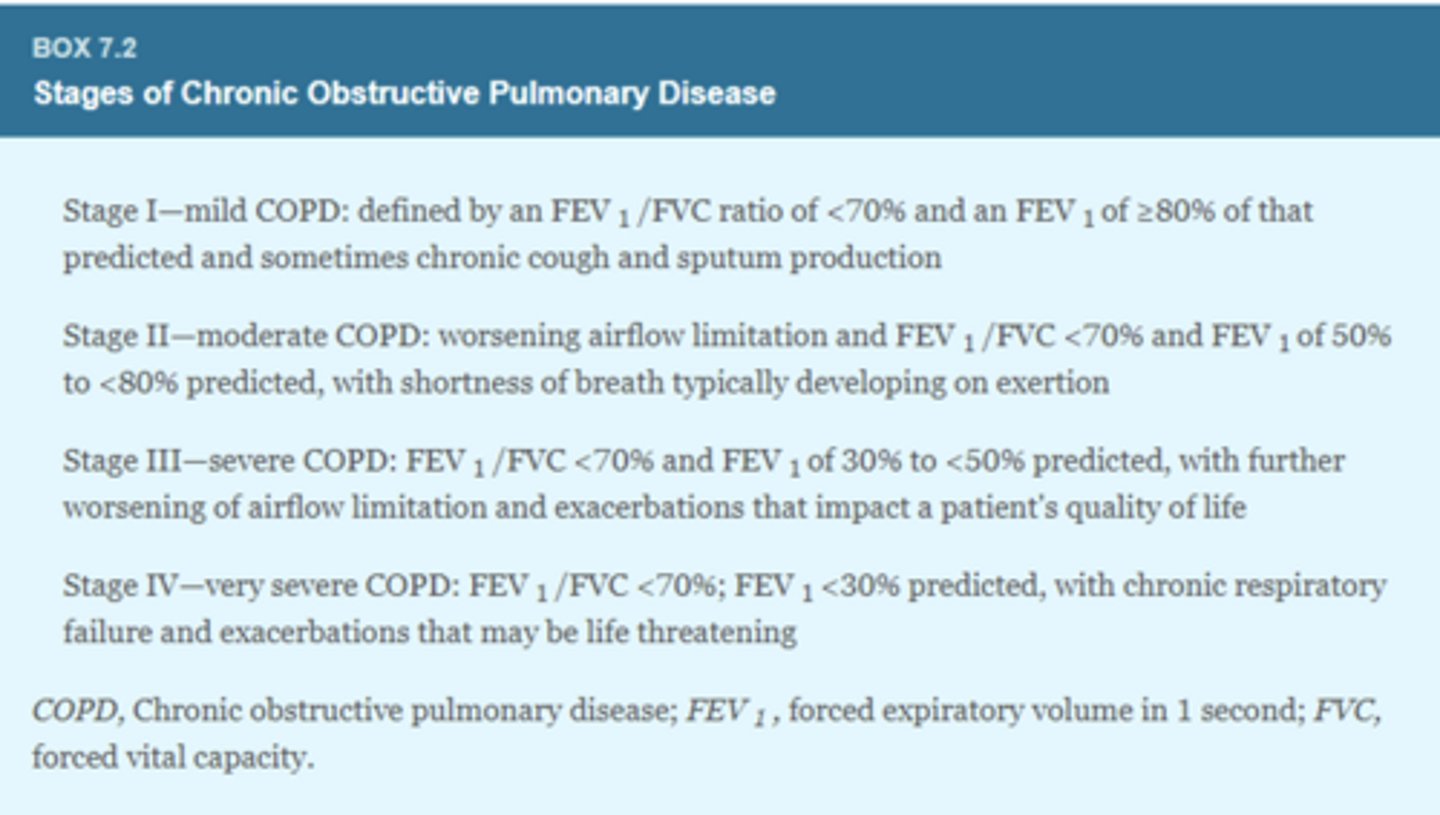
ID the stage of COPD:
- FEV1/FVC ratio <70% and FEV1 of 30-50% of that predicted,
- Worsening air flow limitations and exacerbations that impact the patient's quality of life
stage III
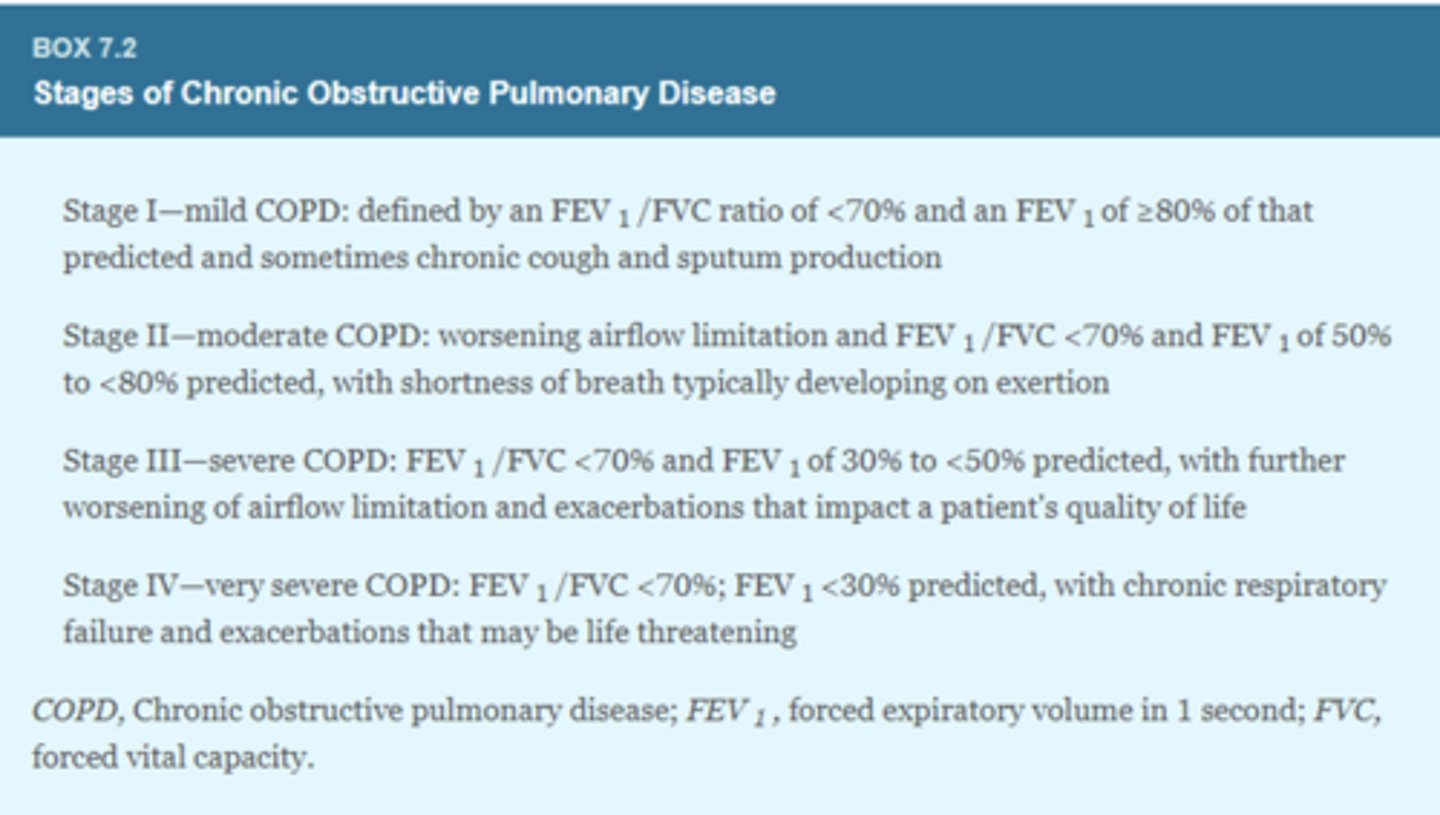
ID the stage of COPD:
- FEV1/FVC ratio <70% and FEV1 of <30% of that predicted,
- Chronic respiratory failure and exacerbation that are life threatening
