TRA NP2 ( MATERNAL)
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
96 Terms
The nurse explains that the "master gland" in the brain sends signals to the ovaries to kickstart the cycle. Which statement by the client indicates an accurate understanding of the source of Follicle-Stimulating Hormone (FSH) and Luteinizing Hormone (LH)?
A. Adrenal glands
B. Corpus luteum
C. Anterior pituitary gland
D. Milk production
Answer: C
Rationale: FSH and LH are secreted by the anterior pituitary to regulate ovarian function.
The nurse describes the first 14 days of the cycle. Which hormone is primarily responsible for "recruiting" a follicle and enhancing the ovarian production of estrogen during this first half?
A. LH
B. hCG
C. FSH
D. GH
Answer: C
The client asks when her estrogen levels will be at their highest. The nurse correctly identifies that the serum estrogen level peaks on which day of a typical 28-day cycle?
a. Day 4
b. Day 10
c. Day 13
d. Day 14
Answer: C
Rationale: Estrogen peaks just before ovulation (~day 12–13).
Once the egg is released, the body needs a hormone to maintain the "nest" (uterine lining) by stimulating progesterone production. Which anterior pituitary hormone is responsible for this during the latter half of the cycle?
a. FSH
b. LH
c. HCG
d. 14th day
Answer: B
Rationale: LH maintains the corpus luteum, which produces progesterone.
the nurse asks the client if she knows what structure in the ovary actually produces the progesterone during the latter (luteal) half of the cycle. The client correctly identifies it as the:
a. Corpus Luteum
b. Anterior Pituitary Gland
c. Posterior Pituitary Gland
d. Ovarian Follicle
Answer: A
Rationale: The corpus luteum secretes progesterone after ovulation.
Goodell’s sign refers to:
A. Softening of the cervix
B. Uterine souffle sound
C. Presence of hCG in urine
D. Fetal movement
Answer: A
Rationale: Goodell’s sign = cervical softening due to increased vascularity.
Maria tells the nurse she is currently pregnant with twins. She has a 5-year-old child at home who was born at 37 weeks. She has no history of miscarriages or abortions. The nurse correctly documents her GTPAL as:
A. G = 3, T = 2, P = 0, A = 0, L =1
B. G = 2, T = 0, P = 1, A = 0, L =1
C. G = 1, T = 1. P = 1, A = 0, L =1
D. G = 2, T = 0, P = 0, A = 0, L =1
Answer: B. G = 2, T = 0, P = 1, A = 0, L =1
Rationale:
G (Gravida) = total pregnancies
Current pregnancy (twins) = 1 pregnancy
Previous pregnancy (5-year-old child) = 1 pregnancy
👉 G = 2
T (Term births ≥37 weeks)
5-year-old born at 37 weeks
P (Preterm births 20–36 6/7 weeks)
Maria asks the nurse about the “fluttering” sensations she feels in her abdomen. The nurse correctly identifies this process as Quickening, which is:
A. “It is the irregular, painless contractions that occur throughout pregnancy.”
B. “It is the soft blowing sound that can be heard when the uterus is auscultated.”
C. “It is the fetal movement that is felt by the mother.”
D. “It is the thinning of the lower uterine segment.”
Answer: C
Rationale:
Quickening refers to the first perception of fetal movement by the mother, usually felt at 16–20 weeks in multiparous women.
The nurse assesses the fetal heart rate (FHR) of the twins. Which of the following FHR readings would the nurse document as normal for a fetus at 38 weeks?
A. 100 BPM
B. 80 BPM
C. 150 BPM
D. 170 BPM
Answer: C
Rationale: Normal fetal heart rate range = 110–160 bpm.
150 bpm falls within normal range.
During a vaginal examination, the nurse feels the fetal presenting part and determines it is 2 cm below the level of the ischial spines. The nurse properly documents this as:
A. Station 0
B. Station -2
C. Station +2
D. Station +- 2
Answer: C
Rationale:
Above ischial spines = negative
At spines = 0
Below spines = positive
👉 2 cm below = +2 station
Maria is currently in the first stage of labor. The nurse notes that her cervix has progressed from 4 cm to 7 cm. In which phase of the first stage does this rapid dilation occur?
A. Preparatory phase
B. Latent phase
C. Active phase
D. Transition phase
Answer: C. Active phase
Rationale:
The active phase of the first stage of labor is characterized by rapid cervical dilation, typically from 4 cm to 7 cm (or up to 8 cm in some references). Contractions become stronger, longer, and more frequent, causing faster cervical changes.
The latent phase is the early part of the first stage of labor. Cervical dilation progresses slowly from 0 to about 3–4 cm. Contractions are usually mild to moderate and less frequent.
The transition phase is the final phase of the first stage of labor, where cervical dilation progresses from 8 cm to 10 cm.
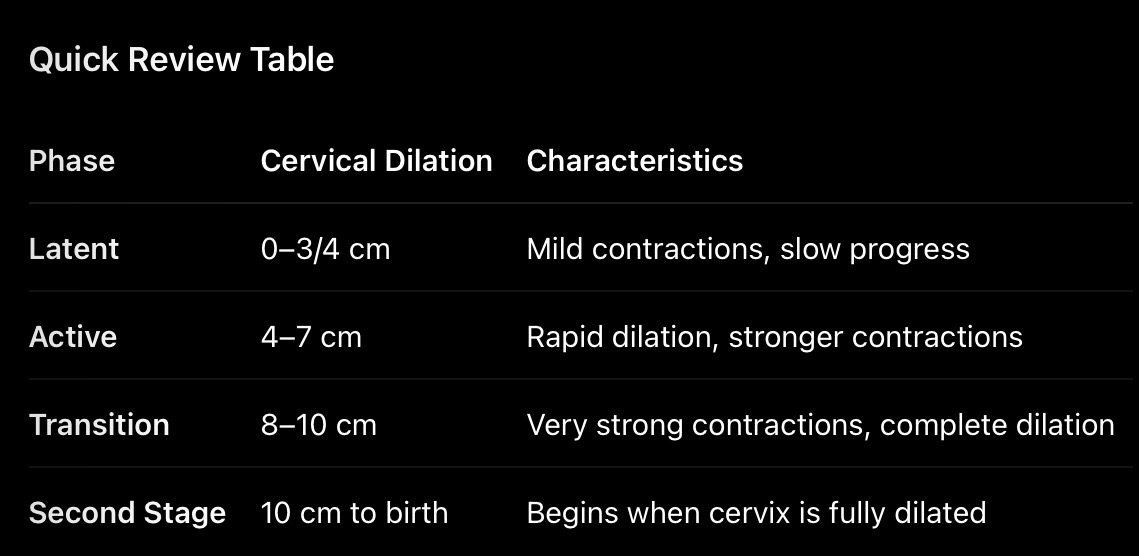
As the nurse continues to monitor Maria, she looks for signs that the first stage of labor has ended. The nurse determines that Maria is beginning the 2nd stage of labor when which of the following is noted?
A. The client begins to expel clear vaginal fluid
B. The contractions are regular
C. The membranes have ruptured
D. The cervix is dilated completely
Answer: D. The cervix is dilated completely
Rationale:
Stage | Begins | Ends |
1st Stage | Onset of true labor | Complete cervical dilation (10 cm) |
2nd Stage | Complete dilation | Birth of baby |
3rd Stage | Birth of baby | Delivery of placenta |
4th Stage | Placenta delivered | First 1 to 4 hours postpartum |
Earlier, when Maria was only 2 cm dilated, the nurse observed her behavior to help determine her labor phase. Which findings are characteristic of the latent phase of labor?
