PHR 946 - Block 4: Advanced Cardiac Life Support (ACLS)
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
cardiac arrest
cessation of cardiac mechanical activity
- leads to no blood flow
cardiac arrest treatment goal
- bring patient from no blood flow → low-flow → return of circulation
- low-flow: intra-arrest; there is at least some blood flow to vital organs
BLS vs ACLS
basic life support (BLS)
- CPR
- defibrillation of shockable rhythms
- done outside of a hospital (typically)
advanced cardiac life support (ACLS)
- BLS +
- medication administration
- advanced airway
- done inside of a hospital (typically)
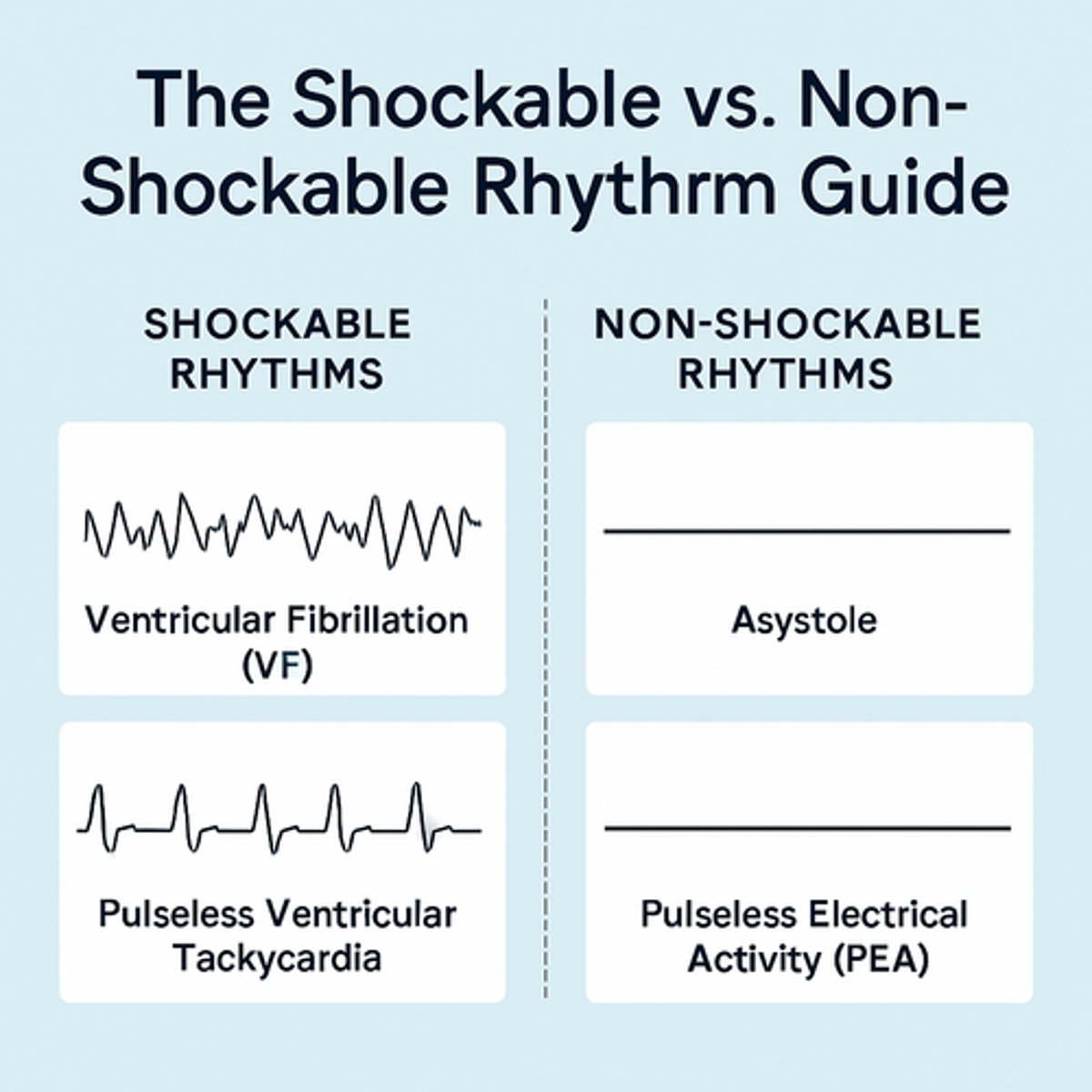
shockable vs unshockable rhythms
shockable
- pVT (pulseless ventricular tachycardia)
- VF (ventricular fibrillation/ Vfib)
unshockable
- PEA (pulseless electrical activity)
> can have many different EKGs
- asystole (flatline)
PEA (pulseless electrical activity)
