Caring for clients w/ impaired tissue integrity-JZ
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
Tissue Integrity
the ability of the body to regenerate & maintain normal physiologic functioning
Skin Integrity
unimpaired condition of the skin
Impaired Skin Integrity
altered dermis &/or epidermis indicated destruction of a skin layer(s)
Risk Factors for Impaired Tissue Integrity
aging
mobility/immobility
nutrition
chronic illness
miscellaneous
Aging Risk Factors
loss of skin elasticity & adipose tissue
drying of the skin
Mobility/Immobility Risk Factors
reducing circulation, atrophy, & impaired sensation
pressure
incontinence
Nutrition Risk Factors
obesity malnutrition
Chronic Illness Risk Factors
hepatic, renal, CV disorders
altered elimination patterns
Miscellaneous Risk Factors
smoking
stress
genetics
previous injury
medications
Assessing the Skin
essential component of whole pt. assessment
Admission Skin Assessment
head-to-toe skin assessment
conducted by 2 nurses
admitting nurse
primary nurse
Shift Skin Assessment
conducted by primary nurse
What are we Assessing?
temperature
turgor
color
moisture
skin integrity
Special considerations
bony prominences
occiput, scapula, sacrum, heels
skin beneath & around devices
oxygen tubing (behind ears)
braces (shin, arms)
skin to skin areas
back of knees, inner thighs, buttocks
all areas where the pt.
lacks sensation
has skin folds
has had previous breakdown
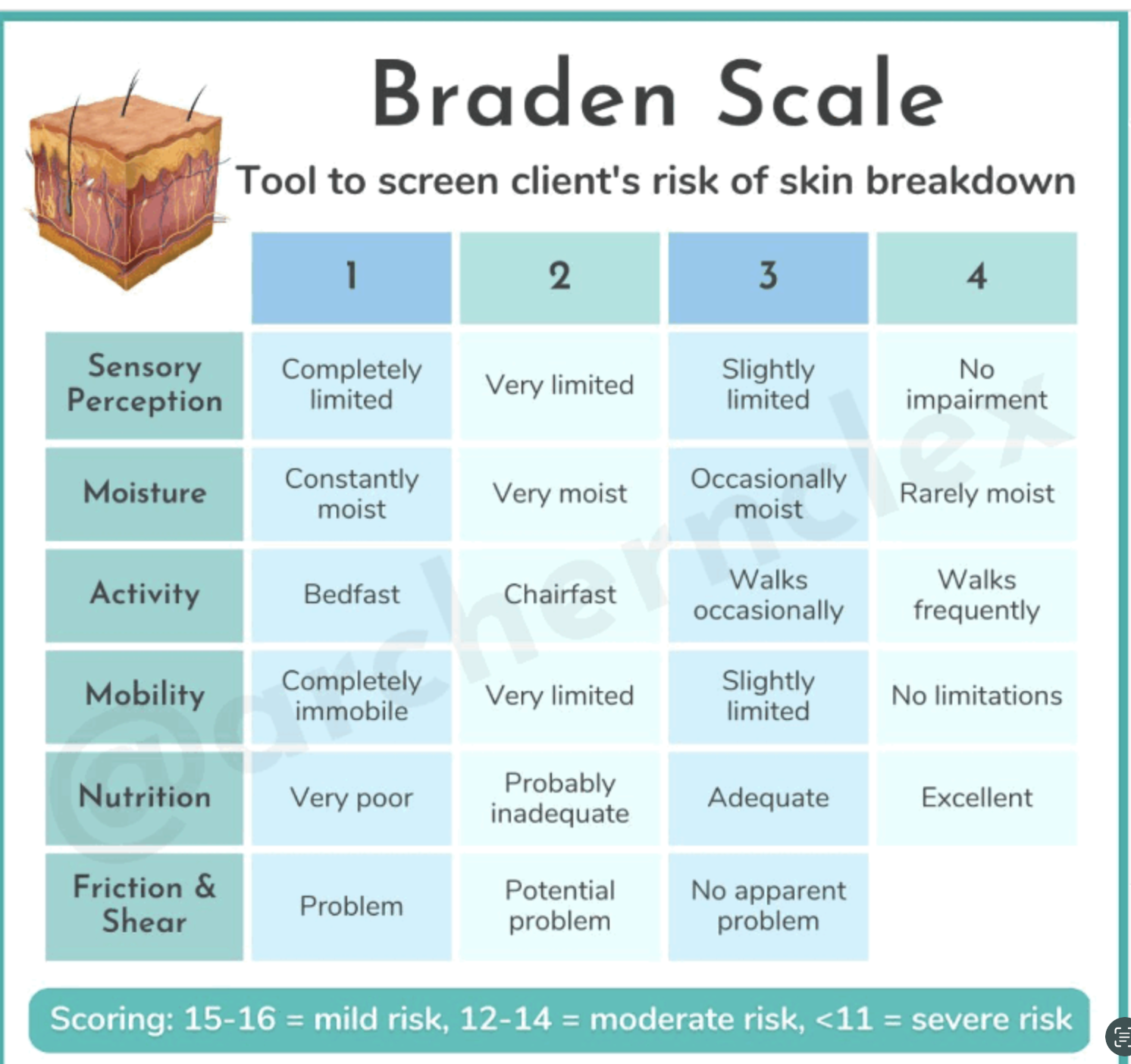
Conducting A Risk Assessment: Braden Scale
assesses for risk of 6 categories
sensory perception
moisture
mobility
nutrition
friction/shear
lower the score = greater the risk
Braden Scale
Promoting Skin Integrity
avoid skin trauma
while in bed
assess every 2 hours
HOB <30 degrees w/ knees bent; lower extremities elevated
pad bony prominences
offload/float heels
use specialty equipment
beds
padding (boots)
while in chair
chair/seat cushion
mobilization
ambulate, ears & often
encourage frequent weight shifting
do NOT slide - increases risk for shearing due to friction
Promoting Skin Integrity Healing
maintain skin hygiene
use Braden Scale assessment tool Q shift
cleanse skin w/ pre-packaged wipes or warm water
cleanse immediately following incontinence
use barrier sprays/creams
do NOT massage bony prominences
ensure proper nutrition
protein intake
nutritional supplements
interprofessional collaboration
wound nurse
Types of Wounds: What to look for
pressure injuries
moisture associated skin damage
venous ulcers
arterial ulcers
diabetic foot ulcers
other wounds
abrasions
skin tears
lacerations
lesions
surgical wounds
burns
Pressure Injury
injury to the skin & underlying tissue resulting from prolonged pressure or pressure & shear
occurs over bony prominences (calcaneus, coccyx, elbow)
HAPI = Hospital Acquired Pressure Injury
Pressure Injury: Staging
Stage 1
Stage 2
Stage 3
Stage 4
unstageable
deep tissue injury
Moisture- Associated Skin Damage (MASD)
inflammation or skin erosion caused by prolonged exposure to a source of moisture
urine
stool
sweat
wound drainage
saliva
mucus
treatment
exudate management
absorbent dressings
barrier creams
Venous Ulcers
most commonly form around the ankles due to a problem w/ circulation (PVD)
treatment
compression stockings/wrap
leg elevation