A. The client is helpless and restless
B. The client feels out of control
C. The client is talkative and eager
D. The client is tired and anxious
Answer: C. The client is talkative and eager
Rationale:
The latent phase is the early part of the first stage of labor (approximately 0–3 cm dilation, though some references say up to 4 cm). Contractions are usually mild to moderate, and many women are excited about the impending birth. They are often talkative, cheerful, eager, and able to cope well with contractions.
Latent (0-3/4 cm) | Talkative, excited, eager, cooperative |
Active (4-7 cm) | More serious, focused on contractions |
Transition (8-10 cm) | Restless, irritable, anxious, feels out of control |
Before admission, Maria wasn’t sure if she was in “real” labor. Which of the following assessment findings would have indicated to the nurse that Maria was experiencing false labor?
A. Contractions decrease in duration and intensity
B. Back pain not relieved by walking
C. Dilatation and effacement of the cervix are noted
D. Bloody show occurs
Answer: A. Contractions decrease in duration and intensity
Rationale:
False labor (Braxton Hicks contractions) is characterized by contractions that are irregular and often decrease in frequency, duration, and intensity with rest, hydration, or changes in position.
❌B. Back pain not relieved by walking
Rationale: Persistent back pain that is not relieved by walking is more suggestive of true labor.
❌C. Dilatation and effacement of the cervix are noted
Rationale: Cervical dilation and effacement occur only in true labor.
❌D. Bloody show occurs
Rationale: Bloody show is caused by the release of the mucus plug as the cervix begins to dilate and is a sign of true labor.
Characteristic | True Labor | False Labor (Braxton Hicks) |
Contraction Pattern | Regular intervals; become closer together over time | Irregular intervals; do not become closer together |
Contraction Intensity | Gradually increase in strength and intensity | Usually weak and do not increase in intensity |
Contraction Duration | Become longer and stronger | Remain short or may decrease |
Effect of Walking/Activity | Contractions continue or become stronger with walking | Contractions lessen or disappear with walking, rest, or position change |
Location of Pain | Usually starts in the lower back and radiates to the abdomen | Usually felt in the abdomen or groin only |
Cervical Changes | Causes cervical dilation and effacement | No cervical dilation or effacement |
Bloody Show | Often present | Usually absent |
Membrane Rupture | May occur | Does not occur |
Response to Sedation/Hydration | Contractions persist despite sedation or hydration | Contractions often stop with sedation, hydration, or rest |
Fetal Descent | Present as labor progresses | Absent |
Outcome | Results in birth of the baby | Does not result in birth |
A nurse is preparing to care for a woman who has just delivered a healthy newborn. To ensure maternal stability during the immediate postpartum period, the nurse follows the standard protocol for taking vital signs:
A. Every 30 minutes during the first hour and then every hour for the next two hours.
B. Every 15 minutes during the first hour and then every 30 minutes for the next two hours.
C. Every hour for the first 2 hours and then every 4 hours.
D. Every 5 minutes for the first 30 minutes and then every hour for the next 4 hours.
Answer: B
PNLE Tip
For postpartum questions, remember:
“15-30-60 Rule”
Every 15 min during the first hour
Every 30 min for the next 2 hours
Then every 60 min or longer as ordered/stable
During one of the 15-minute assessments, the nurse locates the uterine fundus and notes that it feels soft and boggy rather than firm. Which nursing intervention is most appropriate initially?
A. Massage the fundus until it is firm
B. Elevate the mother’s legs
C. Push on the uterus to assist in expressing clots
D. Encourage the mother to void
Answer: A. Massage the fundus until it is firm
Rationale: A boggy uterus indicates uterine atony, the most common cause of postpartum hemorrhage. The nurse’s first action is to massage the fundus to stimulate uterine contraction and reduce bleeding.
The nurse assesses another client in the 4th stage of labor. In this case, the fundus is firm, yet the vaginal bleeding remains excessive. What is the initial nursing action?
A. Massage the fundus
B. Place the mother in the Trendelenburg’s position
C. Notify the physician
D. Record the findings
Answer: C. Notify the physician
Rationale: If the fundus is firm but bleeding remains excessive, the cause is likely laceration, hematoma, or retained placental fragments, not uterine atony. The physician should be notified immediately for further evaluation and treatment.
A client who had a forceps delivery and an epidural is now 6 hours postpartum. Her BP has dropped (systolic by 20, diastolic by 10), her pulse is 120 bpm (tachycardia), and she is anxious. A vulvar hematoma is verified. After notifying the provider, what is the nurse’s immediate plan?
A. Monitor fundal height
B. Apply perineal pressure
C. Prepare the client for surgery
D. Reassure the client
Answer: C. Prepare the client for surgery
Rationale: A large vulvar hematoma with signs of hypovolemia (decreased BP, tachycardia, anxiety) suggests ongoing bleeding. Significant hematomas often require surgical evacuation and ligation of bleeding vessels.
During the seminar, a mother asks when the bright red bleeding will change color. The nurse explains the stages of lochia and notes that Lochia Serosa (the pinkish-brown discharge) typically occurs during:
A. Days 3 and 4 PP
B. Days 4 to 9 PP
C. Days 10-14 PP
D. Days 14 to 42 PP
Correct Answer: B. Days 4 to 9 PP
Rationale: Lochia Serosa is pinkish-brown and typically occurs from postpartum days 4–9.
Type of Lochia | Color | Typical Duration |
Lochia Rubra | Bright/Dark Red | Days 1-3 |
Lochia Serosa | Pinkish-Brown | Days 4-9 |
Lochia Alba | Yellowish-White | Days 10-42 |
Following the previous timeline, the nurse asks the mothers to identify what type of discharge they should expect to find on the sixth postpartum day:
A. Lochia Rubra
B. Lochia Serosa
C. Lochia Alba
D. Absence of Lochia
Answer: B. Lochia Serosa
To ensure the mothers can monitor their own recovery at home, the nurse explains that while lochia amounts vary, the flow should be concerning if it is excessive. Normal lochia should never exceed the need for:
A. One peripad per day
B. Two peripads per day
C. Three peripads per day
D. Eight peripads per day
Answer: D. Eight peripads per day
Rationale: Normal postpartum lochia should not be so heavy that it saturates an excessive number of pads. Requiring more than 8 peripads per day may indicate abnormal bleeding or postpartum hemorrhage.
The nurse emphasizes that mothers should inspect their pads. If a mother notes the presence of clots larger than 1 cm, which of the following is the most appropriate nursing action?
A. Document the findings
B. Notify the physician
C. Reassess the client in 2 hours
D. Encourage increased intake of fluids
Answer: B. Notify the physician
Rationale: Large blood clots postpartum may indicate uterine atony, retained placental fragments, or postpartum hemorrhage. Clots larger than expected should be reported promptly for evaluation.
A mother expresses concern that she has not had a bowel movement since delivery yesterday. The nurse reassures her by stating that normal bowel elimination is expected to return:
A. On the day of the delivery
B. 2-3 days PP
C. 7 days PP
D. Within 2 weeks
Answer: B. 2-3 days PP
The clinical instructor asks a student nurse to perform the first set of vital signs on a stable newborn. To obtain the most accurate data before the infant becomes agitated by touch, the student should follow which sequence?
A. Pulse, respirations, temperature
B. Temperature, pulse, respirations
C. Respirations, temperature, pulse
D. Respirations, pulse, temperature
Answer: D. Respirations, pulse, temperature
Rationale: Respirations should be assessed first because handling or crying can alter the respiratory rate. The pulse is assessed next, followed by temperature, which requires the most handling.