stage IV
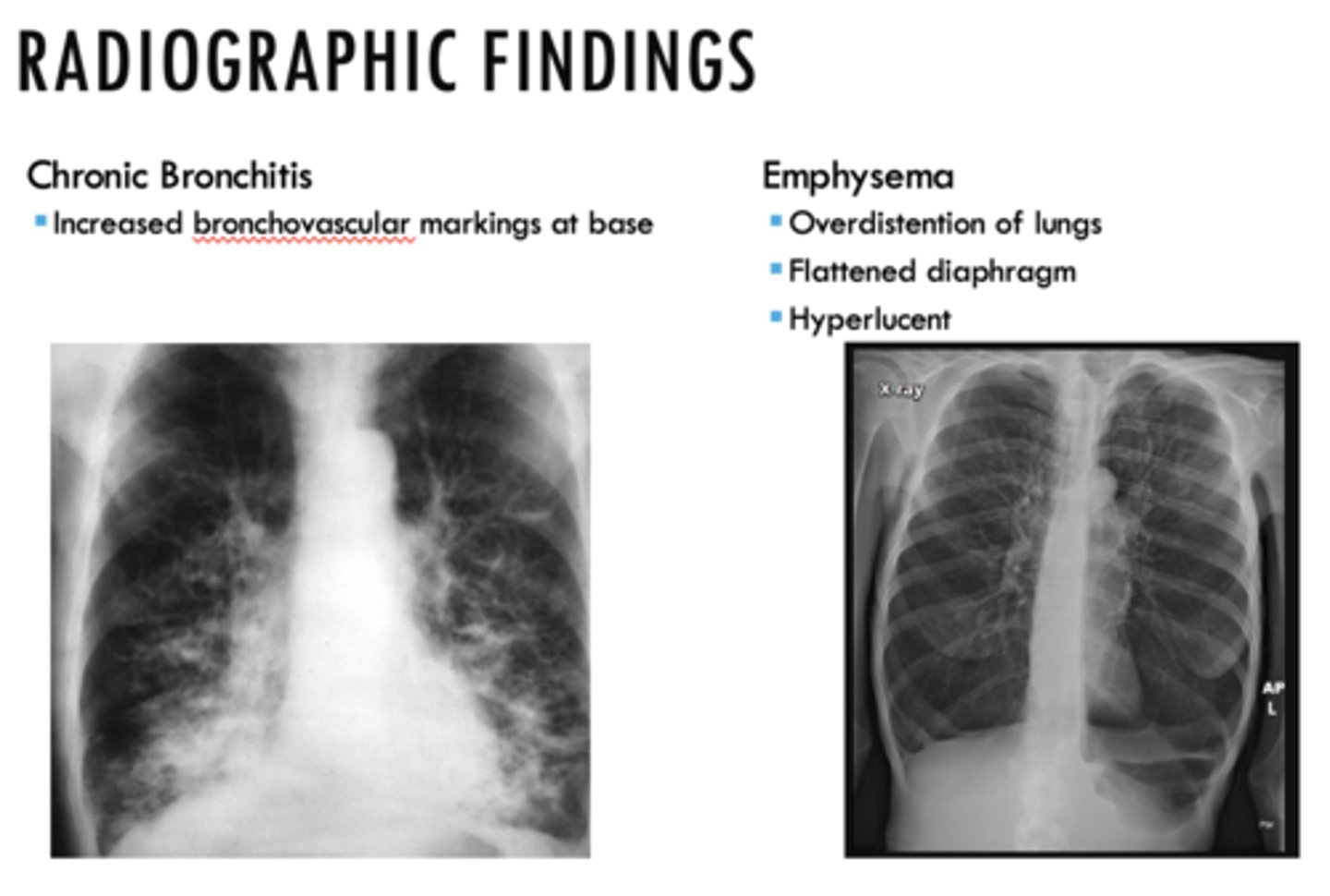
The following are radiographic findings of what?
- Increase bronchovascular markings at base
Chronic bronchitis (know the associated pic!!)
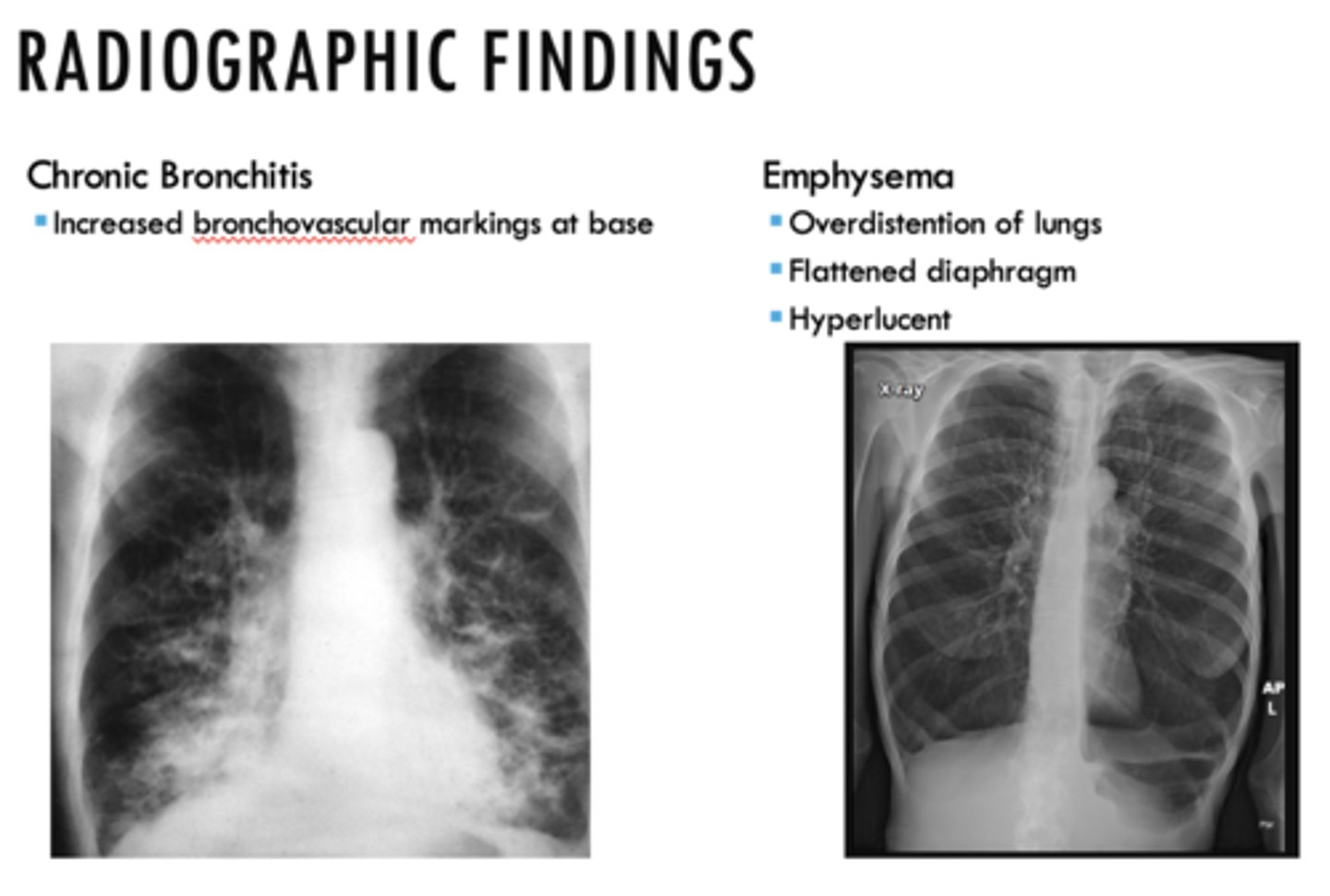
The following are radiographic findings of _______:
- Overdistention of lungs
- Flattened diaphragm
- Hyperlucent
Emphysema (know the associated pic!!)
Is COPD reversible or irreversible?