- any organized rhythm on EKG WITHOUT a palpable pulse
- treatment: focus on high-quality CPR, identifying reversible causes, give epinephrine

asystole
- no electrical or mechanical activity of the heart
- no palpable pulse or blood pressure
- treatment: focus on high-quality CPR, identifying reversible causes, give epinephrine

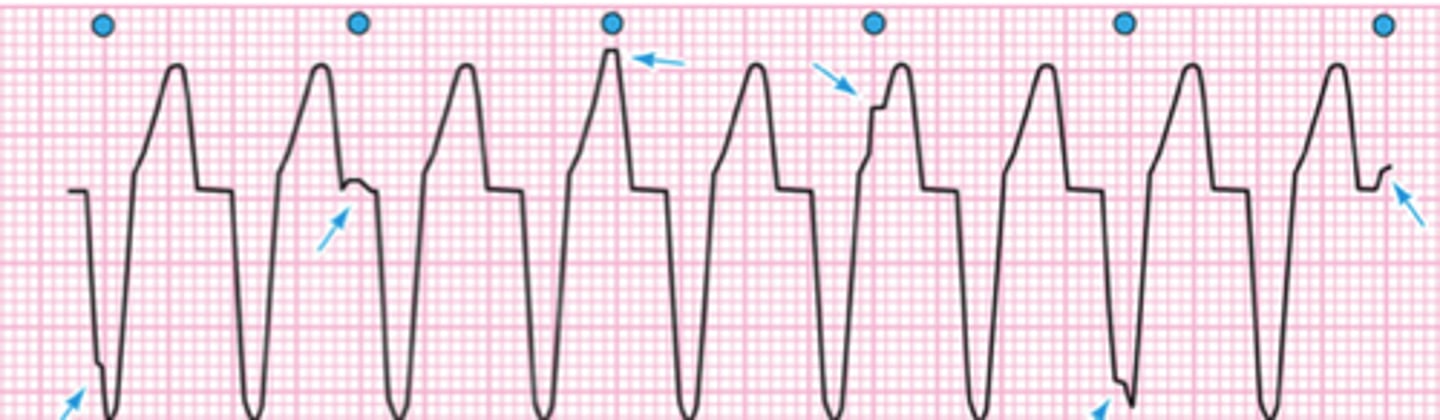
VT (ventricular tachycardia)
- may be perfusing rhythm (pulse) or non-perfusing (pulseless)
- rate: >100 bpm
- regular rhythm with no P waves and wide QRS
*looks like McDonald's arch: Mac attack = Vtach
VF (ventricular fibrillation)
- uncoordinated contraction of the ventricles
- no discernable rate or rhythm
- ALWAYS pulseless
- quivering, squiggles

ACLS algorithm
shockable rhythm
1. shock
2. CPR x2 mins
3. shock
4. CPR x2 mins
5. give epinephrine every 3-5 mins
> consider advanced airway, capnography
6. shock
7. CPR x2 mins
8. amiodarone or lidocaine
