H2 Determinants of behavior and behavior change
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
health behavior
behavior aimed to prevent a disease
illness behavior
behavior aimed to seek remedy
sick role behavior
any activity aimed to get better/well
health impairing habits or behaviors
Some of our behaviors are guided by habits (not necessarily an addiction), more automatic and more difficult to target
health protecting behavior
behavior aimed to protect health
determinants of behavior (3)
why do we behave the way we behave? (can overlap)
biological determinants
personal determinants
environmental determinants
Can be both RISK or PROTECTIVE
biological determinants
genetics, predisposition
metabolic traits (eg: easily sick of alcohol, coma)
personal determinants
personality, learning history, attitudes, knowledge, expectations
environmental determinants
availability (higher price on cigs → less easily available)
socio-cultural norms
financial/economic conditions (education, SES)
protective factors
resilience, strength, skills, environlental advantages
both systemic & individual level
risk vs protective facts = compensation for the other?
1 on 1 relationship can be misleading!
third variables may play a role! = confounds!
example: vitamine E and less coronary disease => is actually part of a general correlation with other variables like education, income, exercise, …
=> healthy habits cluster!
Health behaviors are correlated
healthy habits cluster
due to common determinants
observational findings can be misleading → confounds!
interactions between all these factors = complex and often non-linear
historical evolution of theories on behavior (pre 70s, 70s, 90s, now)
pre 70s : environmental determinants (poverty, housing, preventative health services)
70s : personal determinants (health education, social cognitive theories)
90s: more structural health promotion
present: choice architecture (suggestions, reminders, nudging, …), built enviromnent
choice architecture
~ nudging
A way to give suggestions/reminders/… in favor of a certain (healthy) behavior (e.g. how supermarkets are organized, attractive stairs in a shopping centers, architecture of highways, reminders of doctors appointment, …)
nudge
any aspect of the choice architecture that alters people’s behavior in a predictable way without forbidding opinions of changing economic incentives
FEAR DRIVE MODEL (+ NAÏVE AND COMMON SENSE APPROACHES)
= producing excessively frightening messages to preventively reduce behavior
Common sense, implicit, folk, naïve theories: based on elements such as
inform and educate
fear appeals (e.g. scary pictures on cigs)
disgust
repression, shame
Not so effective (not obvious/certain, short lasting, leads to habituation)
fear appeals
part of fear-drive-model: Make people scared about the risks so that they will not show the related behavior anymore (e.g. scary pictures on cigarette packs)
Why is the fear drive model not so effective? (6)
• Effects of lifestyle changes are not obvious and certain
• Work on knowledge, and negative feelings (which are short-term and not enough for long-term change)
• Punishment/reward
• Fear might not evoke a change in behavior
• It is short lasting without repetition
• Repetition leads to habituation: the fear diminishes with exposure to it
Subjective Expected Utility Theory
theory that purely cogntive models are derived from
> People as economic creatures: weigh costs and benefits of certain behavior
> emphasis on role of individual cognitions, rationality (social context ignored)
focus of (social) cognitive models to behavior change
focus on attitudes/beliefs
Beliefs about risk and efficacy
Beliefs about personal control
Social beliefs (e.g. perceived social norm)
Biases in beliefs about risk, risk perception (4)
Ideal: risk perception would be best approximated by the experts
Reality: risk perception can however be influenced by several biases: we are not completely rational thinkers
unrealistic optimism
availability of information
lack of personal experience with the problem
how the risk is framed
(other: automatic thinking, anchoring)
Unrealistic optimism
bias in beliefs about risk and risk perception
→ 4 problems
Belief that if the problem has never appeared, it won’t
Wrong estimation about frequency (belief that it is infrequent)
Belief that problem is preventable by individual actions, egocentric perspective
Lack of personal experience
adding ‘social’ in cognitive theories = SOCIAL-COGNITIVE THEORIES
Besides bias, also emotional and social components that influence behavior
→ Anxiety and fear
Definitely have an impact, although when isolated they are often not enough for sustainable behavior change
→ Risk (perception) has also a social component (family, peers, school)
