Human Movement and Movement Disorders
1/241
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
242 Terms
What is the job of the motor system?
To transform intentions into patterns of muscle activity. All movement is ultimately produced by muscle contraction.
What are the passive components of the motor system?
The skeleton — provides structure and stability, but also constraints on movement.
What are the active components of the motor system?
The CNS and muscles — responsible for planning, coordination, and execution of movement.
List the 6 challenges of movement control.
1. Noise in sensory system
2. Time delays between visual information & motor systems
3. Uncertainty (eg. where the object is exactly)
4. Multiple degrees of freedom (~200 joints + 600 muscles)
5. Time varying properties (e.g. tool use, fatigue)
6. Complex instability (e.g. raising an arm causes postural instability)
What is sensory noise vs motor noise?
Sensory noise = inaccuracy in what the brain perceives. Motor noise = variability in muscle force and timing.
What is an example of postural instability as a challenge in movement control?
Raising one arm causes postural instability — the body must compensate.
What is endpoint comfort?
the tendency of humans to plan movements (specifically grasping and manipulation) based on the efficiency and comfort of the FINAL posture, not the movement itself.
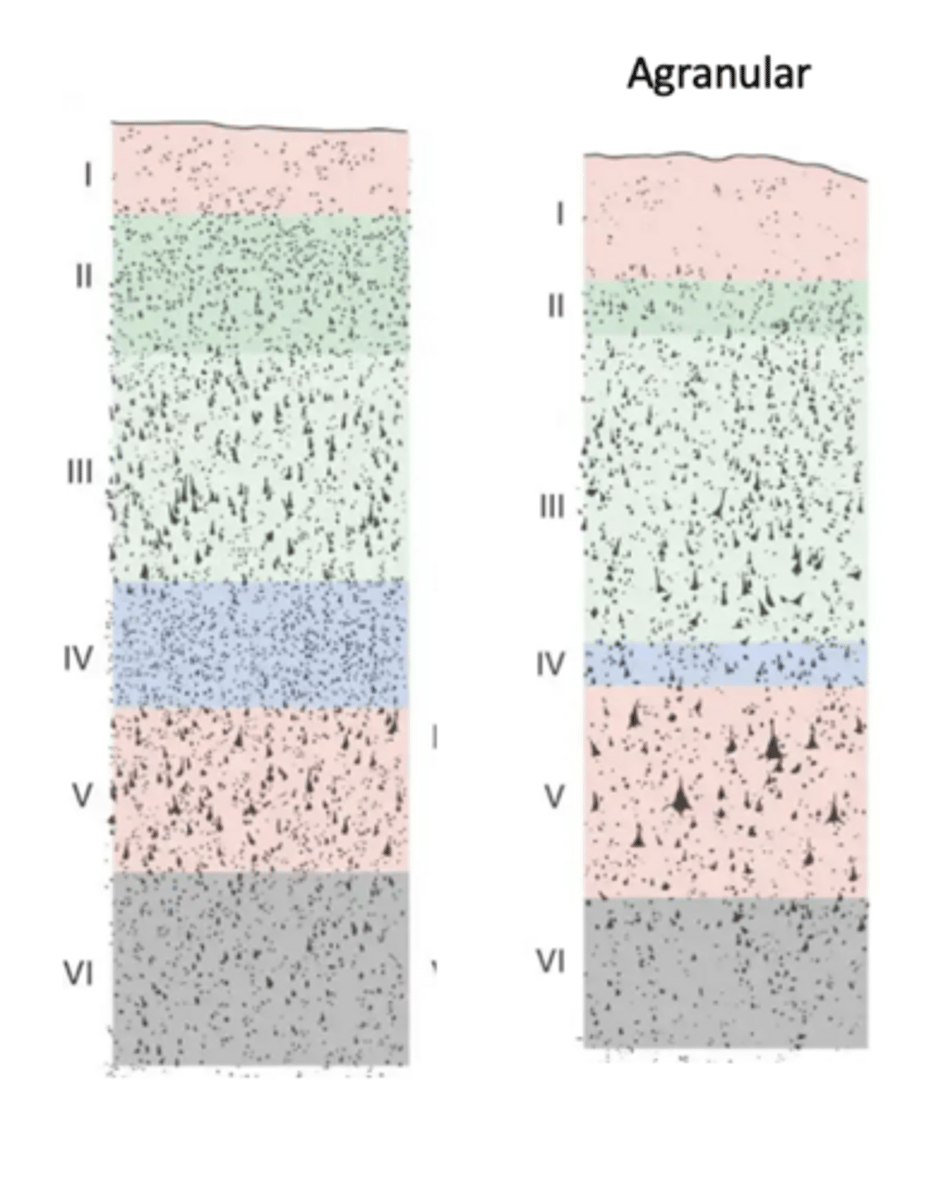
How many cortical layers does the primary motor cortex have?
Six — the same as all neocortex — but their organisation differs from sensory cortex.
Why is the primary motor cortex called agranular?
Layer IV (the granular layer) is largely absent, and layer III is relatively thin.
These two layers normally form the main ascending (info coming into the brain) sensory processing pathways so their reduction indicates that the motor cortex does not engage in serial reprocessing of incoming sensory information.
What do layers III and IV normally do in sensory cortex?
They form the main ascending sensory processing pathways — receiving and re-processing incoming sensory information.
What does the absence of layers III and IV in M1 mean functionally?
M1 does not engage in serial reprocessing of incoming sensory information — it is optimised to generate and transmit motor commands.
Which layer is highly developed in the primary motor cortex and what does it contain?
Layer V — contains giant pyramidal Betz cells that form the main descending output pathways.
What are Betz cells?
The largest neurons in the CNS. They are upper motor neurons whose axons descend via the corticospinal tract to spinal motor neurons. Can reach up to 100 μm in diameter.
What is the corticospinal tract?
The principal descending motor pathway — transmits voluntary motor commands from the cerebral cortex to spinal motor neurons.
From which cortical layer do all corticospinal fibres arise?
Layer 5 of the neocortex — but NOT just from M1.
What is the breakdown of origins of corticospinal fibres?
30% from primary motor cortex; 30% from premotor cortex; 40% from somatosensory cortex in the parietal lobe & cingulate gyrus
Describe the route of corticospinal fibres from cortex to spinal cord.
Cortex → descend through internal capsule → midbrain → pons → pyramids of the medulla oblongata → decussation → spinal cord.
What is decussation and where does it occur in the corticospinal tract?
Decussation = crossing to the opposite side. Occurs at the level of the medulla oblongata.
After decussation, what tracts do the fibres form?
90% form the lateral corticospinal tract; 10% form the anterior corticospinal tract
What structure do all corticospinal fibres pass through?
The internal capsule then the medulla oblongata.
What supplies the internal capsule?
The lenticulostriate arteries.
Why are the lenticulostriate arteries clinically important?
They are vulnerable to narrowing in chronic hypertension. Narrowing causes ~17% of strokes via small punctate infarctions or haemorrhages in the internal capsule → can produce severe motor deficits because they damage many corticospinal fibres concentrated in a small area
In what 3 ways do corticospinal fibres differ from each other?