smoking cessation
weight loss
exercise
vascular referral for imaging
Arterial/Ischemic Ulcers
caused by poor perfusion (delivery of nutrient-rich blood) to the lower extremities
occur mostly on the lower legs & feet
usually originate from a small traumatic injury (hitting shin against table)
treatment
surgery
smoking cessation
blood sugar control
weight loss
Diabetic Foot Ulcers
most occur on plantar aspect of foot
occur due to combo of
neuropathy
poor circulation
foot deformities
pressure &/or friction
trauma
increased risk w/ longer duration of diabetes
treatment
surgery
offloading
blood sugar management
Other Wounds
abrasion
skin tear
maceration
lesion
surgical
burn
Types of Wound Healing
primary intention
secondary intention
tertiary intention
Types of Wound Healing: Primary Intention
1st intention or primary healing
little to no tissue loss
edges well approximated
low risk for infection
minimal scarring
Types of Wound Healing: Secondary Intention
2nd intention or secondary healing
loss of tissue
edges poorly approximated
heals from bottom up
granulation tissue
increased risk of infection/scarring
Types of Wound Healing: Tertiary Intention
delayed primary closure
uses combination of primary & secondary
used for dirty wounds at time of injury
Phases of Wound Healing
hemostasis
inflammation
proliferation
remodeling
Phases of Wound Healing: Homeostasis
stop bleeding
Phases of Wound Healing: Inflammation
prevention of infection
Phases of Wound Healing: Proliferation
new tissue growth
Phases of Wound Healing: Remodeling
wound closure
Complications of Wound Healing
infection
osteomyelitis
necrosis / grangrene
peri-wound dermatitis
edema
hematoma
dehiscence
Risk for Impaired Wound Healing
tissue perfusion
immunocompromise
infection
medications
malnutrition
chronic disease
diabetes
impaired oxygen deliveru
decreased hemoglobin
smoking
Wound Basics: Assessing the Wound
measuring
L x W x D
length = head to toe
width = side to side
depth = straight down into wound bed
use concepts of analog clock & anatomical position
wound edges
tunneling
undermining
observe the wound bed for
granulation
slough
eschar
Wound Drainage
exudate - fluid produced by the healing process
assess
amount - none, scant, small, moderate, large/copious
odor
consistency - thin/watery vs thick/sticky
color
serous - clear, watery
sersosanguineous - pale, blood tinged
sanguineous - bloody
bright
dark
purulent - thick, various colors
Wound Closures
sutures
staples
adhesives
negative pressure wound therapy
Choosing the Right Dressing
wound care = an order
moisture consideration
a wet wound bed = risk for infection
need to dry
dressing will be wet when removed
ex: gauze, foams, alginates
dry wound bed = won’t granulate
need to keep it moist
ex: wet-to-dry, hydrocolloids, hydrogels
goal: moist wound healing
Drains
used to decrease the accumulation of fluid, reduced inflammation, or collect fluid
classification
active or passive
open or close
types
penrose
jackson pratt (JP)
hemovac
Drainage Care
drainage
document: amount (mL), color, consistency, odor, & date/time
insertion site
monitor for s/sx of infection
cleaning
daily w/ NS unless order state otherwise
miscellaneous
monitor for kinking of tubing
regularly empty drain to maintain suction
secure drain