The whole problem with risk perception framed in a cognitive perspective is that it ignores emotional and social aspects
→ importance of riskperception will vary across behaviors
→ motivation to change doesn’t necesarily lead to trigger the change itself
role of ‘beliefs’ in behavior change models
Beliefs are considered a crucial element in predicting health behaviors
personal control
self-efficacy theory
self-efficacy theory
Perceived self-efficacy = people's beliefs about their capabilities to produce designated levels of performance that exercise influence over events that affect their lives
→ beliefs about your ability to effectively perform the tasks needed to attain a valued goal
→ determine how people feel, think, motivate themselves and behave
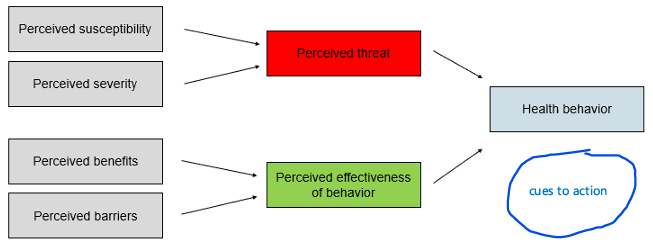
Health Belief Model (HBM) ( = cognitive model)
Assumes that all elements on left predict the likelihood of a (health) behavior
> Negative side: perceived threat ➔ how higher, how greater the likelihood of health behavior
F(perceived susceptibility to a certain condition) heighten likelihood
F(perceived severity of that condition) heighten likelihood
> Positive side: perceived effectiveness of behavior ➔ how higher, how greater the likelihood of health behavior
F(perceived benefits of health behavior) heighten likelihood
F(perceived barriers of health behavior) lower likelihood
Updates:
cues to action
self-efficacy
other: demographics, psychological characteristics
pros/cons
pros and cons of HBM
+) evidence shows associations with the expected directions
-) Relationship is weak and accounts for relatively small amount of variance
Methodology (often cross-sectional)
Measurements vary across studies
The outcome variables were the HBM variables itself rather than the behavior change
(largely) lack of social component, emphasis is on the individual (in the original version atleast)
According to the Health-Belief model (HBM) when will people engage in a behavior to prevent/detect/manage a condition? (4)
If they believe that…
They are susceptible to the condition (Cf. importance of tackling excessive optimism)
The condition has serious consequences
The preventive behavior is effective in reducing the risk or the consequence of the condition
Benefits of performing the behavior outweigh the costs
cues to action (HBM)
update to the health belief model
= internal or external events that trigger individuals to take action
(You might develop intention to do something, but the fact that you translate an intention to an action, might be related to cues)
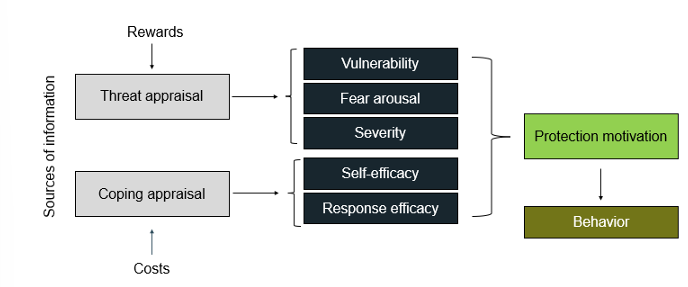
Protection motivation theory (= cognitive theory)
sources of information (environmental (persusion, observational learning), intrapersona (personality, experience))l)
will trigger 2 processes:
threat appraisals: influenced by perception of reward, elements that would increase or decrease maladaptive behavior
rewards = lead to increase in maladaptive behavior
vulnerability & severity = inhibitors of maladaptive behavior
coping appraisal: influenced by the perception of costs
strategies that can be used to deal with the threat
self-efficacy and response efficacy increase chance of adaptive behavior
=>
protection motivation = intention to perform a behavior
= positive function of vulnerability, severity, response efficacy and self-efficacy
= negative function of the rewards and costs
pros/cons
pros/cons PMT
+) different elements have different wirghts (self-efficacy strongest)
useful in predicting health behavior
PMT components may be useful for individual and community interventions
Meta-analysis on research on PMT: Association holds true whether measures based on intentions or on actual behavior
social-cognitive approaches
Central in these theories: social behavior is best understood as a function of perople’s perception of reality, rather than as a function of an objective description of the stimulus environment
Critical note: distinction between cognitive and cognitive-social approaches is sometimes blurred (models here just have relatively more social influences) = continuum
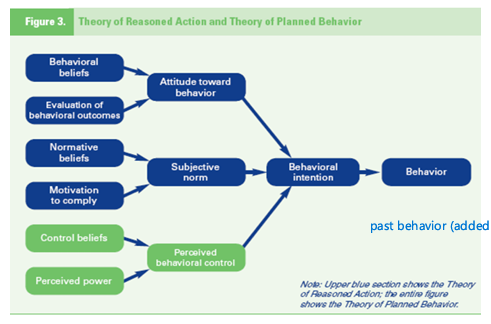
THEORY OF REASONED ACTION (TRA) & THEORY OF PLANNED BEHAVIOR (TPB) (social cognitive model)
Based on the assumption that humans are rational and can use information to make reasonable decisions
Behavior is a function of the willingness to carry out a behavior intention
The intention is a function of a person’s attitudes and social norms (subjective norm)
Attitudes refer to a person belief’s about the behavior and the relationship between behavior and the outcomes
Subjective norms or social norms refer to an individual’s beliefs about what others think about a behavior and the important of other’s approval and disapproval of the behavior
TPB: extension of TRA, adds elements ike..
