essay 5 - Pain - definition, etiology, classification. Pathways o superficial and deep somatic pain
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
20 Terms
Give definition of pain
Pain is a complex, unpleasant sensory and emotional experience associated with actual or potential tissue damage.
IASP (international association for the study of pain) definition: an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.
Kitchel (1987) def: a subjective interpretation of nerve impulses induced peripherally by a stimulus that is actually or potentially noxious to tissue
define pain threshold and pain tolerance
pain threshold: the minimal intensity at which a stimulus is perceived as painful
Pain tolerance: the maximum intensity or duration of pain that a person is willing to endure before responding overtly
what are some influences on pain tolerance?
decreased by: fatigue, anxiety, fear, sleep deprivation, repeated exposure
inceased by: alcohol, medication, hypnosis, warmth, distractions, belief/faith
pain perception depending on age and sex
newborn > adults
adolescents < adults
elderly report pain more than younger adults
women > men in perceived pain intensity
what are the different pathways of pain (neuroanatomy)?
afferent pathway
primary afferent fibers
major ascending pain pathways
describe the afferent pathway
pain begins with activation of nociceptors (pain receptors) which transmit signals via afferent nerve fibers to the spinal cord.
Sensor receptors:
— exteroceptive: skin and mucosa
— Interoceptive: internal organs
— Proprioceptive: position of body parts
Nerve impulse transmission:
resting potential: neuron at rest
action potential: sodium enters → depolarization
repolarization: potassium exits
hyperpolarization: neuron overshoots
refractory period: ion return to resting state
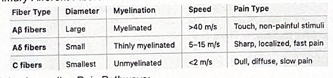
Describe the primary afferent fibers
alpha beta
alpha delta
c fibres
describe the major ascending pain pathways
spinothalamic tract: from body to brain (sharp, local pain)
spinoreticular tract/spinoparabrachial tract: carries dull, aching pain
trigeminal system: or facial pain (via V1, V2, V3 branches)
what is Gate control theory (Melzack and wall)?
pain signals via alpha delta and C fibers synapse in the substantia gelatinosa (SG) in the spinal cord
SG acts as a gate:
— closed gate: decrease t-cell simulation → decrease pain perception
— open gate: increase t-cell simulation → increase pain perception
how is pain classified?
by cause
by type
pain classified by cause
Nociceptive pain - due to actual tissue damage
acute physiological: sharp, sudden pain from injury
pathophysiological: in inflamed/damaged tissues
neuropathic pain - nerve injury or disease
peripheral: e.g trigeminal neuralgia
central: e.g post-stoke pain
chronic pain - lasting >6 months
Includes physical + psychological components (depression, sleep disorders)
pain classified by type
Somatic pain
superficial (cutaneous): sharp, localized (skin/mucosa)
deep (muscles, joint, bones): dull, aching, poorly localized
Visceral pain= internal organs, poorly localized, often referred pain
thalamic pain = due to lesions in the thalamus (central processing)
Neuropathic pain = from damaged nerves (e. post-hepetic neuralgia)
referred pain= perceived in a different area than the actual source (e.g heart attack → jaw pain)
phantom pain= felt in limb or body pat that has been amputated
psychosomatic pain = real pain linked to motional or psychological factors
clinical features of pain
Acute pain response:
increased heart rate
increased blood pressure
sweating (diaphoresis)
dilated pupils
hyperglycemia
decreased gastric mobility and acid secretion
Chronic pain response:
Psychological changes: depression, anxiety, poor sleep, denial
Pain pathways (face vs body)
— Body = spinothalamic tract (from spinal cord o thalamus)
— face = trigeminal nerve → spinal trigeminal nucleus → thalamus
Describe acute pain response
Acute pain response:
increased heart rate
increased blood pressure
sweating (diaphoresis)
dilated pupils
hyperglycemia
decreased gastric mobility and acid secretion
describe the chronic pain response
Chronic pain response:
Psychological changes: depression, anxiety, poor sleep, denial
Pain pathways (face vs body)
— Body = spinothalamic tract (from spinal cord o thalamus)
— face = trigeminal nerve → spinal trigeminal nucleus → thalamus
describe the types of orofacial pain
typical facial pain: e.g trigeminal neuralgia
bone pain: e.g from tumor or fracture
muscle pain: e.g from bruxism or TMJ dysfunction
Inflammatory pain
Ischemic pain - pain caused by a lack of blood supply (ischemia) to a tissue
sensitization pain: increased response to repeated stimuli
describe the management of orofacial pain
pharmacological:
analgesics: NSAIDs, paracetamol
narcotics
antidepressants/ anticonvulsants: for neuropathic pain
anesthetics: topical or injectable
anti-inflammatoy/ anti-microbial/antiviral/antihistamine agents
muscle relaxants , vasoactive agents, neurolytic agents
physical therapy
ultrasounds
electrogalvanic simulation
sensory stimulation (TENS, acupuncture)
psychological support
hypnosis
behavioral therapy
stress management
what are the pharmacological ways of managing orofacial pain?
pharmacological:
analgesics: NSAIDs, paracetamol
narcotics
antidepressants/ anticonvulsants: for neuropathic pain
anesthetics: topical or injectable
anti-inflammatoy/ anti-microbial/antiviral/antihistamine agents
muscle relaxants , vasoactive agents, neurolytic agents
what physical therapy can be done to manage orofacial pain?
physical therapy
ultrasounds
electrogalvanic simulation
sensory stimulation (TENS, acupuncture)
what psychological support can be given to manage orofacial pain?
psychological support
hypnosis
behavioral therapy
stress management