The instructor asks the students to calculate an APGAR score at 1 minute of life. Which of the five signs is considered the primary and most critical observation?
A. Heart rate
B. Respiratory rate
C. Presence of meconium
D. Evaluation of the Moro reflex
Answer: A. Heart rate
A student is charting the respiratory status of a 2-hour-old infant. The instructor identifies that the student understands neonatal physiology if the student describes the respirations as:
A. Regular, abdominal, 40-50 per minute, deep
B. Irregular, abdominal, 30-60 per minute, shallow
C. Irregular, initiated by chest wall, 30-60 per minute, deep
D. Regular, initiated by the chest wall, 40-60 per minute, shallow
Answer: B. Irregular, abdominal, 30-60 per minute, shallow
Rationale: Normal newborn respirations are:
30–60 breaths/minute
Irregular
Primarily abdominal (diaphragmatic)
Relatively shallow
Upon initial physical examination, which finding confirms to the nurse that the neonate is a full-term infant?
A. Lanugo in woolly patches
B. Skin is dry and cracked
C. Fingernails extend beyond fingertips
D. Profuse scalp hair
Answer: C. Fingernails extend beyond fingertips
Rationale: A full-term infant commonly has fingernails that extend beyond the fingertips, indicating maturity.
Assessment Finding | Preterm Infant (<37 weeks) | Full-Term Infant (37–42 weeks) | Post-Term Infant (>42 weeks) |
Weight | Usually lower birth weight | Appropriate for gestational age | May be thin due to loss of subcutaneous fat |
Skin | Thin, translucent, reddish | Smooth, pink, good skin turgor | Dry, cracked, peeling, parchment-like |
Lanugo | Abundant over body | Minimal to moderate | Little to absent |
Vernix Caseosa | Abundant | Moderate amount | Scant or absent |
Hair | Fine, silky hair | Well-developed hair | Variable; may be thick |
Fingernails | Short, do not reach fingertips | Extend to or beyond fingertips | Long and may require trimming |
Plantar Creases | Few or absent | Creases over most of sole | Deep creases covering entire sole |
Ear Cartilage | Soft, folds easily, slow recoil | Firm with instant recoil | Firm and stiff |
Breast Tissue | Small or absent breast nodules | Well-developed breast nodules | Well-developed |
Muscle Tone | Poor muscle tone, limbs extended | Good flexion of extremities | Alert, active, may appear thin |
Male Genitalia | Undescended testes, smooth scrotum | Testes descended, scrotal rugae present | Testes descended with deep rugae |
Female Genitalia | Prominent clitoris and labia minora | Labia majora cover clitoris and labia minora | Labia majora fully developed |
Subcutaneous Fat | Minimal | Adequate | Decreased due to prolonged gestation |
Appearance | Small, fragile-looking | Healthy, well-rounded appearance | Thin, wasted appearance |
While cleaning the infant’s face, you notice tiny, white, pinhead-sized spots scattered across the bridge of the nose. How should you document this normal finding?
A. Milia
B. Lanugo
C. Whiteheads
D. Mongolian spots
Answer: A. Milia
B. Lanugo
Rationale: Fine body hair.
❌
C. Whiteheads
Rationale: Not the proper neonatal term.
❌
D. Mongolian spots
Rationale: Bluish-gray skin pigmentation usually found on the sacral area.
The infant is breathing comfortably without distress. You explain to the mother that this is due to “Surfactant.” What is the primary function of this substance?
A. Assists with ciliary body maturation in the upper airways
B. Helps maintain a rhythmic breathing pattern
C. Promotes clearing mucus from the respiratory tract
D. Helps the lungs remain expanded after the initiation of breathing
Answer: D. Helps the lungs remain expanded after the initiation of breathing
At two hours of age, you notice the infant’s hands and feet have a bluish tint (acrocyanosis), though his trunk is pink. What is your priority nursing action?
A. Activate the code blue or emergency system
B. Do nothing because acrocyanosis is normal in the neonate
C. Immediately take the newborn’s temperature according to hospital policy
D. Notify the physician of the need for a cardiac consult
Answer: B. Do nothing because acrocyanosis is normal in the neonate
Rationale: Acrocyanosis (bluish hands and feet with a pink trunk) is a normal finding in the first 24–48 hours of life due to immature peripheral circulation and vasomotor instability. No emergency intervention is required if central perfusion is adequate.
As you develop the plan of care to prevent the buildup of bilirubin (jaundice), which intervention is most important to include?
A. Monitoring for the passage of meconium each shift
B. Instituting phototherapy for 30 minutes every 6 hours
C. Substituting breastfeeding for formula during the 2nd day after birth
D. Supplementing breastfeeding with glucose water during the first 24 hours
A. Monitoring for the passage of meconium each shift
Rationale: Bilirubin is excreted through stool. Delayed passage of meconium increases enterohepatic circulation and worsens jaundice. Therefore, monitoring stool passage is a key preventive intervention.
Which client must be prioritized as the highest clinical emergency?
A. The client with prolapsed cord
B. The client with BP of 160/100 mmHg
C. The client with oliguria
D. The client with headache and blurred vision
A. The client with prolapsed cord
Rationale: Umbilical cord prolapse causes immediate fetal hypoxia due to cord compression. It is a true obstetric emergency requiring immediate action (positioning, relief of pressure, rapid delivery).
Based on Alora’s confirmed diagnosis of Abruptio Placentae at term, what is the priority action Nurse Leo should prepare for?
A. Conducting weekly coagulation studies until delivery.
B. Preparing the client for the delivery of the fetus.
C. Implementing strict monitoring of the client’s intake and output.
D. Prescribing complete bed rest for the rest of the pregnancy.
Answer: B. Preparing the client for the delivery of the fetus.
Rationale: Abruption placentae is the premature separation of a normally implanted placenta. At 37 weeks (term) with fetal distress and maternal bleeding, the priority is immediate delivery to save the fetus and prevent maternal complications such as hemorrhage and DIC.
PNLE
Abruptio Placentae + Fetal Distress + Term Pregnancy = Deliver the Baby
During the induction of labor with Pitocin, what is the most dangerous uterine response that Nurse Taylor must be vigilant about?
A. Intense pain.
B. Umbilical cord prolapse.
C. Uterine tetany.
D. Low blood sugar levels.
Answer: C. Uterine tetany
Rationale Pitocin (Oxytocin) stimulates uterine contractions. Excessive stimulation may lead to uterine tetany (hyperstimulation), where contractions become too frequent and prolonged.
PNLE Pearl
Pitocin Danger = Hyperstimulation (Uterine Tetany)
Signs:
Contractions lasting >90 seconds
More than 5 contractions in 10 minutes
Minimal resting period between contractions
Fetal distress
Sofia, who had a previous C-section, experienced a sudden “pop,” followed by vomiting and a brief moment of “relief” from the contraction pain before passing out. What does Nurse Taylor suspect happened?
A. A uterine rupture.
B. Dysfunctional labor.
C. Extreme anxiety combined with the flu.
D. A placental abruption.
Answer: A. A uterine rupture
Rationale
Classic signs of uterine rupture include:
Sudden tearing or popping sensation
Severe pain followed by sudden relief
Maternal hypotension
Loss of fetal station
Signs of shock
Previous cesarean section history
Nurse Saru is reviewing the potential risk factors for gestational diabetes mellitus (GDM) with a patient who is 24 weeks pregnant. Which of the following risk factors should Nurse Sam highlight during this conversation?