perceived behavior control
adds concept of habits: past behavior taken in consideration when explaining current behaviors and intention for behavior in the future (automatic, less PFC control) (→ Accounts a bit better for the intention-behavior gap)
pros/cons: the different components predict very well the intention to change, but not so much of the behavior itself explained (gap because of self regulation, past behavior, behavioral & environmental control)
Social cognition theory (social-cognitive model)
Self-efficacy drives you to goals: how higher, the more the tendency to engage in goals and believe that you can achieve them
Expectations about the outcome also have a big impact
Facilitators and impediments
=> Together lead to behavior
main issues with social-cognitive models (7)
“glorified common-sense models”: all have the element of fear that was in the naive models, but just described in a more sofisticated way (perceived susceptibility, perceived severity, …)
Static models (lack of attention to change and fluctuating elements)
Focus on reasoning and intentional behavior (at expense of automatic behavior and habits)
Lack of attention to broader environment (broader than only your narrow social environment)
Intention-behavior gap (as already told)
Lack of predictive validity (as already told)
And: they do not state how to change behavior
TRANSTHEORETICAL MODEL OF CHANGE (Stage model)
Integrating leading theories of psychotherapy and behavioral change => HOW do people change, and why are some more succesful than others
general assumptions:
Behavior changes occur in stages (<> directly to a change in behavior)
Stages are both stable and open to change: you can move forward but also back
Planned behavioral interventions are necessary to assist individuals moving from early stage to later stage and maintenance
Without assistance change is not possible
Individuals at risk are not immediately ready/open to engage in change
=>
5 core concepts: • Stages of change • Processes of change • Pros and cons of changing behavior (decisional balance) • Self-efficacy • Temptation
Stages of change (transtheoretical model of change, stage model) (6)
Precontemplation: stage of unawareness of need of change. Perhaps pressure by others, perhaps a slight awareness/concern in yourself that one day in the future this should change
(motivation needed →)
Contemplation: a person is planning a change in 6 months (not longer somewhere far in the future). They recognize the problem but did not take any action yet (new year’s resolution), intention to change. Typically pros and cons are weighted.
Preparation: engagement in a decision process and prepare to take action (decision making stage in the original model) a. individuals are drinking less- intend to stop in 6 months
Action: commitment stage
Maintenance: avoid going back to old behaviors (6 months-5)
Termination: people believe they will not revert to previous behaviors
TTM and Motivational Interview (stage model)
a possibility to guide someone through the process of behavior changeµ
Expressing empathy: understanding the client’s perspective and not imposing the counsellor will
Develop discrepancy: directive discussion with clients about exploring internal motivations
Roll with resistance: discussing the resistance to change
Support self-efficacy: the counsellor helps the client to increase the belief in their abilities to make a change
problem with all models in general
Problems with risk perception (whether in fear model or in other models): at roots of many models but fails to predict behavior change
=> Risk perception not really needed in these models, not main driver of behavior (while self-efficacy is the best predictor)
SELF-DETERMINATION THEORY
focus on: motivation
Autonomous motivation
Controlled motivation = Extrinsic: someone imposes something/obligation, done for reward or to avoid punishment, you feel pressure to change
Basic psychological needs:
Competence: effective and competence
Autonomyy
Relatedness: cared by and cared for, sense of belonging
=> Needs haver to be fulfilled
if you want results, you need to create circumstances such that people have their basic psychological needs fulfilled
=> Leads to intrinsic motivation
Social networks and social support: the idea
Powerful influence that social relationships have on health behavior
• Social support is intentionally provided (differences with observational learning in Bandura)
• Social networks are a broader concept as compared to social support
o Not only peers, also about how you are embedded in your larger community, how the policies are, …
• They can act as protective factors
• Diminish effects of stressors
• Different members can provide different kinds of support
o Family, friends, school, work, …
• Crucial are the perceptions of support
Conceptual model for relationship of social networks and social support to health: important aspects
Stressors
Individual coping resources, organizational and community resources
o Important difference with other models
▪ One part with individual coping resources (as other models have)
▪ Also resources on a larger scale (goes further than just social support from e.g. peers)
Social ecological models
Features
o Multiple levels of factors influence behavior
o Influences across different levels o Multilevel interventions
o Necessity to be behavior-specific
Engaging in and changing behaviors is also influenced by higher levels
o E.g. on the level of community/policy: prenatal care, insurances, policies for cancer screenings, …
o Other levels did not have an eye for that