1. Dental Plaque and Calculus Composition and Formation
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
Dental Plaque
a Biofilm
Primary etiologic factor in caries and periodontal disease
Communities of microorganisms
Highly organized complex microbial biofilm
Embedded in polysaccharide/glycoprotein matrix
Adheres to tooth surfaces
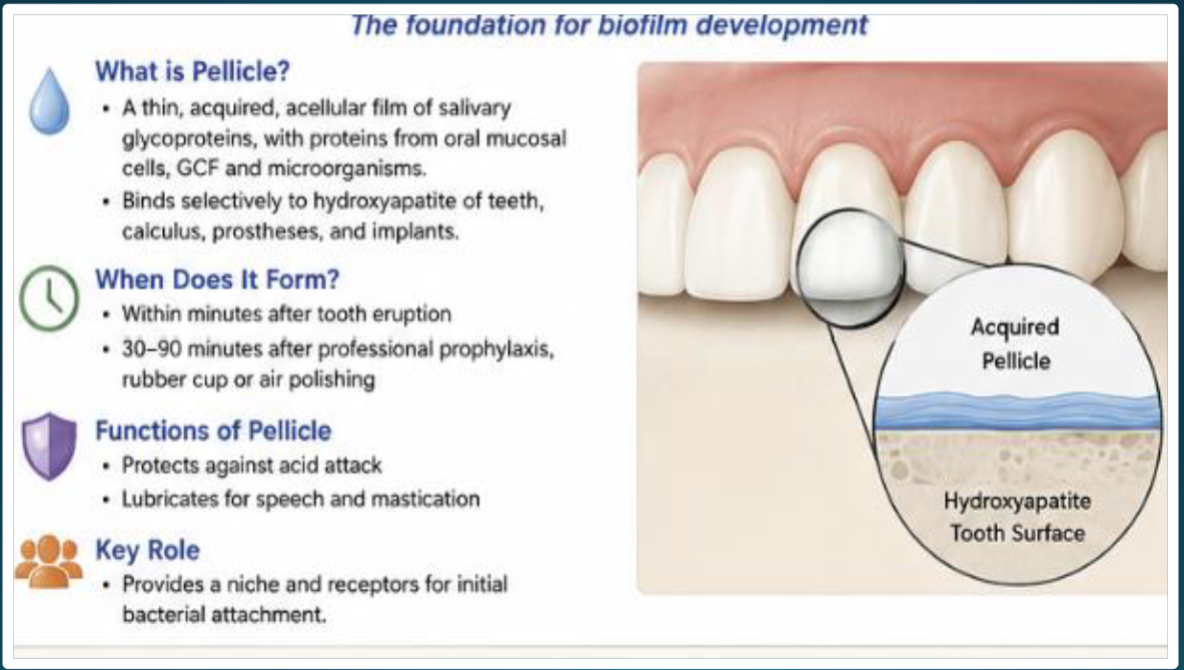
Oral Biofilm Formation Begins with
Acquired Pellicle
Key point: No bacteria are present initially—only the salivary protein film
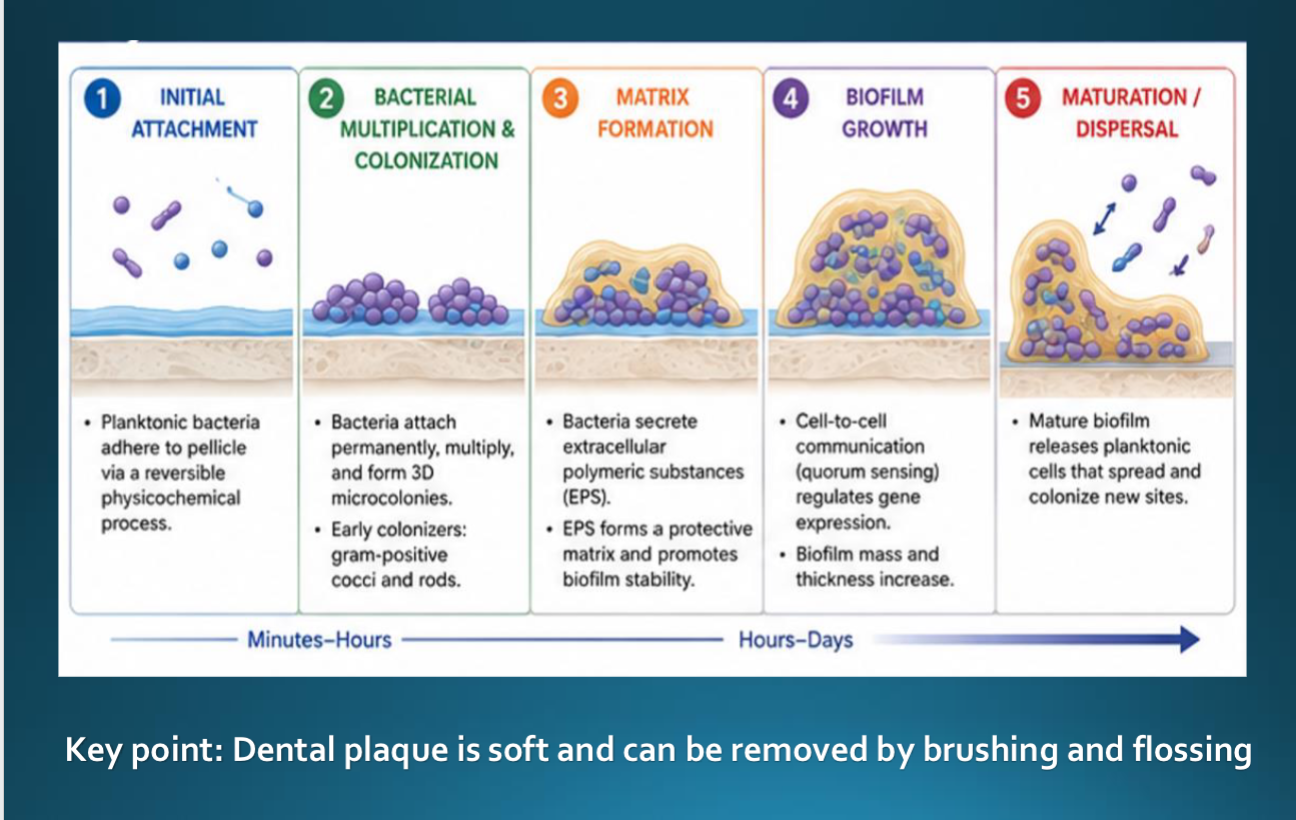
5 Stages of Biofilm Development
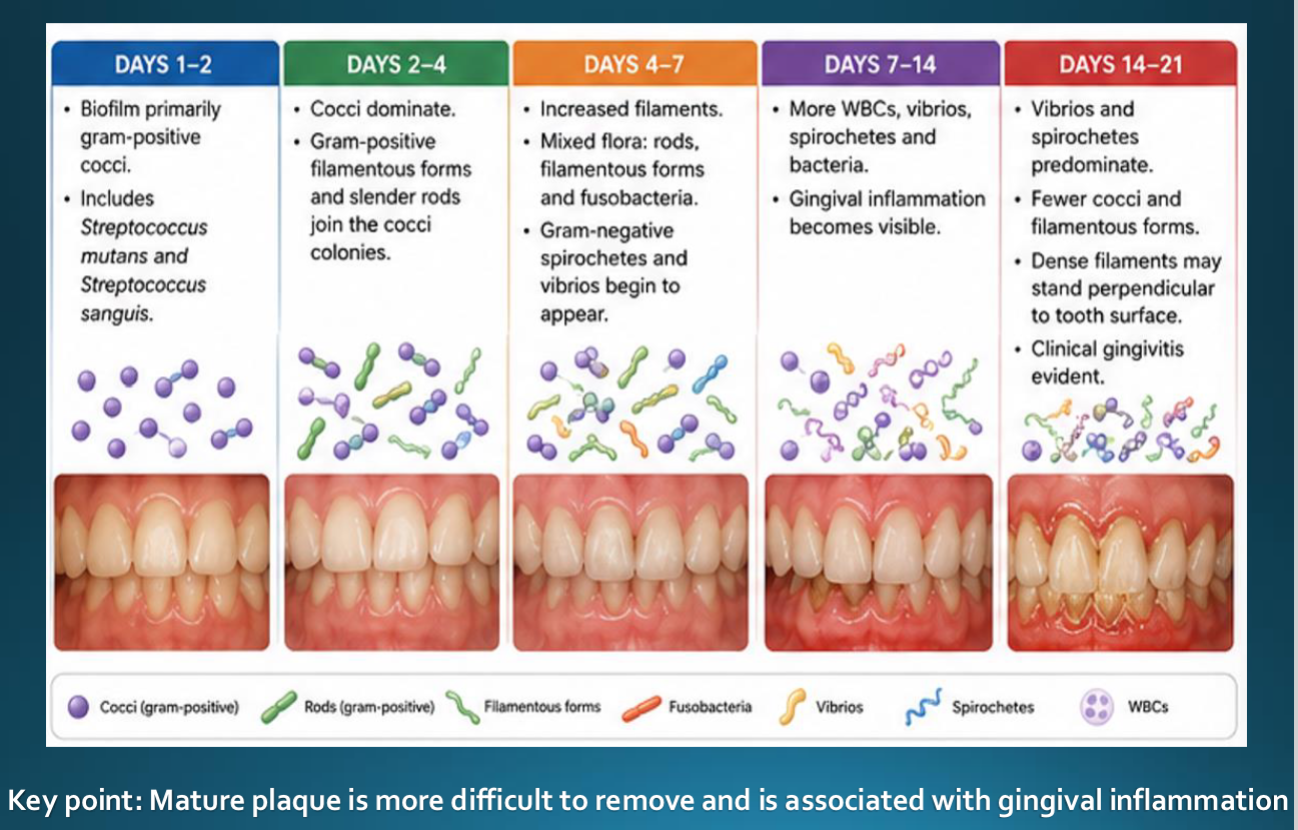
Changes in Oral Biofilm Microorganisms Over Time
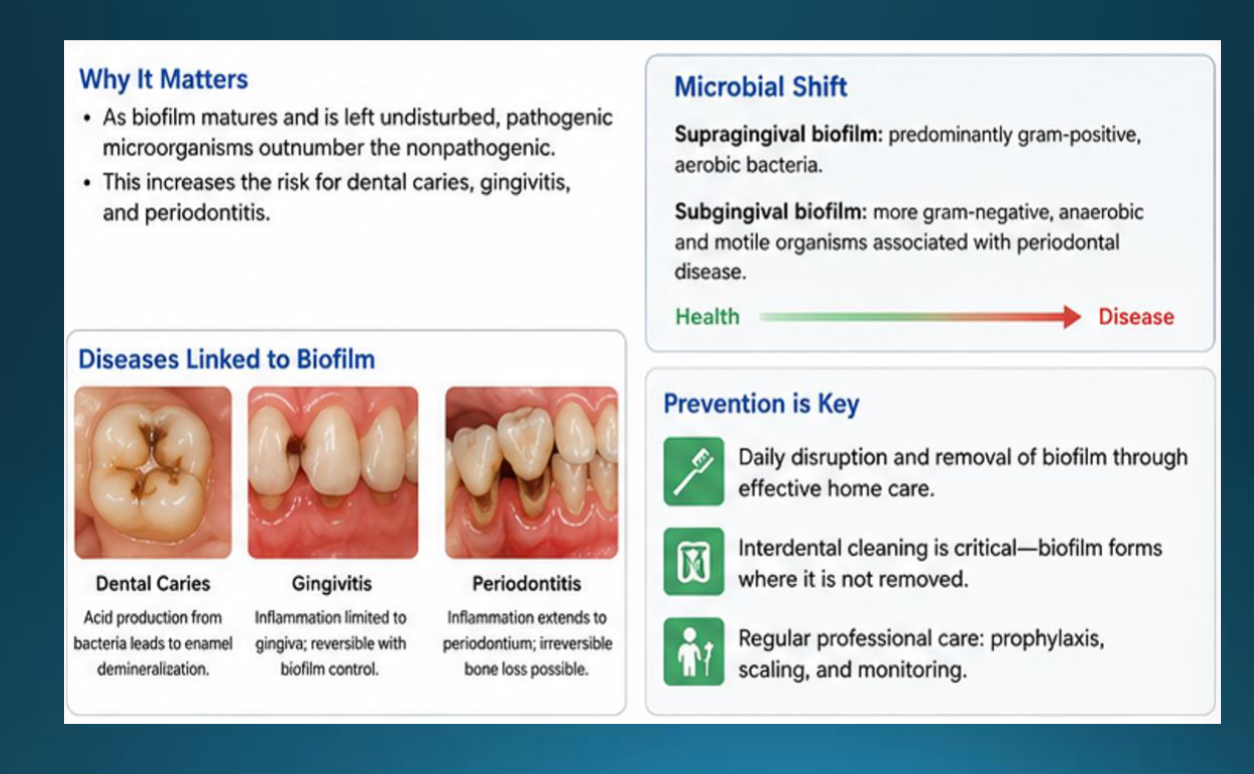
Oral Diseases Associated with Dental Biofilm
Supra vs Subgingival Plaque
Supra-gingival adherent above the gingival margin
Sub-gingival adherent below the gingival margin
Biofilm to Calculus
Pellicle → Plaque → Mineralization → Calculus
Dental Calculus
Mineralized dental biofilm is firmly attached to tooth surfaces and dental appliances
Why Dental Calculus Matters
Major plaque-retentive factor
Contributes to gingival inflammation