- Types of fibres (e.g. cortico-spinal vs cortico-cortical)
- Levels of myelination (94% are myelinated)
- Size (3% large diameter 11-20 μm → >50 m/s = conducts faster; rest small diameter 1-4 μm → ~14 m/s)
What is a monosynaptic connection?
A single synapse between a sensory neuron and a motor neuron. No interneurons in between.
What are corticomotoneuronal (CM) cells?
Neurons from the primary motor cortex that make direct monosynaptic connections with α-motor neurons in the spinal cord.
What is the functional role of the corticomotoneuronal pathway?
First appeared in higher primates. Crucial for hand dexterity and fractionated digit movements (e.g. precision grip).
Which species has the highest number of CM cells and why is this significant?
Humans — particularly for hand muscles. Explains our superior fine motor abilities.
What are polysynaptic connections in the corticospinal tract?
Corticospinal fibres terminate on interneurons within the spinal cord, which then relay to motor neurons.
What is convergence in the corticospinal system?
Multiple descending fibres from different cortical regions influence the same motor neuron — allows integration of information.
What is divergence in the corticospinal system?
A single corticospinal neuron influences multiple motor neurons enabling coordinated activation of several muscles.
What are muscle synergies?
Groups of muscles activated together as functional units. Simplifies motor control and allows efficient, stable movement.
What does the association cortex (prefrontal + posterior parietal) contribute to movement?
Defines goals and intentions — the WHY of movement. Not strictly involved in producing movement itself.
What are the secondary motor cortices and how do they contribute?
Premotor Cortex (PMC) and Supplementary Motor Area (SMA)
Transform abstract intentions into movement patterns (HOW) and convert them into motor commands for M1.
Describe the hierarchical organisation of motor cortical areas
At the bottom, M1 directly executes voluntary movements — the most specific, concrete role. Above it, the secondary motor cortices (PMC + SMA) plan and select appropriate motor patterns, activating before M1 and translating intentions into movement sequences. At the top, the association cortex defines goals and intentions
As you travel upwards specificity and compelexity of function increases
What does the primary motor cortex (M1) do?
Integration, automation, and coordination — the actual execution (Action).
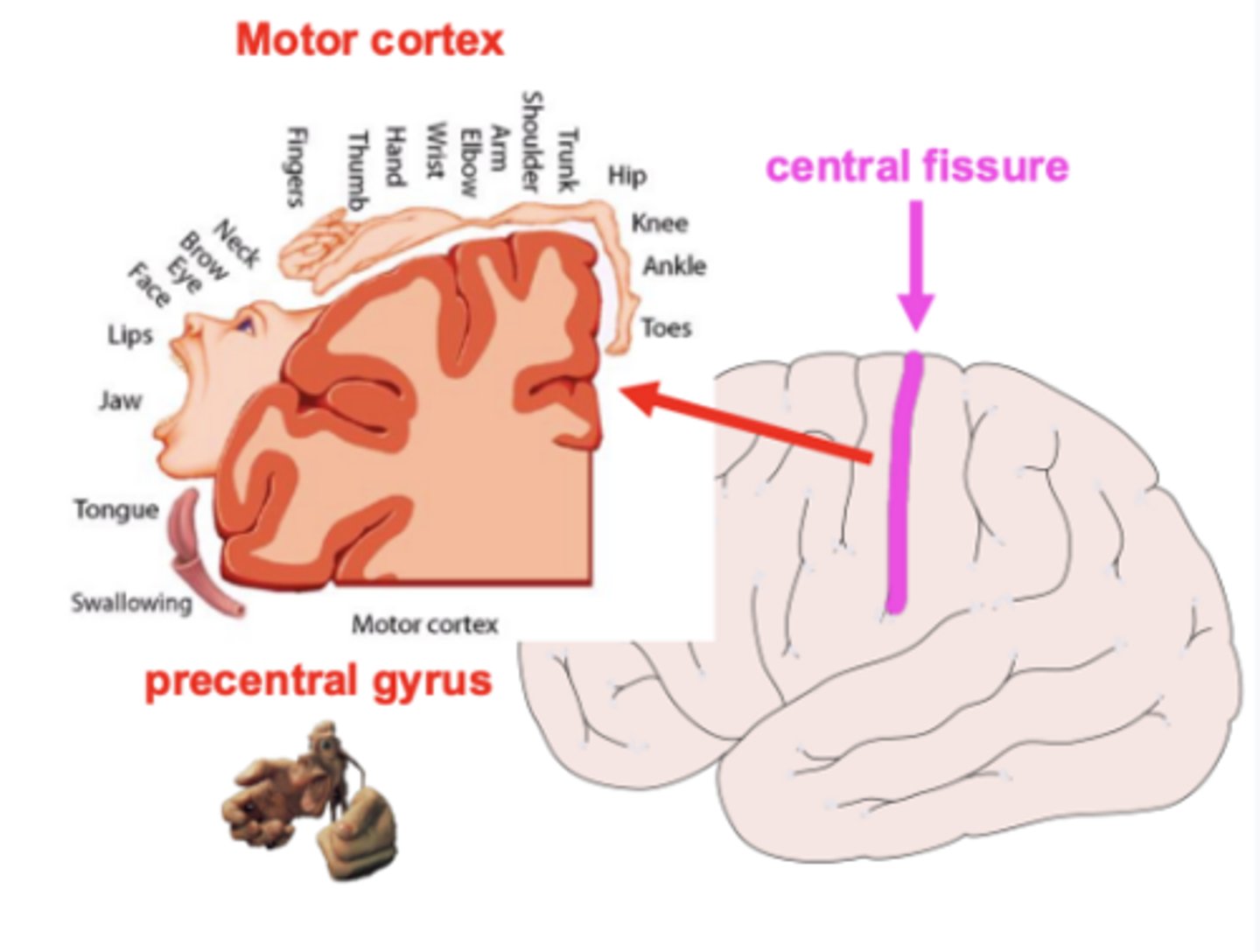
Where is M1 located?
In the precentral gyrus of the frontal lobe.
What inputs does M1 receive?
From other cortical motor areas, subcortical areas, and the cerebellum.
When is M1 active?
During execution of voluntary movements.
What is the motor homunculus?
The somatotopic map of the body in M1 — different regions of M1 correspond to different body parts.