A. Low pre-pregnancy body weight.
B. Excessive nausea and vomiting during pregnancy.
C. History of polycystic ovary syndrome (PCOS).
D. Age under 25 years.
Answer: C. History of polycystic ovary syndrome (PCOS).
Rationale
Women with PCOS commonly have insulin resistance, which significantly increases the risk of developing gestational diabetes.
A nurse is assessing a child suspected of acetaminophen poisoning. Which initial symptoms should the nurse expect?
A. Vomiting, sweating, pallor
B. Hyperactivity, dilated pupils, tremors
C. Seizures, hallucinations, tachycardia
D. Bradycardia, hypothermia, hypotension
Answer: A. Vomiting, sweating, pallor
Which drug is used as an antidote for acetaminophen poisoning?
A. Vitamin K
B. Acetylsalicylic Acid (ASA)
C. Acetylcysteine
D. Ethylenediaminetetraacetic acid (EDTA)
Answer: C. Acetylcysteine
The nurse reviews the laboratory results for a child with a suspected diagnosis of rheumatic fever, knowing that which laboratory study would assist in confirming the diagnosis?
A. Immunoglobulin
B. Red blood cell count
C. White blood cell count
D. Anti–streptolysin O titer
Correct Answer: D. Anti–streptolysin O (ASO) titer
Rationale: Rheumatic fever is a delayed inflammatory complication that occurs after infection with Group A β-hemolytic Streptococcus (such as streptococcal pharyngitis).
The nurse is collecting data on a child with a diagnosis of rheumatic fever. Which question should the nurse initially ask the mother of the child?
A. “Has the child been vomiting?”
B. “Has the child had any diarrhea?”
C. “Does the child complain of chest pain and numbness in the right arm?”
D. “Has the child complained of a sore throat within the past few months?”
Answer: D. “Has the child complained of a sore throat within the past few months?”
RationaleRheumatic fever is a delayed autoimmune response that typically develops 2–6 weeks after an untreated Group A β-hemolytic streptococcal throat infection (strep throat).
Which of the following is the most appropriate activity for a 5-year-old child?
A. Squeeze toy
B. Board games
C. Play-Doh
D. Computer games
Answer: C. Play-Doh
The nurse is observing children playing in the hospital playroom. He would expect to see 5-year-old children playing:
A. Building a tower out of blocks
B. With their own toys alongside other children
C. Alone with handheld computer games
D. Cooperatively with other preschoolers
Answer: D. Cooperatively with other preschoolers
Rationale:
A 5-year-old child is in the preschool stage and typically engages in cooperative play, where children interact, share, follow rules, and work together toward a common activity or goal.
Erikson’s stage of psychosocial development in which social relationships develop and productivity increases.
A. Initiative vs Guilt
B. Autonomy vs Shame and Doubt
C. Industry vs Inferiority
D. Generativity vs Stagnation
Answer: C. Industry vs Inferiority
Erikson's Stage | Age Group | Meaning |
|---|
A. Initiative vs Guilt | 3–6 years (Preschool) | Children begin to initiate activities, explore, and use imagination. Success develops initiative; excessive criticism leads to guilt. |
B. Autonomy vs Shame and Doubt | 1–3 years (Toddler) | Children strive for independence in activities such as feeding, dressing, and toileting. Success develops autonomy; overcontrol leads to shame and doubt. |
C. Industry vs Inferiority | 6–12 years (School-age) | Children develop skills, productivity, and social relationships. Success results in competence and industry; failure results in inferiority. ✅ |
D. Generativity vs Stagnation | 40–65 years (Middle Adulthood) | Adults focus on contributing to society and guiding the next generation. Failure leads to self-absorpti |
Age | Erikson Stage |
|---|
Infant (0–1 yr) | Trust vs Mistrust |
Toddler (1–3 yrs) | Autonomy vs Shame & Doubt |
Preschool (3–6 yrs) | Initiative vs Guilt |
School-age (6–12 yrs) | Industry vs Inferiority |
Adolescent (12–18 yrs) | Identity vs Role Confusion |
Young Adult | Intimacy vs Isolation |
Middle Adult | Generativity vs Stagnation |
Older Adult | Integrity vs Despair |
When assessing a 2-year-old child brought by his mother to the clinic for a routine check-up, which of the following would the nurse expect the child to be able to do?
A. Ride a tricycle
B. Tie his shoelaces
C. Kick a ball forward
D. Use blunt scissors
Answer: C. Kick a ball forward p
Rationale:
A 2-year-old toddler is expected to have developed gross motor skills such as:
Kicking a ball forward
Running
Walking up and down stairs with assistance
Throwing a ball overhand
Age | Expected Skill |
|---|
1 year | Walks with support |
2 years | Kicks a ball, runs, climbs stairs |
3 years | Rides a tricycle |
4 years | Uses scissors, hops on one foot |
5 years | Ties shoelaces, skips |
After having a blood sample drawn, a 5-year-old child insists that the site be covered with an adhesive bandage strip. When the mother tries to remove the bandage before leaving the office, the child screams that all the blood will come out. The nurse interprets this behavior as indicating a fear of which of the following?
A. Injury
B. Compromised Body Integrity
C. Pain
D. Loss of Control
Answer: B. Compromised Body Integrity
Rationale:
Preschool children (3–6 years old) have an incomplete understanding of body functioning. They often fear that a hole in the body will not close and that blood or body parts may "leak out." This reflects a fear of compromised body integrityrather than pain or loss of control.
A preschool child typically views death as:
A. Reversible and temporary
B. Final and Permanent
C. A punishment
D. A part of life
Answer: A. Reversible and temporary
Rationale:
Preschoolers view death as temporary and reversible, similar to sleeping or going away. They do not yet understand the permanence of death.
A. Reversible and temporary – Correct
B. Final and Permanent – Usually understood by older school-age children
C. A punishment – Preschoolers may sometimes associate illness or death with punishment, but their typical concept of death is reversibility
D. A part of life – More mature understanding
After teaching a group of mothers about temper tantrums, the nurse knows the teaching has been effective when one of the mothers states which of the following?
A. “I will ignore the temper tantrums”
B. “I should pick-up the child during the tantrum”
C. “I’ll talk to my daughter during the tantrum”
D. “I would put my child in 10 minute-time out”
Answer: A. “I will ignore the temper tantrums”
Rationale:
Temper tantrums in toddlers are often attention-seeking behaviors. The most effective response is planned ignoring (as long as the child is safe), which prevents reinforcement of the behavior
A 5-year old child with cystic fibrosis is admitted to the hospital due to bronchopneumonia. Which of the following signs and symptoms would be most helpful in providing supportive diagnostic data for this child’s condition?
A. Cough and Fever
B. Constipation and Vomiting
C. Dysuria and Rash
D. Weight Loss and Stringy stools
Answer: D. Weight Loss and Stringy stools
Rationale:
In Cystic fibrosis, thick, sticky mucus affects the lungs and pancreas. Pancreatic enzyme blockage leads to malabsorption, causing steatorrhea (fatty/stringy stools) and poor weight gain or weight loss, which are key supportive findings of the disease.
When teaching the parents of an older infant with cystic fibrosis about the type of diet the child should consume, which of the following would be most appropriate?