*can only give amio or lido after THREE shocks
unshockable rhythm
1. CPR x2 mins
2. give epinephrine every 3-5 mins
> consider advanced airway, capnography
3.. if shockable, go to #3 on above
if unshockable, CPR x2 mins
4. keep repeating if no sign of return of spontaneous circulation (ROSC)
chest compressions
1. push at least 2 inches & allow chest to completely recoil after each compression
2. compress at a rate of 100-120 compression/min
3. rotate compressors every 2 minutes or sooner if compressor is tired
4. minimize interruptions (<10 seconds)
5. quantitative waveform capnography (ETCO2)
> measures end-tidal carbon dioxide
> ensures effective compressions
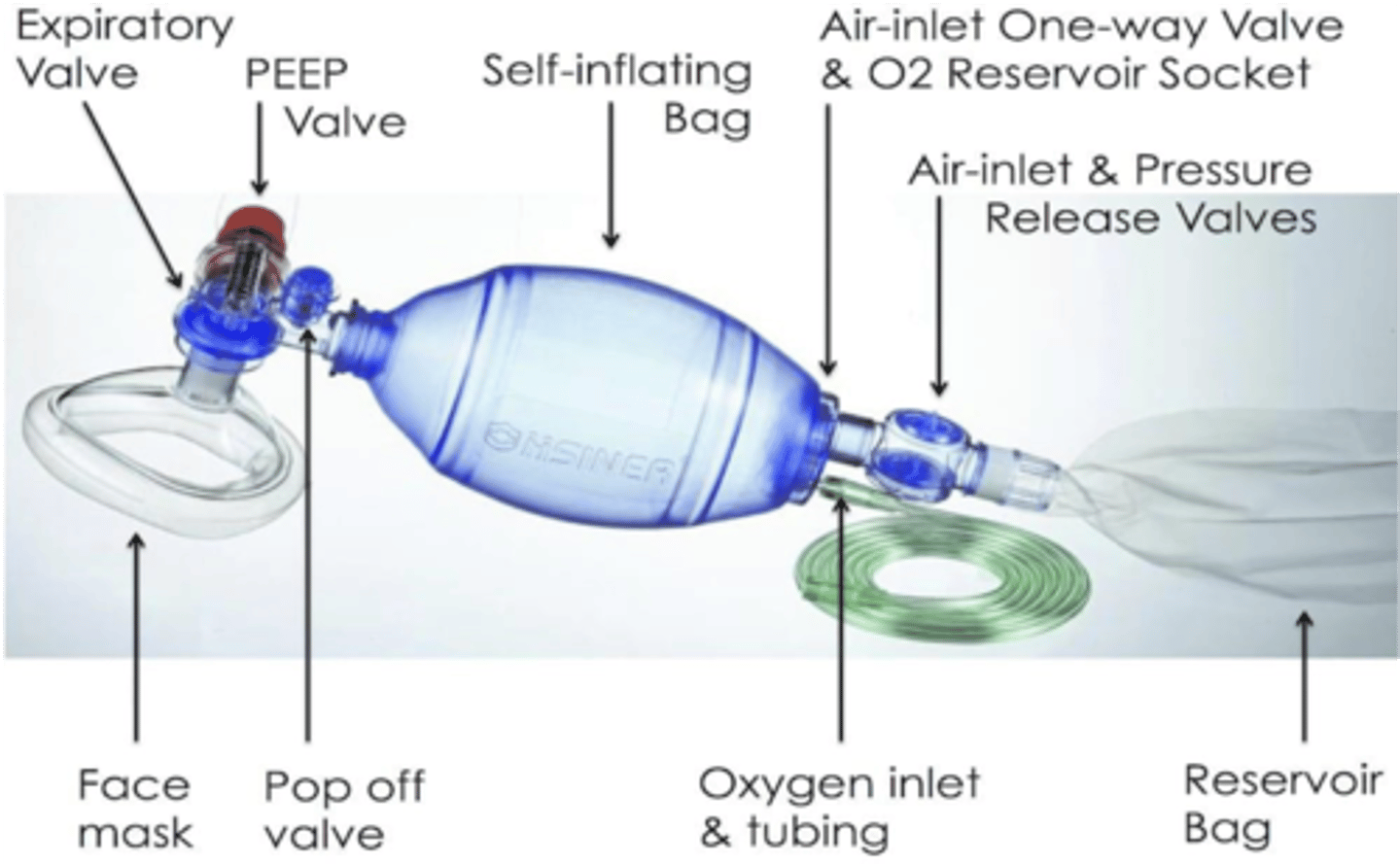
bag-valve-mask ventilation
- (Ambu bag) hand-held device commonly used to provide positive pressure ventilation to patients who are not breathing or not breathing adequately
- 30:2 compression:ventillation ratio
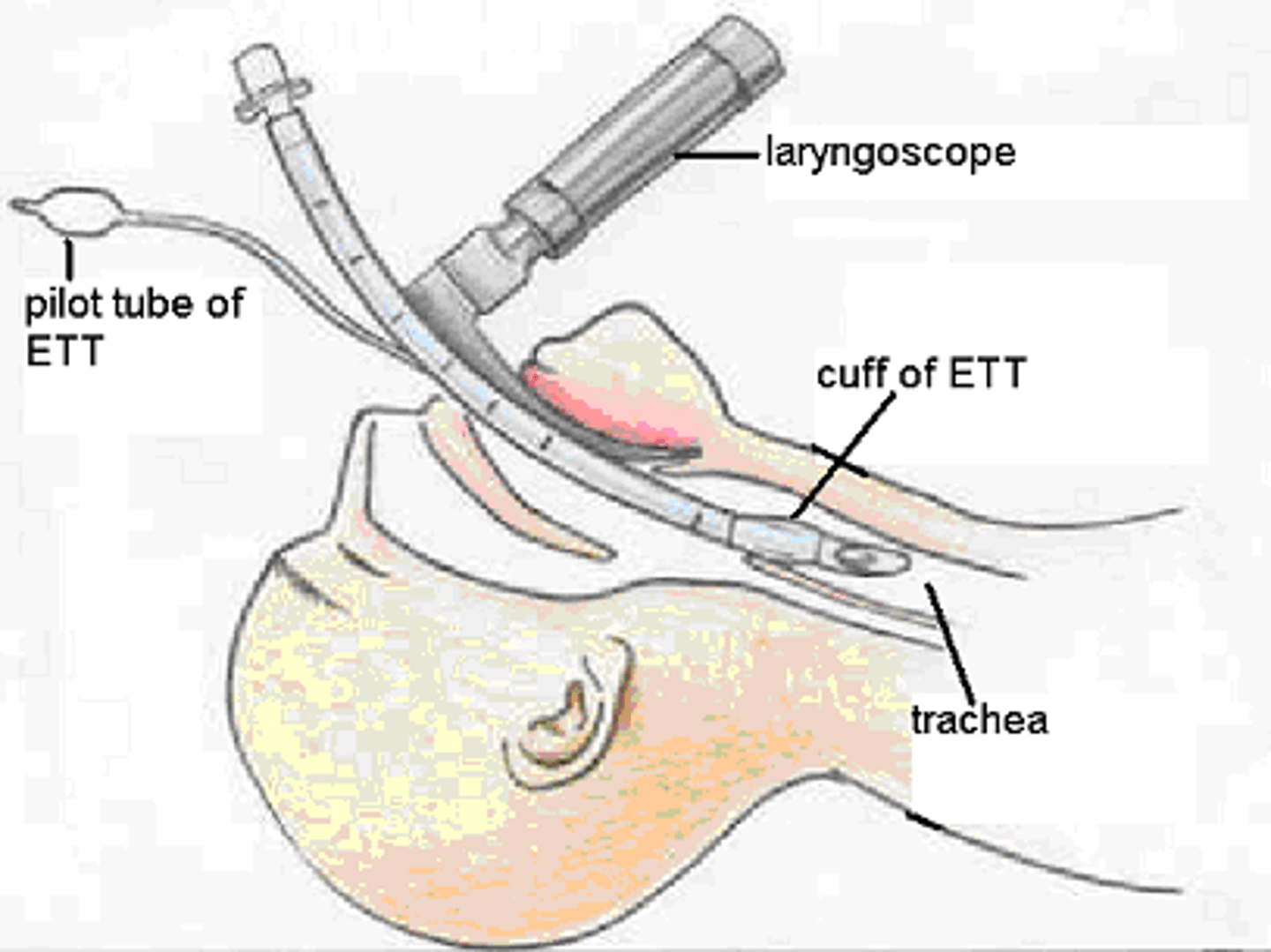