Irreversible
What is the most effective and cost-effective intervention that can reduce risk of COPD and its progression?
Smoking cessation
These are all medical managements of what?
- Avoidance of pulmonary irritants
- Influenza and pneumococcal vaccinations
- Use of short- and long-acting bronchodilators
- Improving exercise tolerance
- Good nutrition
- Adequate hydration
- Smoking cessation
Chronic obstructive pulmonary disease (COPD)
What is the primary pharmacological intervention for COPD?
Inhaled bronchodilators
What medications reduce glandular mucus and relax smooth muscle by blocking Ach at the muscarinic receptors?
Short/long acting anticholinergics (ipratropium, tiotropium)
What medications relax smooth muscle by increasing cyclic adenosine monophosphate levels?
Short/long acting B2 adrenergic bronchodilators
T/F: Combining bronchodilators effective for COPD because they work by different mechanisms
True
Inhaled corticosteroids are added to the regimen for symptomatic patients at COPD stage _____ or above who have repeated exacerbations
Stage III
Supplemental O2 (2 L/min) is recommended when the patient's PO2 is ___% or less
88%
These are all medical managements of what?
- Antibiotics for pulmonary infections
- Additional considerations include: pulmonary rehabilitation, screening for comorbid conditions, and continual monitoring for disease progression
Chronic obstructive pulmonary disease (COPD)
In what stage of COPD should routine dental care be avoided?
Stage IV
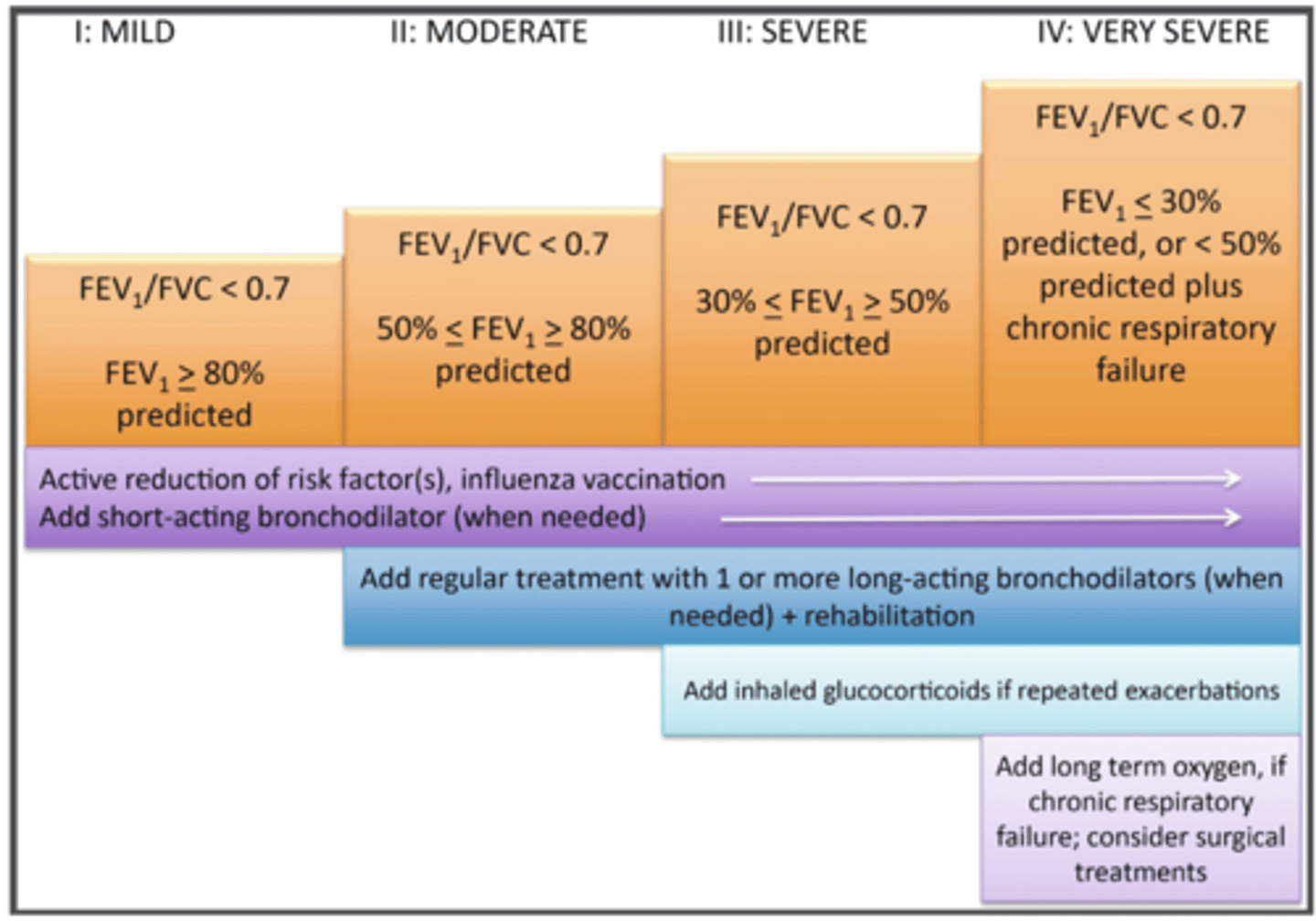
In what stage would you consider adding long term oxygen & if chronic respiratory failure, surgery intervention?
Stage IV
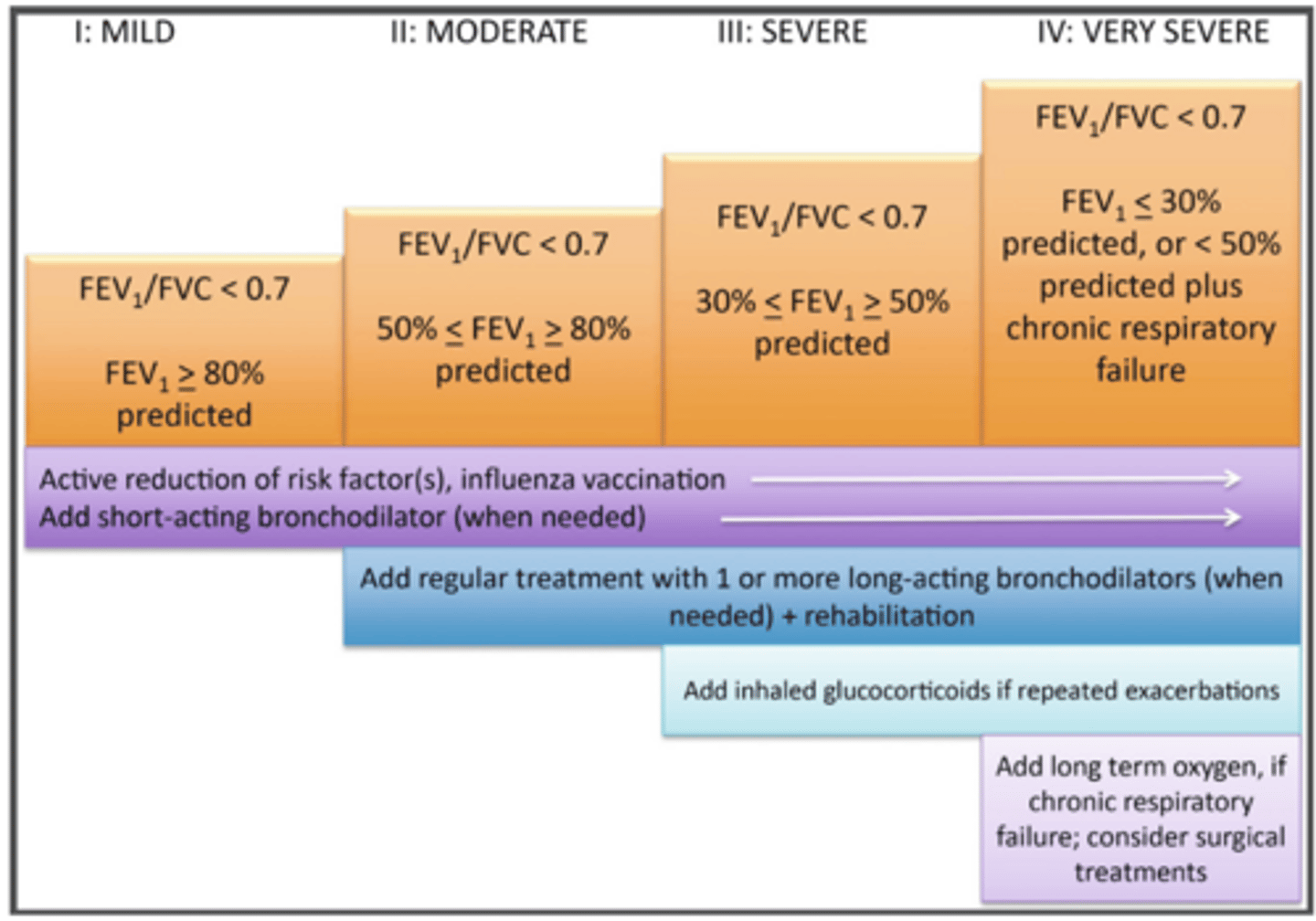
In what stages would you introduce inhaled glucocorticoids if repeated exacerbations?