A. Low Protein Diet
B. High Fat Diet
C. Low Carbohydrate Diet
D. High Calorie Diet
Answer: D. High Calorie Diet
Rationale:
Children with Cystic fibrosis require a high-calorie, high-protein, high-fat diet to compensate for malabsorption and increased energy expenditure from chronic lung disease. The priority is ensuring adequate caloric intake for growth and maintenance.
A mother calls the ER department and reports that her 6-year-old child has awakened with a complaint of sore throat and pain on swallowing. She reports that the child was fine when going to bed. The child has a fever of 39.5°C orally and is restless, having difficulty breathing and appears quite sick. Which of the following questions is a priority for the nurse to ask to triage this client?
Answer: C. “Has the child been drooling?”Rationale:
The child’s symptoms (sore throat, high fever, painful swallowing, respiratory difficulty, and sudden onset) are highly suggestive of a possible upper airway obstruction, such as epiglottitis or severe pharyngeal infection.
The priority nursing concern is airway patency, and drooling is a critical warning sign of airway obstruction due to inability to swallow secretions.
A nurse is assessing a child suspected of acetaminophen poisoning. Which initial symptoms should the nurse expect?
A. Vomiting, sweating, pallor
B. Hyperactivity, dilated pupils, tremors
C. Seizures, hallucinations, tachycardia
D. Bradycardia, hypothermia, hypotension
Answer: A. Vomiting, sweating, pallor
A mother at 39 weeks gestation is undergoing an ultrasound. The physician notes the fetus is not in a cephalic presentation. Nurse Lina reviews the mother’s prenatal history. All of the following are factors that can contribute to a breech presentation EXCEPT:
A. The presence of excessive amniotic fluid
B. A diagnosis of multiple gestations
C. Implantation of the placenta over the cervical os
D. A maternal history of Nulliparity with a normal pelvic structure
Correct Answer: D. A maternal history of Nulliparity with a normal pelvic structure
Rationale:
A breech presentation occurs when the fetal buttocks or feet present first instead of the head. It is commonly associated with conditions that prevent normal fetal engagement or limit space in the uterus.
✔ Factors that increase breech presentation risk:
A. Excessive amniotic fluid (polyhydramnios) → allows excessive fetal movement, preventing stable cephalic positioning
B. Multiple gestations → limited uterine space leads to abnormal presentations
C. Placenta previa (placenta over cervical os) → obstructs the fetal head from engaging in the pelvis
During active labor, a client’s membranes rupture spontaneously. Nurse Lina immediately assesses the fetal heart rate and notes a sudden, prolonged deceleration. Upon vaginal examination, she palpates a pulsating cord protruding through the cervix. Which of the following non-pharmacological interventions is strictly contraindicated at this moment?
A. Placing the mother in a Trendelenburg position.
B. Using a sterile gloved hand to elevate the fetal presenting part off the cord.
C. Attempting to manually gently push the prolapsed cord back into the uterus.
D. Administering 100% oxygen via a non-rebreather mask to the mother.
Correct Answer: C. Attempting to manually gently push the prolapsed cord back into the uterus
Rationale:
In umbilical cord prolapse, the priority is to relieve cord compression and maintain fetal oxygenation. However, certain actions are dangerous.
📌 PNLE TIP:
Cord prolapse management priorities = “RELIEVE, RELIEVE, RELIEVE”
Relieve pressure (manual elevation, position change)
Oxygen to mother
Prepare for emergency delivery
🚫 NEVER push the cord back inside — that is the test’s classic trap.
A primigravida client is experiencing a prolonged second stage of labor. The physician decides to use vacuum extraction. Nurse Lina understands that this intervention places the neonate at highest risk for which specific complication that crosses the cranial suture lines?
A. Caput Succedaneum
B. Cephalohematoma
C. Subdural Hemorrhage
D. Craniosynostosis
Correct Answer: A. Caput Succedaneum
Rationale:
Vacuum extraction applies suction and traction on the fetal scalp, which commonly causes Caput Succedaneum, a diffuse scalp edema.
It is soft, puffy swelling
It crosses cranial suture lines
It is usually benign and resolves within a few days
Four hours postpartum, a client who delivered a 4.2 kg (9.2 lbs) infant complains of a sudden, continuous trickle of bright red vaginal blood. Nurse Lina palpates the uterine fundus and finds it firm, midline, and at the level of the umbilicus. Based on these findings, what is the most likely source of the hemorrhage?
A. Uterine atony secondary to macrosomia.
B. Retained placental fragments in the fundus.
C. Unrepaired cervical or vaginal lacerations.
D. Disseminated Intravascular Coagulation (DIC).
Correct Answer: C. Unrepaired cervical or vaginal lacerations
Rationale:
A firm, midline uterus means the uterus is contracted properly, so uterine atony is unlikely.
However, continuous bright red bleeding (trickling) despite a firm uterus strongly suggests trauma, such as:
Cervical lacerations
Vaginal lacerations
Perineal tears
📌PNLE TIP (VERY IMPORTANT):
Postpartum hemorrhage = think 4 T’s
Tone → uterine atony
Tissue → retained placenta
Trauma → lacerations (✔ correct here)
Thrombin → clotting disorder (DIC)
👉 If uterus is firm + bleeding continues = ALWAYS suspect TRAUMA
A newborn is diagnosed with Esophageal Atresia with Tracheoesophageal Fistula (TEF). Which triad of symptoms observed by Nurse Mark is universally recognized as the cardinal sign of this specific congenital defect?
A. Projectile vomiting, visible peristaltic waves, and an olive-shaped mass.
B. Coughing, choking, and unexplained cyanosis with the first feeding.
C. Currant jelly stools, inconsolable crying, and knee-chest posturing.
D. Failure to pass meconium, ribbon-like stools, and a distended abdomen.
Correct Answer: B. Coughing, choking, and unexplained cyanosis with the first feeding
Rationale:
Esophageal Atresia with Tracheoesophageal Fistula (TEF) is a congenital condition where the esophagus is abnormally connected to the trachea or ends blindly.
The classic hallmark (cardinal triad) appears immediately during the first feeding:
Coughing
Choking
Cyanosis
📌 PNLE TIP:
TEF = “First feeding problem = respiratory distress”
👉 If symptoms start with feeding + choking + cyanosis → THINK TEF immediately
Nurse Mark is planning post-operative care for an infant who just underwent surgical repair for a cleft palate. To ensure the integrity of the fragile oral suture line is maintained, which intervention should the nurse intentionally omit from the care plan?*
A. Administering pain medication around the clock to prevent vigorous crying.
B. Using a rigid suction catheter to vigorously clear oral secretions.
C. Applying soft elbow restraints (No-No's) to keep the infant's hands away from the mouth.
D. Offering clear fluids using a specialized wide-based nipple or cup.
Correct Answer: B. Using a rigid suction catheter to vigorously clear oral secretions
Rationale:
After cleft palate repair, the priority is to protect the suture line from trauma.
A 6-month-old infant is brought to the emergency room with episodes of sudden, severe abdominal pain, causing him to draw his knees to his chest. Between episodes, the infant appears completely normal. Nurse Mark assesses the diaper and notes stool that looks like red currant jelly. This assessment finding strongly points away from appendicitis and toward which condition?