advanced airway management
advanced airway = endotracheal intubation
- used to secure a patient's airway + ensure oxygenation and ventilation
- rapid sequence intubation (RSI) medications: sedation, paralysis, and analgesia
epinephrine
- MOA:
> β-adrenergic receptor agonist: ↑ cardiac contractility and myocardial demand (pro arrhythmic)
> α-adrenergic receptor agonist: ↑ peripheral resistance (vasoconstriction) and coronary perfusion (benefit is here)
- dose: 1 mg IV/IO every 3-5 minutes
> can be given endotracheally if intubated: 2-2.5x the IV dose
- available as: PFS, vial

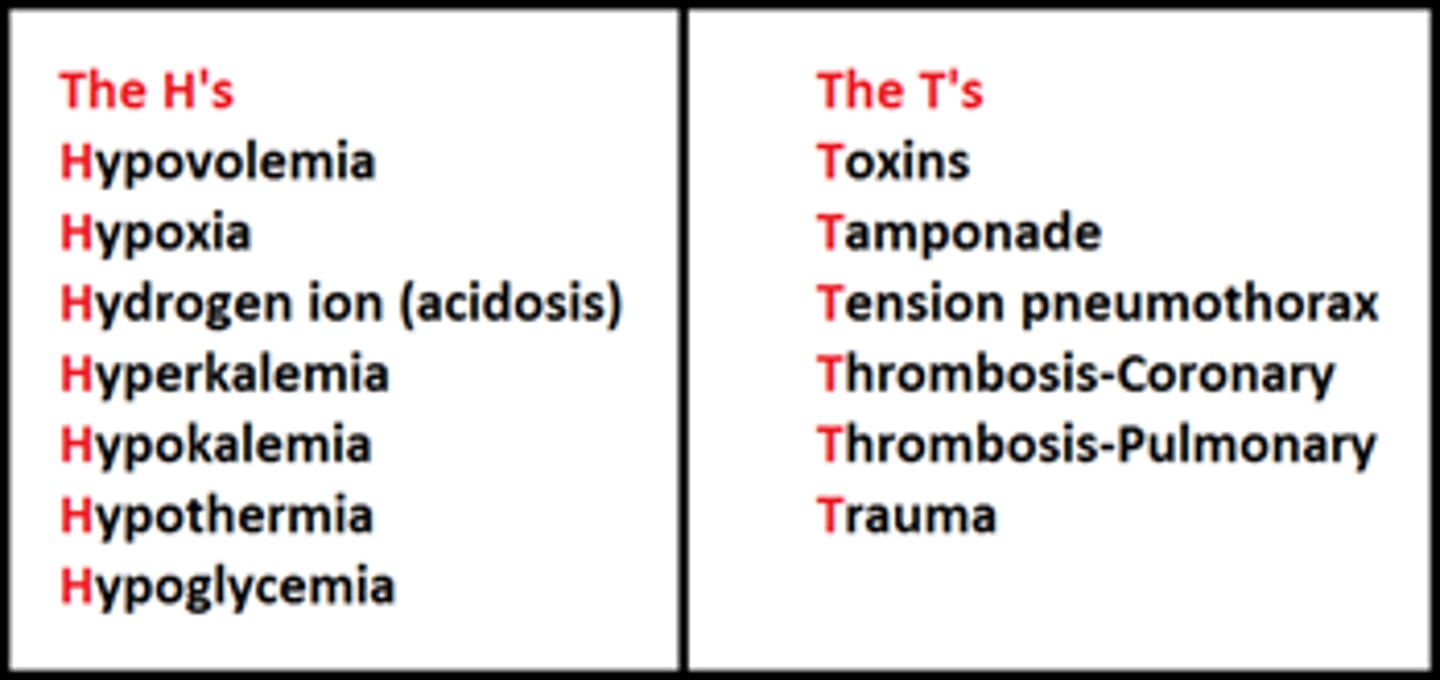
reversible causes of cardiac arrest
H's and T's
H
- hypoxia
- hypovolemia
- hypo/hyperkalemia
- hypothermia
- hydrogen ion (acidosis)
T
- thrombosis (cardiac)
- thrombosis (pulmonary)
- tamponade (fluid/blood/pus around pericardium)
- tension pneumothorax (air trapped in pleural space)
- trauma
- toxins