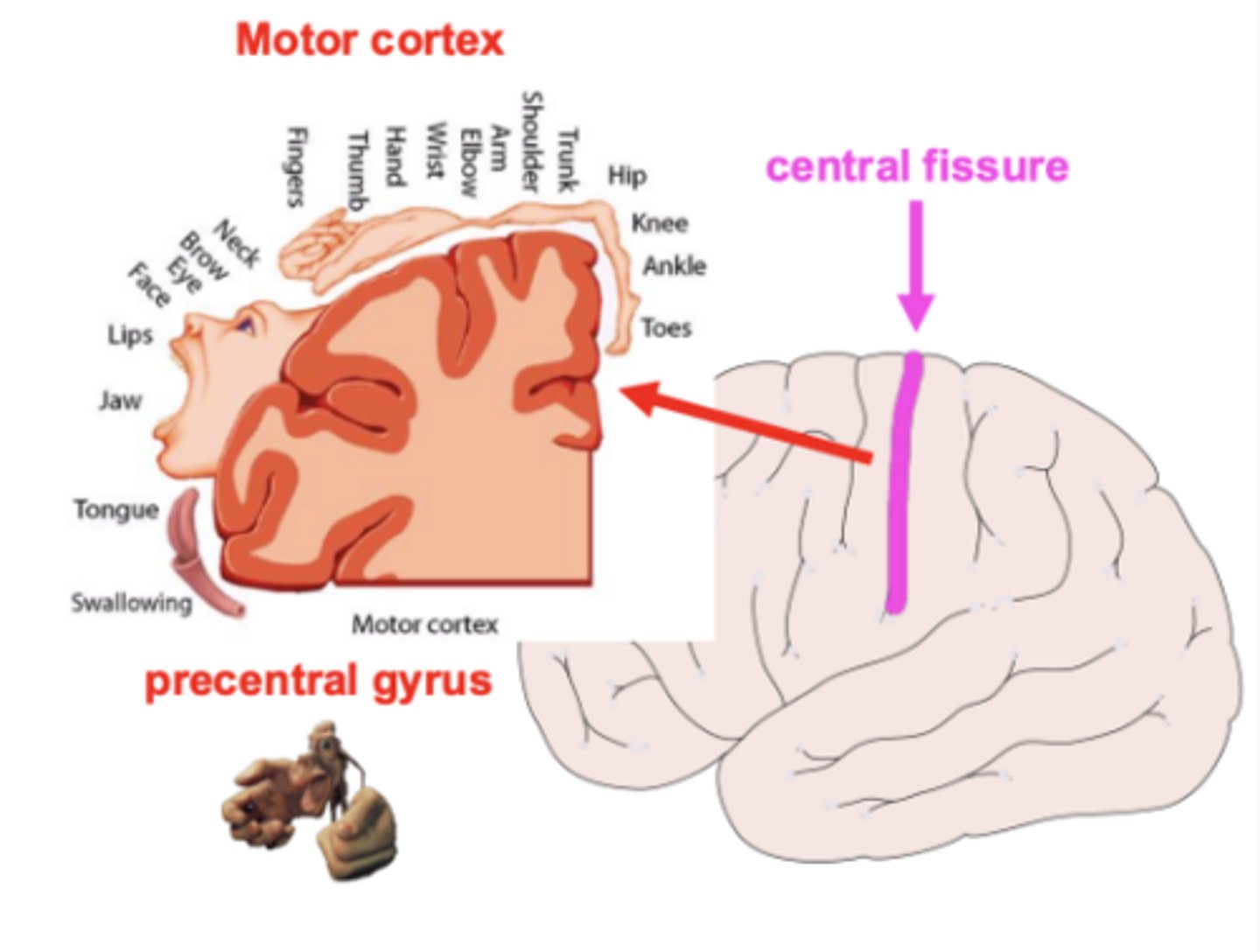
What is cortical magnification in the motor homunculus?
The size of a body part's cortical representation reflects the degree of fine motor control required — not the size of the body part itself.
Is M1 control ipsilateral or contralateral?
Contralateral — M1 controls the opposite side of the body.
What is hemiplegia?
Loss of voluntary movement on the contralateral side of the body caused by damage to the motor cortex. Pattern depends on which region of the motor homunculus is affected.
What are the shared functions of the secondary motor cortices (PMC and SMA)?
- Planning and control
- Motor plan selection (select appropriate motor plans)
- Pre-movement activity (activate BEFORE M1 and actual movement)
- Complex movement coordination
Where is the premotor cortex (PMC) located?
Frontal lobe, anterior to M1, in front of the central sulcus.
What type of movements does the PMC primarily control?
Simple movements involving one limb (single hand). External sensory-guided actions.
What triggers PMC activity?
External cues (e.g. seeing a ball) — it is sensory-driven.
What is the PMC strongly connected to?
The parietal cortex via the dorsal visual stream — processes spatial information.
What are the two subdivisions of the PMC and what does each do?
Dorsal PMC: reaching (spatial location important).
Ventral PMC: grasping (shape and orientation of object important).
What does the supplementary motor area (SMA) control?
Complex bimanual actions and learned actions. Internally generated movements (driven by internal intention, not immediate sensory input).
What is the SMA strongly connected to?
The medial frontal cortex.
Is SMA activity lateralised?
No — active bilaterally during both mental rehearsal and execution.
What is the result of SMA lesions?
Impaired performance in tasks requiring both hands.
What distinguishes the association cortex from the motor cortices?
Activity does not correlate precisely with individual motor acts, and stimulation does not produce motor output. It ensures movements are adaptive and behaviourally appropriate.
What is the posterior parietal cortex specialised for?
How specific actions are put into place; where things are in space; what objects can be used for.
What does the posterior parietal cortex do with external cues?
- Targets movements accurately to objects in space
- Processes spatial relationships
- Constructs a stable representation of space independent of eye or body position.
What does the medial frontal cortex do?
Internally generated action selection — selects appropriate actions for a behavioural context, evaluates consequences, plans according to preferences and goals.
What is the dorsal pathway?
Occipital → parietal lobe. Uses size, shape, location, and motion to guide actions (grasp/manipulate) — vision-for-action.
What are the streams of the dorsal pathway and their functions?
Dorso-dorsal stream: travels to the dorsal premotor cortex + involved in reaching
Ventro-dorsal stream: travels to the ventral premotor cortex + involved in manipulating objects and movements that signify intentions
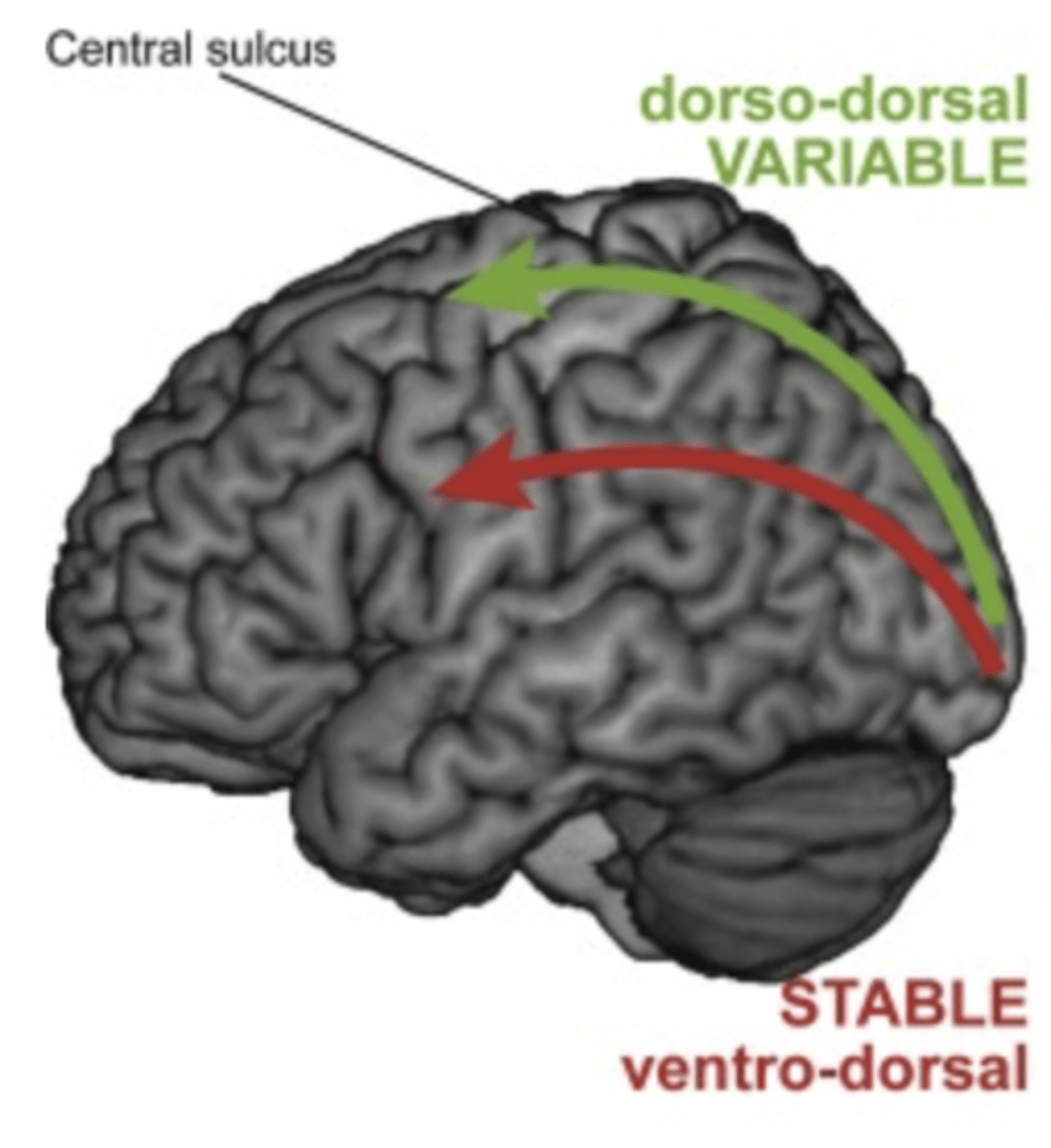
What is optic ataxia?