A. Celiac Disease
B. Necrotizing Enterocolitis
C. Intussusception
D. Biliary Atresia
Correct Answer: C. Intussusception
Key hallmark findings:
Sudden, severe colicky abdominal pain
Infant draws knees to chest (pain relief position)
Periods of normal behavior between attacks
“Currant jelly” stool (mixture of blood + mucus from ischemic bowel)
📌PNLE TIP:
Intussusception =
👉 “Pain + Pea soup (currant jelly stool) + Palpable mass (sausage-shaped)”
❌Why the other options are wrong:
A. Celiac Disease
Chronic malabsorption
Steatorrhea, failure to thrive, abdominal distention
❌ Not acute episodic pain or bloody mucus stool
B. Necrotizing Enterocolitis (NEC)
Mostly preterm infants
Presents with feeding intolerance, distention, bloody stools
❌ More systemic illness, not intermittent well periods
D. Biliary Atresia
Obstructive jaundice
Pale stools, dark urine
❌ No acute abdominal pain or currant jelly stool
4-year-old child is diagnosed with Acute Epiglottitis. The child is drooling, leaning forward, and exhibiting inspiratory stridor. The physician has ordered several interventions. Which intervention should Nurse Sofia sequence as the ultimate priority?
A. Inserting an IV line to administer Ceftriaxone immediately.
B. Drawing a complete blood count (CBC) to check the white blood cell level.
C. Examining the child’s throat with a tongue depressor to confirm the swelling.
D. Leaving the child undisturbed on the parent’s lap while preparing a tracheostomy tray.
Correct Answer: D. Leaving the child undisturbed on the parent’s lap while preparing a tracheostomy tray
Rationale:
In acute epiglottitis, the highest priority is airway protection.
Best immediate action:
Keep the child calm
Allow child to remain in parent’s lap (comfort position)
Prepare for emergency airway (intubation/tracheostomy)
📌PNLE TIP:
Epiglottitis = “NO PEEP, NO LOOK, NO TOUCH”
No tongue depressor
No throat inspection
Priority = airway standby
A 2-year-old is admitted with viral Laryngotracheobronchitis (Croup). The parents ask Nurse Sofia why their child’s cough sounds like a barking seal. The nurse correlates which of the following pathophysiological mechanisms to the child’s current presentation?
A. A severe accumulation of thick, purulent mucus in the lower bronchioles.
B. Edema and inflammation localized in the subglottic area of the trachea and larynx.
C. Bronchospasm triggered by a hyperactive immune response to an allergen.
D. Collapse of the alveoli resulting from a lack of pulmonary surfactant.
Correct Answer: B. Edema and inflammation localized in the subglottic area of the trachea and larynx
📌 PNLE TIP:
Croup = “Barking cough = upper airway swelling (subglottic)”
Nurse Sofia is discharging an 8-year-old diagnosed with moderate persistent asthma. The child is prescribed a Short-Acting Beta Agonist (SABA) inhaler and an Inhaled Corticosteroid (ICS). Which parental statement indicates a need for immediate re-education by the nurse?
A. “I will have my child rinse his mouth out with water after using the corticosteroid inhaler.”
B. “We will use the SABA inhaler 15 minutes before he goes to his soccer practices.”
C. “When he starts having an asthma attack, I will give him the corticosteroid inhaler first.”
D. “I know the corticosteroid is for long-term control and must be used every single day.”
Correct Answer: C. “When he starts having an asthma attack, I will give him the corticosteroid inhaler first.”
Rationale:
This statement is incorrect because:
SABA = rescue medication (first-line in acute attack)
ICS = long-term control, NOT for immediate relief
Correct order:
SABA first (e.g., albuterol)
II. Then corticosteroid for inflammation control
📌 PNLE TIP:
Asthma meds:
SABA = “Save A Breath Immediately”
ICS = “In Control Slowly”
A 6-year-old boy is brought to the clinic by his mother. He has a history of Cystic Fibrosis (CF). The mother reports that despite eating large meals, he is losing weight and his stools are bulky, frothy, and extremely foul-smelling. Nurse Sofia determines that the child is most likely experiencing a deficiency in which of the following?
A. Pulmonary surfactant
B. Pancreatic enzymes
C. Intestinal villi surface area
D. Red blood cell production
Correct Answer: B. Pancreatic enzymes
Rationale:
In Cystic Fibrosis (CF), thick mucus blocks the pancreatic ducts, preventing digestive enzymes from reaching the intestines.
This leads to:
Fat malabsorption (steatorrhea)
Bulky, foul-smelling, frothy stools
Poor weight gain despite good appetite
Failure to thrive
PNLE TIP:
CF = “Thick mucus blocks lungs + pancreas”
Lungs → respiratory infections
Pancreas → ↓ enzymes → malabsorption
Nurse Sofia is conducting an assessment on a 1-year-old infant hospitalized with Bronchiolitis caused by Respiratory Syncytial Virus (RSV). Which isolation precaution must the nurse implement to prevent the transmission of this virus to other pediatric patients?
A. Airborne precautions using a negative pressure room and an N95 respirator.
B. Standard precautions alone, emphasizing strict hand hygiene.
C. Contact and Droplet precautions using a gown, gloves, and a surgical mask.
D. Protective reverse isolation utilizing a HEPA filtration system.
Correct Answer: C. Contact and Droplet precautions using a gown, gloves, and a surgical mask
Rationale:
RSV (Respiratory Syncytial Virus) spreads through:
Droplets (coughing, sneezing)
Direct contact with secretions or contaminated surfaces
📌 PNLE TIP:
RSV = “Runny nose spreads virus”
👉 Always remember: Contact + Droplet precautions
A 5-month-old infant is brought in with a rapidly expanding head circumference. The physician suspects Hydrocephalus. During the physical assessment, which specific ocular finding would Nurse Leo document as highly indicative of increased ICP in this infant?
A. Unilateral ptosis of the right eyelid.
B. Strabismus where both eyes turn inward.
C. The sclera is visible above the iris when looking straight ahead.
D. The pupils are completely unresponsive to noxious pain stimuli.
Correct Answer: C. The sclera is visible above the iris when looking straight ahead
Rationale:
This finding is known as the “sunsetting eyes” sign, a classic indicator of increased intracranial pressure (ICP) in hydrocephalus.
A 7-year-old child with a known seizure disorder experiences a sudden generalized tonic-clonic seizure in the playroom. Nurse Leo assists the child to the floor. Which of the following postictal assessment findings should prompt Nurse Leo to intervene immediately rather than observe?
A. The child is difficult to arouse and wishes to sleep continuously.
B. The child exhibits confusion and asks where he is.
C. The child has high-pitched inspiratory stridor and circumoral cyanosis.
D. The child complains of a severe, dull headache and generalized muscle aching.
Correct Answer: C. The child has high-pitched inspiratory stridor and circumoral cyanosis
Rationale:
This indicates airway obstruction and hypoxia, which is an emergency.
Post-seizure, the priority is:
👉 AIRWAY FIRST
📌 PNLE TIP:
Seizure care priority =
👉 “Airway is always first after seizure”
Nurse Leo is reviewing the cerebrospinal fluid (CSF) analysis of a 3-year-old admitted with suspected bacterial meningitis. Which set of findings confirms the physician’s diagnosis of a bacterial etiology?
A. Decreased glucose, elevated protein, and cloudy appearance.
B. Elevated glucose, decreased protein, and clear appearance.
C. Normal glucose, normal protein, and bloody appearance.
D. Normal glucose, slightly elevated protein, and clear appearance.
Correct Answer: A. Decreased glucose, elevated protein, and cloudy appearance
📌 PNLE TIP:
Bacterial meningitis CSF =
👉 “Low sugar, high protein, cloudy fluid”
10-month-old infant is brought to the clinic because he is not meeting his motor milestones. Nurse Leo suspects Spastic Cerebral Palsy based on a specific motor assessment. Which finding is universally recognized as an early hallmark of this condition?