treatment of H's
- hypoxia → maintain airway
- hypovolemia → fluids/ blood
- hypokalemia → K replacement
- hyperkalemia → insulin/dextrose, Na bicarb, Ca chloride
- hypothermia → rewarming
- hydrogen ion (acidosis) → Na bicarb
treatment of T's
- thrombosis (cardiac) → cath lab
- thrombosis (pulmonary) → alteplase
- tamponade → pericardial drain
- tension pneumothorax → needle decompression
- trauma → surgery
- toxins → antidote
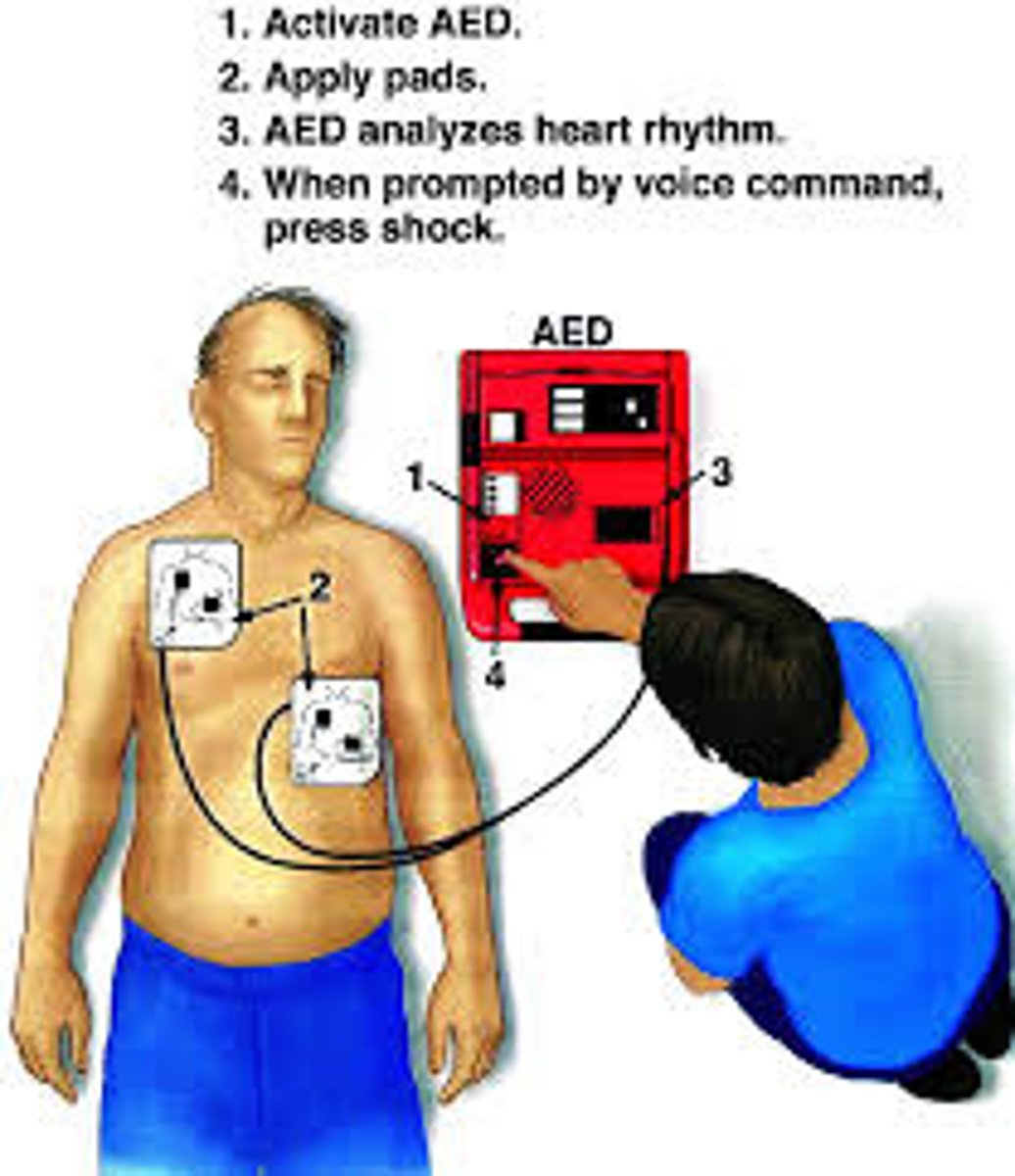
defibrillation
- application of an electric shock to the myocardium through the chest wall to restore normal cardiac rhythm
- pads are placed on either side of the heart
- early defibrillation is best
- may use an automated external defibrillator (AED) or a defibrillator (in the hospital)
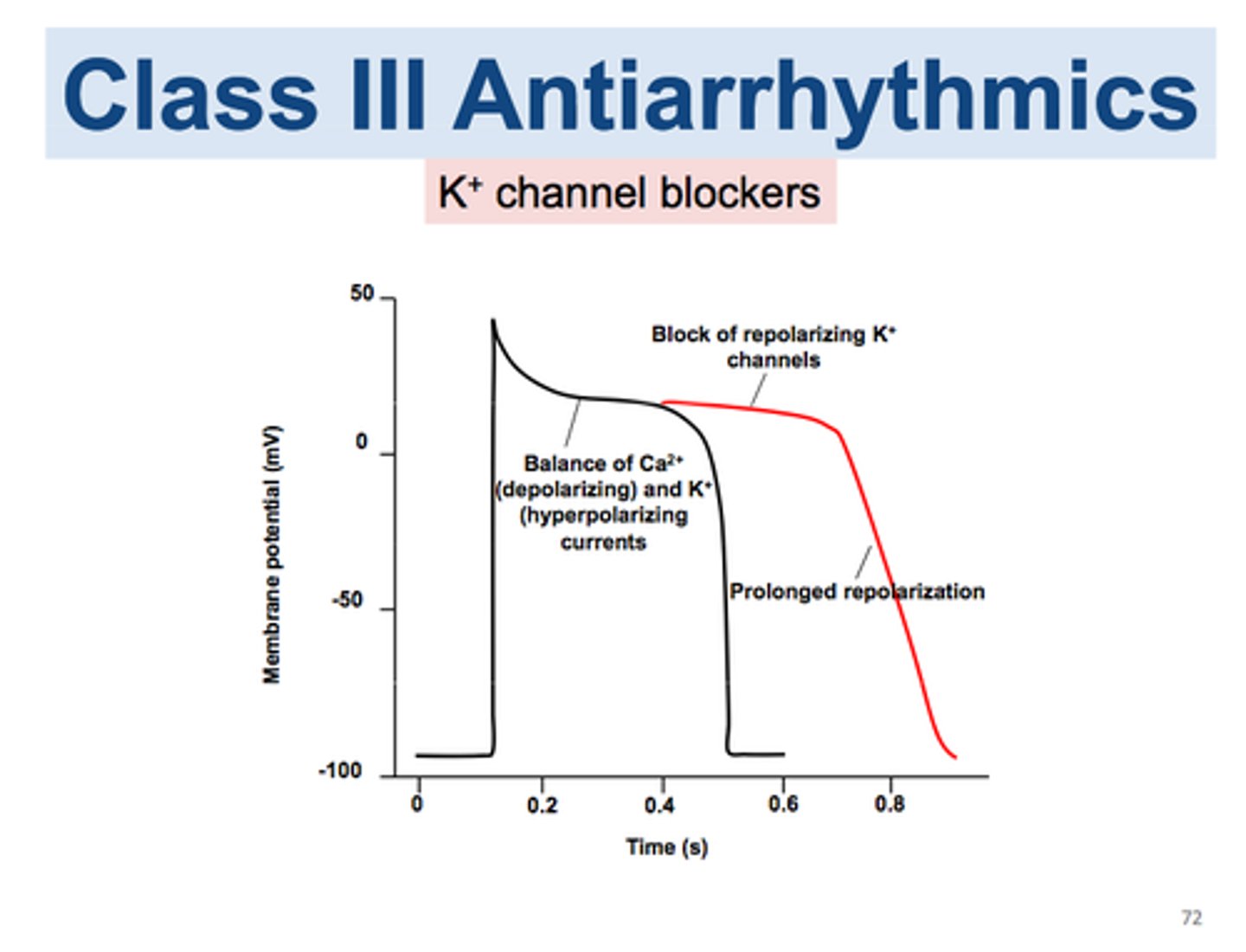
amiodarone
- shock x3, then can use this (or lidocaine)
- used for VF or pVT
- MOA: affects Na+/K+/ Ca²⁺ channels; has alpha and beta blocking properties