Damage to the dorso-dorsal stream — inability to use vision to guide reaching accurately; failure to transform visual information into appropriate motor output.
What is apraxia?
Damage to the ventro-dorsal stream — loss of skilled action, affecting motor planning.
What is the ventral pathway?
Occipital → temporal lobe. Vision-for-perception — object, face, and scene recognition.
What are the 3 muscle types in humans?
Skeletal, smooth, and cardiac (myocardium).
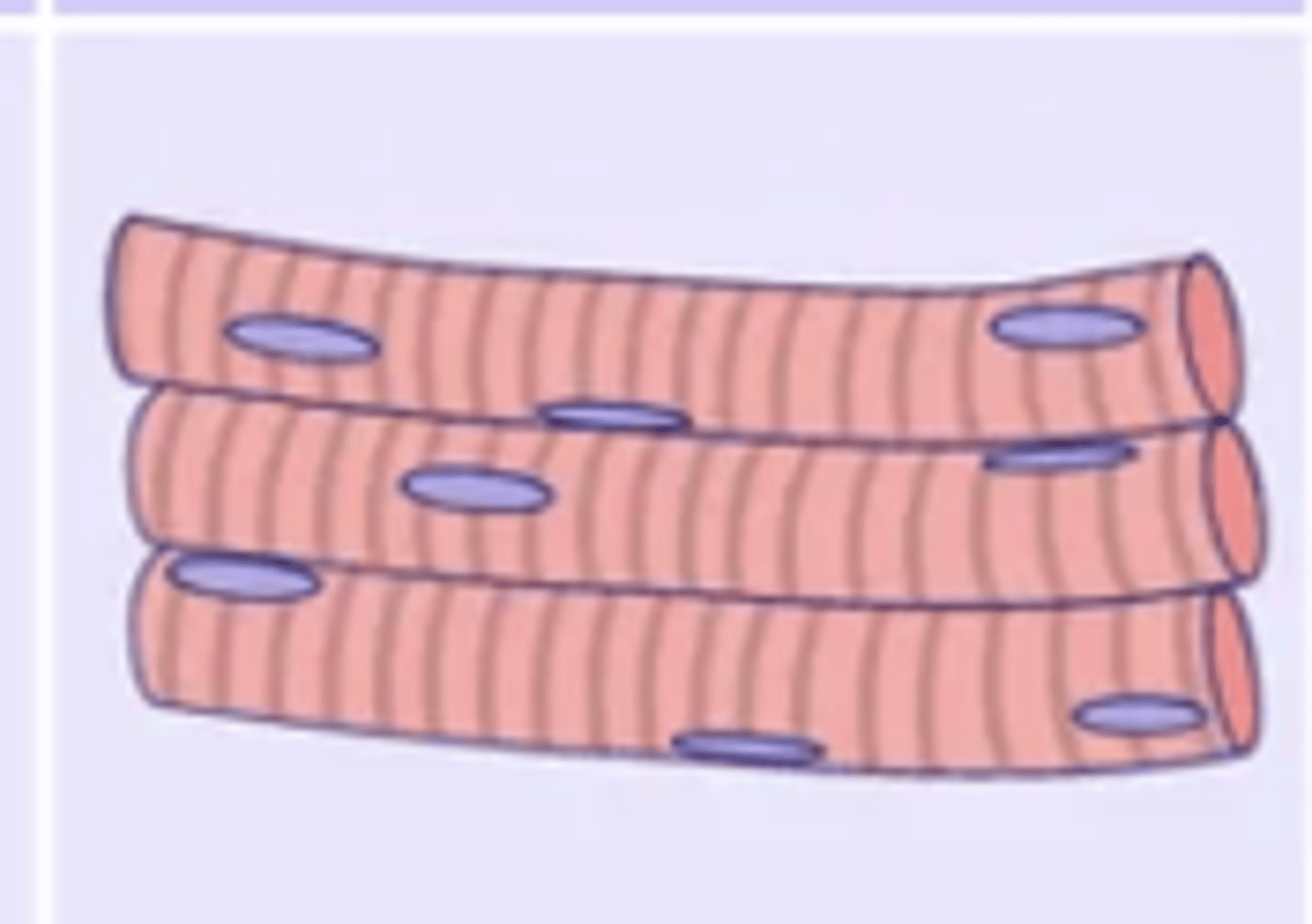
Describe skeletal muscle.