stage III and IV COPD
During a risk assessment for a patient with SOB, productive cough, URI, or oxygen saturation less than ____% is unstable
91%
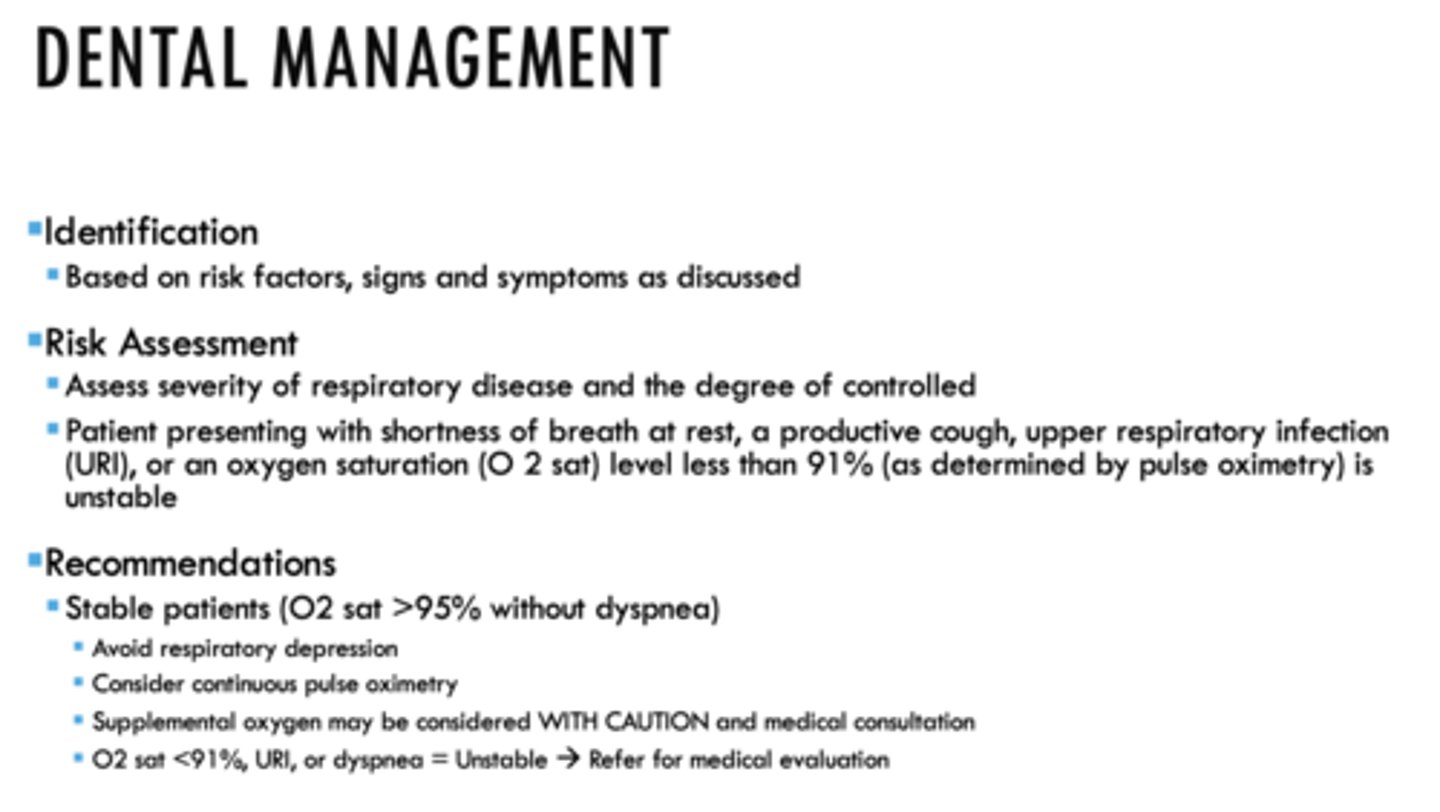
What is a COPD stable patient?
O2 sat >95% without dyspnea
(Avoid respiratory depression; Consider continuous pulse oximetry; Supplemental oxygen may be considered WITH CAUTION and medical consultation; O2 sat <91%, URI, or dyspnea = Unstable --> Refer for medical evaluation)
Which of the following indicate that your COPD patient is UNSTABLE EXCEPT?
a. SOB at rest
b. productive cough
c. URI
d. O2 sat >91%
D - LESS THAN 91% is UNSTABLE
All of the following are comorbidities associated with COPD except:
a. Hypertension
b. Coronary heart disease
c. Retinopathy
d. Shortened life span
e. Higher risk of heart failure, arrhythmia, and MI
c. Retinopathy
What should you do if you are treating a COPD patient with coexisting cardiovascular disease?
- Stress reduction measures should be implemented
- Vital sign monitoring
- Supplemental oxygen may be considered
All of the following are dental management considerations for a patient with COPD except:
a. supine position
b. possible discomfort for bilateral IAN blocks
c. avoid meds that depress respiratory drive
d. Extreme caution with NO2
e. Be aware of corticosteroid use and need for supplementation
A. SEAT PT IN UPRIGHT OR SEMI RECLINED POSITION
What type of local anesthetic could cause possible discomfort for patients with COPD?
Bilateral IAN blocks
Nitrous oxide-oxygen should be used with extreme caution with patients with COPD. What are two main concerns?
- Ruptured bullae
- Relative contraindication
Patients with COPD who are ___________ have increased likelihood of all the following:
- Halitosis
- Extrinsic tooth stains
- Nicotine stomatitis
- Periodontal disease
- Premalignant mucosal lesions
- Oral cancer
- Xerostomia
Chronic smokers
T/F: Poor oral hygiene, oral bacteria, and periodontitis can contribute to acute respiratory exacerbations and aspiration pneumonia in frail older adults who have COPD
True
What medication is associated with dry mouth?