- dosing: 300 mg IV/IO for first dose, then 150 mg for second dose
lidocaine
- shock x3, then can use this (or amiodarone)
- used for VF or pVT
- MOA: affects Na+/K+ channels
- dosing: 1-1.5 mg/kg IV/IO for first dose, then 0.5-0.75 mg/kg
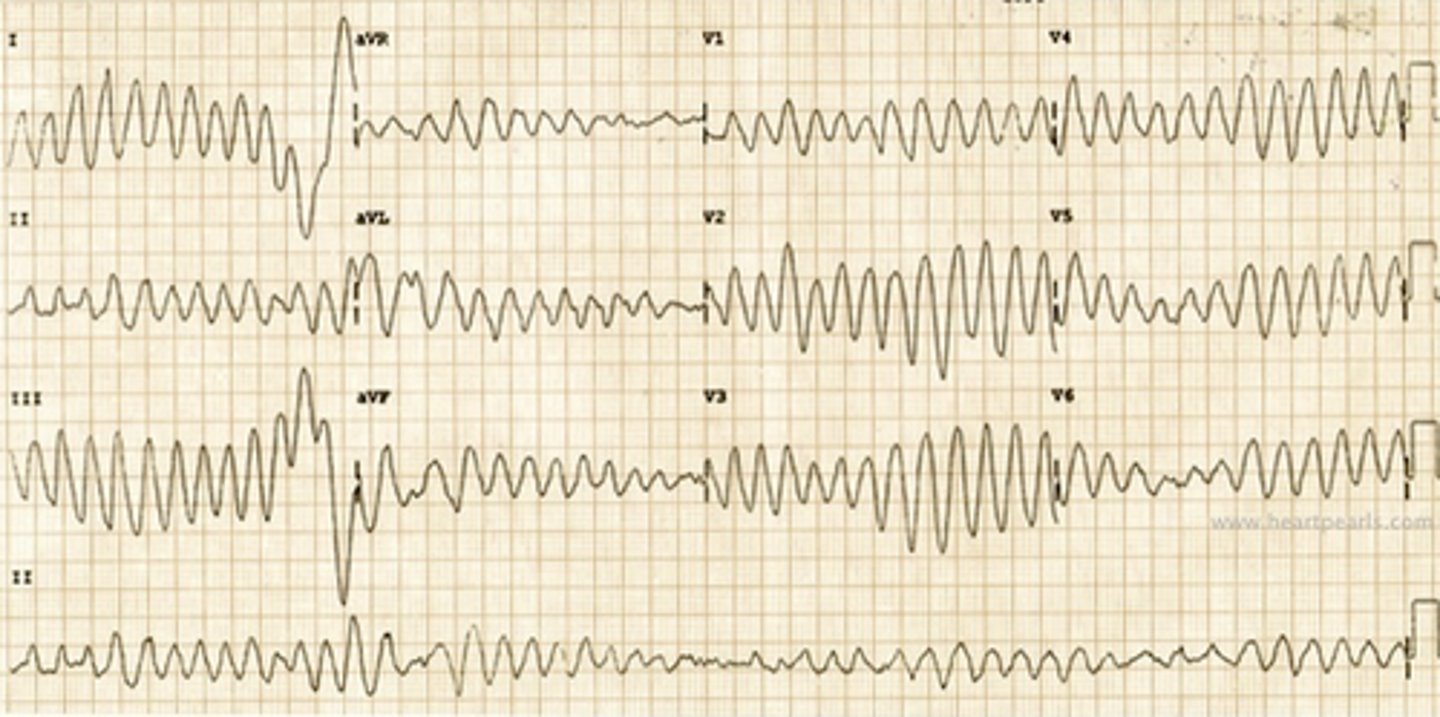
torsades de pointes (TdP)
- oscillatory changes in the amplitude of QRS complexes
- "twisting of the points"
- polymorphic pulseless ventricular tachycardia (pVT)
- commonly associated with medications, electrolyte imbalances, and QTc prolongation
- treatment: magnesium 1-2 g IV over 1-2 minutes
tachycardia management
HR >150 + pulse
1. identify and treat underlying cause
if symptomatic (hypotension, altered mental status, shock, chest discomfort, acute HF)
1. synchronized cardioversion
> consider adenosine
if asymptomatic
1. if wide QRS: consider adenosine or antiarrhythmic infusion
2. if normal QRS: use vagal maneuvers; consider adenosine, BB, or CCB