- Most common type
- Usually attached to bones via tendons (some, like facial muscles, are not)
- Controls joint movement under voluntary control
- Fibres are striated, tubular, and multi-nucleated
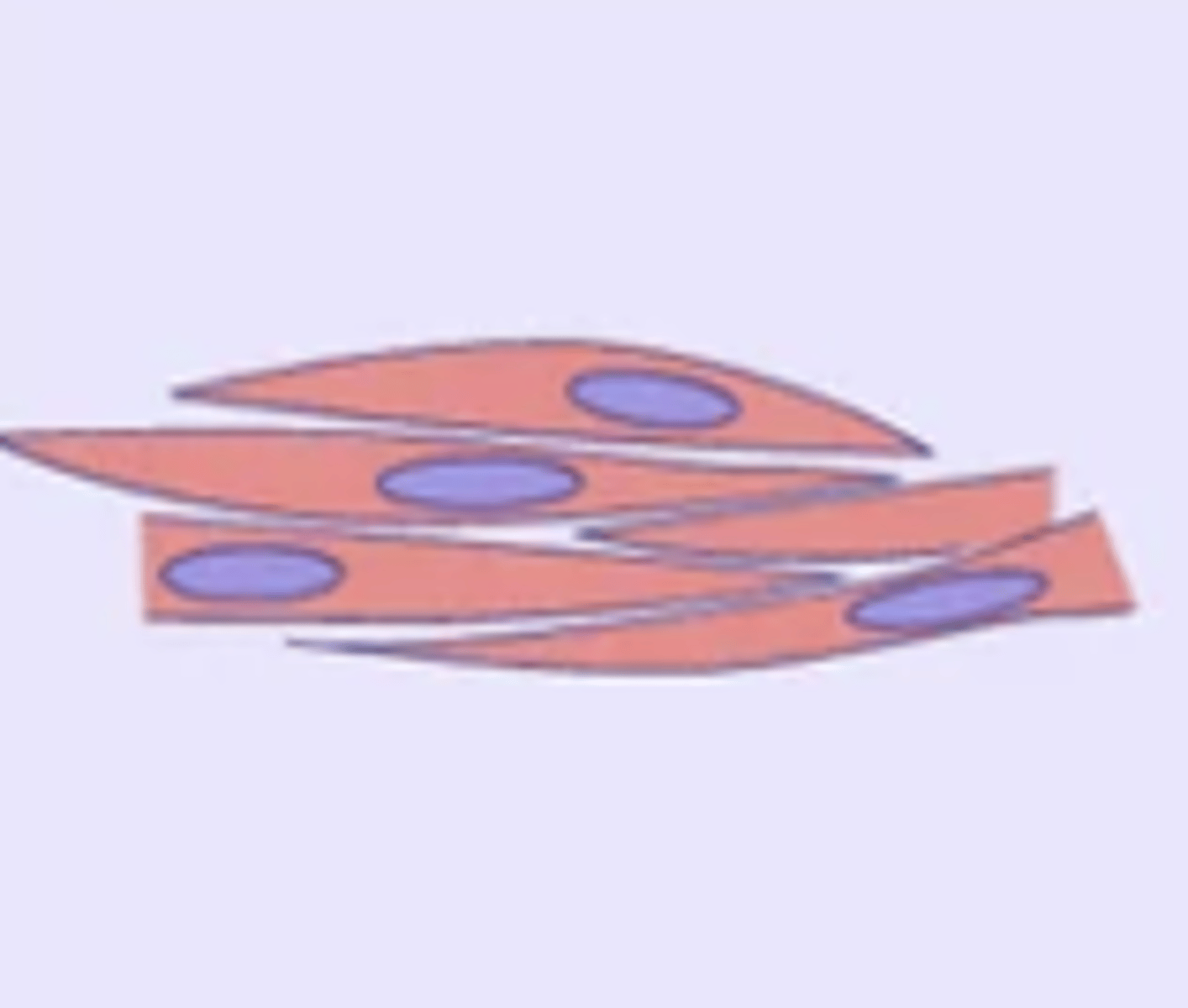
Describe smooth muscle.
- Involuntary
- Found in walls of internal organs (stomach, intestines, urinary system, blood vessels) — moves substances through them
- Fibres are non-striated, spindle-shaped, and uninucleated.
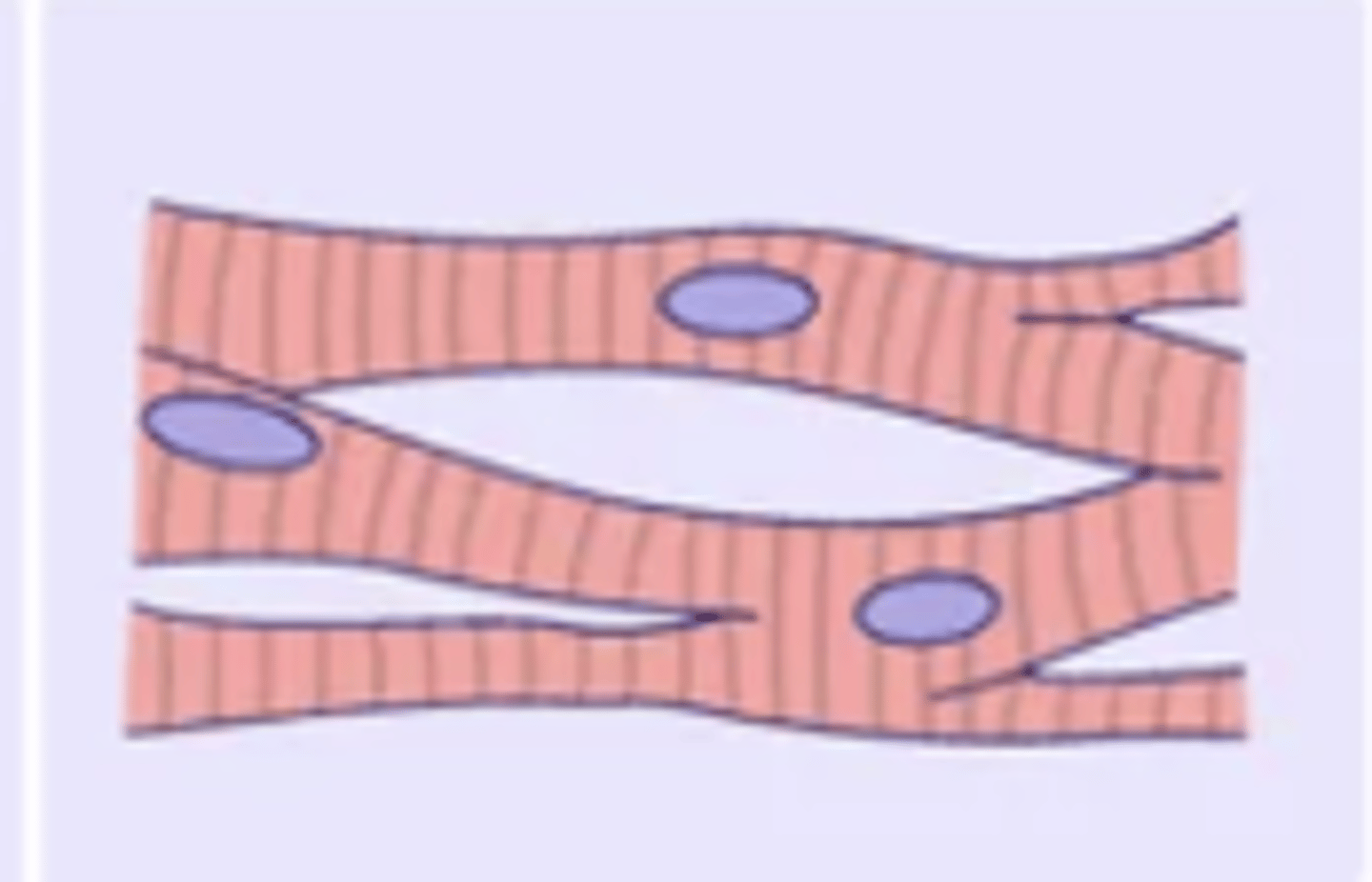
Describe cardiac muscle (myocardium).