Anticholinergics
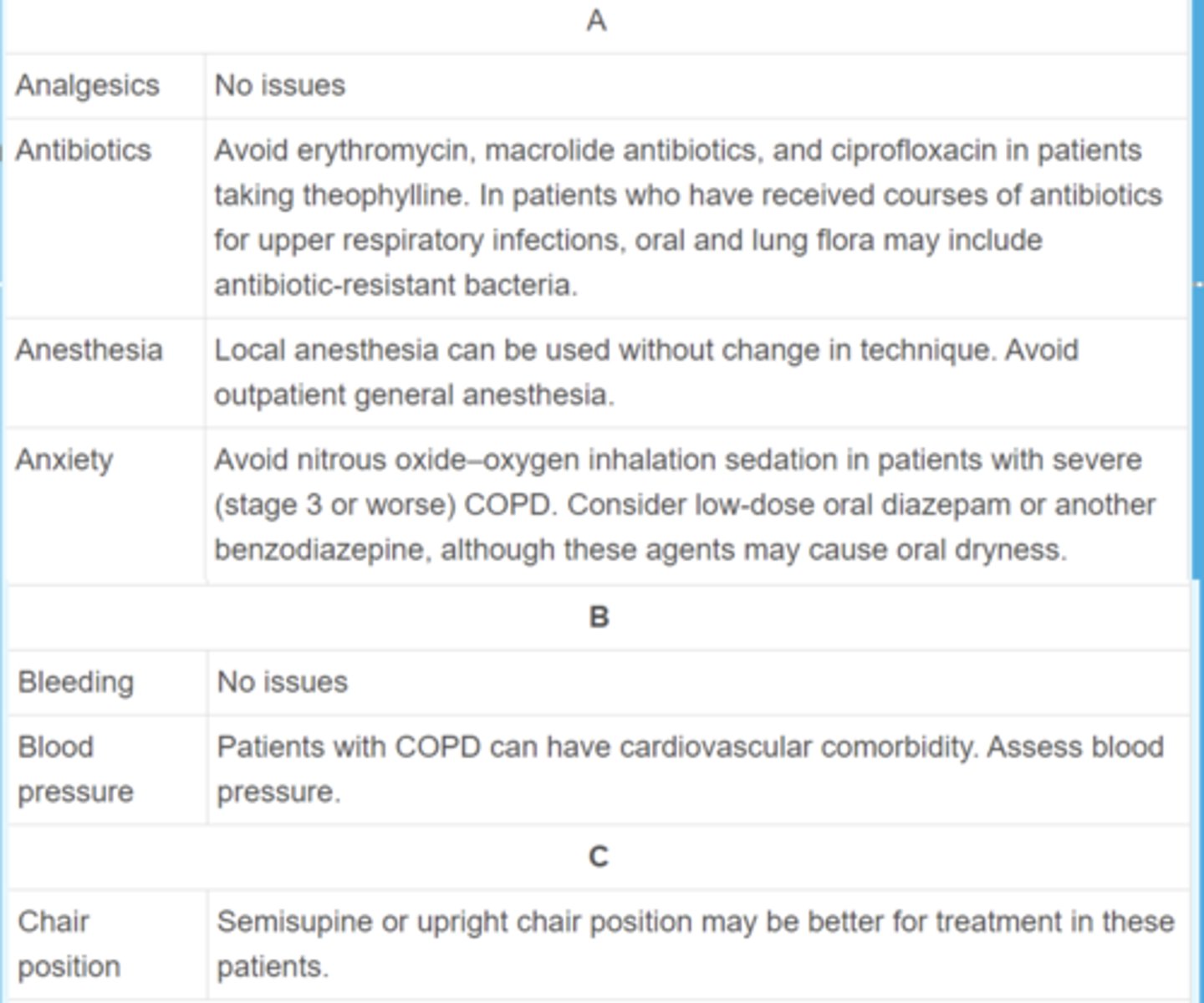
For patients with COPD, avoid avoid erythromycine, macrolides, & ciproflaxine in patients taking ________
Theophylline
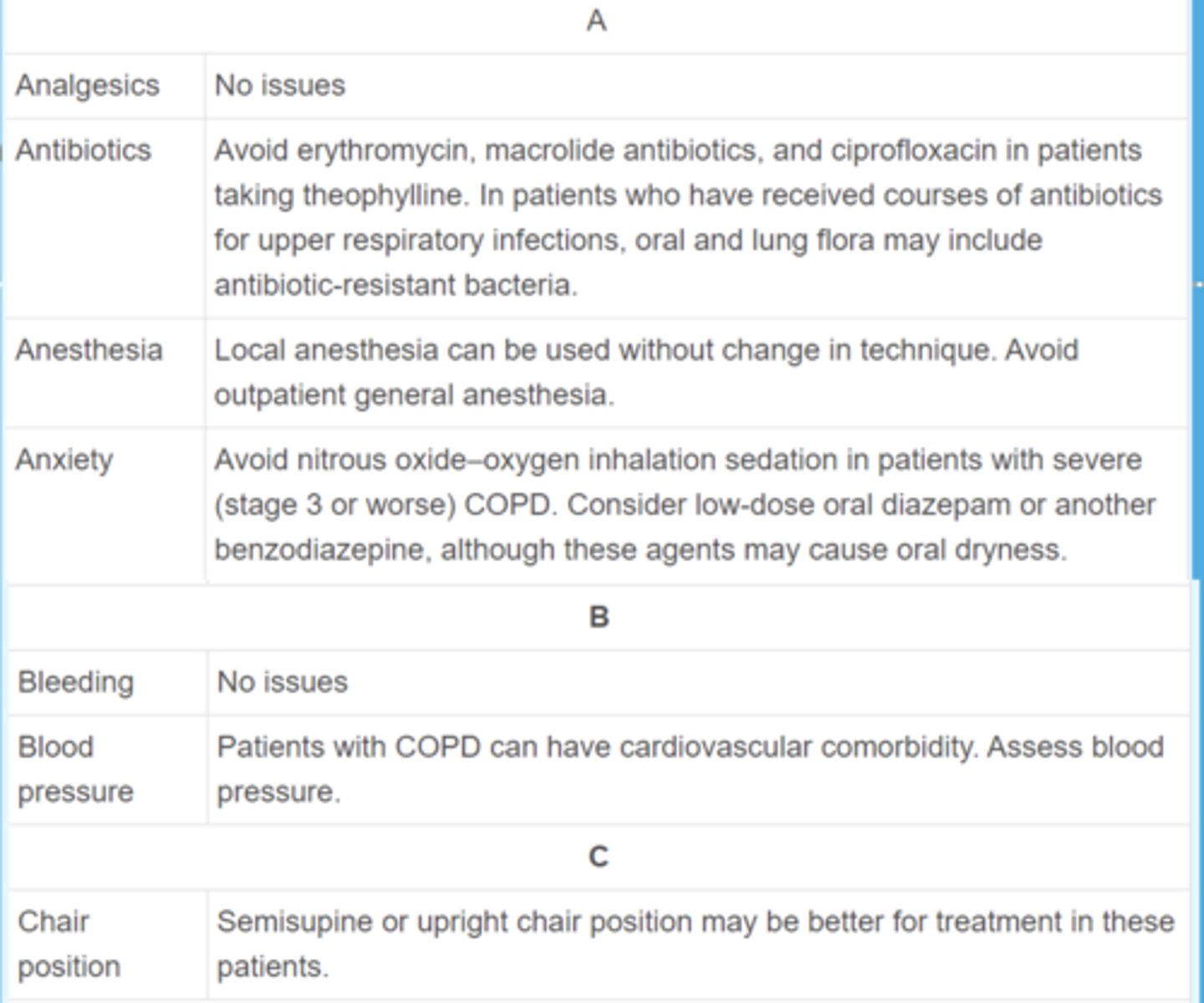
What are the dental considerations for patients that have COPD in terms of anesthesia?