*if adenosine is given, it is given VERY fast
adenosine
- antiarrhythmic, used in tachycardia
- MOA: slows conduction time through the AV node
- dosing: 6 mg IV push, followed by 10 mL flush
> if no improvement, can repeat with 12 mg in 1-2 minutes
bradycardia management
HR <50 bpm + pulse
1. assess appropriateness for clinical condition, low HR is fine unless other issues are present!
2. identify and treat underlying cause
if symptomatic (hypotension, altered mental status, shock, chest discomfort, acute HF)
1. give atropine
2. if atropine ineffective: give transcutaneous pacing, dopamine infusion, or epinephrine infusion
3. consider expert consult or transvenous pacing
if asymptomatic
1. monitor and observe
atropine
- anticholinergic, given for bradycardia
- MOA: blocks the action of acetylcholine
- dosing: 1 mg every 3-5 minutes (max 3 mg)
opioid-associated emergency management
1. if suspected opioid overdose: check for responsiveness, shout for help, activate emergency response system, and get naloxone + AED if available
if person is breathing
1. prevent deterioration (keep airway open, person alert, may use naloxone, transport to hospital)
if person is not breathing normally
1. check for pulse
if pulse
1. support ventilation (keep airway open, rescue breath)
2. give naloxone
if no pulse
1. start CPR
2. use an AED
naloxone
- for opioid reversal
- MOA: competitive antagonist that displaces opioids at opioid receptor sites
- dosing: 0.4-2 mg IV/IM or 4 mg IN
> can repeat every 2-3 minutes
medication routes of administration
- intravenous (IV): central is preferred if available
- intraosseous (IO): emergency route, special needle is inserted into bone; IV dose = IO dose
- endotracheal (ET) tube: only certain meds can be given; dose is 2-2.5x IV dose
N naloxone
A atropine
V vasopressin
E epinephrine
L lidocaine