- Found only in the heart
- Involuntary
- Fibres are striated, branched, and uninucleated
- Has myoglobin (oxygen storage) and many mitochondria (constant ATP production) → non-fatiguing.
Why is cardiac muscle non-fatiguing?
High myoglobin content for oxygen storage and many mitochondria for constant ATP production — essential for life.
What is the key structural difference between skeletal/cardiac muscle and smooth muscle?
Skeletal and cardiac muscles are striated (have sarcomeres). Smooth muscle has no striations or sarcomeres.
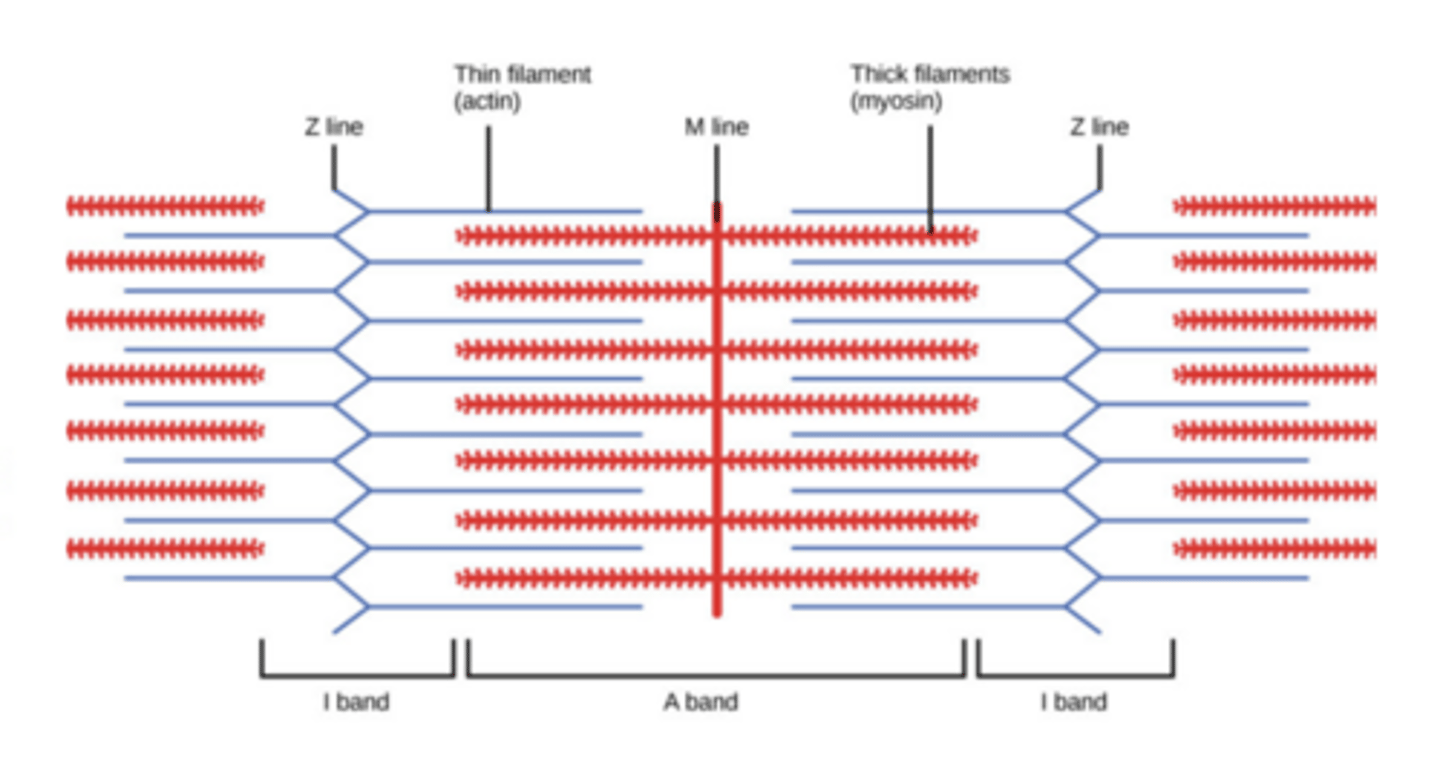
What are sarcomeres?
Bundles of overlapping actin and myosin filaments tethered at the M line so they can slide over each other → produces muscle contraction.
What are the 6 major types of skeletal muscle movement?
Flexion (decreases joint angle)
Extension (increases joint angle),
Abduction (away from midline)
Adduction (towards midline),
Medial rotation (towards midline)
Lateral rotation (away from midline).
What two coordinate systems can the brain use to represent movement?
Cartesian/allocentric (world-centred) and egocentric (body-centred). Motor control primarily uses egocentric coordinates.
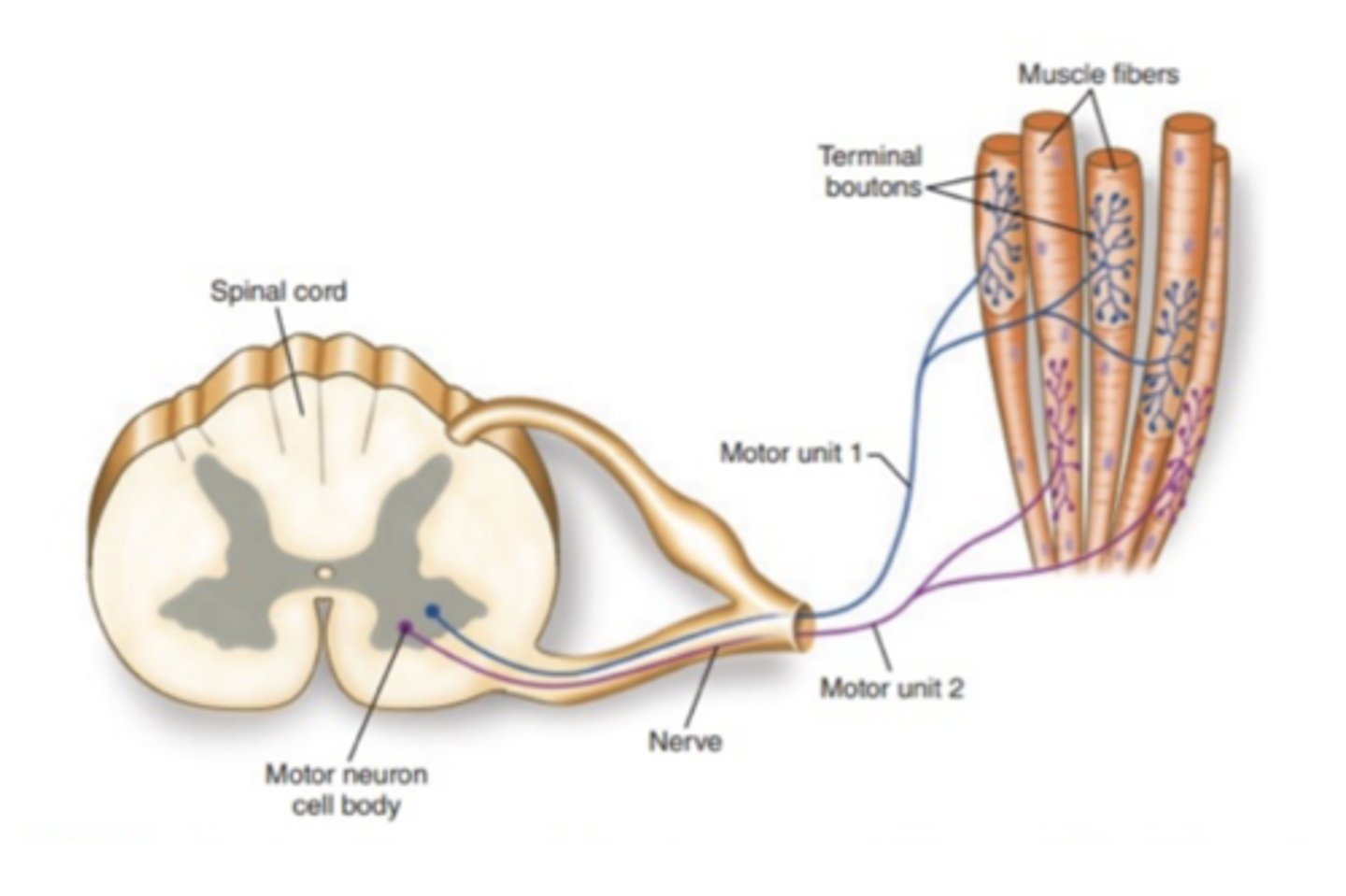
What is a motor unit?