Avoid outpatient GA
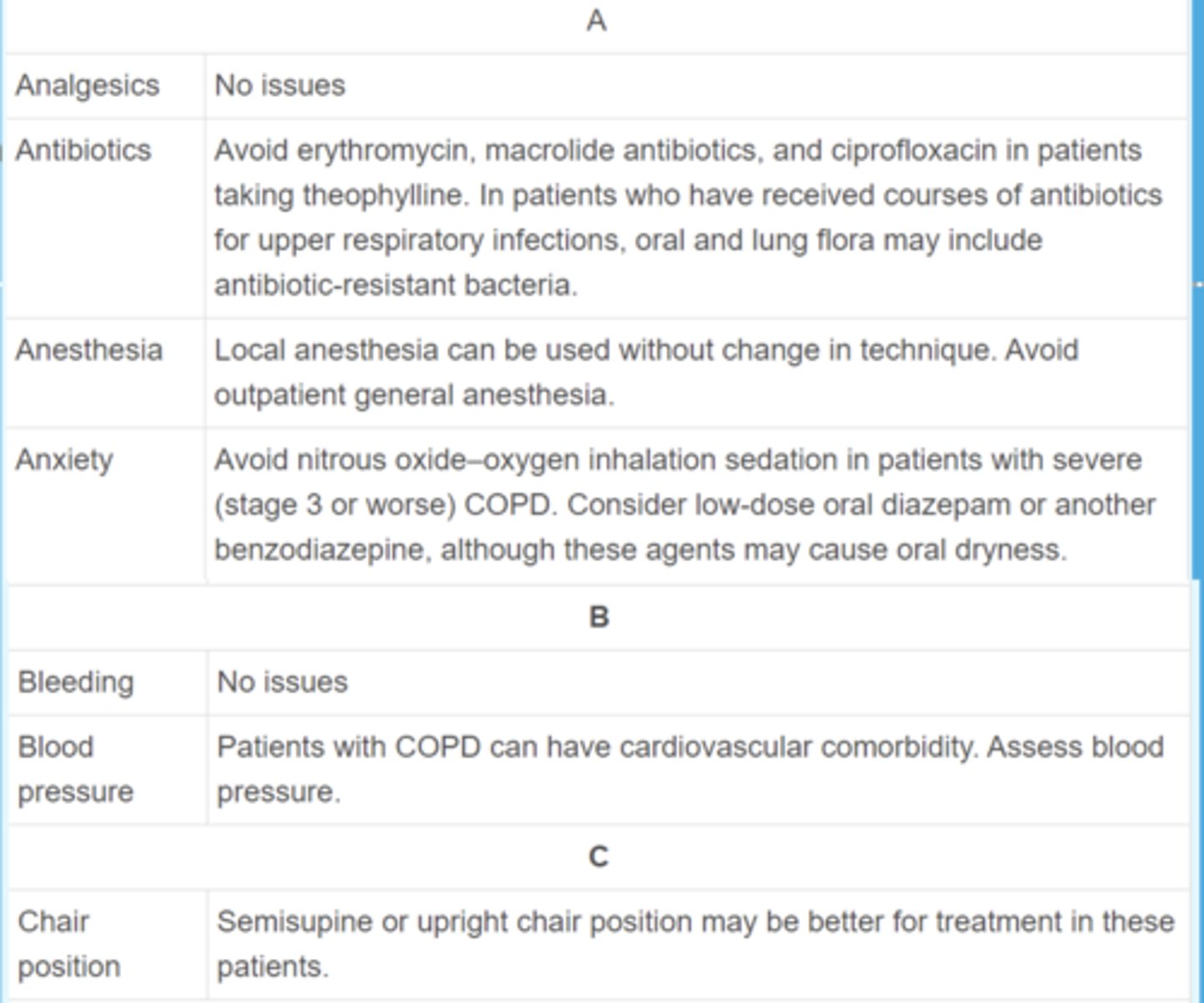
What are the dental considerations for patients that have COPD in terms of anxiety?
Avoid nitrous in stage III and up, consider low-dose diazapam
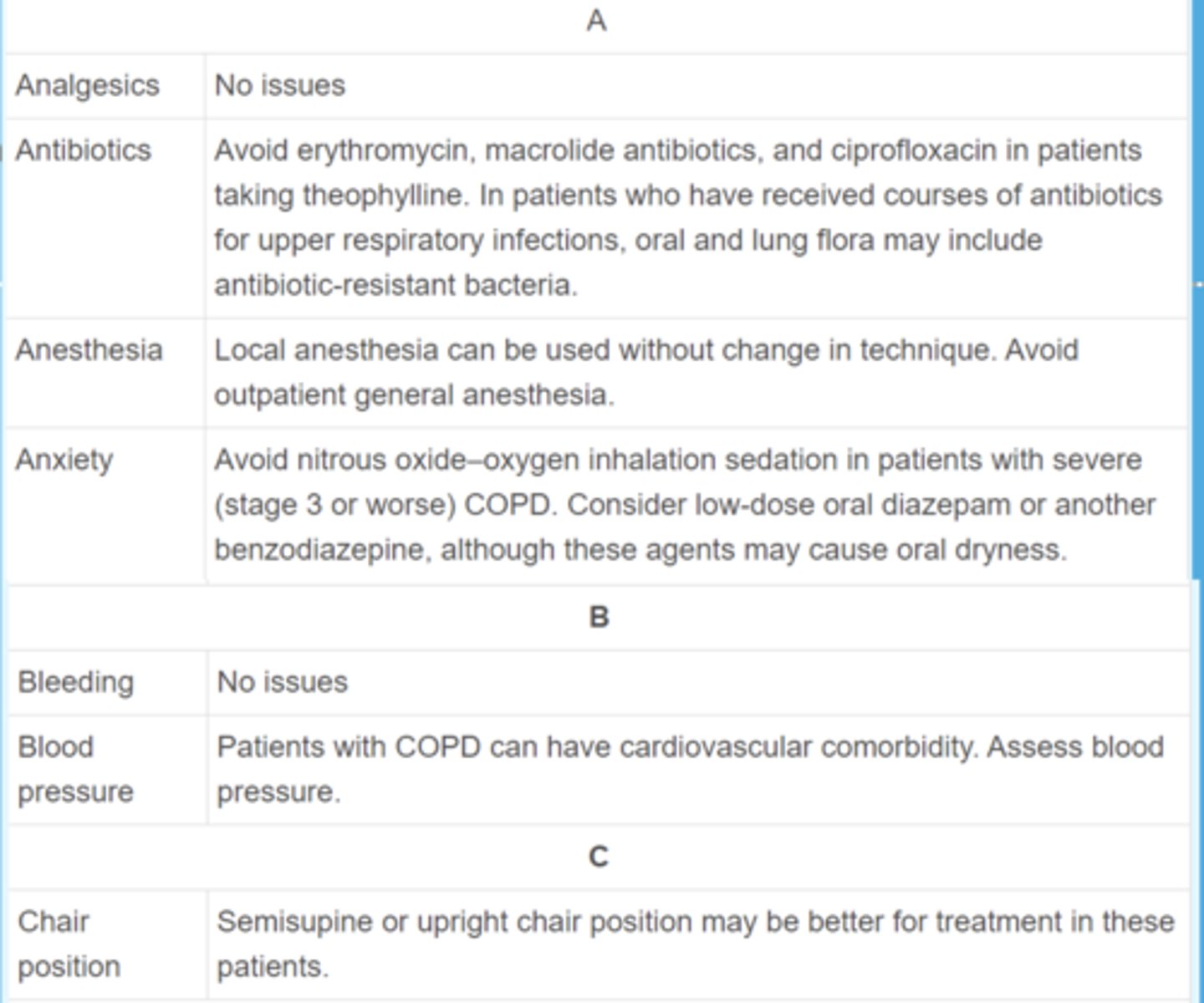
What are the dental considerations for patients that have COPD in terms of blood pressure?