A. The infant exhibits a negative Babinski reflex.
B. The infant’s legs cross stiffly like a pair of scissors when lifted by the armpits.
C. The infant uses a neat pincer grasp to pick up small objects.
D. The infant turns his head toward a loud sound in the room.
Correct Answer: B. The infant’s legs cross stiffly like a pair of scissors when lifted by the armpits
Rationale:
This is the classic “scissoring gait posture”, due to:
Hypertonia (increased muscle tone)
Spasticity of lower limbs
Early sign of spastic cerebral palsy
📌 PNLE TIP:
Spastic CP =
👉 “Scissoring legs = spasticity”
A 6-month-old infant diagnosed with Tetralogy of Fallot becomes highly cyanotic and begins breathing rapidly while crying during a blood draw. Nurse Mia recognizes this as a hypercyanotic (“Tet”) spell. Of the following anticipated orders, which should the nurse sequence as the ultimate priority?
A. Administering Intravenous Morphine Sulfate.
B. Applying 100% oxygen via a blow-by mask.
C. Placing the infant immediately into a knee-chest position.
D. Administering an intravenous fluid bolus of Normal Saline.
Correct Answer: C. Placing the infant immediately into a knee-chest position
Rationale:
A Tet spell is an acute episode of severe hypoxemia caused by increased right-to-left shunting in Tetralogy of Fallot.
📌PNLE TIP:
Tet spell management =
👉 “Knee-chest FIRST, Oxygen SECOND, Morphine NEXT”
✔ Always remember:
Position → Oxygen → Medication → Fluids
A newborn in the nursery is diagnosed with a Patent Ductus Arteriosus (PDA). When Nurse Mia performs a cardiac auscultation, which abnormal sound should she expect to clearly identify?
A. A harsh, holosystolic murmur at the left lower sternal border.
B. A continuous, loud machinery-like murmur at the upper left sternal border.
C. A weak, distant, muffled heart sound with a pericardial friction rub.
D. A diastolic rumble at the apex radiating to the left axilla.
Correct Answer: B. A continuous, loud machinery-like murmur at the upper left sternal border.
Rationale:
A Patent Ductus Arteriosus (PDA) is a congenital heart defect in which the ductus arteriosus fails to close after birth, allowing blood to flow from the aorta to the pulmonary artery.
The hallmark finding is:
🎧 A continuous “machinery-like” murmur heard best at the left upper sternal border (LUSB) or left infraclavicular area.
Why the others are incorrect:
A. Harsh holosystolic murmur at the left lower sternal border → typical of a Ventricular Septal Defect (VSD).
C. Muffled heart sounds with a friction rub → suggests pericarditis or pericardial effusion.
D. Diastolic rumble at the apex → associated with mitral valve disorders.
PNLE Tip 🩺
PDA = “Machine keeps running”
➡ Think continuous machinery murmur.
Nurse Mia is assessing a 4-year-old child admitted with Kawasaki Disease. The child is receiving high doses of oral Aspirin. The mother asks why her child is receiving Aspirin when she was taught it causes Reye's syndrome. Which response by the nurse is the most accurate?
A. "Your child is over the age of two, so the risk of Reye's syndrome no longer applies."
B. "Aspirin is strictly being used to bring down the dangerously high fever."
C. "Aspirin prevents the blood from clotting inside the inflamed blood vessels of the heart."
D. "Aspirin is the only medication that can cure the viral infection causing Kawasaki disease."
Correct Answer: C. “Aspirin prevents the blood from clotting inside the inflamed blood vessels of the heart.”
Rationale:
In Kawasaki Disease, high-dose aspirin is initially used for its anti-inflammatory and antipyretic effects. After the acute phase, low-dose aspirin is continued for its antiplatelet effect, helping prevent clot formation in the inflamed coronary arteries and reducing the risk of coronary artery complications.
Nurse Mia assesses the blood pressure and pulses of an infant suspected of having Coarctation of the Aorta. Which paired assessment finding provides the most definitive evidence for this structural defect?
A. High blood pressure in the arms and low blood pressure in the legs.
B. Bounding pedal pulses and absent radial pulses.
C. Severe cyanosis in the arms and pink skin in the legs.
D. Equal, bounding pulses in all four extremities.
Correct Answer: A. High blood pressure in the arms and low blood pressure in the legs.
Rationale:
Coarctation of the Aorta causes reduced blood flow to the lower body and increased pressure proximal to the narrowing.
Classic findings:
💪 Hypertension in upper extremities
🦶 Hypotension in lower extremities
Weak or delayed femoral pulses (radio-femoral delay)
PNLE Tip:
“Coarctation = COARCT = C.O. = Cut Off flow to lower body”
7-year-old child returns to the unit following a cardiac catheterization via the right femoral artery. One hour post-procedure, Nurse Mia assesses the right foot and notes that it is cool, pale, and the pedal pulse is completely absent, whereas it was present 30 minutes ago. What is the nurse's priority action?
A. Elevate the right leg on two pillows to reduce venous congestion.
B. Apply a warm, moist compress to the right groin to dilate the artery.
C. Document the finding as a normal consequence of arterial spasm.
D. Notify the primary healthcare provider immediately.
Correct Answer: D. Notify the primary healthcare provider immediately.
Rationale:
After femoral artery catheterization, sudden:
❄ cool
⚪ pale
❌ absent pulse
indicates acute arterial occlusion or impaired circulation, which is an emergency.
A child with thalassemia was given deferoxamine (Desferal); which of the following should alert the nurse to notify the physician?
A. Decreased hearing
B. Hypertension
C. Red urine
D. Vomiting
Correct Answer: A. Decreased hearing
Deferoxamine is ototoxic. Thus, any hearing problem should be immediately addressed to the physician.
Mr. and Mrs. Robertson’s son was diagnosed with idiopathic thrombocytopenic purpura. They should be aware that the drug to be avoided is:
A. Acetaminophen
B. Aspirin
C. Codeine
D. Morphine
Correct Answer: B. Aspirin
Aspirin exerts an antiplatelet action and therefore may increase platelet destruction in ITP.
.A nurse provides medication instructions to a first-time mother. Which statement made by the mother indicates a need for further instructions?
A. "I should mix the medication in the baby food and give it when I feed the child".
B. "I should administer the oral medication sitting in an upright position and with the head elevated".
C. "I will give my child a toy after giving the medication".
D. "I will offer my child a juice drink after swallowing the medication".
Correct Answer: A. “I should mix the medication in the baby food and give it when I feed the child”.
The nurse would teach the mother to avoid putting medications in foods because it may cause an unpleasant taste to the food, and the child may refuse to accept the same food in the future.
A physician prescribes an IV solution of 500 ml 0.45% Saline with an incorporation of 20mEq potassium chloride for a child with dehydration. The nurse should check which of the following before administering this IV prescription?
A. Blood pressure
B. Height
C. Weight
D. Urine output
Correct Answer: D. Urine output
When it comes to hypotonic dehydration, electrolyte loss exceeds water loss
A child with Kawasaki disease is admitted to the pediatric ward. Which of the following medications will you expect to be a part of the treatment? Select all that apply.
A. Gamma Globulin
Correct answer
B. Warfarin.
C. Acetaminophen
D. Aspirin
E. Atenolol
Correct Answer: A, B, & D
The principal goal of treatment for Kawasaki disease is to prevent coronary artery disease and to relieve symptoms such as fever and joint pain so an antipyretic, antiplatelet, and gamma globulin is used.