One α-motor neuron + all the muscle fibres it innervates. α-motor neurons are lower motor neurons.
How does motor unit size relate to force and precision?
Small motor neuron → few fibres → small force, high precision. Large motor neuron → many fibres → large force, low precision.
What is the neuromuscular junction?
The synapse between the α-motor neuron terminal and the muscle fibre.
Describe the sequence of events at the neuromuscular junction.
AP arrives → Acetylcholine (ACh) released → sodium channels open → AP in sarcolemma (the membrane around the fibre) → AP travels T-tubules → calcium released from sarcoplasmic reticulum → muscle contraction.
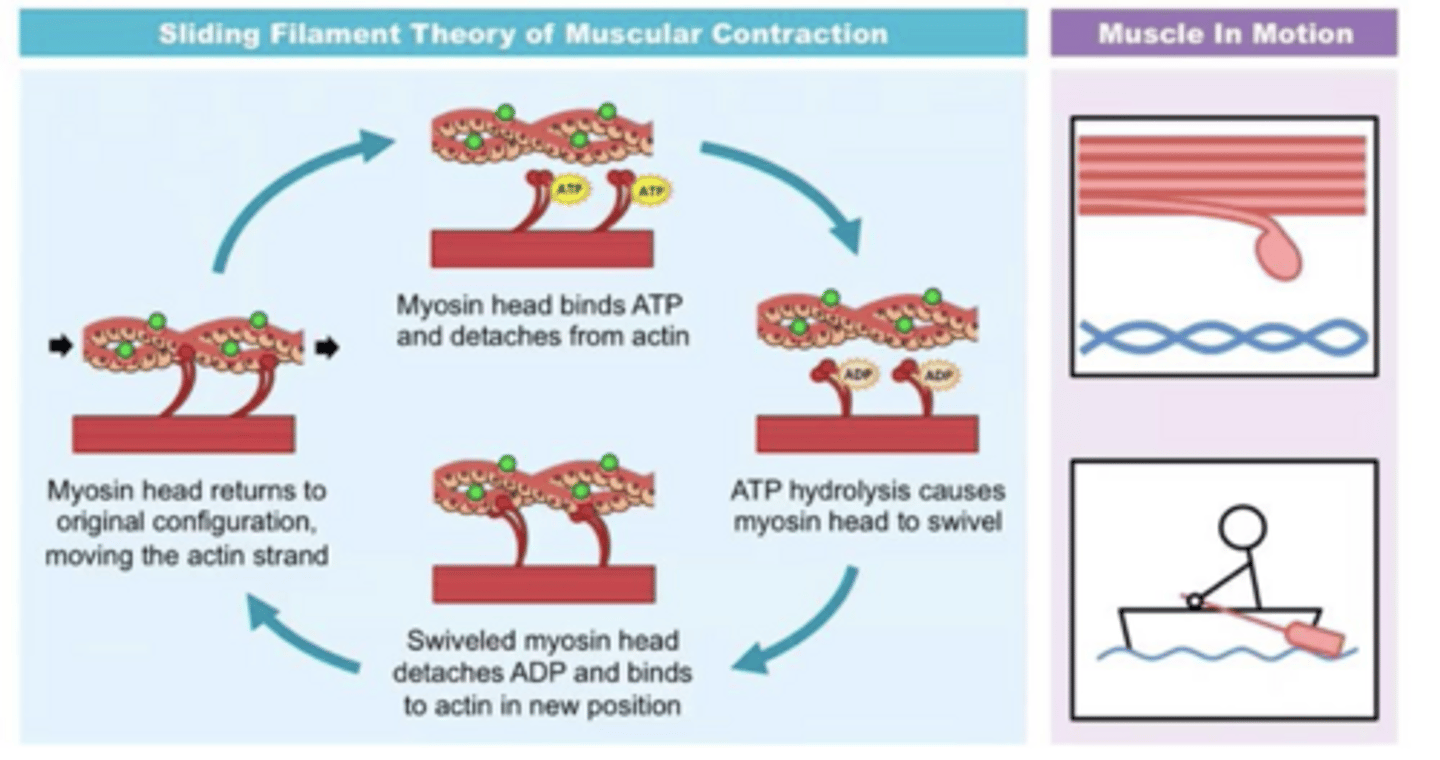
What is the sliding filament theory?
Muscle contraction occurs when calcium allows myosin heads to bind to actin, and ATP-driven cross-bridge cycling pulls actin filaments toward the centre of the sarcomere, shortening the muscle without changing filament length.
What is the sliding filament theory steps?
Step 1 — Signal arrives Action potential at the neuromuscular junction → ACh released → sarcolemma depolarises → AP travels down T-tubules → voltage-gated calcium channels (VGCCs) open → Ca²⁺ released from sarcoplasmic reticulum
Step 2 — Binding sites exposed Ca²⁺ binds to troponin → troponin changes shape → tropomyosin moves away → myosin-binding sites on actin exposed
Step 3 — Cross-bridge forms Myosin heads (already in high-energy position, bound to ADP + Pi from previous ATP hydrolysis) bind to exposed actin sites → cross-bridge formed
Step 4 — Power stroke Myosin head bends → ADP + Pi released → actin pulled toward centre of sarcomere → sarcomere shortens
Step 5 — Cross-bridge breaks ATP binds to myosin head → myosin detaches from actin → cross-bridge breaks
Step 6 — Reset ATP hydrolysed to ADP + Pi → energy used to reset myosin head back to high-energy position → ready to bind again
What keeps the sliding filament cycle going?
As long as calcium and ATP are both present, the cross-bridge cycle repeats.
What are the 3 types of muscle fibres?
Type 1 (SO) — slow, oxidative, fatigue-resistant.
Type 2A (FO) — fast, oxidative, intermediate.
Type 2B (FG) — fast, glycolytic, fatigable (most force, shortest duration).