Patients have cardiovascular comorbidities, monitor BP
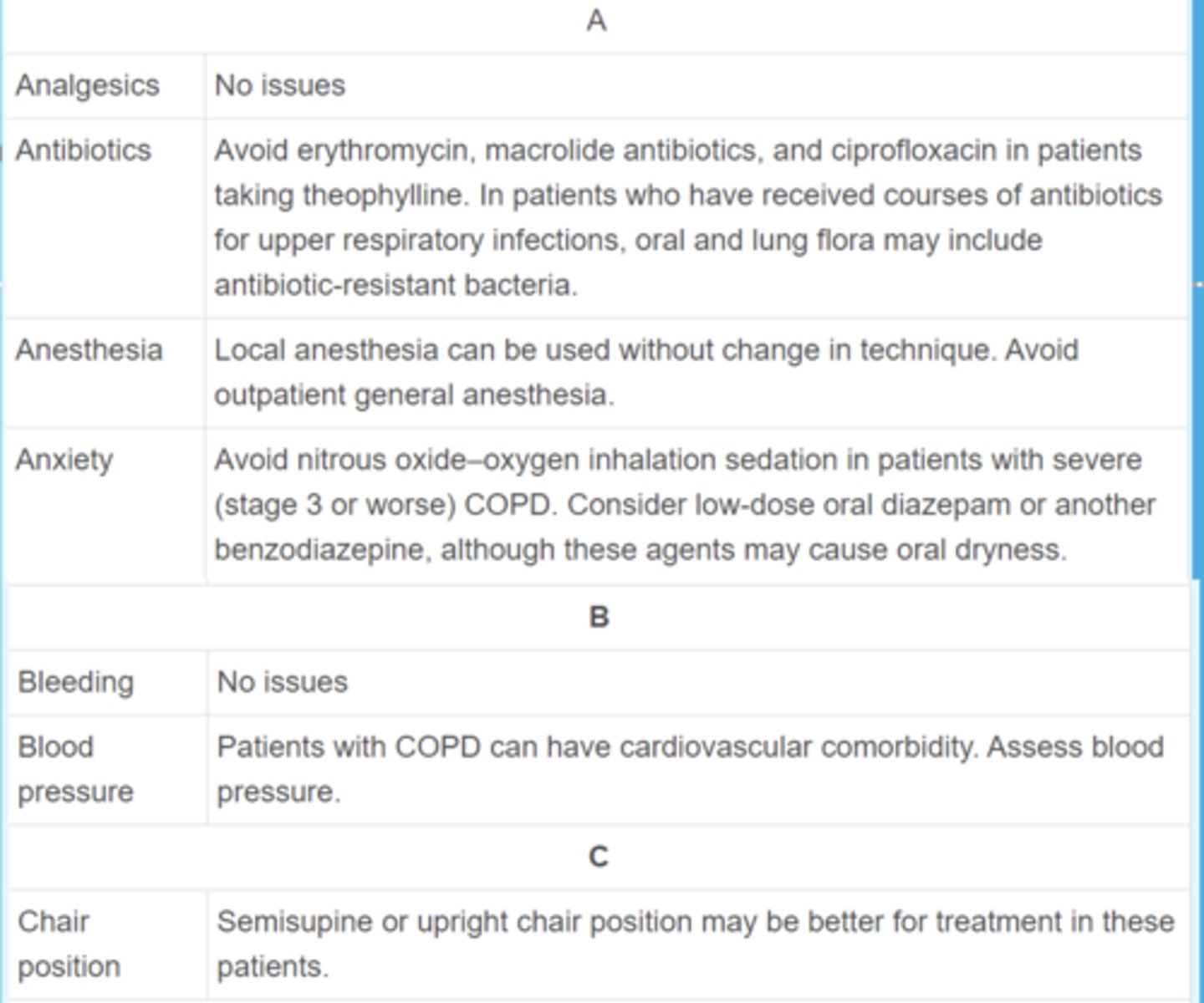
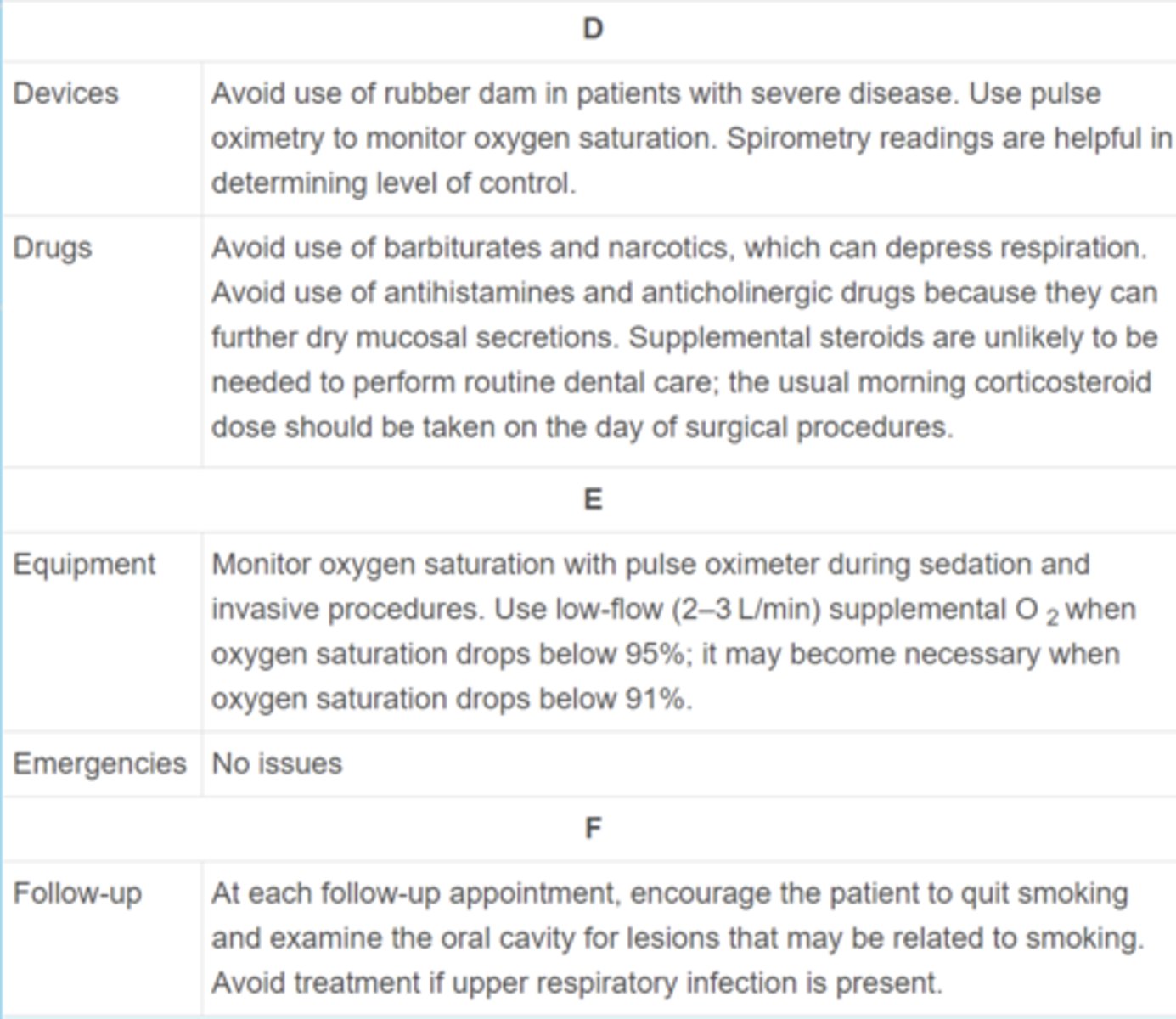
What are the dental considerations for patients that have COPD in terms of chair position?
