Pain
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
What is pain?
an unpleasant sensory or emotional experience associated with actual or perceived tissue damage
What is congenital insensitivity to pain and why is it dangerous?
condition where cannot feel pain though sensation of touch usually normal
continue to do things that causes injury which could cause infections etc
What does congenital insensitivity to pain teach us about pain?
pain is a learned response
pain and touch are different
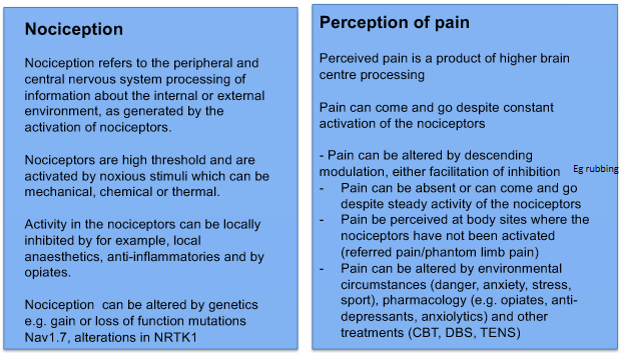
What are nociceptors?
sensory receptors that respond to dangerously intense stimuli
What are the 3 main types of nociceptors?
A delta mechanosesnsitive nociceptors
A delta mechanothermal nociceptors
C fibre polymodal receptors
What are 2 features of nociceptors?
high thresholds of stimulation
large receptive fields making fine localisation difficult
What is perception of pain from A delta fibres like?
sharp, brief, better localised
What is perception of pain from C fibres like?
duller, poorly localised, longer lasting with burning quality
Can you separate the 2 fibres to look at them indiividually?
yes - selectively blocked pharmacologically and so stimulated separately
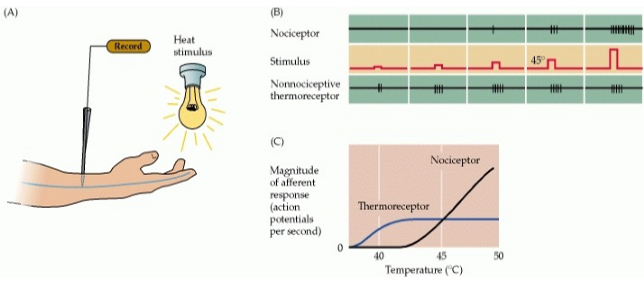
What experiement shows separate activation of specialised nociceptors and thermoreceptor rather than a greater discharge from neurons responding to normal stimuli?
Smith and Lewin 2009
place hand under lamp and increase temp gradually
thermoreceptor activity gradually increasaes then plateaus
nociceptor only active once temp becomes noxious
at this point thermoreceptors are already at max rate
indicates that nociception is not overstimulation of receptor but just different neurons responding differently
Who did this experiment?
Smith and Lewin 2009
What are the 3 ascending pathways within pain?
spinothalamic tract
important in localisation of painful or thermal stimuli
spinoreticular
motivational/affective aspects of pain
level of attention
spinomesencephalic
important in activating descending modulation (PAG)
orientation towards stimulus
escape behaviours and aversive memory
Apart from the skin where can nociceptors also be found?
in the internal organs though alarm signals less easy to pinpoint resulting in pain being perceived in wrong body location
What does the ‘convergence projection theory’ of referred pain suggest?
Ruch, 1949
What is brown sequared hemiplegia?
condition which causes loss of motor function and numbness to touch on same side as injury but loss of pain sensation on opposite side
What causes brown squared hemiplegia?
lateral hemisection of spinal cord eg injury or tumour
What does brown squared hemiplegia show?
sensations of touch and pain are carried by different anatomical routes
What is hyperalgesia?
increased sensitivity to pain from a stimulus that normally causes pain
Why might hyperalgesia happen?
following injury polymodal C fibres do not adapt to stimuli so become sensitised to pain and normal touch (allodynia)
Better:
C fibres do not adapt to stimuli they can become sensitised to pain by mediators released by injured tissue that can diffusse to non-injured areas and activate nociceptors
What is allodynia?
pain caused by a stimulus that does not normally provoke pain
What does hyperalgesia involve?
sensitisation of peripheral nociceptive nerve terminals
central facilitation of transmission at the level of the dorsal horn and thalamus
neuroplasticity - ‘wind up’
What is central sensitisation or wind up phenomenon?
spinal neurons subject to repeat or high-intensity nociceptive impulses
become progressively and increasingly excitable sometimes even after stimulus removed
alteration of strength in circuitry
What can central sensitisation lead to?
non responsive or chronic pain
facilitates pain transmission particularly in extended pain states
What is the biological mechanisms behind wind up?