What are the 3 types of motor units?
Slow (S), Fast Fatigue-Resistant (FR), Fast Fatigable (FF).
Describe Slow (S) motor units.
Contract slowly; generate small forces; innervate small "red" muscle fibres; fatigue-resistant (rich myoglobin, plentiful mitochondria, rich capillary beds). Important for sustained contraction e.g. posture.
Describe Fast Fatigable (FF) motor units.
Large α-motor neurons; innervate large pale muscle fibres; generate the most force; easily fatigued (sparse mitochondria). Important for brief, large force exertions e.g. running and jumping.
Describe Fast Fatigue-Resistant (FR) motor units.
Intermediate size; not as fast as FF but more fatigue-resistant; generate about twice the force of slow motor units.
What is the order of motor unit recruitment?
Small to large: Slow → FR → FF units.
What are the 3 ways force output can be increased?
1. Recruiting more motor units
2. Increasing firing rate
3. Synchronising firing (rare — causes simultaneous fatigue).
Why is synchronised firing normally avoided?
If all units fire together, they all fatigue simultaneously, creating a period of total inability to fire. Good for one maximal contraction but not for the system overall.
What is maximum voluntary contraction?
The greatest force produced voluntarily — does not reflect the absolute maximum capacity of the muscle.
What is proprioception?
The sense of knowing where your limbs are in space and how much force muscles are producing — from sensory receptors inside muscles.
What are the 2 main proprioceptive receptors in muscle?
Muscle spindles and Golgi tendon organs (GTOs).
What does the muscle spindle detect?
Muscle length (primarily) and speed of stretch. Has both sensory and motor components.
How does the muscle spindle convey information to the CNS?
Via afferent nerve fibres — transmits changes in the rate of action potentials.
What are the afferent sensory fibres?
Primary Type Ia Sensory Fibers and Secondary Type II Sensory Fibers
What do Type Ia (primary) sensory fibres detect?
Rate of change of muscle length and velocity (dynamic stretch).
What do Type II (secondary) sensory fibres detect?
Absolute muscle length (static/ongoing length).
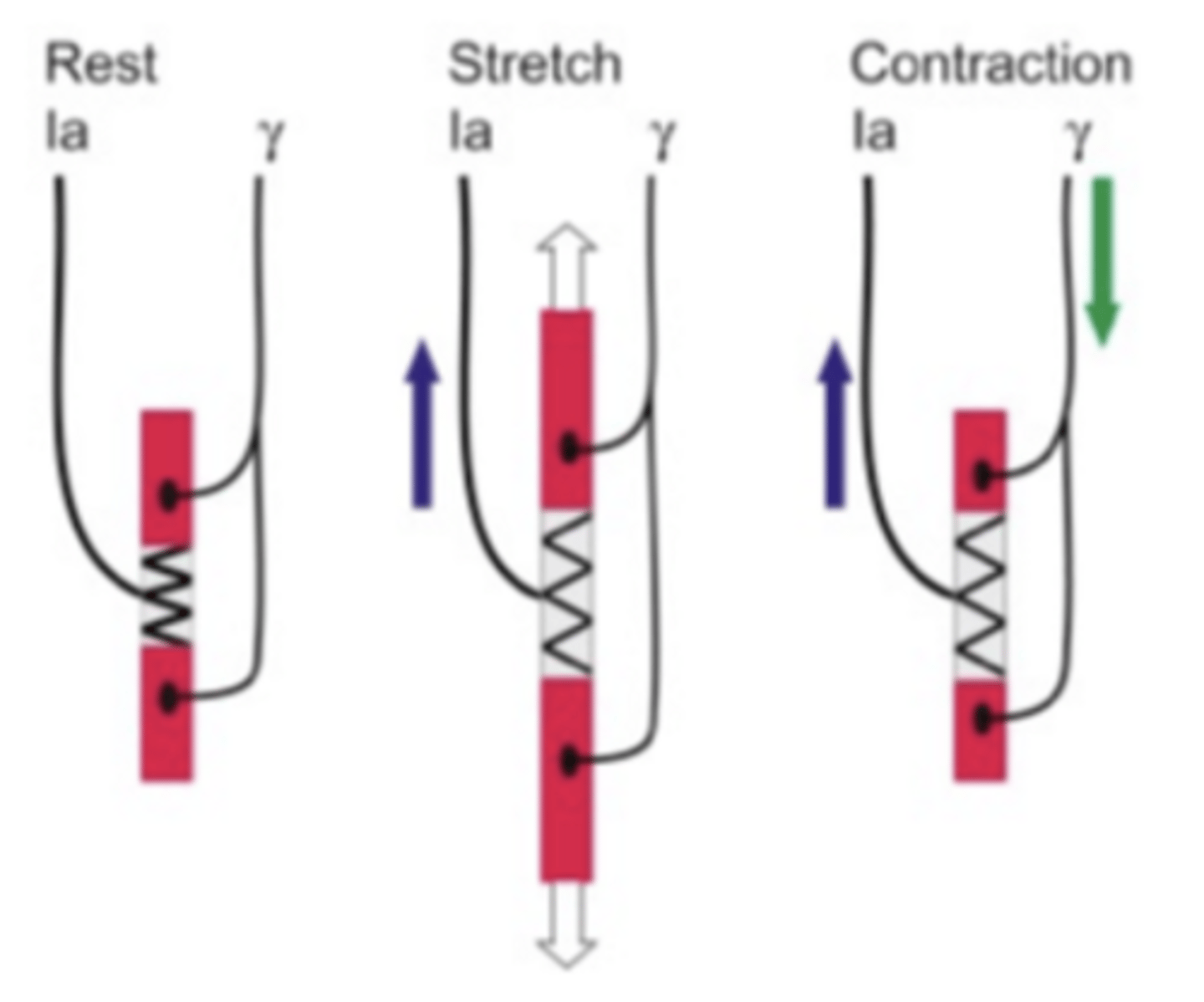
What are gamma motor neurons?
Efferent neurons that innervate intrafusal muscle fibres (myofibrils) within the muscle spindle. They keep the spindle taut (streched), allowing continued alpha motor neuron firing, and adjust spindle sensitivity.
What is the state of muscle spindle discharge at rest vs. during stretch vs. during contraction?
Rest → little discharge.
Stretch → Ia firing increases.
Contraction → gamma activation maintains tension (prevents silence).
What does the system need to track for accurate proprioception?
allows continuous limb position tracking and prevents sensory silence during contraction
muscle length + the level of gamma activation.
What is the Golgi tendon organ (GTO)?
A receptor that lies in series with extrafusal muscle fibres. Detects muscle force/tension. Receives no motor innervation.
How does the GTO prevent excessive force?
It sends force info to the spinal cord. If force exceeds the set point specified by the brain, GTO inputs via inhibitory interneurons suppress α-motor neurons → reduces force. Acts as a safety brake (reflex inhibition).
What do muscle spindles and GTOs regulate together?
Muscle tone, force & protect against damage (spindles: length + velocity; GTOs: force)
What is the stretch reflex?
The automatic response to muscle being stretched. Processed entirely in the spinal cord (one of the fastest reflexes). Muscle spindle detects stretch → stimulation of Ia afferents → activates α-motor neurons → muscle contracts.