Increases periodontal disease risk
Impacts patient outcomes and maintenance
Stages of Calculus Formation
1. Acquired Pellicle formation
2. Biofilm accumulation
3. Mineral precipitation
4. Crystal growth and maturation
Mechanisms of Mineralization
Precipitation of calcium and phosphate
Seeding agents
Epitactic concept
Mineral transformation over time
Composition of Calculus
Organic: Bacteria, Proteins, Lipids, Polysaccharides
Inorganic: Calcium phosphate salts (~70–90%)
Major Crystal Forms
Hydroxyapatite
Magnesium whitlockite
Octacalcium phosphate
Brushite
Supragingival Calculus
White/yellow appearance
Salivary origin
Common near salivary ducts
Subgingival Calculus
Dark brown/black appearance
Gingival crevicular fluid increases with inflammation
Dense and firmly attached
Factors Influencing Formation
Saliva composition
Oral hygiene
Diet
Smoking
Biofilm retention areas
Clinical Detection
Explorers
Air drying
Radiographs
Tactile assessment
Periodontal Significance
Calculus does not initiate disease
independently but facilitates biofilm
retention and inflammation
Clinical Significance and Prognosis
Dental calculus serves as a plaque-retentive factor that facilitates continued biofilm accumulation and maturation.
Subgingival calculus is strongly associated with increased gingival inflammation, bleeding on probing, periodontal pocket formation, and clinical attachment loss.
Calculus removal is a fundamental component of nonsurgical periodontal therapy and supports resolution of inflammation.
Long-term periodontal stability depends on effective calculus removal combined with patient biofilm control and routine periodontal maintenance.
Prognosis improves when deposits are detected early and managed before significant periodontal destruction occurs
CDCA Clinical Expectations
Accurately identify and assess supragingival and subgingival plaque
and calculus deposits.
Demonstrate effective use of explorers and periodontal probes for
calculus detection.
Correlate radiographic findings with clinical calculus assessment.
Distinguish between burnished calculus and root surface anatomy.
Select appropriate instrumentation based on deposit location,
morphology, and accessibility.
Demonstrate complete removal of calculus while maintaining root
integrity and patient comfort.
Apply infection control and ergonomic principles during
instrumentation procedures.
Educate patients regarding biofilm control, calculus prevention, and
periodontal maintenance.
Evaluate treatment outcomes and determine the need for continuing
periodontal therapy
Key Takeaways
Dental plaque is a highly organized microbial biofilm and the primary etiologic factor in caries and periodontal disease.
Acquires pellicle forms within minutes and serves as the foundation for biofilm development.
As biofilm matures, microbial composition shifts toward more pathogenic species associated with inflammation and periodontal destruction.
Dental calculus is mineralized dental plaque composed primarily of calcium phosphate crystals.
Calculus itself is not pathogenic but serves as a plaque-retentive factor that promotes continued biofilm accumulation.
Supragingival and subgingival calculus differ in composition, location, appearance, and source of mineralization.
Effective periodontal therapy requires accurate detection and complete removal of calculus deposits.
Long-term periodontal stability depends on ongoing biofilm disruption, patient self-care, and professional maintenance