occurs in dorsal horn and thalamus
repetitive stimulation, C fibres fire repetitively
leads to substance P release which acts on NK1 receptors
causes slow depolarisation
NMDA receptors on postsynaptic neurones only open is glutamate binds and depolarisation occurs tomove Mg block
opening NMDA causes influx of Ca
activates calmodulin kinase and protein kinase C
makes/inserts new AMPA receptors
increases sensitivty to glutamate
hyperexcitability of nociceptive neurones after severe or persistent injury
What is an NMDA antagonist that can reduce wind upin animals but not translated well into human drugs?
ketamine
What are pain medications for inflammatory pain? (3)
NSAIDS eg aspirin
COX 1 and 2 inhibitors, reduce prostglandin synthesis
local anaesthetics eg lidocaine
block voltage gated Na+ channels
opiates eg morphine
cause hyperpolarisation through binding to u receptors and subsequent opening of K+ channels/closure of Ca++ channels
Couple examples of alternative pain medications and therapies for longer lasting pain?
acupuncture
CBT
deep brain stimulation
How does acupuncture work?
look at particular nodes with highest conc of adenosine receptors
adenosine release and binds to A1R
causes analgesia = pain relief
Two example of experiemnts testing pain relief from acupuncture?
acupuncture with A1R agonist = no analgesia
acupuncture and adenosine degradation inhibitors = prolonged analgesia
What is transcutaneous electrical nerve stimulation?
delivery of a mild electric current through patches to skin
creates electrical impulses in A beta fibres that are believed to reduce sensation of pain
How might TENS reduce pain?
production of natural endorphins?
gating of pain transduction?
How does the gate theory of pain work?
Melzack and Wall (1965)
A beta fibre stimulates an inhibitory interneuron that causes IPSP on to the pain projection neuron and reduces firing
why rubbing may make better
no anatomical evidence but may be to do with different speeds of nerve fibres
Who argued slightly differently for gate theory of pain (lots of controversy)?
Inui et al, 2006
suggested this is all by cortical mechanism with minimal spinal involvement
Why may the perception of pain be different in different circumstances?
different environmental circumstances affect pain perception
eg soldier with battle wound
reward system from being able to continue may overcome pain
why pain of same injury may feel different in training vs competition
may be descending modulation from the PAG
What is likely to be the main control of pain?
natural opioids???
What are opioids doing - descending modulation? (2)
modulating the PAG
conditioned to not be affected as much by pain
blocking periphery sensation and also at dorsal horn
What are the mechanisms behing allodynia?
remodelling of the spinal cord circuitry at the first synapse (perhaps descending modulation and gate control theory)
What is deep brain stimulation used for and how does it work?
treat chronic nerve pain
targets PAG, thalamus, cingulate cortex
electrodes implanted into brain which send electrical current
Who did a systematic review of 22 articles for DBS?
Frizon et al (2020)
228 patients with varying diagnoses and DBS placement (PAG one of most common)
outcomes heterogeneous
promising but work to do
mayeb try include more placebo and look at differences for different diagnoses
What is the nocebo effect?
predictions about how painful a stimulus is likely to be exerts a dominant effect on what we perceive
descending facilitation of pain through the periaqueductal grey rather than the inhibition
Investigation with nocebo effect?
Yoshida et al (2013)
participants were shown a group of pain ratings from a thermal stimulus by other people before they were then exposed to that stimulus
the pain rating of each participant was recorded beforehand to make sure that individual differences in pain tolerance does not affect ratings produced
found that the group pain ratings correlated with the subjective pain ratings given by the participants afterwards
when the group ratings showed high variability there was also an increase in pain ratings from the participants which implies that uncertainty of what will be received can increase sensitivity and perception of the stimulus
if pain was simply overstimulation of the touch receptors, then it could be assumed that uncertainty would play no role in how pain is received as pain would instead correlate with just the intensity of the stimulus
Examples of circumstances which may close the gate to pain?
mechanosensitive stimulation
emotional support
distraction
acupuncture
placebo
Example of circumstaces which open the gate to pain?
depression and anxiety
learned safety signals
uncertainty
What is phantom limb pain?
occurs when nerves that would normally innervate the missing limb are abnormally stimulated and cause the perception of pain (limb twisted, contracted etc)
Potential reasons for phantom limb pain? (70% experience)
damage to nociceptor endings
cortical reorganisation (Schone 2025 argues not this)
feeling of pain without touch suggests pain could be caused by separate receptors and more controlled by brain and higher processing
What therapy is there for phantom limb pain?
mirror box therapy
tricks brain and alleviates pain
aware what’s happening but still works
Difference between nociception and perception of pain summary?
What 2 things show interactions between pain and touch pathway?
gate theory
allodynia
What 2 things demonstrate the independent use of two different systems (dorsal vs anterolateral)?
Brown Sequard syndrome
congenital insensitivity to pain
Is pain simply overstimulation of the touch receptors essay plan?
different neurons respond differently
lamp experiment
injury and unique situations
Brown sequard hemiplegia
CIP - Stefan Betz
outlined by Cox (2017) he could put hand in boiling water but would shudder at a cold wind
phantom limb pain
pain is subjective
nocebo effect