Semisupine or upright
What are the dental considerations for patients that have COPD in terms of devices? (2)
- Avoid use of dental damn in severe cases
- Use pulse oximetry to monitor oxygen saturation
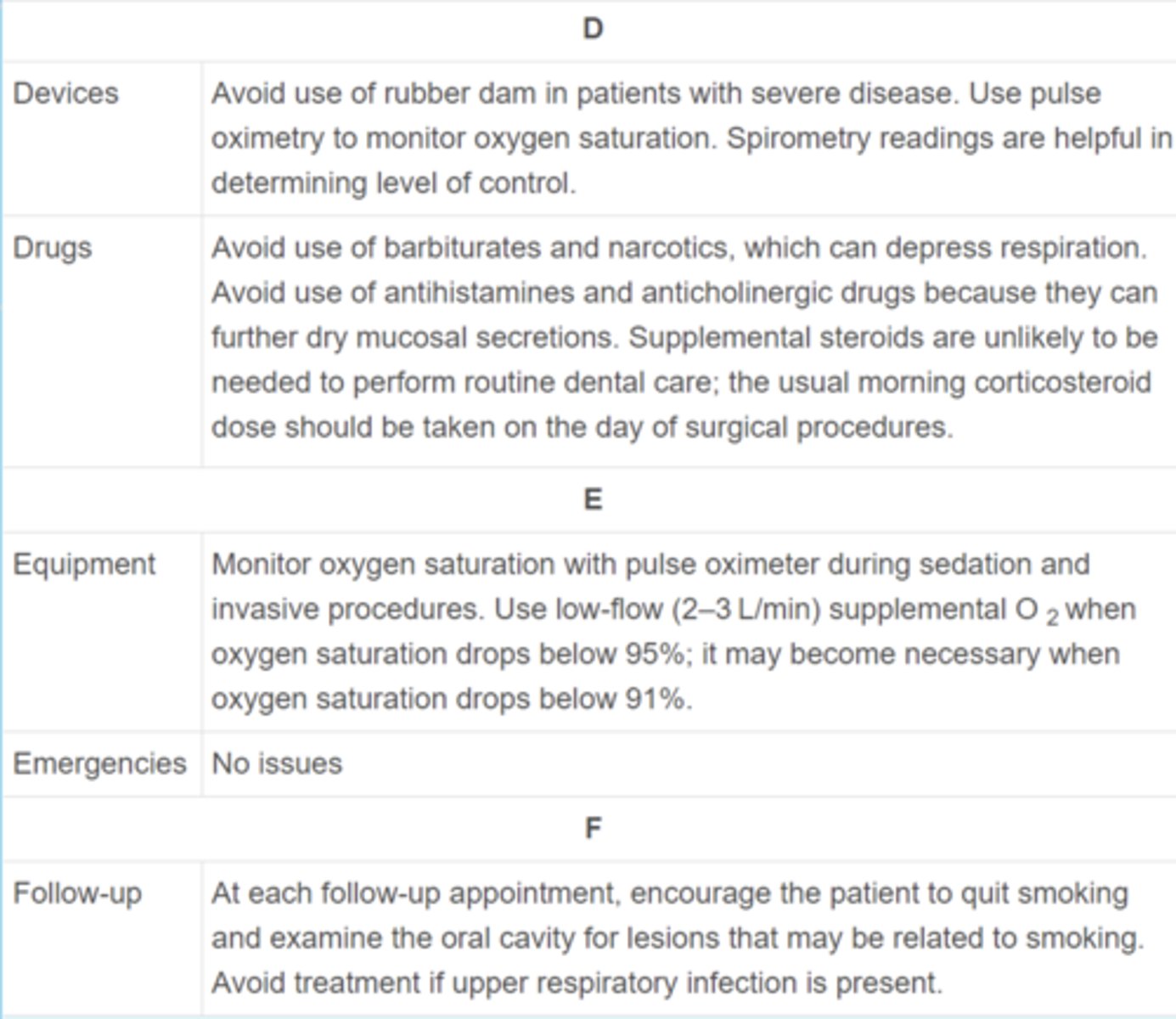
For patients that have COPD, what drugs should we avoid and why?
- Narcotics & barbiturates (respiratory depression)
- Antihistamine anticholinergics (further dry mucosa)
ID the condition:
Chronic inflammatory disease of the airways characterized by reversible episodes of increased airway hyperresponsiveness, which results in recurrent episodes of dyspnea, coughing, and wheezing
Asthma

All of the following can cause hypersensitivity leading to asthma EXCEPT:
a. allergens
b. URI
c. exercise
d. cold air
e. medications (salicylates, NSAIDs, cholinergics, B-blockers)
f. stress
g. chemicals
h. smoke
i. anxiety
f. stress

Asthma is more common in males or females?
females
This is the epidemiology for what condition?
- United States prevalence- 8%
- 10% of children have asthma
- Higher prevalence in families living below poverty line
- Accounts for ~2 million ED visits and 3500 deaths per year
Asthma
This is the epidemiology for what condition?
- Multifactorial and heterogenous disease
- Combination of environmental and genetic factors
- Clinical manifestations are a result of dysfunction of
- - Airway epithelium
- - Smooth muscle
- - Immune cells
Asthma
What is important to understand when treating any patient for asthma?
Triggers/stimuli (Ex: Extrinsic, Intrinsic, Drug induced, Exercise induced)
What is the most common form of Asthma?
Extrinsic (allergic) asthma (~35% of all adult cases)
ID the type of asthma:
- Exaggerated inflammatory response
- Triggered by inhaled seasonal allergens such as pollens, dust, house mites, and animal dander
- Usually is seen in children and young adults
Extrinsic (allergic) asthma
ID the type of asthma:
- Inflammatory responses are mediated primarily by type 2 helper T (T H 2) cells
- Secrete interleukins and stimulate B cells to produce IgE
Extrinsic (allergic) asthma
ID the type of asthma attack:
1. Allergens interact with IgE antibodies affixed to mast cells, basophils, and eosinophils along the tracheobronchial tree
2. Antigen-antibody complex à leukocyte degranulation -> cytokines release (bradykinins, histamine, leukotrienes, and prostaglandins)
3. Histamine and leukotrienes cause smooth muscle contraction (bronchoconstriction) and increased vascular permeability
4. Platelet-activating factor sustains bronchial hyperresponsiveness
5. Recruitment of leukocytes (neutrophils and eosinophils) to the airway wall --< increases tissue edema and mucus secretion
Extrinsic (allergic) asthma
What is responsible for smooth muscle contraction (bronchoconstriction) as seen in Extrinsic Asthma?
- Histamine
- Leukotrienes
ID the type of asthma:
- Seldom is associated with a family history of allergy or with a known cause
- Patients usually nonresponsive to skin testing and demonstrate normal IgE levels
- Generally is seen in middle-aged adults
Intrinsic asthma
What three endogenous factors is intrinsic asthma usually associated with?
- Emotional stress (implicated in at least 50% of affected persons)
- Gastroesophageal acid reflux (GERD)
- Vagally mediated responses
These are triggers for which condition?
- Drugs (aspirin, NSAIDs, beta-blockers, angiotensin converting [ACE] enzyme inhibitors)
- Exercise
- Food substances (nuts, shellfish, strawberries, milk, tartrazine food dye yellow color no. 5)
- Aspirin
- Metabisulfite
Intrinsic asthma
What causes the following with intrisnic asthma?
- Causes bronchoconstriction in about 10% of patients with asthma
- Sensitivity occurs in 30% to 40% of people with asthma who have pansinusitis and nasal polyps (triad asthmaticus)
- Block the cyclooxygenase pathway --> buildup of arachidonic acid and leukotrienes mediated by the lipoxygenase pathway --> bronchial spasm
Aspirin
What is a preservative found in foods and drugs (specifically in local anesthetics containing epinephrine) that triggers intrinsic asthma?
Metabisulfite
What drug classes are known to trigger intrinsic asthma? (4)
- Aspirin
- NSAIDs
- Beta blockers
- ACE inhibitors
For dentists , were are Metabisulfites founds?
preservative for epi in LA
*be cautious of local with epi in pts who are sensitive to sulfite presrvatives
What analgesic is contraindicated in patients w/ Asthma?
Aspirin
ID the type of asthma:
- Stimulated by exertional activity
- Thermal changes during inhalation of cold air provoke mucosal irritation and airway hyperactivity
- Children and young adults are more severely affected because of their high level of physical activity
Exercise induced asthma
ID the type of asthma:
- Several respiratory viral infections during infancy and childhood can result in the development of asthma
- Causative agents of respiratory infections (bacteria, dermatologic fungi Trichophyton spp., and Mycoplasma organisms) can exacerbate asthma
- Treatment of the respiratory infection generally improves control of bronchospasm and constriction
Infectious asthma
Obstruction of airflow as seen in asthma occurs as the result of... (4)
- Bronchial smooth muscle spasm
- Inflammation of bronchial mucosa
- Mucus hypersecretion
- Sputum plugging
What is the primary macroscopic findings in the asthmatic lung?
Occlusion of the bronchi and bronchioles by thick mucous plugs
All of the following are histological findings of what?
(1) Thickening of the basement membrane (from collagen deposition) of the bronchial epithelium
(2) Edema
(3) Mucous gland hypertrophy and goblet cell hyperplasia
(4) Hypertrophy of the bronchial wall muscle
(5) Accumulation of mast cell and inflammatory cell infiltrate
(6) Epithelial cell damage and detachment
(7) Blood vessel proliferation and dilation
Asthma