A 6-year-old child is scheduled to have measles, mumps, and rubella (MMR) vaccine. Which of the following routes will you expect the nurse to administer the vaccine?
A. Intramuscularly in the vastus lateralis muscle.
B. Intramuscularly in the deltoid muscle.
C. Subcutaneously in the gluteal area.
D. Subcutaneously in the outer aspect of the upper arm.
Correct Answer: D. Subcutaneously in the outer aspect of the upper arm.
(MMR) the vaccine is administered subcutaneously in the outer aspect of the upper arm. The dosage for both MMR and MMRV is 0.5 mL.
Mrs. Cooper is concerned about her 4-month-old son’s unusual condition; which of the following statements made by her would indicate that the child may have cerebral palsy?
A. "He holds his left leg so stiff that I have a hard time putting on his diapers."
B. "My baby won't lift his head up and look at me; he's so floppy."
C. "My baby's left hip tilts when I pull him to standing position."
D. "I'm very worried because my baby has not rolled all the way over yet."
Correct
Correct Answer: B. “My baby won’t lift his head up and look at me; he’s so floppy.”
Hypotonia or floppy infant is an early manifestation of cerebral palsy. Typically, the infant lifts his head to a 90-degree angle by age 4 months with only a partial head lag by age 2 months.
Which of the following is the most common permanent disability in childhood?
A. Scoliosis
B. Muscular dystrophy
C. Cerebral palsy
D. Developmental dysplasia of the hip (DDH)
Correct Answer: C. Cerebral palsy
Cerebral palsy is the most common permanent disability of childhood.
A child newly diagnosed with diabetes mellitus has been stabilized with insulin injections daily. A nurse prepares a discharge teaching plan regarding the insulin. The teaching plan should reinforce which of the following concepts?
A. Always keep insulin vials refrigerated
B. Increase the amount of insulin before exercise
C. Ketones in the urine signify a need for less insulin
D. Systematically rotate injection sites
Correct Answer: D. Systematically rotate injection sites.
It is necessary to rotate injection sites because injecting in the same place much of the time can cause hard lumps or extra fat deposits to develop.
MgSo4 injections are painful to the patient. Which of the following is the BEST route for injection to prevent such negative experience for patient Joyce?
A. Intravenous injection at the main IV line.
B. Intravenous injection given through “piggy back”.
C. Intramuscular on each of the deltoid muscle.
D. Deep intramuscular using z-track technique on buttocks.
B. Intravenous injection given through “piggy back”.
The nurse must be alert to MgSo4 toxicity. Which of the following in NOT included?
A. Fetal bradycardia
B. Urine output of <30 ml per hour
C. Respiration of <12 per min
D. Increase in maternal pulse rate
Answer: D. Increase in maternal pulse rate
Rationale:
Signs of MgSO₄ toxicity include:
🚨 Respiratory rate < 12/min
🚨 Urine output < 30 mL/hr
🚨 Absent deep tendon reflexes (DTRs)
🚨 Decreased level of consciousness
🚨 Fetal bradycardia
A postpartum client is concerned because she can feel a "gap" between her abdominal muscles and the area feels soft. Upon assessment, the nurse confirms a painless separation of the rectus muscles. Which of the following statements by the nurse provides the most accurate information regarding this condition?
A. "This is an abdominal hernia that requires immediate surgical correction."
B. "This separation is a sign that your uterine ligaments have been permanently damaged."
C. "This is a rare complication caused by excessive weight gain during pregnancy."
D. "This is called diastasis; if it persists, we can offer you physical therapy."
D. "This is called diastasis; if it persists, we can offer you physical therapy."
According to the physiologic requirements listed in the textbook, how much additional daily iron does a pregnant woman need to support fetal growth and the increase in red blood cells?
A. 200 µg
B. 400 µg
C. 600 µg
D. 800 µg
C. 600 µg
Percentage increase of GFR during pregnancy
50%
Which of the following physiologic changes to the urinary system makes a pregnant woman more susceptible to bladder infections and pyelonephritis?
A. A 25% decrease in the diameter of the ureters.
B. Physiologic increase in urinary stasis.
C. A decrease in total bladder capacity by 1,000mL
D. A significant increase in the renal threshold for sugar.
B. Physiologic increase in urinary stasis.
An ultrasound reveals that a client has a platypelloid pelvis. During the second stage of labor, the nurse should be particularly observant for which of the following difficulties based on this pelvic shape?
A. The fetal head might not be able to rotate to match the curves of the pelvic cavity
B. The fetus will be unable to enter the pelvic inlet at all due to its large size
C. Rapid precipitate labor because the pelvis is exceptionally wide
D. Prolapse of the umbilical cord due to the "apelike" narrow transverse diameter
A. The fetal head might not be able to rotate to match the curves of the pelvic cavity
What is the specifically recommended resting or sleeping position for a pregnant person that allows for good circulation in the lower extremities and puts the weight of the fetus on the bed?
A. High-Fowler's position
B. Right-sided Trendelenburg
C. Supine with knees flexed
D. Left-sided Sims position
D. Left-sided Sims position
What is the recommended total weight gain range for a singleton pregnancy in a patient who is considered underweight before pregnancy?
A. 11–20 lb
B. 15–25 lb
C. 25–35 lb
D. 28–40 lb
D. 28–40 lb
nurse is teaching a client about Supine Hypotension Syndrome. Which physiological mechanism correctly describes why this condition occurs when a pregnant person lies flat on their back?
A. The fetus compresses the abdominal aorta, increasing blood pressure to the head.
B. The uterus compresses the renal arteries, causing fluid retention.
C. The expanding uterus puts pressure on the inferior vena cava.
D. The diaphragm is pushed upward, causing respiratory alkalosis.
C. The expanding uterus puts pressure on the inferior vena cava.
Rationale:
During pregnancy, especially in the 2nd and 3rd trimesters, the enlarged uterus can compress the inferior vena cava (IVC) when the client lies supine (flat on the back).
A nurse is reviewing the lab results from a client's first prenatal visit. The rubella titer is reported as 0.6. How should the nurse interpret this result?
A. The client is immune to rubella.
B. The client is susceptible to rubella.
C. The client has an active rubella infection.
D. The client should receive the MMR vaccine immediate
B. The client is susceptible to rubella.
Why the other choices are incorrect:
A. The client is immune to rubella. ❌
Immunity is indicated by a higher positive rubella IgG titer (usually ≥1.0 or ≥10 IU/mL depending on the test).
C. The client has an active rubella infection. ❌
A low titer indicates lack of immunity, not active infection. Active infection is assessed through rubella IgM testing and symptoms
34. A newborn is diagnosed with Congenital Rubella Syndrome. When assessing the infant, which cluster of physical findings caused by its teratogenic effects would the nurse expect to find?
A. Macrosomia, hypoglycemia, and hyperbilirubinemia.
B. Phocomelia, hearing loss, and intestinal atresia.
C. Cataracts, patent ductus arteriosus (PDA), and cleft lip.
D. Spina bifida, clubfoot, and hydrocephalus.
C. Cataracts, patent ductus arteriosus (PDA), and cleft lip.
Other possible findings:
Microcephaly
Developmental delay
Growth restriction
“Blueberry muffin” rash
35. Toxoplasmosis is a protozoan infection that is most commonly spread through which of the following routes?
A. Contact with uncooked meat or contaminated cat stool.
B. Droplet transmission from an infected person's cough.
C. Skin-to-skin contact with an infected feline.
D. Consuming unwashed leafy green vegetables only.
A. Contact with uncooked meat or contaminated cat stool.