disorders of the pancreas - tosto
1/51
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
first branch of superior mesenteric artery
pancreatoduodenal artery
gastric ulcer in posterior wall could damage
inflammation or infection of pancreas
pancreatitis
what is consumed in saponifcation
calicum → hypocalcemia, calcifications in chronic
inflammatory disease with little or no fibrosis
initiated by several factors:
acute cholelithiasis or ETOH abuse
acute pancreatitis
single or recurrent episode of pain
abdomen with elevated pancreatic enzymes
acute focal/diffuse swelling/inflammation
symptoms resolve after acute attack, blood biochem becomes normal
acute pancreatitis
GET SMASHED: GET part
gallstone: female, fat, fifty, fertile
ethanol
trauma: mva
GET SMASHED: SMASHED part
steroid
mumps/virus
autoimmune
scorpion bites
hyperlipidemia
ERCP
Drugs: so many, NSAIDS, thiazide diuretic
clinical presentations of acute panc
abdominal pain
N/V, bloating
low grade fever
guarding
tachy, tachypnea, hypotn, hyperthermia
elevated hematocrit, pre renal azotemia
abdominal pain in acute pancreatitis
epigastric pain
radiates to back, flank, chest, lower abdomen
worse in supine, better leaning forward
clinical sequelae of acute panc
respiratory sx: atelectasias, pleural effusions, ARDS
abdom: CULLEN sign (umbilicus bluish), Grey Turner (bluish flanks)
hypovolemic shock: 3rd spacing, hemorrhage, increased vascular perm, vasodilation, cardiac depresh, vomiting

grey turner and cullens sign
serum amylase: normal doesn’t exclude. nonspec. doesn’t predict severity
amylase
what best predicts disease severity in acute panc
BUN
found in pacna nd salivary glands, low levels in many tissues
may be normal , poor specificity
amylase
found predominantly in panc but also in gastric, intestinal mucosa, and liver
better specificity
2-3x normal level is good cutoff
lipase
renal failure and lipase
lipase is cleared by the kidneys so levels would be elevated
diagnosis acute panc: xray
rules out other diagnoses too
may see calcifications if chronic
may see sentinel loop, elevated hemidiaphragm, pleural effusion
US and acute panc
may detect gallstones
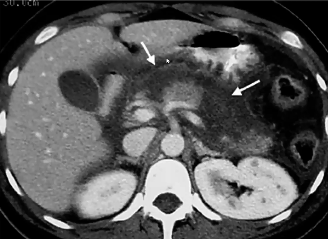
ct scan abdomen and acute panc
estimates severity and prognosis
complications → phlegmons, abscesses, pseudocysts. 2-3 wks after acute pancreatitis
pathophy of acute panc
central cause → acitvation of digestive zymogens in acinar cells and subsequent autodigestion of pancreas
and then they digest cellular membranes within pancreas → edema, interstitial hemorrhage, vascular damage, coag, and cellular necrosis
scoring criteria for panc
ranson’s criteria
also apache-2
biochemical markers and CT scan
RANSON CRITERIA Admission
age, wbc, glucose, LDH, AST
from first aid: Drugs generate a violent abdominal distress
Diuretics
glucocorticoids, valproate, alcohol, azithoprine
ranson crit wbc count
>18000
ranson criteria during first 48 hours
hematocrit
serum calcium
base deficity
increase in bun
fluid sequestration
ransons WBC admission
>18000
ranson glucose admission
>220
ranson ldh admission
>400
ranson admission AST
>250
ranson hematocrit drop
>10%
ranson serum calcium 48hrs
<8
ranson base deficit
>5.0r
ranson Increase in BUN
>2
ranson fluid sequestration
>4L
<2 pos signs ranson criteria
mortality rate is 0
3-5 positive signs ranson criteria
mortality rate is 10-20%
>=7 pos signs ranson criteria
>50% mortality rate
pancreatic necrosis
tx mild pancreatitis
rest
supp care
fluid resus → watch BP and urine output
pain control
NG tubes
refeeding (3-7 days)
tx severe pancreatitis
rest and supp care
fluid resus: may req 5-10 liters a day (norm is 2-3)
careful pulm and renal monitoring
maintain HCT of 26-30
pain ctl (pump)
correct electrolytes
prophy AB
nutritional support (may be NPO for weeks, TPN)
local complications of pancreatitis
abscess, pseudocyst, ascites, phlegmon
adjacent organ involvement
systemic complications
pulm effusions, hypoxemia, ards
myocardial depress, hemorrhage, hypovolemia
hypocalcemia, hyperglycemia, hyperlipidemia, coagulopathy
renal failure
gi hem
fat necrosis
irreversible damage to panc, incurable
chronic pancreatitis
70% of chronic panc caused by
ETOH
steady and boring pain, epigastric
not colicky
N/V
anorexia
malabsorption, weight loss
apancreatic diabetes
chronic pancreatitis
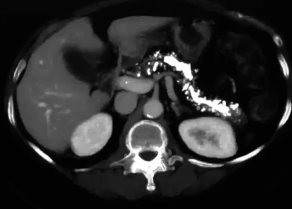
chronic pancreatitis calcifications
abnormally dilated ducts
chronic panc
minimally invasive test that allows simultaneous assessment of ductal and parenchymal structure
endoscopic ultrasound
noninvasive alternative to ERCP for imaging pancreatic duct
MRCP
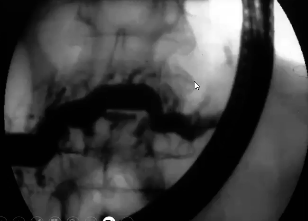
highly sens test for CP (radiographic)
ERCP
splenic and portal vein thrombosis
complication of chronic panc
tc for chronic panc
stop alcohol
enzyme tx
analgesia
ppis
surg,